Factors Associated with Recovery of Activities of Daily Living
in Elderly Pneumonia Patients
Ryohei Goto, PT, MS,
1,2Hiroki Watanabe, PT, MS,
1,2Naoki Tanaka, PT, PhD,
2Takeshige Kanamori, PT,
2and Hisako Yanagi, MD, PhD
31 Department of Medical Science and Welfare, Graduate School of Comprehensive Human Sciences,
University of Tsukuba, Tsukuba, Japan
2 Department of Rehabilitation, Tsukuba Memorial Hospital, Tsukuba, Japan
3 Department of Medical Science and Welfare, Faculty of Medicine, University of Tsukuba, Tsukuba, Japan
Background: The current study aimed to investigate factors associated with the prognosis of activities of daily living (ADL) in elderly patients with pneumonia who had undergone rehabilitation during their hospitalization.
Methods: The study included patients of age²65 years who were hospitalized due to pneumonia and had undergone rehabilitation for disuse syndrome at Tsukuba Memorial Hospital. The main outcome was measured using the functional independence measure (FIM) scores to assess ADL. The participants were divided into a high-recovery group (²80%) and a low-recovery group (<80%) based on the FIM recovery rate score. Further, factors associated with the prognosis of ADL were evaluated using multivariate logistic regression analysis. Basic characteristics, consciousness, usual mode of transportation, FIM score, grip strength, range of motion, orthostatic hypotension, exercise tolerance (6-minutes walking distance), respiratory disorder (Hugh–Jones classification), constipation, malnutrition (mini-nutritional assessment), cognitive (mini-mental state examination), depression (geriatric depression scale), balance (functional balance scale), urinary incontinence, and pressure ulcers were included as the evaluation items.
Results: Among the 51 elderly patients with pneumonia (average age« SD; 82.0 « 11.3), 34 patients were classified in the high-recovery group and 17 in the low-recovery group. In multivariate logistic regression analysis, it was revealed that the number of days from the onset until the initiation of rehabilitation (days of inactivity) and nutritional status were factors associated with a high-recovery FIM score.
Corresponding author: Hisako Yanagi, MD, PhD
Department of Medical Science and Welfare, Faculty of Medicine, University of Tsukuba, 1-1-1 Tennodai, Tsukuba, Ibaraki 305-8577, Japan
E-Mail: [email protected]
Received for publication 22 July 2014 and accepted in revised form 14 January 2015 © 2015 The Japan Primary Care Association
Conclusions: The study results suggest that days of inactivity and early management of nutritional status after hospitalization are important for elderly patients with pneumonia to return to their ADL.
Introduction
Hospitalization for acute illness is a stressful and potentially hazardous event for elderly patients.1–4 Acute illness and prolonged bed rest are associated with a significant decline in functional ability called disuse syndrome. Disuse syndrome includes symptoms that are a) musculoskeletal, b) cardiovascular and pulmonary, c) genitourinary and gastrointestinal, d) metabolic and endocrine, and e) cognitive and behav-ioral caused by inactivity, immobility, and prolonged bed rest.5 The effectiveness and feasibility of early
physical rehabilitation programs for hospitalized eld-erly patients in preventing a decline in functional ability due to disuse syndrome have been reported in a previous study,6 which indicated that early physical rehabilitation care for acutely hospitalized elderly patients could lead to functional benefits and be safely done.
Pneumonia is the third most common cause of death and is one of the most frequent reasons for the initiat-ing the Long-Term Care Insurance (LTCI) system in Japan.7Guy et al. reported that the extent and mobility outcomes of acute inpatient rehabilitation for hospital-associated deconditioning in the elderly were associ-ated with mobility from admission to rehabilitation and indicated the importance of rehabilitation in elderly patients including those with pneumonia.8 Early physical rehabilitation programs seem to be important for the elderly patient to reduce required care after pneumonia. However, it is unclear whether the prognosis of activities of daily living (ADL) for elderly patients with pneumonia is affected by the initiation time of rehabilitation. Furthermore, factors associated with the prognosis of ADL, including disuse symp-toms, in elderly patients with pneumonia have not yet been clarified.
The purpose of the current study was to investigate factors associated with the prognosis of ADL in elderly patients with disuse syndrome due to pneumonia who had undergone rehabilitation during hospitalization.
Methods
Participants
The study included patients of age²65 years who were hospitalized at the Tsukuba Memorial Hospital from August 2012 to July 2013 and had undergone a rehabilitation program for disuse syndrome due to pneumonia diagnosed by a physician. Patients who were discharged within one week, died during hospi-talization (because it is impossible to evaluate at discharge), or did not consent were excluded from the study.
All patients and their families read and signed the informed written consent. This study was conducted in accordance with the guidelines proposed in the Declaration of Helsinki, and the study protocol was reviewed and approved by the Ethics Committee of Tsukuba Memorial Hospital and the University of Tsukuba, Japan.
Measures
Each subject’s main characteristics [age, sex (male or female), living place before hospitalization (home or facility), use of the LTCI system (independent, support level, or care level), usual mode of transportation before onset (gait, wheelchair, or other), functional independence measure (FIM) score9before onset (total,
motor, and cognitive), number of days from onset until initiation of rehabilitation (days of inactivity), duration of stay, number of days from hospitalization until initiation of rehabilitation, and the A-DROP system10]
were collected from medical records.
The Japanese LTCI system consists of seven eligibility levels, including two support levels and five care levels. For support levels, the service is basically used to prevent the care level from worsening. Alternatively, care level 1 or higher means some help is required for ADL, and care level 3 or higher means total care for ambulation or clothing is required.11 The A-DROP
system is severity stratification of pneumonia modified CURB-65,12 and it comprises five items (Table 1). It
three items pertain.
An evaluation was performed for each subject within three days of the initiation of rehabilitation and no more than three days before discharge. The initiation of rehabilitation was defined as the day when instruction regarding rehabilitation was given by a physician. For evaluation, basic characteristics, consciousness, usual mode of transportation (gait, wheelchair, or other), FIM score (total, motor, and cognitive), and the following twelve items were included.
1) Muscle strength: grip strength (kg)
2) Range of motion: cervical spine, shoulder, elbow, hip, knee, and ankle
3) Orthostatic hypotension (Yes/No)
4) Exercise tolerance: 6-minute walking distance (6-MWD) test (m)13
5) Respiratory disorder: Hugh–Jones classification ranging from 1–514
6) Constipation (Yes/No)
7) Malnutrition: Mini Nutritional Assessment (MNA) ranging from 0–3015
8) Cognitive: Mini-Mental State Examination (MMSE) ranging from 0–3016
9) Depression: Geriatric Depression Scale 15 (GDS15) ranging from 0–1517
10) Balance: Functional Balance Scale (FBS) ranging from 0–5618
11) Urinary incontinence (Yes/No) 12) Pressure ulcers (Yes/No)
Functional disability was assessed using the FIM score, which can measure both physical and cognitive ability. The FIM comprises thirteen motor items and five cognitive items. The items are scored on a seven-point ordinal scale based on the amount of assistance required. The minimum score for the FIM is 18, which
indicates a low level of functioning, and the maximum score is 126, which indicates a very high level of functioning.19
Analysis
The participants were classified into two groups according to their FIM recovery rates [FIM score at discharge/FIM score before onset © 100 (%)]. The participants with a FIM recovery rate ²80% were defined as the high recovery group (high group), whereas those with a FIM recovery rate <80% were defined as the low recovery group (low group). Student’s t-test was used for quantitative variables when comparing the means of the two groups. A»2test was used to test the significance of the association between the two qualitative variables. Variables were removed if collinearity diagnostics found correlation coefficients between variables of ²0.7.20 Multivariate
logistic regression analysis (forced entry) was used to determine the factors associated with a high FIM recovery rate. The level of statistical significance was set atp < 0.05. All statistical analyses were performed on SPSS 21.0 for Windows.
Results
A total of 167 elderly patients with pneumonia were hospitalized during the study period, and of these, 72 patients underwent rehabilitation for disuse syndrome due to pneumonia. Further, of the 72 patients who underwent rehabilitation, 21 of them were excluded. A total of 51 patients were included in the study (Figure 1). The average age (« SD) of the subjects was 82.0« 11.3 years (high group: 83.2 « 7.6 years, low group: 79.6« 16.0 years) and 56.9% were female (high group: 58.8%, low group: 52.9%). Analysis of living place before hospitalization revealed that 68.6% of the patients were at home and 31.4% of the patients were in a facility. Evaluation of their LTCI system levels revealed that 29.4% of subjects were inde-pendent and 70.6% were at the care level. No subjects were at the support level. A total of 23 patients (45.1%) had been able to move on their feet and 26 patients (51%) used a wheelchair before onset. The total FIM score was 61.2« 35.6, motor FIM score was 43.8« 27.8, and cognitive FIM score was 17.3 « 9.7 Table 1. A-DROP system
Age male: 70 years or older female: 75 years or older
Dehydration BUN: 21 mg/mL or more, dehydration Respiration SpO2: 90% or less
(PaO2: 60 Torr or less)
Orientation disturbance of consciousness Pressure SBP*: 90 mmHg or less *SBP, systolic blood pressure
before onset. Days of inactivity was 4.6« 4.5 days, duration of hospital stay was 22.7« 14.4 days, and duration of hospitalization before initiating rehabilita-tion was 2.7« 1.7 days.
As shown in Table 2, days of inactivity was signifi-cantly different in the comparison between the high group and low group (high group: 3.5« 3.4 days, low group: 5.6« 5.2 days, p = 0.048). According to the A-DROP pneumonia severity index,five patients (14.7%) had severe pneumonia in the high group and five patients (29.4%) had severe pneumonia in the low group.
The variables significantly different at the initiation of rehabilitation in comparison between the two groups Figure 1. Flow diagram of the sample
Participants in the study (n=51)
Exclude (n=21)
discharged within one week (n=6) died during hospitalization (n=8) did not consent (n=7)
Undergone rehabilitation for disuse syndrome
(n=72)
Hospitalized elderly patients of pneumonia during study
period (n=167)
Table 2. Demographic and clinical characteristics of elderly pneumonia patients
participants high group low group P value (high vs low) n= 51 n= 34 n= 17 Age (Mean« SD) 82.0« 11.3 83.2« 7.6 79.6« 16.0 0.285 Sex Male n (%) 22 (43.1) 14 (41.2) 8 (47.1) 0.769 female 29 (56.9) 20 (58.8) 9 (52.9)
Living place before hospitalization
home n (%) 35 (68.6) 25 (73.5) 10 (58.8) 0.345 facility 16 (31.4) 9 (26.5) 7 (41.2) LTCI system independent n (%) 15 (29.4) 9 (26.5) 6 (35.3) 0.532 support level 0 (0.0) 0 (0.0) 0 (0.0) care level 36 (70.6) 25 (73.5) 11 (64.7) Transportation before onset
gait n (%) 23 (45.1) 18 (52.9) 5 (29.4) 0.275 wheelchair 26 (51.0) 15 (44.1) 11 (64.7)
other 2 (3.9) 1 (2.9) 1 (5.9) FIM before onset
Total (Mean« SD) 61.2« 35.6 64.9« 36.4 54.6« 29.5 0.366 Motor 43.8« 27.8 46.1« 28.2 40.4« 23.3 0.516 Cognitive 17.3« 9.7 18.7« 9.3 14.2« 9.5 0.142 Number of days
days of inactivity (Mean« SD) 4.6« 4.5 3.5« 3.4 5.6« 5.2 0.048 duration of stay 22.7« 14.4 22.5« 16.1 23.1« 8.7 0.908 before rehabilitation 2.7« 1.7 2.4« 1.4 3.0« 1.7 0.189 Rehabilitation intervation
amount (minutes per day) (Mean« SD) 51.8« 21.5 53.7« 14.7 49.8« 15.9 0.679 A-DROP
mild case n (%) 41 (80.4) 29 (85.3) 12 (70.6) 0.270 severe 10 (19.6) 5 (14.7) 5 (29.4)
LTCI, Long-Term Care Insurance; FIM, functional independence measure. days of inactivity, number of days from onset until initiation of rehabilitation; before rehabilitation: number of days from hospitalization until initiation of rehabilitation
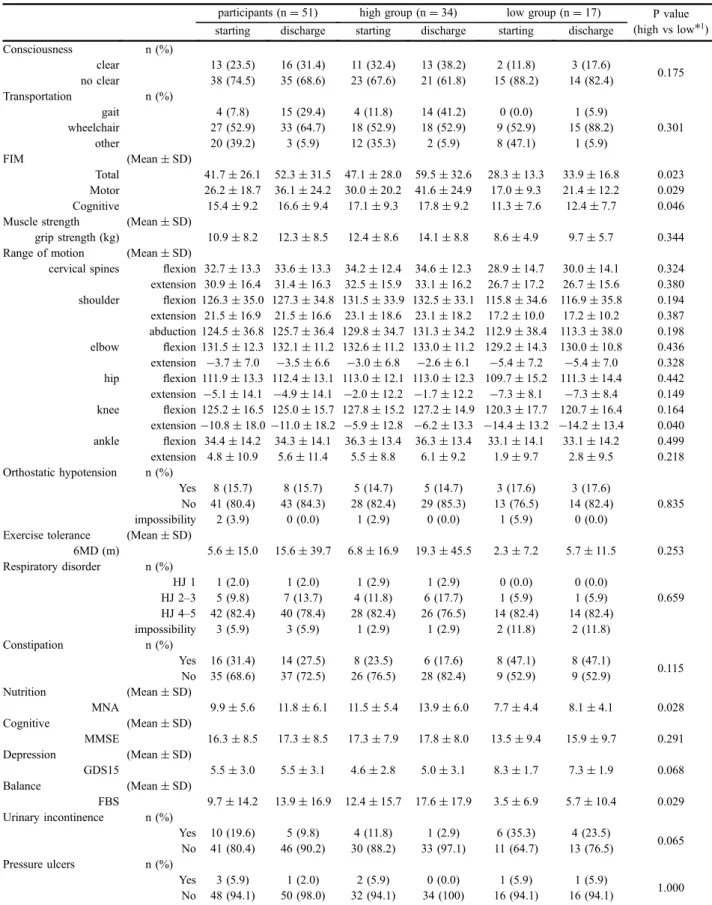
Table 3. Comparison of patients between high recovery group and low recovery group
participants (n= 51) high group (n= 34) low group (n= 17) P value (high vs low*1)
starting discharge starting discharge starting discharge Consciousness n (%) clear 13 (23.5) 16 (31.4) 11 (32.4) 13 (38.2) 2 (11.8) 3 (17.6) 0.175 no clear 38 (74.5) 35 (68.6) 23 (67.6) 21 (61.8) 15 (88.2) 14 (82.4) Transportation n (%) gait 4 (7.8) 15 (29.4) 4 (11.8) 14 (41.2) 0 (0.0) 1 (5.9) 0.301 wheelchair 27 (52.9) 33 (64.7) 18 (52.9) 18 (52.9) 9 (52.9) 15 (88.2) other 20 (39.2) 3 (5.9) 12 (35.3) 2 (5.9) 8 (47.1) 1 (5.9) FIM (Mean« SD) Total 41.7« 26.1 52.3 « 31.5 47.1 « 28.0 59.5 « 32.6 28.3« 13.3 33.9« 16.8 0.023 Motor 26.2« 18.7 36.1 « 24.2 30.0 « 20.2 41.6 « 24.9 17.0« 9.3 21.4« 12.2 0.029 Cognitive 15.4« 9.2 16.6« 9.4 17.1« 9.3 17.8« 9.2 11.3« 7.6 12.4« 7.7 0.046 Muscle strength (Mean« SD)
grip strength (kg) 10.9« 8.2 12.3« 8.5 12.4« 8.6 14.1« 8.8 8.6« 4.9 9.7« 5.7 0.344 Range of motion (Mean« SD)
cervical spines flexion 32.7 « 13.3 33.6 « 13.3 34.2 « 12.4 34.6 « 12.3 28.9« 14.7 30.0« 14.1 0.324 extension 30.9« 16.4 31.4 « 16.3 32.5 « 15.9 33.1 « 16.2 26.7« 17.2 26.7« 15.6 0.380 shoulder flexion 126.3 « 35.0 127.3 « 34.8 131.5 « 33.9 132.5 « 33.1 115.8 « 34.6 116.9 « 35.8 0.194 extension 21.5« 16.9 21.5 « 16.6 23.1 « 18.6 23.1 « 18.2 17.2« 10.0 17.2« 10.2 0.387 abduction 124.5« 36.8 125.7 « 36.4 129.8 « 34.7 131.3 « 34.2 112.9 « 38.4 113.3 « 38.0 0.198 elbow flexion 131.5 « 12.3 132.1 « 11.2 132.6 « 11.2 133.0 « 11.2 129.2 « 14.3 130.0 « 10.8 0.436 extension ¹3.7 « 7.0 ¹3.5 « 6.6 ¹3.0 « 6.8 ¹2.6 « 6.1 ¹5.4 « 7.2 ¹5.4 « 7.0 0.328 hip flexion 111.9 « 13.3 112.4 « 13.1 113.0 « 12.1 113.0 « 12.3 109.7 « 15.2 111.3 « 14.4 0.442 extension ¹5.1 « 14.1 ¹4.9 « 14.1 ¹2.0 « 12.2 ¹1.7 « 12.2 ¹7.3 « 8.1 ¹7.3 « 8.4 0.149 knee flexion 125.2 « 16.5 125.0 « 15.7 127.8 « 15.2 127.2 « 14.9 120.3 « 17.7 120.7 « 16.4 0.164 extension¹10.8 « 18.0 ¹11.0 « 18.2 ¹5.9 « 12.8 ¹6.2 « 13.3 ¹14.4 « 13.2 ¹14.2 « 13.4 0.040 ankle flexion 34.4 « 14.2 34.3 « 14.1 36.3 « 13.4 36.3 « 13.4 33.1« 14.1 33.1« 14.2 0.499 extension 4.8« 10.9 5.6« 11.4 5.5« 8.8 6.1« 9.2 1.9« 9.7 2.8« 9.5 0.218 Orthostatic hypotension n (%) Yes 8 (15.7) 8 (15.7) 5 (14.7) 5 (14.7) 3 (17.6) 3 (17.6) 0.835 No 41 (80.4) 43 (84.3) 28 (82.4) 29 (85.3) 13 (76.5) 14 (82.4) impossibility 2 (3.9) 0 (0.0) 1 (2.9) 0 (0.0) 1 (5.9) 0 (0.0) Exercise tolerance (Mean« SD)
6MD (m) 5.6« 15.0 15.6« 39.7 6.8« 16.9 19.3« 45.5 2.3« 7.2 5.7« 11.5 0.253 Respiratory disorder n (%) HJ 1 1 (2.0) 1 (2.0) 1 (2.9) 1 (2.9) 0 (0.0) 0 (0.0) 0.659 HJ 2–3 5 (9.8) 7 (13.7) 4 (11.8) 6 (17.7) 1 (5.9) 1 (5.9) HJ 4–5 42 (82.4) 40 (78.4) 28 (82.4) 26 (76.5) 14 (82.4) 14 (82.4) impossibility 3 (5.9) 3 (5.9) 1 (2.9) 1 (2.9) 2 (11.8) 2 (11.8) Constipation n (%) Yes 16 (31.4) 14 (27.5) 8 (23.5) 6 (17.6) 8 (47.1) 8 (47.1) 0.115 No 35 (68.6) 37 (72.5) 26 (76.5) 28 (82.4) 9 (52.9) 9 (52.9) Nutrition (Mean« SD) MNA 9.9« 5.6 11.8« 6.1 11.5« 5.4 13.9« 6.0 7.7« 4.4 8.1« 4.1 0.028 Cognitive (Mean« SD) MMSE 16.3« 8.5 17.3« 8.5 17.3« 7.9 17.8« 8.0 13.5« 9.4 15.9« 9.7 0.291 Depression (Mean« SD) GDS15 5.5« 3.0 5.5« 3.1 4.6« 2.8 5.0« 3.1 8.3« 1.7 7.3« 1.9 0.068 Balance (Mean« SD) FBS 9.7« 14.2 13.9« 16.9 12.4 « 15.7 17.6 « 17.9 3.5« 6.9 5.7« 10.4 0.029 Urinary incontinence n (%) Yes 10 (19.6) 5 (9.8) 4 (11.8) 1 (2.9) 6 (35.3) 4 (23.5) 0.065 No 41 (80.4) 46 (90.2) 30 (88.2) 33 (97.1) 11 (64.7) 13 (76.5) Pressure ulcers n (%) Yes 3 (5.9) 1 (2.0) 2 (5.9) 0 (0.0) 1 (5.9) 1 (5.9) 1.000 No 48 (94.1) 50 (98.0) 32 (94.1) 34 (100) 16 (94.1) 16 (94.1)
*1 high group vs low group at starting rehabilitation. FIM, functional independence measure; 6MD, 6-minutes walking distance; HJ, Hugh–Jones classification; MNA, mini nutritional assessment; MMSE, mini-mental state examination; GDS, geriatric depression scale; FBS, functional balance scale.
were as follows: the total FIM score (high group: 47.1« 28.0, low group: 28.3 « 13.3, p = 0.023), motor FIM score (high group: 30.0« 20.2, low group: 17.0« 9.3, p = 0.029), cognitive FIM score (high group: 17.1« 9.3, low group: 11.3 « 7.6, p = 0.046), knee extension range of motion (high group: ¹5.9 « 12.8, low group: ¹14.4 « 13.2, p = 0.040), MNA (high group: 11.5« 5.4, low group: 7.7 « 4.4, p = 0.028), and FBS (high group: 12.4« 15.7, low group: 3.5« 6.9, p = 0.029) (Table 3).
In multivariate logistic regression analysis, the total FIM score and the cognitive FIM score at the initiation of rehabilitation, knee extension range of motion, and FBS were removed due to collinearity with the motor FIM score at the initiation t of rehabilitation. Therefore, the motor FIM score at the initiation t of rehabilitation, days of inactivity, and MNA were established as independent variables and FIM recovery rate (²80%, <80%) was established as a dependent variable. According to the results of logistic regression analysis, days of inactivity (odds ratio: 0.72, 95% CI: 0.54–0.96) and MNA (odds ratio: 1.37, 95% CI: 1.02–1.85) were shown to be significantly associated with a high FIM recovery rate (Table 4).
Discussion
In the present study, we aimed to investigate factors associated with the prognosis of ADL (FIM score) in elderly patients with disuse syndrome due to pneumo-nia. To investigate the factors associated with good recovery, we compared a high group (FIM recovery rate²80%) and low group. The total FIM score, motor FIM score, cognitive FIM score, knee extension range of motion, nutritional status (MNA), and balance ability (FBS) were significantly different between the
two groups. Furthermore, multivariate logistic regres-sion analysis revealed that days of inactivity and nutritional status were associated with a high FIM recovery rate.
Generally, prolonged bed rest results in disuse syndrome which includes muscle weakness, joint contractures, and orthostatic hypotension. However, the effectiveness and feasibility of early physical rehabilitation have been investigated in a previous study and the importance of early rehabilitation has been reported among patients with stroke, cardiopul-monary disease, and other conditions.6,21,22The current
study also showed that initiating rehabilitation early was an important factor associated with a high probability of recovery of ADL in elderly patients with pneumonia. A previous study showed that func-tional decline two weeks before hospitalization in elderly patients influences hospital discharge and functional outcomes.23 In the current study it is
interesting to note that no significant difference was observed in the FIM score before onset between the high group and low group. In addition, severity of pneumonia at admission was not different between the two groups. Thesefindings may support the importance of early rehabilitation.
Nutrition status was reported to be important for recovery of ADL. In a previous study, low serum albumin was associated with weaker muscle strength and future decline in muscle strength in older women and men.24It has been considered that weaker muscle strength causes a reduction in activity which may lead to severe disuse syndrome. In the another study using the MNA as an assessment of nutrition it was reported that the prevalence of malnutrition was considerably different between settings (hospital: 38.7%, rehabili-Table 4. Multivariate logistic regression analysis for recovery of ADL
B SE Odds Ratio 95% CI P Independent variables
days of inactivity ¹0.33 0.15 0.72 0.54–0.96 0.024 motor FIM score 0.06 0.04 1.06 0.99–1.15 0.094 MNA 0.32 0.15 1.37 1.02–1.85 0.036 Constant ¹2.66 3.02 0.07
Adjusted variables include age and sex. days of inactivity, number of days from onset until initiation of rehabilitation; FIM, functional independence measure; MNA, mini nutritional assessment
tation: 50.5%, nursing home: 13.8%, community: 5.8%).25 The prognosis of ADL in rehabilitation was reported to be poor when there was malnutrition in the previous study.26–29 In the present study, nutritional status was already significantly different at the initiation of rehabilitation between two the groups. Therefore, it is believed that early management of nutrition may be important for elderly patients with pneumonia who have undergone rehabilitation. It has been suggested that pneumonia itself has little effect on ADL; however, ADL in elderly patients with pneumonia is reduced due to disuse syndrome. Therefore, we believe it is important to utilize early rehabilitation to prevent or treat disuse syndrome.
Limitations
The current study contains significant content suggest-ing the importance of early rehabilitation in elderly patients with pneumonia. Nevertheless, there are three limitations. (1) The sample size of the study was small, so the variables that were included as independent variables in multivariate analysis were limited. There-fore, we excluded the variables that showed collinear-ity, and included minimum variables. (2) There are no unifying criteria among physician regarding the optimal time of initiating rehabilitation after admission. Therefore, we cannot deny the possibility that patients who were expected to have a high recovery of ADL were given the instruction of rehabilitation early by a physician although there was no significant difference in the duration of hospitalization before initiating rehabilitation between the high group and low group. Therefore, we considered that this limitation had a small effect on the results. (3) Only limited conclusions can be drawn because the study was a single-center design. A multi-center study with a larger sample size is required to confirm our results.
Conclusions
The study results suggest that days of inactivity and early management of nutritional status after hospital-ization are important for elderly patients with pneumo-nia to return to their ADL by treatment including rehabilitation.
Acknowledgments
We are grateful to the rehabilitation staff and patients at Tsukuba Memorial Hospital, Tsukuba, Japan, for their support of this study. We thank Brian K. Purdue of the Medical English Communications Center, University of Tsukuba for his native English speaker revision.
Conflict of interest
There is no conflict of interest with regard to this study. References
1 Volpato S, Cavalieri M, Sioulis F, et al: Predictive value of the short physical performance battery following hospitalization in older patients. J Gerontol A Biol Sci Med Sci. 2011;66:89–96.
2 Boyd CM, Xue QL, Guralnik JM, Fried LP: Hospitalization and development of dependence in activities of daily living in a cohort of disabled older women: the Women’s Health and Aging Study 1. J Gerontol A Biol Sci Med Sci. 2005;60:888–893. 3 Covinsky KE, Palmer RM, Fortinsky RH, et al: Loss of independence in activities of daily living in older adults hospitalized with medical illness: increased vulnerability with age. J Am Geriatr Soc. 2003;51: 451–458.
4 Gill TM, Gahbauer EA, Han L, Allore HG: Factors associated with recovery of prehospital function among older persons admitted to a nursing home with disability after an acute hospitalization. J Gerontol A Biol Sci Med Sci. 2009;64:1296–1303.
5 Halar EM, Bell KR: Immobility and Inactivity: Physiological and Functional Changes, Prevention, and Treatment. In: Delisa JA, Gans BM, eds. Physical Medicine and Rehabilitation. Principles and Practice, 4th Ed, Lippincott Williams & Wilkins, Philadelphia, 2005, 1447–1467.
6 Kosse NM, Dutmer AL, Dasenbrock L, Bauer JM, Lamoth CJ: Effectiveness and feasibility of early physical rehabilitation programs for geriatric hospi-talized patients: a systematic review. BMC Geriatr. 2013;13:107.
7 The Ministry of Health, Labour and Welfare. Summary report on the 2010 Comprehensive Survey of Living Conditions of the People on Health and Welfare. Available at: http://www.mhlw.go.jp/toukei/
saikin/hw/k-tyosa/k-tyosa10/4-2.html. (In Japanese) Accessed July 1, 2014.
8 Guy N, Justo D, Lerman Y, Rabinovich A: Length and outcome of acute inpatient rehabilitation for hospital-associated deconditioning in the elderly. Hare-fuah. 2012;151:500–504.
9 Granger CV, Hamilton BB, Linacre JM, Heinemann AW, Wright BD: Performance profiles of the functional independence measure. Am J Phys Med Rehabil. 1993;72:84–89.
10 Yanagihara K, Kohno S, Matsusima T: Japanese guidelines for the management of community-acquired pneumonia. Int J Antimicrob Agents. 2001;18(Suppl 1):45–48.
11 Kamiya K, Sasou K, Fujita M, Yamada S: Predictors for increasing eligibility level among home help service users in the Japanese long-term care insurance system. Biomed Res Int. 2013;2013:374130. doi:10.1155/2013/374130.
12 Lim WS, van der Eerden MM, Laing R, et al: Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax. 2003;58:377–382.
13 Butland RJ, Pang J, Gross ER, Woodcock AA, Geddes DM: Tow-, six-, and 12-minute walking tests in respiratory disease. BMJ. 1982;284:1607–1608. 14 Fletcher CM: The clinical diagnosis of pulmonary emphysema. Proc R Soc Med. 1952;45:577–584. 15 Vellas B, Villars H, Abellan G, et al: Overview of the MNA —Its history and challenges. J Nutr Health Aging. 2006;10:456–465.
16 Folstein MF, Folstein SE, McHugh PR: “Mini-mental State”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189–198.
17 Yesavage JA, Brink TL, Rose TL, et al: Develop-ment and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. 1982;17: 37–49.
18 Berg KO: Measuring balance in the elderly: preliminary development of an instrument. Physiother Can. 1989;41:304–311.
19 Mutai H, Furukawa T, Araki K, Misawa K, Hanihara T: Factors associated with functional recov-ery and home discharge in stroke patients admitted to a
convalescent rehabilitation ward. Geriatr Gerontol Int. 2012;12:215–222.
20 Schiemanck SK, Kwakkel G, Post MW, Kappelle LJ, Prevo AJ: Predicting long-term independency in activities of daily living after middle cerebral artery stroke: does information from MRI have added predictive value compared with clinical information? Stroke. 2006;37:1050–1054.
21 Abizanda P, Leon M, Dominquez-Martin L, et al: Effects of a short-term occupational therapy interven-tion in an acute geriatric unit. A randomized clinical trial. Maturitas. 2011;69:273–278.
22 Blanc-Bisson C, Dechamps A, Gouspillou G, Dehail P, Bourdel-Marchasson I: A randomized con-trolled trial on early physiotherapy intervention versus usual care in acute care unit for elderly: potential benefits in light of dietary intakes. J Nutr Health Aging. 2008;12:395–399.
23 Isaia G, Bo M, Aimonino N, et al: Functional decline two weeks before hospitalization in an elderly population. Aging Clin Exp Res. 2010;22:352–355. 24 Schalk BW, Deeg DJ, Penninx BW, Bouter LM, Visser M: Serum albumin and muscle strength: a longitudinal study in older men and women. J Am Geriatr Soc. 2005;53:1331–1338.
25 Kaiser MJ, Bauer JM, Ramsch C, et al: Frequency of malnutrition in older adults: a multinational perspective using the Mini Nutritional Assessment. J Am Geriatr Soc. 2010;58:1734–1738.
26 Wakabayashi H, Sashika H: Malnutrition is associated with poor rehabilitation outcome in elderly inpatients with hospital-associated deconditioning a prospective cohort study. J Rehabil Med. 2014;46: 277–282.
27 Anker SD, John M, Pedersen PU, et al: ESPEN Guidelines on Enteral Nutrition: Cardiology and pulmonology. Clin Nutr. 2006;25:311–318.
28 Davis JP, Wong AA, Schluter PJ, Henderson RD, O’Sullivan JD, Read SJ: Impact of premorbid under-nutrition on outcome in stroke patients. Stroke. 2004; 35:1930–1934.
29 FOOD Trial Collaboration: Poor nutritional status on admission predicts poor outcomes after stroke: observational data from the FOOD trial. Stroke. 2003; 34:1450–1456.