トップページ - 横浜国立大学学術情報リポジトリ
22
0
0
全文
(2) 70. (212). 第 10巻 第 2 号 (2005 年 8 月 ). 横浜国際社会科学研究. A@liberal@soci8@policy@stems@from@individu3@freedom,@equ3@opportunities,@and@non-government@intervention , It@has@been@difficu. ぬldersen. (1990). for@liberalist@reformers@to@imp. Ⅰ. Ⅰ. ment@th@@ market@based@po. cy@into@ state@poli y , Esping-. Ⅰ. s ぬ tes. Barg3ned@or@contracted@p. Ⅱ. guaranteed@to@prev3l@m3n. vate@we. Ⅰ. are@wil@logica. among@the@more@priV. Ⅰ. Ⅰ. y@rep. Ⅰ. cate@market@inequaliies,@but@is@a. Ⅰ. Ⅱ. o. ged@strata@in@the@ bor@forcC@ @@will@cert@n not Ⅰ. address》he『e are]eeds{f》he[ost}reca ouSy} ced『orkers・ , 64) Ⅰ. Ⅰ. Ⅰ. Ⅰ. ・. The@outcomes@of@most@liber3@ regimes@have@resu ed@in@a@combination@of@individu8@ se -responSbiliy@and du3i m These@outcomes@inCude@one@group@which@depends@on@the@we are@system,@a@middle@Cass@which Ⅰ. Ⅰ. Ⅰ. ・. depends@on@soCal@insurance,@and@a@privieged@group@with@p. Ⅱ. vate@insurance , This@type@of@. Ⅰ. ve@and@corporatist@we. Ⅰ. beralist@regime. , 1990). includes@the@United@States@and@British@welfare@systems@(Esping-Andersen The@conserva. Ⅰ. are@state@focuses@on@class@and@status:@Aust. Ⅱ. a,@ France,@. Germany@and. It3y@are@examples@of@this@modC THe@important@aspect@of@the@conservative@modC@ is@to@protect@the@status@and Cass@as@wCl@as@defend@soC8@ rights Contrary@to@liber@@ soC3@ policy,@the@conservaLve@poli y@dev3ues@the@market ・. ・. mechanism@of@the@provision@of@welfare@. services@ (Esping-Andersen. , 1990). ・. Another@characteristic@of@the. corporatist@modC@@@that@this@regime@has@usu3 Y@been@formed@by@the@Church@whi h@values@the@preservation@of@the Ⅰ. famiy , The@corporaLst@modC@. 8lows@the@government@to@intervene@in@famiy@matters@du. family@members@are@deemed@incompetent. Ⅱ. ng@the@period@when. , The“overnment(s》he〕ast〉esort’or《eeking》he『eare}rovi ions Ⅰ. in@the@corporatst@regime. Corporatism@had@a@strong@baSs@in@the@European@nations@not@only@because@of@tradition3@ mechani ms@such@as ℡ al@guilds, but@because@of@the@preservation@of@both@hierarchy@and@privilege. commer. , Most@of@all, the@Catholic. Church@has@played@an@important@role@in@shaping@all@social@reform. Scandinavian@countries@are@pioneers@of@soci3ist@soC3@ poli y In@th@@type@of@regime,@soC3@ rights@become uni ers8i Ⅰ c@and@"de-commodified"@even@for@midd Cass@ci zens@(Esping-Andersen,@1990) , The@go8@ of@a@soC8 ・. Ⅰ. Ⅰ. democra. Ⅰ. c@regime@ @@ to@ achieve@ equal@provi. univers3istic@insurance@system soC3im We. Ⅰ. , The@socia. ions@of@high@ qua. st@model@@@ we. Ⅰ. . "@ Esping-Andersen@menLons@that@not@8l@we. Ⅰ. Ⅰ. ty@welfare@for@a. ciizens@based@on@. Ⅰ. characterized@as@the@"fusion@of@. Ⅰ. are@states@are@di hotomied@into@th@@. are@policies@in@some@countⅡ es@might@be@a@combinaton@of@both@liber3@. Ⅰ. one. berali m@and. exact@Cassifica Ⅰ on. and@soC8@ democraLc@characteristics. Since@soCal@structure@has@changed@over@time,@soCalists@WCre@forced@to@inCude@the@middle@Cass@into@their universali tic@welfare@state Theヾwedi socialist‥emocra the}ioneer〉egarding》he「niversalism{f h. Ⅰ. c . middle@class@standards. As@such,@corporatist@po. Ⅰ. cy@has@diferen. a. Ⅰ. Ⅰ. for@soCal@insurance@and@its@various@benefits@depend@on@the. , liberal@policy@is@well@described@as@"welfare@states , residualism" occupational@and@status@base , On@the@other@hand. and@private-sector@weare Ⅰ. benefits@(Esping-Andersen. SoC3ist@poli y@is@idenⅠ fied@as@uni ersali m@and@has@the@least@differenals@of@the@soC8 Ⅰ. ・. , 1990) 3. New ̄ublic`anagement‖nd?ealth ̄olicy. As@a@liberalist@model,@New@Publ@@ Management@ management@during@the@1990's. ・. NPM@@@. deregulations@based@on@the@manageF8@ Eng. Ⅰ. nd,@Australia,@and@New@Zea. Ⅰ. Ⅰ. r@an3ySs@in@publi. publ@@ management@characterized@as@privatiza on,@contrac ng@out,@and form Especia y,@in@devCoped@countries@such@as@the@Unied@States, Ⅰ. Ⅰ. Ⅰ. ・. nd,@the@NPM@has@been@appli. organizations@and@agenCes@have@focused@on@imp McCourt・. (NPM)@ served@as@the@most@popu. Ⅰ. d@in@publ@@ management. menti g@the@NPM@program@@@. ・. Internation8@ aid. devCoPng@countries. examined》he‘ffecLveness{f¨PM[ethods{n《erVce‥every(n‥eveloping…ountries Ⅰ.
(3) ⅢleWe He@conCudes@that@there@@@. a@prob. Ⅱ荻. m@of@imp. Ⅰ. (K ㌶umiN0guch. eS ぬtemdHeaIthPoIicy. Ⅰ. menta. (213). け. on,@especi8ly@in@contractng@out. Ⅰ. there@are@non-NPM@methods@that@have@brought@the@success@of@the@implementati countries@such@as@BraZl@and@South@Africa. 71. Moreover,@he@argues@that. ・. n@of@programs@@@ devCopi. g. ,. 4@ The@Health@Care@System@in@Brazil There@are@three@m3or@ Ⅰ ers@of@heah@care@administration@in@Brazi;@Mini try@of@Health@located@in@Brasia,@a special@district@of@Brazil , the@State@Secretary@of@Health@in@each@state@and@the@Municipal@Secretary@of@Health@in@each Ⅰ. Ⅰ. muni. i ality. The’in3 path》o》he…urrent”ea h…are}rogram『as]ot‘asy’or》his…ountry》o‖chi ve‖nd]eeds》o|e Ⅰ. described@before@exp. ining@the@depth@of@the@current@hea. Ⅰ. Ⅰ. h@care@system .. In@the@authoritarian@era@from@1964@to. 1985.@a@highly@speciali ed@bureaucracy@dominated@control@of@various@policies@including@economic@and@even@health care@policies , A@highly@centralized@system@of@soC3@ poli y,@par@culay@at@the@feder8@ vC,@resu ed@in@economi growth@and@the@strength@of@the@private@sector@and@broadened@the@hea h@care@system@as@we However,@thi Ⅱ. Ⅰ. Ⅰ. Ⅰ・. Ⅰ. economic@power@which@faded@away@drastically@by@the@end@of@the@1960 , s , resulting@in@the@economic@cLsis@of@the 1970's@whi h@grea y@affected@the@soCal@fabric@of@BraZl Essent@ lly,@the@debt@cris@@@@ the@1980's@put@immeasurably@negative@effects@on@the@private@sector,@i clu4ng Ⅰ. va. ous@state@. Ⅱ. ・. stitutions,@whih@ended@up@wih@privati. Ⅰ. ati n@as@the@structur8@a4ustment. regime@during@th@@. pe. od@gradualy@lost@3l@of@abiiy@to@solve@th@@. government@was@di. trusted@by@cii ens,@@@ was@pressured@by@CVl@and@soCal@organi. Ⅱ. finanC8@ criSs. ・. , In@fact,@the@miliary. Since@th@@ authoria a. Ⅰ. Ⅱ. ons,@whi h@eventu8. an Ⅰ. 8lowed@them@to@form@the@baSs@of@the@public,@uni ersal,@and@democratc@hea h@care@system SoC3@ organi atons Ⅰ. and@civ@@ soCe bureaucracy. Ⅰ. es@put@forward@this@hea. Ⅰ. ・. h@care@initia ve,@which@was@par Ⅰ. Ⅰ. y@accepted@by@the@hea. h@care. Ⅰ. ・. Lobato@and@Burlandy@(2000)@ propose@that@the@conservative@elites@put@themse es@in@a@situation@where@they had@no@choice@but@to@enact@hea h@care@measures However,@when@the@elected@government@fo owing@the Ⅰ. Ⅰ. Ⅰ. ・. dictatorship@took@power,@it@focused@on@ ber3i m@and@rCected@these@proposed@soci3@. programs. Ⅰ. 4.1@ Centralized@Health@ Care@ Administration Hea pⅡ. Ⅰ. h@care@po. vate@sectors. ・. Ⅰ. cy@was@organized@into@the@three@subsystemS@. soC3@ security,@the@Mini try@of@Hea h,@and Ⅰ. SoC@@ security@was@unified@in@the@1930's@when@the@state@j0ned@@@. the@finanCng@of@publ@@ and. pFvate@companies'@ soCal@security@benefits,@one@of@whi h@was@to@provide@hea h@care@for@both@workers@and Ⅰ. h@the@Instiuton@of@Retirement@and@PenSon@was@establi hed, dependents , The@soCal@security@system,@in@whi became@the@dominant@provider@of@hea Bu. Ⅱ. Ⅰ. h@care@servi. es@for@the@exCuSve@BraZ. Ⅰ. an@populaton@. (Lobato@and. andy,2000) .. The@Minitry@of@Hea. Ⅰ. h@was@organized@as@a@para el@structure,@8ong@with@soci3@ security,@and@focused@on Ⅰ. preventive@care@until@the@1950's. ・. Moreover,@@@ was@responSb. Ⅰ. for@the@management@of@over8l@faC. the@provision@of@serVces@by@physi third@system , the@private@sector@engaged@@@. Ⅰ. ties, In@the. i ns@through@direct@payment. ,. Under@the@military@regime@from@ 1964@to@ 1985.@the@central@government@intervened@in@a social@poliCes, espeCa y@concerning@health@care@pol y,@whi h@stimulated@the@private@sector@and@legitmized@the@government Ⅰ. Ⅰ. ise. Ⅰ・. Ⅰ. During@th@@ pe. Ⅰ. od,@hea h@care@coverage@increaSngly@became@univers8@ Ⅰ. assume@responsibility@for@servi e@provi i n@itse. Ⅰ・. 市 eIns 廿杣廿on0fRe. 廿. rementandPenslonwe. 72@enacted@on@November@21. 丘. as@the@government@started@to. Wih@th@@ trend@of@uniersali ati n,@the@various@organiations@of. eunl%edastheNa. 億. 0nalIns 億血teforSoclaISecu lゆ underDecree 丘. , 1966.@ Under@this@unification , people@in@the@formal@labor@market@were@exclusively.
(4) (214). 72. 第 10 巻第 2 号 (2005年 8 月 ). 横浜国際社会科学研究 Brazilian?ealth,areヾystem(n》he・,. Figure・ Central. Mlnls rv,,0. .yof Budge@. Government. Health. -- Publlchospl は. 廿. ほ. Budget. 凹口 Compulso 卍 c0n@nbU 百 On. General Un Ⅳ frs 辻y 及. General@ TaXa Ⅱ 0n. government. DRG-like@fee れ. ぬ "" 。。. non@pro [. Budget. He3th-SUS. Government@. &‖mbulatories. Taxation. Sは le ゐ l0cal. Brazilian?ealth,areヾystem(n》he・, s. Figure・. s. №cal. Ⅹ. 皿. Ⅰ. Se 丘下Ⅱ Ce. Public. d. hoSP@ ロ l. 丘. hospltal. sぬ te. General. Fee@for. Taxation@ government. 用b№ ambulator. Social《ecurity. Bud ミ el Contribut@. Private. hoSPl 臼尽. Social SeCU ㎡Ⅱ. D. he 田 th. Subsidies. Private. Ellle Per@capil eefor. v"olun pr p ⅢdⅤ. 中 lrises ゐ. 色. た. Se. イスⅡ CeS. ㎡. pr Fee@for@service pd He田山 告. e.e-pald/ffteefo Own《ervices Salaries. pservice. Ⅰ. reimbursement. て. Company. hospi 田sand. ・. て. 30%}op. て. 甘 adeunlonS. Hospitals. ・. companies. POpula. Ⅱ. Private. 0n. hospi 臣尽. Ente 申 hses. ambulatories. S田 aneS. Fee’or. ニ. Se てⅤⅠ CeS. Private,li. Pa れ enlS Pre-paid}lans. Population. Se@りⅡ CeS. Pa Ⅱ entS. Doctors Fi ancing@flow De. Ⅱ. ven,. 皿. Fee. Ente 中 rlses. イ. o. て. is. seM㌧Ⅱ CeS. FinanCng@flow. 0w. Delivery@flow. 舖 urce:l 刀 bato,L.(2㏄O ,P.117. 舖 u 「 ce: ぬ bato 几 (2 ㏄ 0),P.122 ・. covered@by@social@security,@however,@those@in@the@rur8@ areas@were@not@Cigib for@the@proviion@of@hea h@care Ⅰ. servi es,@which@demonstrates@that@hea (Lobato@and@Burlandy. Ⅰ. h@care@was@mostly@reserved@for@p. Ⅱ. Ⅰ. vieged@peop. Ⅰ. to@receive@in@Brazil. , 2000). In@the@1970, s , the@National@System@of@Social@Security@and@Social@Assistance@(SINPAS). , which@was@responsible. for@soC3@ security@benefits,@and@then@Nation3@ Institute@of@Medi8@ Care@and@SoC8@ Security@ (INAMPS),@whi was@responSb. Ⅰ. for@medi 3@ were@created , Medi. 3@. serVces@were@pro. by@the@private@sector , The@health@centers,@publ@@hospita governments@provided@hea. Ⅰ. ded@not@only@by@the@publ@@sector@but@a o Ⅰ. and@pFmary@hea. Ⅰ. h@care@units@at@the@three@ve Ⅰ. Ⅰ. of. h@care@services@to@the@people , The@private@servies@were@CasSfied@as. Independent}rofesSonaor”ea. 1.. Ⅰ. Ⅴ. h. Ⅰ. Ⅰ. h《eitv@ ,. es…ontracted|y(nd* idua. Ⅰ. or…ompani s‖nd’inanced. by@the@private@sector@itsCf ・. 2.@ Private@sector@contracts@in@whi h@profit@and@nonprofit@unis@provided@serVces@to@the@publ@@ sector under@contract@to@the@federal@government@(Lobato@and@Burlandy. , p , 84). Since@p vate@medical@serVces@were@p3d@by@each@service,@it@became@cost Y@and@onY@served@certain@regions@where Lobato@and@Burlandy@ (2000)@ argue@that@there@were@no@health@care the@affluent@populaton@was@concentrated Ⅱ. Ⅰ. Ⅰ. ・. policies@established@based@on@actual@health@needs@and@epidemiological@profiles. economi 3ly@vulnerab Ⅰ. peop. During@the@centr3ized@mi. , which@led@to@the@exclusion@of@all. Ⅰ, Ⅰ. tary@regime,@there@was@an@increase@in@private@medi. al@servi es. ・. Since@social. security@coverage@was@extended@to@previouSy@uninsured@workers,@and@emergency@care@was@provided@for@t whole@popula. Ⅰ. on,@the@demand@throughout@the@health@care@system@increased,@and@INAMPS@contracted@to@the. private@sector In@th@@manner,@only@27@percent@of@a hospi8@ beds@were@publ@@ and@73@percent@were@in@the@private ・. Ⅰ.
(5) The@Welfare@State@and@Health@Policy@ (Kazumi@Noguchi). (215). 73. sector , This@expansion@of@the@role@of@the@private@hospit3@ gitimized@the@exitence@of@the@mitary@government@and Ⅰ. Ⅰ. , 2000). stimulated@the@private@sector@(Lobato@and@Burlandy. 4.2@ Health@ Care@ Reform It@is@important@to@note@that@there@was@such@a@great@struggle@for@BraZl@to@reach@the@imp mentation@of@the Ⅰ. universal@health@care@system@(SUS)@in@1988.@ The@Brazilian@reform@movement@started@as@a@reaction@to@the@highly unequ3@. health@system@imp. Ⅰ. mented@by@the@autho. 4.2.1@The@Universal@Health@System. ・. tarian@miliary@government@(1964-1985). Ⅱ. Sistema@Unico@de@Saude@(SUS). In@BraZl,@a@strong@socil@movement@in@the@hea and@bureaucrats. Ⅰ. h@field@began@in@1970.@among@professors,@par. In@the@Cv@@ soCety,@there@gradua. ,. Ⅰ. Ⅰ. amentarians,. y@emerged@a@saniary@movement@3med@at@the@radi. 3. transformation@of@the@na on , s@health@sector@in@order@to@uniy@the@current@fragmented@system,@so@as@to@decentrali e Ⅰ. health@care@dC. ery@and@introduce@the@democratic@deciSon-making@process. Ⅰ. di cusSon@of@health@demands@and@hea. Ⅰ. , The@1980's@were@a@pe. h@care@poli ies , The@ 1988@BraZli. Ⅰ. Ⅰ. institutional@obstacles@of@the@health@care@reform@movement@in@Brazil and@ a@lack@of@a@so. Ⅰ. d@ mass@base@. in@the@ soCety. ・. Moreover,@. ・. od@of@intense. Constiuton@guarantees@univers8. n@. health@care@coverage,@which@gives@acitizens@equal@access@to@hea h@care. Ⅱ. Weyland@ (1995)@ examined@the. ・. These@obstacles@were@pervasi. e@clientalism. the@ state-centered@strategy@recorded@. accomplishment@although@it@did@have@some@positive@results@in@its@ear. Ⅰ. Ⅰ. mied. stages ,. Ar@cle@of@33@of@the@Basic@Law@of@Health@8,080@declared@that@the@financial@resources Saude@ (SUS)@ should@be@deposited@into@special@accounts@and@allocated@under@Ministry@of@Health@control@ (Brasil 2003). It@a o@dec red@that@finanC3@ resources@for@heah@care@come@from@sever3@ sources,@inCuding@the@soC3 security@budget@and@other@feder3@ budget@sources These@resources@are@adminitered@by@the@Mini try@of@Hea h Ⅰ. Ⅰ. Ⅰ. Ⅱ. ・. through@the@National@Health@Fund. The@Mini. ・. try@of@He8th@admi. i ters@matters@through@an@auditing@system@and. the@confirmation@of@health@care@programs@approved@as@the@resources@of@the@states@and@muniCpalities of@corrupti n@or@the@miappropr@. ti n@of@health@care@funds , the@Mi. Ⅰ. ・. In@the@case. stry@of@Health@has@the@authority@to@appthe Ⅰ. ed@by@ w ,. necessary@punihments@as@determi. Ⅰ. Article@35@of@the@Basic@Law@of@Health@declared@that@the@establishment@of@the@amount@of@the@money@transfer to@states,@the@feder8@ditⅡ ct@and@muni. ip8ities@should@be@based@on@the@following@criteria@according@to@an@an3ysis. of@the@program , s@techniqueS I,. II,. Region8@ demographic@profile Epidemiological}rofiof》he〉eSdent}opu tion Ⅰ. Ⅰ. III,. Quantitatve@and@qualiative@characteristics@of@the@hea h@care@system@in@these@areas. IV ,. Techni. V,. VI ,. Ⅰ. a,‘conomic,‖nd’inancil}erformance(n‘a i r}eriods Ⅱ. Distribution@to@the@health@sector@in@the@state@and@municipal@budget Provi i ns@of@the@five-year@p n@for@i vestment@@@ he3th Ⅰ. Moreover,@half@of@the@resources@to@. states@and@muni. ipal ies@are@di t buted@based@on@the@number@of Ⅰ. Ⅱ. residents. Law@8,142/90@regulated@community@participation@in@the@Universal@Health@System@and@the@intergovernmental financial@transfers@related@to@he3th@care , The@SUS@established@the@following@organizations@within@each@sphere@of government;.
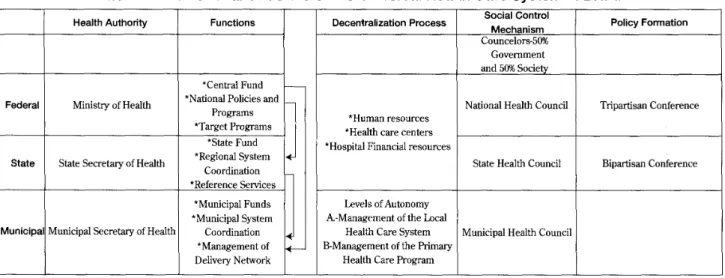
(6) 74. (216). 第 10巻第 2 号 (2005年 8 月 ). 横浜国際社会科学研究. Tab@. l stituti. 1. Health@Authority. n@. Structure{f》heゞniversG Heath,areヾystem(n。razil. Functions. Decent. ア. Social@Control. allza Ⅱ on Process. Policy@Formation. Mechanism Counre@ors-5㈱. Govemmment md5. ㎝ Socie. ・. *"Central:und. Pede al ァ. *Na 廿 on 目 P0 Ⅱ ciesand. Minis 廿rryofHe 引山. Pr0gr. Na 廿 OOnalHe引山 Councll. 皿Ⅱ S. *Target@Programs 。 Sぬ teFu Ⅱ d State. *Health@care@centers Sね leHeal 山 C0unc. " unicipalFunds *Municipal@System al@Mu Ⅰ ci al@Secretary@of@Health@. Coordi. A.-M ㎝aeemenlof. Health@Care@System. ation. *Management@of De Ⅱnve 卍Ne ㎞ork Source:@Fleury. ㎡ s挺lC0@ ㎡ e丘 ence. Bip 沖. Ⅱ. Levels@of@Autonomy 市 e №。 杣. ㍉Ⅰ. Munici. 氏 nce. *Hospial@Financi3@resources. *@Re8on8@ System Coordination *Reference@Services. Sぬ tteSecre ぬ lryofHe 田田. Tnpa ㎡sanConfe. *Human@resources. Municip 田 Heal 伍 Counc Ⅱ. B-Management@of@the@Primary Health,are ̄rogram. , S . (2001) , p , 20. (1)?ealth,onferences (2)@He3th@CounC. Ⅰ. A@Hea h@Council@consists@of@representatives@of@government,@service@providers,@hea h@speCalists,@and@users@of@the Ⅰ. Ⅰ. hea h@service, Ⅰ. Representa. Ⅰ. ves@of@users@must@comprise@50@percent@of@this@group. ・. Additiona. Ⅰ. y,@the@Hea. Ⅰ. h. Conferences@ and@the@Hea h@ Councis@have@func onal@organizations@and@rules@that@deTne@the@proper admlnls 比a Ⅱ onofeachCounc Ⅱ (Bras Ⅱ, 2003) Regarding@finanC3@ resources,@ Law@8142/90@declared@the@allocaton@of@the@financi3@ resources@from@the Ⅰ. Ⅰ. National@He3th@Fund@to@the@muni. i ali@ s,@states,@and@feder3@ di tricts@@@regular@and@automat@@ form , In@order. for@the@munii alities,@states,@and@feder8@ districts@to@recCve@these@finanC3@ resources,@they@must@have@the@He3th Fund , Health@Councils , Health@Pan P. Ⅰ. , Admi. strat* e@Report , and@Commissi. n@based@on@occupaton,@posiion,@and@s3a. Ⅱ. es@(BraSl,@2003) A@@ muni ・. must@audit@the@resources@for@the@he3th@sector@budget. n@for@the@elaboration@of@the@Health ipali es,@states,@and@the@feder3@di tricts Ⅰ. ・. One@of@the@purposes@of@the@Basic@operational@Regulations@(NoB)@ 1991@was@to@treat@equal both@public@and (Brasil private@providers@based@on@a@financial@model@for@payment@to@both@private@and@public@service@providers@ Ⅰ. 2003) , The@NoB@. 1991@was@administered@at@the@federal@level. , through@the@National@Institute@of@Social@Security. (INAMPS) , and@established@the@conventional@instrument@for@transferring@financial@resources@from@INAMPS@to@th states,@feder3@ districts@and@muni ipalii s . Moreover,@it@enacted@the@muniCp3iza muniCp3ities@should@meet@8l@of@the@baSc@requiements. MuniCp3@ CounCl@of@a@He3th@and@MuniCp3@. Heath@Fund. Ⅰ. on@of@the@SUS@and@stated@that. The@first@requiement@@@. ・. ・. The@MuniCp3@. Health@serv@ e@planning@and@budgeLng@are@det@led@in@each@state@or@muni. NOB@ 1991@ a o@establi hed@an@agreement@between@the@INAMPS@. He8th@P. that@muni Ⅰ. ipa ties@create@a Ⅰ. n@approves@each@CounCl. ipal@health@plan@ (BraSl,@2003). ・. ・. The. (National@Institute@for@Medic3@ AsSstance@i. Ⅰ. SoC8@ Insurance)@ and@the@states@on@stimuting@the@resource@transfer@from@INAMPS@to@the@State@Secretary@of Ⅰ. He3th@and@the@Muni. i 3@ Secretary@of@Health. ・. 4.2.2@ Municipalization@of@Health@Care@Service@Delivery ation@and@the@Path@to@the The@9t@@National@Hea h@Conference@set@as@its@centr3@ theme@"MuniCp3i Muni i 3i a on"@ and@establi hed@the@Bi arti an@and@Tripartian@Commi Sons@as@important@venues@for@the Ⅰ. Ⅰ. negotiation,@contracting,@art@ ulation,@and@integraton@in@the@hea h@care@adminitration , Addii Ⅰ. n3ly,@the@Nation3.
(7) The@Welfare@State@and@Health@Policy@ (Kazumi@Noguchi). (217)@ 75. Operation3@ Regulations@1993@(NoB@1993)@gave@muni ip3ities@the@authority@to@administer@the@health@care@system, which@was@an@unprecedented@step@on@the@path@to@a@decentr3ized@hea. The@flow@of@resources@was@based@on@the@. Ⅰ. h@care@policy@(BraSl,@2003). stage@of@management@autonomy@attained@by@the@. state@and. municipality@involved@in@the@NoB@1993@and@1996@respectively The@NoB@1993@esta6ished@three@4fferent@stages@of@management. , wHch@were@steps@along@the@defi. ℡. te@path. , 2002) , toward@the@total@municipalization@of@the@health@care@services@(De@Souza. The@three@stages@were@the@following:@(1)@the@Incipient@Management@Stage@(2)@the@Partial@Management@and@(3)@th Semi-complete@Management@Stage. ・. Under@the@InCpint@Management@Stage,@the@muni ipaliy@formed@a@MuniCpal. Health@ Council@and@a@Municipal@Health@Fund@that@separated@health@resources@from@other@public@resources. Federal@resources,@transferred@through@the@state,@were@deposited@in@part@in@this@fund,@with@the@amount@depend on@the@ contracts,@ pub. Ⅰ. c@ or@p. Ⅱ. vate,@ already@signed@by@the@. municipa. Ⅰ. ty. ・. Furthermore,@. the@ muniCpaliy. partiCpated@in@setting@the@limits@for@inpatent@and@ambulatory@care@payments At@the@second@stage@of@management. , the@Partial@Management@Stage. , the@municipality@participated@in@the. financing@and@was@abto@recei e@the@difference@between@the@limis@on@inpatient@and@outpaLent@services@and@what Ⅰ. had@actu8ly@been@spent muni. , As@for@the@thid@type@of@management,@the@Semi-complete@Management@Stage,@the. ipalty@took@complete@responsibility@for@providing@pub. Ⅰ. indi i u3@ health@servi es@through@publ@@ and@private@proⅤ ders. c@and@preven. Ⅰ. Such[uni ipa. ve@health@actvii Ⅰ. s,@ as@we@@ as. ties〉ece* ed》he’ull‖mount{f. resources@up@to@the@speCfied@lim@@ (De@Souza,@2002) Under@the@NoB@1996.@only@two@management@Stuations@rem3ne4@. Complete@Management@of@BaSc@Care@and. Complete@Management@of@the@Munci. al@Health@System ,. the@requiements@of@the@former@InCpi. nt@Management@Stage. federal@resources@for@the@full@health@system@or@for@on. Under@either@of@them. , the@mu. Ⅰ. cipaliies@had@to@fu @l Ⅰ. , The@main@diference@was@in@the@abiliy@to@rece*. e. basic@care According@to@2001@ statistics, 4,952@of@5,560. Ⅰ. ・. municipalities@qualified@as@the@Complete@Management@of@Basic@Care@and@the@remaining@of@564@qualified@as@the Complete@Management@of@the@Muni. ip8@ Health@System@(De@Souza,@2002). , 1). In@order@to@be@qu8ified@as@the@Complete@Management@of@BaSc@Care,@the@muni ip3iies@had@to@meet@cert3n tons@and@to@partiipate@in@the criteria,@which@inCuded@a@commiment@to@provide@the@basic@package@to@their@popu Ⅰ. implementation@of@information@systems@and@a@BaSc@Hea ev3uation@purposes. , In@those@mun. Ⅰ. Ⅰ. h@Care@Agreement@used@for@both@monio. Ⅱ. ng@and. ip8ii s@that@did@not@qualify@as@eiher@management@category,@the@resources. were@controlled@by@the@state , which@had@the@responsibility@to@bring@them@up@to@the@level@of@the@first@management situation@(Lobato@and@Burlandy , 2000) Moreover,@both@NoB@ resources. 1993@and@1996@establihed@the@provi. , The@first@method@was@the@automa. Ⅰ. ion@of@two@baSc@mechani. ms@for@transferⅡ ng. c@transfer@of@resources@from@the@feder8@ government@to@state@and. municipalities@for@primary@and@ambulatory@care,@based@on@popula@on@criteria , Under@this@transfer@system,@the feder@@ government@presc inhabiant@of@the@muni. bed@the@transfer@of@a@fixed@amount@of@12@Brazilan@rea@@. Ⅱ. ipa ty Ⅰ. ・. Special@incentives@for@municipaltes@that@estab. programs,@such@as@famiy@doctors,@were@a. Ⅰ. o@presc. Ⅱ. (R$)2)@per@year@for@each Ⅰ. shed@baSc@primary@health. bed , This@direct@transfer@from@the@feder3@. government@to. municipal@government@eliminated@the@role@of@the@state@to@3locate@the@resources@to@the@muni ip8ii s@(Lobato@and Burlandy,2000). ,. In@September,@2000.@Congress@approved@Constiu. Ⅰ. onal@Amendment@29@mandatng@an@increase@in@funding. levels@for@the@health@care@sector , This@Constitution8@Amendment@requies@states@and@muni. ipalities@to@earmark. 12%@and@15%@respectvely@of@the own@revenue@for@health@and@the@federal@government@to@maint3n@the@fiscal@effort Ⅰ. attached@to@health@by@linking@growth@in@health@sector@financing@to@nominal@GDP@growth@(Wo. Ⅱ. d@Bank , 2003).
(8) (218). 76. 第 10 巻第 2 号 (2005年 8 月 ). 横浜国際社会科学研究. The《econd[ethod{f》ransfer『as》he‥iect》ransfer》o}ubl@ and}rivate”ea h}ro Ⅴ ders,’or《ervices Ⅰ. re ⅠⅠ ng@to@hospi8@stays,@high comp Ⅰ. x@procedures,@and@ambu. Ⅰ. Ⅰ. tory@ser Ⅴ ces,@especi3 office@v@ is@ (Lobato Ⅰ. and。urlandy , 2000) ,. 4.2.3@ Regionalization@of@Health@Care@Services The@federal@government@in@2001@issued@the@Normal@operational@Law@of@Health@Assistance@ (NOAS). The. ・. man@features@of@the@NoAS@are@the@promoton@of@greater@equiy@in@the@use@of@resources@and@access@by@the population@to@all@levels@of@health@care@(World@Bank , 2003) , In@order@to@prevent@the@continued@fragmentation@of@the. hea h《ystem}lus》he‖ssoCated〕oss{f‘conomi s{f《c8e‖nd{f》he《ize{f》he〉isk}ool,[uniCpalities『ere grouped@into@micro-regions This@built@on@NoB@96@by@expanding@the@use@of@per@capia@payments@to@cover@a@wider Ⅰ. ・. package{f《ervices‖nd|y…omPeting》he》ransfer{f》he[anagement{f’ederal’unds》o[icro re8ons , ・. Some@new@features@of@NoAS@improved@equality@among@the@municipalities , regulating@the@funds@distributed government》o》he[uniip8ii. from》he’eder8. s. ・. The’irst’eature . as@an@instrument@for@greater@equity@in@the@ditribuLon@of@feder3@ states》o‥ivide》he@. territory(nto[ul -muni. ip8. Ⅰ. 8locaton@of@feder3@ recurrent@funds@and@a. Ⅰ. resources. Ⅰ. , Moreover,@the@NoAS@2001@requires. hea h[icro-regions‖nd》o「se》h@. as‖|aSs’or》he. Ⅰ. o@for@investment@p. Ⅰ. nning , The@second@characteris. establi hed@a@transparent@system@for@resource@3locaLon@across@mi. imp ment@speCfic@methodo. that》he¨oAS・. Ⅰ. c@of@NoAS@2001. ro-regions Th@@ system@requies@states@to ・. gi s,@plus@devCop@expli @@criteria@for@both@investment@as@weas@budget@p nning. Ⅰ. Ⅰ. Ⅰ. Budget@p nning@(uSng@Intergovernment3@Budget@Programming@Agreements)@estimates@the@financil@needs@of Ⅰ. each[uni ip8iy|ased{n》heヾze‖nd》he‘pidemiologi status{f》he}opula on‖nd‥ivides・ 3. transfers@to@muni i 3i@ manage》he@. s@ (grouped@@@. Ⅰ. micro-regi n)@based@on@the@@ needs , Mi ro-regi ns@are@then@ent@ d@to Ⅰ. own》ransfers‖nd‖ssign》hem》o}ay’or《peCfic《ervices(n》he@ territory{r「se》hem》o}ay’or. serVces@proVded@to@the@@. popu. Ⅰ. Ⅰ. on@e. Ⅰ. ewhere@(Wo. Ⅱ. d@Bank,@2003). Although》he(nfluence{f》he¨oAS・. mi ro-regi ns@are@undefined , Three@mode. , the“overnance‖nd[anagement’or》he. of@the@management@are@presen y@being@tested@in@diferent@parts@of Ⅰ. Ⅰ. Brazi , In,eara,31》he[icro-regions‖re[ainly[anaged|y》he〉egi n3 outposts{f》he《tate”ea h《ecretariat with@varying@degrees@of@partiipation@by@muniip3iies In@some@areas@of@Brazil,@micro-regins@are@formed@by@a consortia@of@muniip3ities@that@create@an@ad@hoc@agency@for@managing@hea h@care@wihout@part@ipaton@of@the Ⅰ. ・. Ⅰ. state , In@other@states@of@BraZl,@the@muni sma. ip8i es@are@allowed@to@manage@part@of@the@budget@of@neighbo. er@muni ipa ties@(sate ies)@ wih@varying@participaton@of@the@sate. Ⅰ. Ⅰ. Ⅰ. Ⅱ. Ⅰ. Ⅰ. ng. ies@and@of@the@state@in@the@daiy. management{f〉esources{r(n…ontrol Diferent[anagement《tYes‖re[ore kCy》o|e(nfluenced|y》he Ⅰ. ・. politic3@ affili on@of@the@parti ipaLng@mayors@and@state@governments@than@by@techni There . a. Ⅰ. oヽegion3i aton.iector ̄ (PDR) n. Ⅰ. consideraLons@of@deSgn. 3@. Ⅰ. Among》hese〉egions,『hich”ea h《ervi es『@l|e Ⅰ. ・. transferred@depends@on@vaFous@servi es@needed PDR@@@ coordinated@by@the@State@Hea h@Secretary Each@state@i Ⅰ. ・. ・. subdivided|y[odules,[iro-regions,‖nd[acro-regions Methods‖nd…oncepts‖dopted‥ifer‖mong《tates, ・. reflecLng@speci3@characteris cs@of@each@state , More@importanLy,@the@macro-region@@@ Ⅰ. high》echnology[edi serVces 3. ・. the@suppli r@of@terti ry@or. In》he〉egi n,》he”ea h[anagers‖re’u y〉esponSb for(den fying》he Ⅰ. Ⅰ. Ⅰ. Ⅰ. resources@and@cooperation@needed@to@promote@the@health@serv@ e@qu3iy@(Miniterio@da@Saude,@2004) Theゞniversal?ealthヾystem‖ndヽegionalization. 4.2.3.1. There@are@sever3@agendas@for@the@regin3i ation@of@the@uni ers@@ health@care@system , It@is@essenLal@to@define the〉o. Ⅰ. of‘ach“overnment(n》he〉egi n3izati n‖nd…o-management『ih》he「nivers3 he3th《ystem‖nd》o. establi h@a@more@s0@@ financi l@mechani m@@@ concert@wih@the@uni In》he「ni ers3. ers8@. he8th@system. hea h《ystem,》he”ea h〉egions‖ssume‖」it3 importance(n〉elaLon》o》he}erformance Ⅰ. Ⅰ.
(9) (219). The@Welfare@State@and@Health@P0y@ (Kazumi@NogucL) Ⅰ. of@health@poliy The@hea. Ⅰ. ・. h@regi ns@are@di ided@by@territories@composed@of@one@or@more@cii. the@cultural, economical , and@social@environment characte. Ⅱ. 77. s@and@are@based@on. , A@health@region@should@be@organized@based@on@the@identical. stcs@of@territo 3@ spaces@and@formed@wih@10-15@muni Ⅱ. ip8ities@(Miniterio@da@Saude,@2004). The@region@should@have@strategi s,@programs@and@proects@whi h@3l@reflect@the@partiular@needs@of@the@regin as follows. @@Creation@of@region3@ management @@Insta aLon@of@regul Ⅰ. Ⅰ. on@of@centr3@ offices. @@Accompli hment@of@region8@ agreements @@Qualifyi g@the@managers @@Qu8iying@of@3l@muni. ipa ties@in@the@regi n Ⅰ. @@Guarantee@for@risk@situations@to@cit@ ens. @@Guarantee@of@basic@attenLon@to@citizens @@Regionalized@hospi8@ attenLon @@Guarantee@of@urgency@and@emergency@serv@. es. @@Integration@of@humanizaLon@pr0ects @@Permanent@education@structure @@Re8onalizati @@Region3i. n@of@oral@health, mental@health , and@labor@health. aton@of@health@monito. Ⅱ. ng. @@Popular@pharmacy@implantation 4.2.3.2@ The@Role@of@the@Government@in@the@Regionalization It@@@very@important@to@identiy@the@task@shared@by@the@three@spheres@of@the@government@in@regi. n3i. because@of@the@complex@system@of@the@universal@health@system Municipalities@should@be@responsible@for@the@following@tasks. @@Take@part@in@regional@organi aLon,@making@services@available@for@all@citizens @@Parti ipate@in@the@regi nali ation@through@managers. @@Hire@skilled@workers @@Cooperate@in@prioritized@pr0ects@for@regi nal@health@devCopment @@Motvate@soC3@parti ipaⅠ on@in@the@region @@Ca for@technic3@ support@from@other@government@spheres Ⅰ. The@state@should@be@responSb. @@Coordina. Ⅰ. fo Ⅱ. Ⅰ. ng@and@provide@techni. @@. support@in@the@process@of@the@healh@regions. @@Iden fyi g@the@needs@of@itegration@with@@ the@he3th@regions Ⅰ. @@Parti ipating@in@regi nal@mee. Ⅰ. ngs. @@Inst3ling@services@@@ the@regi ns @@ProVding@technical@and@logis. Ⅰ. c3@. support@to@other@spheres. @@PlaCng@the@health@workers@who@make@perSstent@information@av3. Ⅰ. b. Ⅰ. to@hea h@regi ns Ⅰ. @@Moti ating@soci6@ participation@in@the@regi ns @@Organi i. g,. analyZng@and@making@available@all@information@gi. en@by@the@health@regins. @@Cooperating@financially@to@reduce@any@inequalities@in@the@regions @@Establishing@the@references@in@the@case@of@proVding@the@high@complexity@medical@services. a Ⅰ on.
(10) (220). 78. 第 10巻第 2 号 (2005年 8. 横浜国際社会科学研究. The@feder8@ government@shou. 月). be@responsib@@ for. Ⅰ. @@Pro Ⅴ ding@the@support@to@the@he8th@regins. @@Cooperati g@finanC3 w@h@other@spheres@of@government @@Gi ing@techni 8@ and@finanC3@support@to@vulnerabregi ns Ⅰ. Ⅰ. @@Integrat@ n@of@the@priority@of@the@feder3@government@program@@@ regi n@@ deve pment 8@ support@to@the@state @@ProVding@the@techni Ⅰ. @@Di cusSng@and@propose@a. Ⅰ. erna. Ⅰ. ve@too. @@Proposing@and@identifying@3l@posSb @@CoordinaLng@the@integra. Ⅰ. Ⅰ. for@region3@agreement. strategi s@for@SUS@in@the@regi ns. on@of@interstate@regions. Ⅰ. In@co-management@with@SUS , the@autonomy@of@the@each@government@sphere@should@be@guaranteed , especial the Ⅰ. muni. ip@@ government@(Ministerio@da@Saude,@2004). 4.2.4 NOAS 2002 The@main@changes@in@NoAS/SUS@01/01 , introduced@by@NoAS/SUS@01/02@were: can@be@as@enti d@as@the@Muni ipa (1)@The@muniCp3ity@whi h@serves@as@the@headquarters@of@an@asSstance@un@@ System@P nary@Adminitra on@in@the@case@of@a@sing muni ip3@ command@or@as@the@Extended@BaSc@Atten Ⅰ on Ⅰ. Ⅰ. Ⅰ. Ⅰ. Plenary@Administration@(GPABA)@in@the@case@of@single@state@command. (2)@NOAS fol. Ⅰ. SUS@01/2002@established@the@fact@that@the@financi l@assi tance@lim@@ for@each@state, sh8l@present@the. wing. Ⅰ. a@finanC3@ asSstance@ mit@wi be@imposed@on@every@state,@regardl. a.. Ⅰ. ss@of@is@adminitra@on@condi. Ⅰ. Ⅰ. on. b . conditions@of@adminitration@of@each@muni ip3ity,@or@vel@of@government,@are@responSbfor@medium@and@high Ⅰ. Ⅰ. complexity@command c.. share@of@financi3@ resources@for@the@attendance@of@reSdents@under@municipal@admini. traton. resources@for@the@attendance@of@inter-municip3@ references d , share@of@financi8@ e. share@of@financi8@ resources@for@the@attendance@of@reSdents@under@state@admini. ・. tration,. f. other@finanC8@resources@under@state@administration,@3located@in@muni ip3ities@or@in@states g. ・. global@financial@limits@of@each@state , the@sum@of@items@c , d , e@and@f,. (3)@NOAS Ⅰ SUS@01/2002@established@that@the@states@are@responsib for@the@admi istratin@of@publ@@ unis@of boratories@and@for@information@regarding@quaity@control,@saniary,@and@epidemiologi 8@ vigiance@and@public Ⅰ. Ⅰ. hea h@ boratories Ⅰ. Ⅰ. ・. 4.2.5@Expansion@of@Services@Provided@at@the@Municipal@Level The@NoAS@2001@c3ls@for@an@expansion@in@baSc@he3th@care@and@requies@muniCp8ities@to@pro Ⅴde@a@wi er array@of@serVces@(now@cad@PAB-ampliado@or@PAB-A)4'@to@the@@ popu tions SerVces@must@now@include@care@for the@control@of@tubercu Ss,@Hansen's@diease,@hypertenSon,@di betes,@childcare,@as@we as@matern3.@and@dent8 Ⅰ. Ⅰ. ・. Ⅰ. care .. Ⅰ. In@addii n,@a@new@feature@of@the@NoAS@2001@reinforces@equiy@by@expanding@the@use@of@capiation@systems. and@increases@the@share@of@funds@that@are@dist buted@automaLca Ⅱ. increaSng@the@v3ue@of@capita. Ⅰ. ons@associated@w@h@PAB-A. Ⅰ. y@on@a@per-capia@baSs@to@muni ip3iies,@by. ,. The@referral@system@among@the@mi ro-regi ns,@whi h@@@ part@of@the@NoAS@2001.@@@a o@one@of@the@new features, The@NoAS@2001@establihes@more@transparent@systems@to@manage@care@at@the@loc3@ vel@based@on@the Ⅰ. Ⅰ. use@of@networks@and@requires@mi ro-regions@to@imp ment@better@management@too Ⅰ. medium@complexiy@health@care@to@the@@ preven. Ⅰ. popula. ve@care@and@to@ration3ie@the@use@of@compl. profesSona. Ⅰ. to@prioritize@access@to@compl x@care. Ⅰ. ons ,. These@management@too. to@improve@the@regulation@of. Ⅰ. Ⅰ. wil@be@used@to@emphaSze. x@care@by@strengthening@the@use@of@referra. Ⅰ. from@baSc@care.
(11) ℡ eWeU Furthermore,@the@NoAS@2001@ performance@of@muni. enSUnngthec0mP. 肛 eS. ㌶. ぬteand Heal 由 Pol;cy (K umiN0%ch. makes@the@ state@responSble@for@both@ monioring@and@evalua. ipalii s@in@the@implementation@of@key@health@programs Ⅱ. (221). け. anCeofmunlclpa. Ⅱ廿. eSwlththebaSlcc. ng@the. States@become@responsib. ・. 「. for. Ⅰ. ㎞ ce ㎏ reements.. ぬ getssetbyBaSlcAsslS. 肛e. also@become@responSble@for@ensuring@that@sm3l@muni. Ⅰ. 79. S ぬteS. ipalities@obt3n@effec Ⅰ ve@access@to@referrals@for@servi es. provided@in@large@municipalities@(Brasil , 2003). 4.2.6@ Community@Participation@in@the@Decision-Making@Process@of@the@SUS The@federal@legislation , Article@of@the@Constitution@and@the@Law@of@8080/90@established@the@general@principles ,. whi h@inCude@communiy@part@. ipation@in@the@adminitration@of@the@Un*ersal@Health@Care@System@by@forming@the. Health@Conferences@and@the@Health@Councils@that@are@regulated@by@article@1@of@Law@8142 The@ Hea admini tra. Ⅰ. h@ Conferences@. Ⅰ. on. are@. the@ consu. Ⅰ. ation@ bodies@ whi h@ exerci e@ soci8@ control@ over@ hea. , Moreover,@they@have@the@function@of@assessing@the@hea. hea h@care@po Ⅰ. cy@at@each@level@of@government,@whi. Ⅰ. Ⅰ. h@care@Stua. Ⅰ. h@ care. on@and@of@propoSng@the. Ⅰ. h@gives@cii ens@the@right@to@partCpate@in@health@care. administration , Proper@Health@Conferences@must@be@establi. hed@in@four@years, while@the@m3n@ro. of@the@Health. Ⅰ. Conferences@is@to@di cuss@various@predetermined@issues@in@order@to@adopt@both@related@hea h@sector@agenda@and Ⅰ. practic3@ guidCines@for@the@upcoming@period@(BraSl,@2003). ,. The@Health@Councils@have@a@diferent@funcLon@from@that@of@the@Health@Conferences. , They@are@more@focused. on@he8th@care@deciSons@and@p0icy@making,@by@making@efforts@to@participate@@@ discusSon@concerning@health@care p0i y@i cludi g@the@independent@acti. iy@of@the@government. Although@the@Health@CounC. ・. Ⅰ. are@part@of@the. government@structure,@and@the@p ce@where@the@interests@of@diferent@segments@of@the@soc ty@converge,@they@have Ⅰ. Ⅰ. made@@@ posSble@to@negotate@the@proposa d ㎡erentphoh. は es. Ⅰ. and@to@deCde@the@direc. on@of@the@flow@of@resources@based@upon. (Brasil,2003). The@Law@of@8142/90@stipulated@that@the@Health@CounC. percent@of@the@@ membership@composed@of@government3@ Ⅰ. Ⅰ. Ⅰ. are@a@permanent@and@deliberative@organ,@w@h@50. representatives@and@of@representatives@of@the@soci ty@at. rge,@inCudi g@health@care@users,@pro Ⅴ ders,@and@speC8ists , Th@@ structure@enab. supervise@health@care@deci i n@making,@budgeting,@and@poli. Ⅰ. s@Ct@ ens@to@partiCpate@@@ and. y@execution@(BraSl,@2003). SoC3@ Control@in@the@case@of@Ceara3@p ys@an@important@ro in@the@d cusSon@and@poliy@making@of@healh Ⅰ. c 肛 epoIicy.. Ano 伍 ceroftheSecre. need@of@the@hea. Ⅰ. ぬryrofHealthofCear. 養. men. 廿. Ⅰ. onedthatsocl. h@care@users@which@represents@50@percent@of@the@Health@CounCl. Ⅰ. 引 con 比olexlststodetermnlne , Among@representa. Ⅰ. ぬe. ves@of@the. hea h@care@users,@the@communiy@health@agents@(explained@ ter@th@@paper)@are@important@advocates@for@ci@ en's Ⅰ. Ⅰ. interests, The@members@of@the@State@Health@Council@hold@a@monthly@meeting@to@dscuss@health@care@policy. , At@a. meeting@in@July@2003.@representatives@of@the@government@included@the@Secretary@of@Hea h@of@Ceara,@the@Minitry Ⅰ. of@Health,@the@Minitry@of@Educa Ⅰ on@and@Culture,@the@Council@of@State@and@MuniCp8iy@of@Hea h,@the@LegiSa Ⅰ. Assembly,@the@AssoCa. on@for@Mayors@of@Ceara,@the@Secretary@of@BaSc@Educa. Ⅰ. In 止ast丁Ⅱc 抽丘e. Assewlceprovlde Ⅱ. 丘. s,theFede. in@Ceara@attended@the@State@He3th@CounCl inCuded@medi. 3@. Ⅱ. ・. atlonofPh. Ⅱ. anth oplesofCe 丘. Ⅰ. ve. on,@and@ the@Secretary@of. Ⅰ. 肛后 andtheAss0clatlonf0rHospl. ぬls. Medical@profesSonals@who@partiCpated@in@the@Health@CounCl. assoCati n@representatives,@nurses@and@dentists. Most@of@the@muni. i 8ities@have@health@care@counC. Ⅰ・. 9@ In@most@of@muniCpali. Ⅰ. s@there@are@ten@muni. i al. counCls@whi h@cover@not@only@the@i sues@of@education,@health,@and@ bor@but@also@intersectional@iems . Health@care Ⅰ. issues@overlap@a of@the@muni ip3@counCls , A@new@program@was@launched@to@combat@domestic@ Ⅴo nce@against Ⅰ. adolescents@and@children nurses,@ educa. Ⅰ. Ⅰ. ・. At@a@seminar@for@th@@ program,@there@was@interdisciplinary@cooperation@among@doctors,. soci l@workers,@health@agents,@educators,@ and@directors@of@the@counc@@and@members@of@the@council@of on.
(12) (222). 80. Some@scho. 第 10巻第 2 号 (2005年 8 月 ). 横浜国際社会科学研究. rs@have@exami ed@the@effectieness@of@the@he8th@care@counCls , Souza@(2002)@ argues@that@the. Ⅰ. soC8@ poli y@counC. inCuding@hea. Ⅰ. counci@@ are@a@form3@reproduc. Ⅰ. h@poli y@counC. Ⅰ. Ⅰ. are@just@a@form3iy@of@the@system. on@of@what@the@rules@say,@undermining@fundament8@. Moreover,@there@@@an@accusaton@that@sub-na. on3@ e. Ⅰ. , Many@communiy. assump. Ⅰ. ons@of@partiipation. tes@exerCse@control@over@these@counCls. Ⅰ. Moreover,@CoCho@argues@that@state@and@soC3@ actors@in@the@saniary@movement@(the@soCal@movement@for health@reform@in@Brazil@started@from@the@1970 , s)@failed@to@establish@the@health@council@as@the@dynamic@political instituLon CoCho@uses@the@muni ip3@hea h@councils@in@Sao@Paulo@as@an@example@and@presents@sever8@ problems Ⅰ. ・. in@these@health@counC. , Firstly,@the@representaLon@and@criteria@for@organiZng@politic8@ representa. Ⅰ. Ⅰ. on@@@ the@one. matter@for@the@health@counci, In@the@case@of@secting@the@representatives@of@CVl@society@to@the@health@counci Ⅰ. Ⅰ. there@@@ no@raLon3e@involved@in@the@se. Ⅰ. ction@process@and@for@determining@the@exact@number@of@seats@availab. Ⅰ. ,. Ⅰ. for. this@group. The@ second@ i sue@is@the@ organi. a. of@procedures@for@di. on@. Ⅰ. parti ipatory@arena , In@the@muniCpal@hea h@counci ,@m8or@ro Ⅰ. Ⅰ. counc@@ or@the@chairperson@of@the@sesSon,@whi. as@hea h@counC Ⅰ. Ⅰ. cusSon@. s@were@p. Ⅰ. on@as@poliic3@instituⅠ ons. government@officia. and@med. Ⅰ. Ⅰ. Ⅰ. proVders@(CoCho,@2004). @@. ・. ip8@ hea h@counC Ⅰ. Schonleiner@ (2004)@ argues@that@only@pos ive@interac on@among@polii Ⅰ. Ⅰ. instiution@make@dCiberation@work@through@h@@ es@in@po. Ⅰ. The@body. , Some@representatives@of@the@Cvil@soCety@are@in@fact@ ss@educated@than@the. There@@@ another@an3ysis@regarding@the@effectveness@of@the@muni. Ⅱ. ・. should@guarantee@sharing@various@opini ns@and@having@the@equ8@opportunity@of@speaking@on@3l. Ⅰ. i sues@among@the@counCl@members. va. a. yed@by@the@execuLve@secretary@of@the. Ⅰ. h@were@inadequate@as@a@func. and@ deci ion@ making@suied@to@. tic8@ commitment,@Cvi. Ⅰ. commitment,@ Cvi ness,@and. 8@. case@studi s@in@four@muni ip8ii s@in@Brazil, Each@municip3ity. ness,@and@institu. Ⅰ. ons@and@has@some@diferent@outcomes@of@the@health@counC. Ⅰ. 4.2.7.@ Community@Participation@in@the@Implementation@Process@of@Health@Policy. 7. 七久. Program{f》he,ommunity?ealth、gents・. .1. The@pilot@program@of@Community@Health@Agents@(PACS)@was@launched@at@the@University@of@Brasilia@in@1974 and@1978@(Lavor@et@al ,, 2004) , For@the@Pilot@Project , the@University@of@Brasilia , government@of@the@Federal@District , the@KClogg@Founda. Ⅰ. on@and@the@Inter-American@FoundaLon@were@assemb. the@experiment@to@control@schistosomi Ss@within@the@communii. Ⅰ. d , The@idea@was@to@take@advantage@of. s@in@Pernambuco@(at@the@end@of@the@1940's). through@publ@@ education@efforts Through@the@prac ce@and@performance@of@hea h@agents,@heah@profesSona Ⅰ. ・. discovered@that@the@s0uti. n@for@many@prob. Ⅰ. ms@wihin@that@popu. Ⅰ. Ⅰ. Ⅰ. Ⅰ. t@ n@was@not@@@ the@hosPt3@ but@rather@@@ the. realm@of@the@fami and@community Ⅰ. P or@to@the@na on3ia. on@of@the@Program@for@the@Communiy@Hea h@Agents,@in@the@early@1980's,@Dr Lavor mented@th@@ program@in@the@state@Ceara@for@the@first@time@and@suggested@th@@ idea@to@Tasso@Jerei sati@who Ⅱ. imp. Ⅰ. Ⅰ. Ⅰ. Ⅰ. ・. became@the@governor@of@Ceara@in@1986. In@1987 , the@state@of@Ceara@experienced@a@severe@drought@and@hired@men@to@build@an@irrigation@system @@ hied@6,000@women@as@community@hea chidren,@ tuberculoSs@pa. Ⅰ. Ⅰ. h@agents@who@were@responsible@for@iden. ents,@ and@infants@in@need@ of@immuni. categorized@as@priary@health@care@services@ (Lavor@et@al, 2004) ・. Ⅰ. , while. fying@pregnant@women,@young. ation,@ 8l@of@whom@regarded@attention@that@i ・. In@Ceara@there@were@3,433@community@health. agents@in@ 1990 , 7,818@agents@in@1994@as@total , and@ 11591@ in@2002@ (IPLANCE. , 2003). ・. In@ 1991 , the@PACS@was. launched@as@the@national@program@and@the@Program@of@Fami He3th@was@commenced@in@ 1994.@ In@the@city@of Ⅰ・ Since Maranguape,61@there@were@123@communiy@health@agents@who@assisted@16,602@famii s@and@74,186@peop Ⅰ. then,@they@have@been@p. Ⅰ. ying@an@important@ro. Ⅰ. as@a@b dge@between@Ctizens@and@doctors Ⅱ. The…ompensation’or》he‖gents p3d|y》he《tate“overnment(n,eara,7'‖hough》he…ommuniy”ea h Ⅰ. Ⅰ.
(13) The@Welfare@State@and@He3th@Policy@ (Kazumi@Noguchi) agents@are@not@conSdered@publ@@. servants. (223). 81. Qualificati ns@for@the@communiy@health@agent@are@as@f0lowS@. ・. resident@of@the@ditrict@and@a@high@school@graduate , Regarding@selec. Ⅰ. on,@the@municipal@government@car. a Ⅱ. ed@out. the@se ction@process , Since@the@work@of@the@community@hea h@agents@has@become@more@speci li ed@after@twenty Ⅰ. Ⅰ. of@years@of@the@imp. menta. Ⅰ. Ⅰ. on@of@this@community@hea. Ⅰ. h@agents@program,@there@exists@an@argument@that@they. need@to@have@highly@specialized@training@from@both@social@workers@and@psychologists. The@city@of@Sobral@in@Ceara. ・. financed@and@implemented@a@pilot@program@one@year@ago@for@a@two@year@training@program@for@high@school@graduat community@health@agents. ・. As@for@future@prospect , community@health@agents@should@be@multi-specialists@and residents@more@profoundly. should@be@able@to@communicate@wih@the@@. Communiy@hea. Ⅰ. h@agents@formed@an@assoCaton@whi. Th@@ associaLon@establi hed@a@contract@w@h@the@state@whi to@communiy@hea. ,. h@@@ one@of@the@strongest@interest@groups@in@Brazi h@@@ responSble@for@paying@the@necessary@compensation. h@agents@(Lavor@et@al ,@2004), There@is@a@movement@for@giving@the@censes,@however,@there@has. Ⅰ. Ⅰ. ・. been@some@concern@regarding@th@@ point,@Snce@licenSng@could@take@the@@ interest@and@commiment@away@from@the districts@where@they@serve@as@the@agents@and@could@ ad@them@to@become@ Ⅰ. Ⅰ. ss@responsive@to@the@need@of@reSdents ,. The@he3th@agents@are@p3d@by@the@state@government@and@the@se cti n@of@the@commuHty@he3th@agents@@@ carried Ⅰ. out@by@the@muHci. al@government. ・. 4.2.7.2 The Fam Ⅱy Health Program The@Fami the@Commu. Health@Program@(PSF)@was@launched@@@. Ⅰ. Ⅰ. (PSF). ty@Health@Agent@Program. 1994 , b ℡Ⅰ i g@on@the@strength@of@its@1991@predecessor ,. , PSF@was@concei. curative@and@hospial-centered@health@care@ inter-section3@ integra on@and@baSc@hea Ⅰ. Ⅰ. ed@as@a@li chpin@@@ the@transformation@of@the@mai. system@toward@one@that@@@. oⅡ. ented@toward@prevention,@. ・. Ⅰ. Ⅰ. tions@in@a@proactive@manne. Ⅱ. eventu3ly@these@serVces@are@expected. to@serve@as@an@entry@point@to@highervC@ services, Under@the@PSF,@a@team@conSsts@of@community@hea Ⅰ. prac. Ⅰ. ce@or@family@hea. Ⅰ. h@physiCan,@a@nurse,@one@or@two@auxili. Ⅰ. an@popula. Ⅰ. Ⅰ. h@agents,@a. ry@nurses,@and@part-time@denti. team@@@ asSgned@the@responSbiliy@of@proVding@care@to@a@pre-defined@set@of@fam nearly@one-fourth@of@the@entire@BraZ. promotion,. h@care@(Lavor@et@8 , ,@2004) The@program@seeks@to@devCop@high@qu3iy. primary@servi es@that@serve@vulnerab popu gener3@. Ⅰ. Ⅰ. ies. ・. Na. Ⅰ. ona. Ⅰ. ts, Each. y,@the@PSF@covers. It@@@one@of@the@largest@federally-funded@health@programs,. on ,. spending@US$380@million , Under@current@government@plans , in@the@near@future@the@PSF@will@provide@coverage@to 50@percent@of@the@BraZlian@popu. Ⅰ. Lon. 4.3@ Brazilian@ Health@Administration 4.3.1@ Role@of@Each@Level@of@the@Health@Ministry@of@the@SUS Hea. Ⅰ. h@ care@po. cy@must@comply@with@the@fo. Ⅰ. poli ies@and@planning;@financC@. coordina. Ⅰ. owing@four@m3or@admini. Ⅰ. oH@ regu. Ⅰ. Ⅰ. oⅠ. tra. Ⅰ. ve@func. onS@. Ⅰ. formulation@of. control@and@ev3uation@of@the@SUS;@and@direct@assi. tance. for@health@services@(De@Souza,@2002) 、 Each@m3or@functon@includes@a@series@of@sub-functions@and@administrative authority@in@the@hea. Ⅰ. h@care@sector , For@instance,@one@of@the@four@functions,@the@formu. tion@of@po Ces@and. Ⅰ. Ⅰ. planning, includes@the@diagnosis@of@the@necessity@of@public@health@as@well@as@the@identification@of@m3or@priorities and@programs@of@hea 4.3.1.l. Ⅰ. h@care@acLviies. The ⅣIinistで y 0fHealth. in B Ⅰ azil. In@gener8.@the@role@of@the@Minitry@of@Hea h@ (MS)@ @@ to@estab sh@the@strategis@of@the@heah@care@of@the Ⅰ. naton@on@the@who decentr3i. Ⅰ. and@focus@on@planning,@contro. Ⅰ. Ⅰ. ation@(De@Souza,@2002) , Moreover,@the@Mini. for@three@national@systems;@complex@medical@treatments. Other〉o Ⅰ. s. of》he. ing,@ev8ua. Ⅰ. Ⅰ. ng@and@audiing@to@check@the@process@of@the. try@of@Hea h@has@focused@on@definition@and@coordina. Ⅰ. Ⅰ. on. , public@health@laboratories , blood@dia sis Ⅰ. Ministry{f?ea h‖re》o〉egulate》he}rivatesectors, and》o,a fy》he〉egula ons Ⅰ. Ⅱ. Ⅰ.
(14) 第 10 巻第 2 号 (2005年 8 月 ). 横浜国際社会科学研究. (224). 82. pertai ing@to@both@the@SUS@and@private@health@services In@ad4tion , the@Ministry@of@Health@estaDishes@the@criteria ・. and@remuneraton@for@serVces@w@h@the@approv3@ of@the@Nation8@Council@of@Heah . Within@the@SUS,@the@Mini try Ⅰ. of@Health@has@the@task@of@identifying@the@health@care@services@at@state@and@municipal@levels@and@of@establishing@the techni 3@ mode. for@hea h@care@assistance. Ⅰ. Ⅰ. Many@responsi. ilities@are@imposed@on@the@Miistry@of@Health@@@ the@area@of@admi istration@of@the@SUS Frst , ・. the@MS@e borates@the@natinal@plan@of@the@SUS@@@regard@to@the@techni 8@ cooperat Ⅰ. and@the@feder3@ di trict Regarding@region3i. a. ・. p0iy@making@(De@Souza,@2002). Ⅰ. on@of@asSstance,@the@MS@@@. pro Ⅴ ders. n@with@states,@muni ipalities. responSb. for@fo owing@areas@of Ⅰ. Ⅰ. ,. @@Defini g@regulat@ ns,@and@the@techni 8@ instruments@for@the@imp. Operaton8. such‖s¨orm3. Ⅰ. Law. Ⅰ. mentat@ n@for@these@regu t@ nS@ for@the@SUS Ⅰ. (NOAS) and〉egu ng〉e ti ns|etween》heヾUS‖nd}Fvate《ervi e Ⅰ. Ⅰ. Ⅰ. ・. @@Pro Ⅴ di g@finanCal@cooperation@for@states@to@claLfy@the@plan@and@to@imp ment@the@p n@w@hing@the@state@he3th Ⅰ. Ⅰ. care@system. @@Provide@both@technic8@ and@financi3@cooperation@to@states,@the@feder3@ di trict@and@municipaliies,@in@order@to achieve@the@perfect@institutonal@8ms , @@Admi. istering@a@reference@system@among@states. @Control@and@ev8uate@hea The@chi. h@care@servies,@espeCally@the@competence@of@states@and@muniCpai@. Ⅰ. f@of@the@decentr8iza. Ⅰ. on@sec. Ⅰ. on@of@the@Ministry@of@Health@men. Ⅰ. s. ・. oned@at@an@interview@that@it@was. important@to@regute@the@re Lonships@between@the@SUS@and@private@health@care@providers,@Snce@many@patients Ⅰ. come@to@the@pub. Ⅰ. Ⅰ. c@hospit8@ for@advanced@treatment@under@the@SUS@. treatment@under@the@SUS@has@become@a@prob treatment@at@publ@@hospia. Ⅰ. admi. Ⅰ. , Moreover,@the@i. sue@of@payment@for@medi. 3. m@Snce@many@patients@insured@under@private@he8th@p ns@recei. e. Ⅰ. i tered@under@the@SUS@and@the@cost@of@the@@. treatment@@@ p8d@by@the@SUS. ・. Some@argue@that@the@private@i surance@compani s@have@a@duty@to@pay@the@costs@for@the@insured@even@though@the medi 8@ treatments@are@performed@at@a@publ@@ hospial , Moreover,@the@Mini. try@of@Health@defnes@and@regu. Ⅰ. tes@the@techni. al@coopera. Ⅰ. on@between@na. on3. Ⅰ. instiuLons@of@Nation8@ Blood,@Components@and@Devices@and@the@Publ@@ Health@Care@Laboratories,@and@contro and@coordinates@the@integraLon@of@highly@compli ated@hea h@care@asSstance@ (De@Souza,@2002) Furthermore, the@ro of@the@MS@is@extended@to@the@carrying@out@the@direct@control@over@the@reduc Ⅰ on@of@dispa Ⅱties@across@the Ⅰ. Ⅰ. ・. Ⅰ. country. ,. In@sum,@the@federal@government@aims@at@regulating@and@controlling@the@national@health@care@system@on@the whole. 4.3.1.2 The State Secretary ofHealth to@plan,@program@and@organize@the@regi nal@organ@ ations@and The@role@of@the@State@Secretary@of@Health@@@ CasSfication@of@the@SUS@at@the@state@levC@ (De@Souza,@2002) The@State@Secretary@@@responSb for@articu ting Ⅰ. ・. and@conso admini. Ⅰ. da ng@the@region3i. aton,@and@integration@of@the@program@in@the@states@and@for@imp. Ⅰ. te ng@regulations@wihin@the@state Ⅱ. ・. Moreover,@@@. has@responSbiiy@for@admini. Ⅰ. Ⅰ. men. ng@and. Ⅰ. te ng@the@reference Ⅱ. system@among@municipalities@and@coordinating@the@building@of@collaboration@among@the@public@medical organi. a. Ⅰ. ons@for@high. recelveassls ぬnce wihin@the@state. Ⅰ五二. Ⅰ. comp. omtheM. Ⅰ. Ⅰ. x@medi. 8@. treatments. ・. In@re tion@wih@the@Mini Ⅰ. rnls 町 ofHealthforthehlghlycomplexmedlcalc. try@of@Health,@the@state@will. 肛ethatcannotbe. ぬkencareof. ,. There@are@other@general@functions@for@the@coordination@and@regu tion@of@the@state@health@care@system States Ⅰ. ・. need@to@cooperate@with@muni ip8i@ s@over@the@techni3@ and@finanC3@matters,@as@well@as@establih@regulations,@i.
(15) The@Welfare@State@and@Health@Policy@ (Kazumi@Noguchi) Table@2@ Policy@Formulation e. "[den Ⅴ [hep 0blems 皿 d decision0 Ⅱ hep0 cyasnau0n Ⅲ pn0 iⅡ eS れテ. Tab@@ Municipal. State. Ⅰ de 「 al ト. ァ. *Identify@the@problems@and deci ion@as@national@priorities. Municipal. d. "'"p 。""'" 。 。。 穫 。 ra@r 。 so'urces. 'ReditLbution@of@financia. *Pr0m0te 山 ere 陣 0n 由 izaⅡ 0n. *Guarantee{f}roper‖loca@on of@resource. sources. Planning@of@necessary@actions and@services. 'Equality@of@financial. integ ati0nof@hepr0 町a Ⅲ ト. , C00 ぴ rah0n 皿 dincen而 esfor the 帥 en 麒 h0fthehea 皿 c打 e in甜 mu0n 皿 dfor 山 Ⅱ nn0vative hea ℡ c打 ep0 Ⅱ cy0f Ⅲ es ぬ te andmunicip団 minis ㎡ es.. andCon け aCtsWl血 pnvate. "Co0 ド ra Ⅱ onandincen廿 Vef0r h。 。 ㌔。「。 ""ロ 。 fM 。。"p,l Hea Ⅱ h. *Decision@of@clear@crite Ⅰ a@for resources di tribu on@of@federal@resources. dis ㎡ bu れ on. *Organize@the@publc@services *Oversee@the@inequ3iies. *Clear@cr@eria@for@approp Ⅱ aton. of@federal,@state@and@municipal. ・. "Bu Ⅱ d 田 eincen血 e㎡ 0rthe. 仁. n. State. ・・. *Ks ぬ bbⅡ sshⅡ .s 甘 ate 臼 ees ㎝ d re 糾 latlons. Ⅰ. *Nation3@ priorit@ s@and@criterion of 丘 n皿 cia@dis㎡ bu れ 0n. ServlCeSlfnecess ㎝Ⅳ. poliy‖reas‖nd[uni ipalii. s. 鯛 urce:De 飴 ㎎a,R R (2㏄ 2),P.42. 4@ Coordi. ati n,@Reg. Fede al. Ⅱ. *C0ordlnaⅡ onandregula. 廿. 0n0f. C00rd@na血 onaⅡ dregula. municipal@system. 「. "A"@c Ⅱ la Ⅰ 0n0fI. Ⅱ. 0n0f. Es 担 bllsh 廿@e. Ⅱ. ブ. a廿 On. COOPera. Ⅱ. 0Wofreference. *C0operateW@@hthe0tl@e munlClpaⅡⅡ eS. *Decide@the@o Ⅱ entation@of@a@. "Implementa Ⅱ on0fcen. regulations@of@SUS. re Ⅲ. 臼a. Ⅱ. 甘 al. 正. Ⅰ. Ⅰ. *Strategic@ac@ons. 0Ⅱで eference. pubic 皿 dpnvatepro. れ. onal@cases. cn0f. 鯛 urce. ㎡ dders. system. *Eval. Ev3uate@the@national@policy. ation@of@the@mu Ⅱ cipal. poli y@outcomes. outcomes. ヒ u ㏄e:De. 舖雌 , RR.(2. *Con 廿 zact,adminis 比 aate, Ⅲ c打 e. 山 e №Ⅱ 笏, R R (2 ㏄2),P.43. implementation@of@mun@ip3. esvstem. *Adminis 甘 aⅡ 0nofheal@h. c町 eunils. *Service@provided@in@the ㎝@d ヒま n@heheal case@of@lack@of@municipal professionals. 0nmechan,sm , Regulatlon⑪ devalua. Sa. *Exception@@cases. ア. SVstem. 'Ev3uate@the@implementation@of *@EvaluaLon@of@the. Ⅰ. @Strategic@areas. ' m 。。l。 lp"l. Ⅴ ders. State "Excep. 。 。,. 0n. Di ect@Ser Ⅴ ce@Pro. Ⅰ. 'Integration@of@service@nets. ,A nl 「.uね廿 Onof № 捷 「. s榛佗. 5@. Fede al. gional@reference. Ⅰ. Tab@@. n. Municipal. / e c e , 回 ssem. safesl,sfem. COOPe. ati ns,@and@Evauati. State. ア. Mun@ip3. № urce:De 飴 ㎎ a,R R (2㏄2),P.42. Tab@@. 83. Ⅱ. Ⅱ. 丁. 3@ Fi c@@ Rel ti. Federal. 'Ident@y@the@probl ms@and deciion@of@prio ty@for@the muni ip3ities. (225). ㏄ 2),P.43. addit@ n@to@supplementary@procedures@to@control@and@evaluate@the@health@care@services. , As@the@Ministry@of@Health. at@the@national@levC,@the@state@@@ responSble@for@overseCng@the@reduction@of@inequ6ity@wihin@the@states. ・. More. important , the@state@par@cipates@@@ the@p0icy@form ℡ ation@of@the@national@health@care@system@as@a@member@of@the Ⅰ. Tripartisan@Counsel@(De@Souza. , 2002). 4.3.1.3@ The@Secretary@of@Municipal@Health The@Secretary@of@MuniCp3@ Hea h@@@ responsible@for@an8yzing@the@necesSty@of@health@care@serVces@and@for Ⅰ. carrying@out@8l@plans@and@pr0ects@concerning@loc8@ with@private@health@care@providers,@and@establi. hea h@care@serVces Ⅰ. h@coordina. health@care@service@is@insufficient@for@the@needs@of@patents. Ⅰ. ・. ・. Moreover,@@@ needs@to@m3nt8n@contract. on@w@h@the@federal@government@in@case@the@pub The@most@cruCal@role@of@the@muni. Ⅰ. c. ipal@health@care. adminitration@@@ to@make@sure@that@peopin@the@muniCpality@have@proper@access@to@8l@hea h@care@ser Ⅴ ces . The Secretary@of@Muniip3@Hea h@participates@in@the@region3@ hea h@care@plan@with@the@State@Secretary@of@Health@in@a h@care@services@useful@for@reSdents@in@the@muni ip8i@es, In@the@poliy way@that@@@w@l@receive@informaLon@on@hea Ⅰ. Ⅰ. Ⅰ. Ⅰ. Ⅰ. formu % 4. Ⅰ. tion@process,@the@muniip3ities@parti ipate@in@the@Bipartisan@and@Tripartisan@Counci Ⅰ. Administrativefunctions. of》he. SUS. When@making@health@care@policy,@each@government@has@its@own@important@functions@and@focuses@is@o priorities@and@needs@of@is@reSdents@w@hin@each@sphere. , In@an@interVew@wih@the@coordinator@for@poli. of@the@State@Secretary@of@Heah@of@Ceara@mentioned@that@the@state@concentrates@on@promo Ⅰ. Ⅰ. y@speC3i. ts. ng@the@regi nali ation.
(16) (226). 84. 第 10 巻第 2 号 (2005年 8 月 ). 横浜国際社会科学研究. Table@6@ Brazilian@National@Budget@for@Health@Expenditure@in@2000 Federal. Municipal. State. Expendltu e 山ⅡⅢ 0nR$) ア. Pe. 「. capi ぬ. Per@ cap@. EXpend Ⅱ ure (如 lillionR$). Total. Expenditure (M ㎜0nRS). Expenditure@ (Million@R$)@. Pe 「 CaPl ぬ. Per capita. 20,351,[email protected]%@. 119,86@ 6,313,436@ 18.56%@. 37,18@ 7,347,[email protected]%@ 43,80@. 34,012,089@ 200,84. N0 れ h. 1,285,518@. 53.15%. 99,65. 821,830. 33.98%@. 63,70@. Northeast@. 4,582,914@. 66.94%. 95.99. 1,259,051. 18.39%. Southeast@. 8,074,371@. 51.70%@. 111,51. 2,977,387. 2,623,004@. 59.62%@. 104,47. Central@west@ 1.233,181@. 56.63%@. 105.97. Brazil. South. Source:@http://portal. saude. ・. ・. 311,096@. 12.86%@. 24,11. 2,418,444@. 187,47. 26,37. 1,004,070. 14.67%. 21,03. 6,846,035. 143,40. 19.06%. 41,12. 4,566,409. 29.24%. 63,06. 15,618,167. 215,68. 718,744. 16.34%@. 28,63@. 1,057,621@. 24.04%@. 42,12. 4,399,368@. 175,22. 536,424. 24.63%@. 46,10@. 407,964@. 18.73%@. 42,56. 2,177,569. 194,63. gov , br/saude/aplicacoes/anuario2001/recfin/Mrecfint08.cfm. ,. by@dividing@the@muni ipaii s@into@macro-region@and@mi ro-regions@and@focuses@on@spreading@the@system@of medi 3@ serVces@among@the@muni. ip3iies ,. ResponSbilities@for@finanC8@ resource@3loca. Ⅰ. on@are@wih@the@feder8@government. ・. The@state@government@has. the@authority@of@overseeing@the@a ocation@of@HTnanC3@ resources@of@muni ip3@ government. , Three@levels@of. Ⅰ. government@have@focused@on@the@ev3uaton@of@po muni. ip3@ coopera. Ⅰ. on. It@ very@Cear@that@the@muni Ⅰ. ・. Ⅰ. cy@outcomes@and@have@estab ip3@ government@@@. Ⅰ. shed@inter-state@and@inter-. in@charge@of@the@proVding@diect@healh. care@services@as@shown@in@the@table@5. 4.5@ Health@Care@Expenditures@in@Brazil 4.5.1@ Intergovernmental@Fiscal@Relations@on@Health@Care@Policy@in@Brazil. Health@care@expenditure@increased@from@R$23,581@million@in@2000@to@R$24,737@million@in@2002.@ The@federal government@expendiure@@@. about@60@percent@and@the@state@government@expendiure@conSsts@of@18@percent. Moreover,@the@muniCp3@government@expendiure@@@ 20@percent@of@the@tot3@health@expendiure, In@BraZl,@5560@muni. ip8@ governments@are@catego. Ⅱ. zed@into@two@systemS@the@BaSc@Hea. Ⅰ. h@Care@System@and. the@ComPete@Health@Care@System@based@on@the@capacity@of@their@health@care@services. Muni ip3ities@qu8ified@w@h@the@provi ion@of@hea h@care@services@recCve@the@@financi3@resources@direcy from@the@feder3@ government Th@@ diect@transfer@of@resources@from@the@federal@government@to@the@muni ip8 government@@@ ca ed@"from@fund@to@fund"After@recei ing@the@finanC3@ support@from@the@feder3@ government, ed@to@8locate@18@percent@of@the@fund@to@the@hea h@care@program 、 In@this@way,@the@feder3 muni ip3ii s@are@requ Ⅰ. Ⅰ. ・. Ⅰ. ・. Ⅰ. Ⅰ. government@can@exert@pressure@on@muni ip3@governments@on@how@to@use@the@fund , For@the@baSc@heah@care,@the total@transfer@@@ calcu ted@by@per@capia For@instance,@RS@12@per@capia@annu3ly@is@transferred@to@the@muni ip3 Ⅰ. Ⅰ. government. ・. , As@for@the@advanced@health@care@servi. es,@hospi3@ fees@are@p3d@based@on@pertinent@estimates. Muni ip3ities@categorized@as@the@baSc@health@care@p n@receive@the@transfers@from@the@government@for@baSc Ⅰ. health@services@ (De@Souza , 2002) ,. However , they@will@directly@receive@payment@for@having@specialized@services. from@the@state@government@when@the@state@government@is@categorized@as@advanced@hea capaci es Ⅰ. ・. The@muniCp8iies@catego. Ⅱ. zed@as@comp. Ⅰ. government@for@both@baSc@and@speC3ized@health@care@servi. Ⅰ. h@care@admini trative. te@health@care@plans@recCve@transfers@from@the@feder3 es@(De@Souza,@2002) ,. Although@the@state@government@weakened@its@control@over@the@financi. l@transfers@to@the@municipali es,@@@has Ⅰ. g3ned@control@over@the@monio ng@of@finanC3@spending , The@ra o@of@the@"from@fund@to@fund"@ has@been increasing@Snce@1997@and@as@of@2001@ 8most@60@percent@of@the@fund@W8s@transferred@from@the@feder8@ to@the Ⅱ. Ⅰ.
(17) The@WCfare@State@and@He8th@P0iy@ (Kazumi@Noguch). (227). 85. Tab@@ 7@ Direct@Transfer@from@the@Feder8@ Government@to@Muni i G@ Governments@(Milli n@R$) 94@. 95@. l". 2". 3". Transfer@based@on@service@provided@5,158@ 5,563@ 5,275@ 5,875@ 5,087@ 5,439@ 3,603@. 3,603@. 3,928@. 4,082. From@Fund@to@Fund@(Di ect@transfer from@the@federal@government@to@the@ _@. 8,422@. 9,366@ 10,664. 567@. 96@. 97@. 98@. 99@. 0*. 1,429@ 2,327@ 4,534@ 5,903@ 7,597@. municipal@government) Tot@@ of@transfer@of@fund. 6,130@ 6,704@ 8,202@ 9,621@ 11,342@ 11,200@ 12,025@ 13,294@ 14,746. Percentage@of@Fund@to@Fund. 9%@. Source:@Ministerio@da@Saude@. muni. i al@government,@whi. (2000) ,. p , l3.@. 21%@. 28%@. 47%@. 52%@. 67%@. 70%@. 70%@. 72%. *@(projection@from@2000@to@2003). h@shows@that@the@verti3@ re ti nsh@@ between@the@feder@@ and@muni Ⅰ. i al@government. is@very@Sgnificant@in@hea h@care@financil@relations@in@BraZl , Ⅰ. The@total@amount@of@funds@flowing@from@the@federal@government@to@the@municipalities@through@direct@transfer. ,. increased@from@R$@6,839,189@in@2000@to@R$@7,910201@in@2001.@ Moreover , the@total@amount@of@funds@transferred@to states@increased@from@R$@1,226,220@in@2000@to@R$@1,937,462@in@2001@(Ministerio@da@Saude@2000). 4.6@ Emergence@of@a@New@Actor The@non-government6@ organizations@(NGOs)@ in@BraZl@have@been@a@newly@emerging@actor@in@imp menting Ⅰ. soC3@ poli i s,@espeCally@regarding@hea. Ⅰ. h@policy. ・. The@devCopment@of@BraZ. Ⅰ. an@third@sector8@has@been@very. intense. 4.6.1@ History@of@the@Third@Sector@in@Brazil Going@back@to@the@coloni. l@era,@a organi aLons@establi hed@in@BraZl@for@social@we Ⅰ. are,@health,@educa on, Ⅰ. Ⅰ. and@leisure@have@been@supported@by@the@Catholic@Church@whi h@was@backed@by@the@Portuguese@crown@ (Landm 1997). For@instance , the@Brotherhood@of@Mercy@was@responsible@for@the@first@hospitals@and@is@still@among@the. ・. leaders@of@non-profit@initiaves@in@BraZlian@soCety Ⅰ. ・. At@the@end@of@the@19@H@century , the@first@trade@uni ns@emerged@and@the@members@of@the@trade@unions@had@the priV. Ⅰ. ge@of@recCving@medic3@. care,@as@wCl@as@assistance@in@cases@of@unemployment,@di. abiliy,@or@death Du ・. Ⅱ. ng. , professional@associations@linked@to@the@middle@class@were@established. this@time. Du. Ⅱ. ng@the@Vargas@regime,@the@centr3@ government@intervened@in@the@society@and@economy,@controlling@trade. unions@and@soCal@welfare@services admini traLvCy. government…ontroled》hese organi. The…entr3. aⅠ. ons}o. Ⅰ. tic3. and. ・. During@the@miiary@era,@the@Catholic@Church@stood@against@the@mil ary@regime@and@p yed@an@important@ro Ⅰ. Ⅰ. Ⅰ. in@the@development@of@secular@movements@of@workers,@laborers,@and@professionals,@and@residents@of@the@poor nCghborhoods@that@created@a@vast@new@fiCd@of@associa. Ⅰ. ons ,. More@recen. Ⅰ. y,@in@the@1990, s,@Cvil@organizations@in. BraZl@developed@rapidly@and@now@inCude@the@i sues@of@the@women's,@anti-racit,@envionment,@and@indigenous people. Even@in@the@health@ sector,@ NGOs@have@developed@in@. state,@ and@in@muni. interna on3@ and@loc3@ health@NGos@have@been@planned@by@important@roles@in@ser Ⅰ. have@not@had@previous@access@to@hea low@income@famii. s@has@been@p. He3th@ and@ SoC3@ Deve. Ⅰ. Ⅰ. Ⅰ. h@serv@ es. ・. Especia y,@the@HIV/AIDS@preven. nned@by@a@loc3@ NGO@. pment@ (ISDS. Ⅰ. Ⅰ. Ⅰ. ce@dCi ery@for@the@poor@who. Ⅴ Ⅰ. on@program@for@youths@from. such@as@the@Institute@of@Pr0ects@and@Inves. '@and@ BEMFAM10'. Pathfinder12'@have@been@supporting@the@finance@of@these@programs. ipa ties@in@BraZl , In@ Ceara,. . Internati nal@NGos@. Ⅰ. ga. such@ as@PoMMAR1"@. Ⅰ. ons@in and.
(18) (228). 86. 第 10巻第 2 号 (2005 年 8 月 ). 横浜国際社会科学研究. @ surance,overage|y〕 come;roups. Table・. Not@covered@by. Total. 157,681,526. Fami@@icome@Casses. %. %. private”eath}ln Covered|y. 119,032,323. 38,595,206*. 15,242,118. 14,847,647@. 97.41%. More@than@1@to@2@mi imum@wages. 24,984,005. 23,768,495@. 95.13%. 1,207,310@. 4.83%. More@than@2@to@3@minimum@wages. 20,389,819. 18,470,691@. 90.59%. 1,909,288. 9.36%. More@than@3@to@5@mi. 30,138,777. 24,532,830@. 81.40%. 31,492,454. 20,549,643@. 65.25%. 10,935,038. 34.72%. 7,772,126. 45.93%. 9,144,361. 54.03%. 10,135,732. 2,413,381@. 23.81%. 7,721,211@. 76.18%. 4,370,723 4,004,625. 4,090,130@ 2,587,380@. 93.58% 64.61%. 279,299@ 1,409,200@. 6.39% 35.19%. Up@to@1@. Ⅲ ni. p Ⅱ vatehealthplan. um@wage**. imum@wages. More@than@5@to@10@mi More@than@10@to@20@. More》han・. imum@wages Ⅲ ni. Ⅲ ni. 16,923,273. um@wages. um『ages. No@ income. Undeclared. 389,926@. 5,599,573@. 2.56%. 18.58%. *Including‥ependent‖nd[ain”olders. **@Minimum@wages@is@R$@260@(approximately@US$88)@a@month@as@of@May@2004.@ Minimum@wage@was@R$130@(approx@ ately U ㏄ 44)amonthasofAp. 血 1998. Source:@IBGE:@PNAD-National@Household@Sample@Survey-Brazil@1998. http://www. , ibge , gov , br/english/estatistica/populacao/trabalhoerendimento/pnad98/saude/sb04_l. . shtm. Table@9@ HeGth@Care@Access@by@Income@Groups Outpatient Pl ces》o《eek[edi a. Total@ Pharmacy@. cares. Totalfar. 下川Ⅱ. y. More@than@. 1@ to@2. Ⅲ nl. um@wages More@than@ 2@to@3. minimum@wages More@than@3@to@5. minimum@wages. 什 oriabo unlon. Ⅱ什. Ⅵ. ア. ア. 而. C@lnlC. 1,670,693. 1.49%. 9,265,139. 8.25%. 55.76%. 281,440. 2.82%. 38,464. 0.39%. 480,506. 4.82%. 17,052,638@ 330,[email protected]%@ 9,732,[email protected]%. 711,767. 4.17%. 163,633. 0.96%. 854,316. 5.01%. 14,135,317@. 900,834. 6.37%. 180,843. 1.28%. 946,857. 6.70%. 9,967,892@. 2.16%. 46,934,231. 246,820@ 2.48%@. 329,412@ 2.33%@. 41.79%. 5,557,914@. 7,653,649@. 54.15%. 21,660,385@ 486,[email protected]%@ 10,553,[email protected]%@ 2,727,[email protected]%@ 384,434@1,77%@ 1,855,[email protected]% 534,707・. More@than@10@to@20 mnium@wa@es. 257,029. 22,957,945. 12,785,011. Undecl. PO. 19.69%. 2,429,661. More@than@5@to@10 mnium@wages More@than@ 20 minimum@wa@ No@ i come. OutPatlent. Vate iCe % ente O Ceof cpnSe 0 O Ceof Ⅵ。. %. 22,116,312. 112,302,330. Up@to@1@minimum@wage*@. Center He8th. %. 8,016,863@. 2.01%. 118,352@ 1.48%. 8,015,657. 34.91%. 5,644,630・. 549,708・. 2,521,492・. 2,503,162. 19.58%. 5,562,839. 43.51%. 235,706. 1.84%. 380,789. 4.75%. 5,300,735. 66.12%. 74,056. 0.92%. 761,426. 9.50%. 1,420,010・. es. red. 3,078,049@. 45,465@ 1.48%@. 1,823,397@. 59.24%. 193,725. 6.29%. 11,620. 0.38%. 190,882. 6.20%. 2,㎝8,230. 80,941 3.06%. 713,611. 26.95%. 793,173. 29.95%. 32,229. 1.22%. 233,732. 8.83%. Source:@PNAD-National@Household@Sample@Survey-Brazil@1998. *Minimum@wages@is@R$@260@(approximately@US$88)@a@month@as@of@May@2004.@ Minimum@wage@was@R$130@(approximately@US$44). amon. 山 asofAp. Ⅲ 1998. 4.7@ Impact@of@the@Health@Reform. , Inequality@of@Access@of@Health@Service@in@Brazil. Only@approximately@20@percent@of@the@tot3@ popu. Ⅰ. Ⅰ. on@@@ enro. Ⅰ. ed@in@private@heah@program , 13'@Moreover,@the Ⅰ. table@shows@that@most@of@the@low@income@population@seeks@medical@care@at@health@centers At@the@high@income vC,@of@the@most@people@go@to@private@medi al@offices@that@proⅤ de@high@qu6iy@medi 3@ serv@ es@for@the@@medical ・. Ⅰ. experti e , Regarding@the@qu8iy@of@medi. 3@. serVces,@the@gap@between@the@haves@and@have-nots@has@been@huge. , 14'. High(ncome“roups‖pparent tend》o|e…overed|y} Ⅱvate(nsurance『hiⅠⅠ wer( come“roups「su3 Ⅰ. Ⅰ.
(19) The@Welfare@State@and@Health@Policy@ (Kazumi@Noguchi) Tablel0. HealthCa. ァ. e. 巳く. pend. 叶u. Heath. Expenditure@Per Capita. (US$). モ sln[ ゑⅡ nAme. こ. 二. (%@of@GDP). 2001. 2001. 5.1 3.2 2.9 3.6 2.7 2.6 3.5 2.3. 4.4 4.4 3.9 1.9 3.4 2.1 1.8 2.5. on. け covered by theSUS.. ㏄ donda ぬ W. 億eauTorba. ℡ issegmen. 87. es. (%@of@GDP). Ⅰ. 舖町 ce:Madeby. Ⅰ. Private@He9th Expend Ⅱ ure. 1. 30 573 792 356 544 231 125 199. Ⅱ. canCount. Pu5@@ Heath Expend Ⅱ ure. 2001 Araentina Br Ⅱ Ch@e Colombia Mexico Peru Bolivia Guatemala. 自. (229). 村朴 Ie丘om h 坤ゾ/h ヤ mdp.o ㎎・ ・. ぬti0n 0fhigh and low incomegroupshasbecome0b. ㎡ ousphenomenon. It@appears@that@the@private@expenditures15'@of@both@Brazil@and@Argentna@are@among@the@highest@in@the@se cted Ⅰ. Latin@American@countries@and@that@the@populati insurance@than@in@other@La. Ⅰ. n@in@these@two@nations@has@been@. n@American@countries , Based@on@available@data,@Argen. spending@more@ ㌔. on@p. Ⅱ. vate. na@spent@US$1,130@per@capia,. whi h@marked@the@hihest@among@Lat@@ American@countries,@whiBraZl@spent@$@573@per@caPta@on@he8th@care Ⅰ. Conclusion. 5. A. hough@va. Ⅰ. Ⅱ. ous@issues@related@to@de bera ve@ democra Ⅰ. Ⅰ. regionali a on@of@the@health@po Ⅰ. Ⅰ. Ⅰ. c@. systems@ such@ as@hea. Ⅰ. h@ councis@ and@the. cy@have@been@raised@as@important@points@to@be@solved,@the@most@prominent. diference@between@centralized@and@decentrali ed@health@systems@is@that@at@least@3l@ciizens@are@guaranteed@for primary@he8th@care@access@by@the@1988@Constitution Although@the@health@counC. lack@the@funcLon@of@the@polii. Ⅰ. policy@making@is@nonetheless@being@provided counC. Ⅰ. , Current. , the@Brazilian@health@policy@is@fiscal centralized. Ⅰ. Ⅰ. 3@. institu ons,@a@place@for@the@dicusSon@of@hea Ⅰ. Ⅰ. h. , The@characteristics@of@Brazilian@federalism@show@that@health. do@function@from@regin@to@region ,. Although@the@clasSficat n@by@Espi g-Andersen@can@hard be@apPi d@to@anayze@soci3@ policy@@@developing countries,@it@is@benefiC8@ to@understand@that@the@diverSficaton@of@socio-econom@@ aspects@wi affect@the@formation policies@and@the@necessity@of@forming of@the@soC3@policies, Th@@ modC@ is@made@for@the@devCoped@nations'@soC3@ Ⅰ. Ⅰ. Ⅰ. the@models@which@analyze@the@social@policy@in@developing@countries@is@high expenditures@are@highest@among@Latin@American@nations,@it@is@dificu. Ⅰ. , Although@Brazil , s@private@health. to@categorize@as@a@liber8@ model , If@thi. segmentation@continues@in@BraZl,@@@ appears@that@Bra2l@may@become@the@li eral@modC@ @@ is@health@poliy As@long@as@the@inequality@of@access@to@hea h@care@servies@perSsts,@@@ @@ hard@to@ca the@BraZli n@system@as@a Ⅰ. Ⅰ. soC3ist@poliy@although@the@. 1988@Constitu. Ⅰ. on@guarantees@univers3@. healh@care@to@3l@ci@. ens ,. In@hea h@care Ⅰ. governance,@the@NGos@have@played@a@cruC@@ role@@@fillig@the@gap@of@qu3ity@of@serv@es@between@the@haves@and haves-nots@in@BraZl At@the@feder8@ level,@in@the@recent@naton3@program,@Piano@Bras@@ para@Todos@ (Plan@for ・. everyone@in@Brazil),@the@he3th@care@program@has@been@among@th@@. program. ・. The@author@of@this@paper@conducted@a@fiCd@research@in@Ceara,@BraZl@and@in@the@future@plans@to@publish@a@ study@of@a@role@of@culture@in@publ@@management@in@Ceara.
(20) 88. (230). 横浜国際社会科学研究. 第 10巻第 2 号 (2005年 8 月 ). Appendix@1@ Capacity@of@the@Brazilian@Municipalities. Appendix@2@ Municipal@Councils. ㎝笏 (2 ㏄2),P.26. Source:DeS. Source:@IBGE. , Diretoria@de@Pesquisas. , Coordenacao. de@Popula@ao@e@Indicadores@Socials , Pesquisa@de Idomag ㏄ sB ゑsi㏄ sM ㎡ cip㎡s2 ㏄ 1. Notes. 1)@See@Appendix@1. 2)@Brazilian@Real=0.39200@US@Dollar@as@of@April@22 , 2005 3)@Ceara@is@a@state@located@in@Northeastern@Brazil 4)@PAB@is@basic@package@of@services 5)SeeAppend. , where@the@author@conducted@research@for@this@case@study@in@June. , PAB-A@is@the@expanded@basic@package@of@services. , 2004. ,. 注2. 6)@Maranguape@is@a@municipality@of@Ceara , Brazil, where@the@author@conducted@research@for@this@case@study@in@June , 2004 7)@Mu Ⅰ ci 3ities@in@Ceara@receie@fund@from@the@feder3@and@state@government@to@pay@for@the@sa ry@for@commuHty@health Ⅰ. agents. ・. 8)@The@third@sectors@in@Brazil@include@associations , philanthropic , benefit@or@charity-related@organizations , nongovernmental@organizations. 9)@ISDS@was@founded@in@May. , and@foundations. , 1993@and@a@non-governmental@organization@in@Fortaleza , Ceara. improvement@of@the@health@of@population@and@focuses@on@problem@of@public@health@and@social@development. 10)@BEMFAM@@@. a@non ,government3@. ・. It@contributes@to@the ,. organiza on@that@promotes@reproducLve@rights@as@a@fundament3@ human@right , Through@health@and@educational@services@in@sexuality@and@reproductive@health , BEMFAM@uses@participatory@methods Ⅰ. and“roup‥ynamics《upported|y《pecialized‘ducational‖nd(nformative[aterials , The}artnership『ith.
図
関連したドキュメント
In the q -th row these differentials compute the homology of the quotient W/Γ with coefficients in the system of groups H q (Γ τ ). In fact, we claim that the coefficients are
The main problem upon which most of the geometric topology is based is that of classifying and comparing the various supplementary structures that can be imposed on a
Let G be a split reductive algebraic group over L. In what follows we assume that our prime number p is odd, if the root system Φ has irreducible components of type B, C or F 4, and
Our method of proof can also be used to recover the rational homotopy of L K(2) S 0 as well as the chromatic splitting conjecture at primes p > 3 [16]; we only need to use the
It is worth noting that the above proof shows also that the only non-simple Seifert bred manifolds with non-unique Seifert bration are those with trivial W{decomposition mentioned
• Informal discussion meetings shall be held with Nippon Kaiji Kyokai (NK) to exchange information and opinions regarding classification, both domestic and international affairs
静岡大学 静岡キャンパス 静岡大学 浜松キャンパス 静岡県立大学 静岡県立大学短期大学部 東海大学 清水キャンパス
In our opinion, the financial statements referred to above present fairly, in all material respects, the consolidated financial position of The Tokyo Electric Power
