【原著】孤立性腸骨動脈瘤に対する血管内治療
6
0
0
全文
(2) 74. 日血外会誌 14巻 2 号 Table 1 Clinical characteristics. 視下の結紮を行い動脈瘤内の血流を消失させた.さら に,中枢側からのe n d o l e a k が見られる 1 例では,. Characteristics. endoleak部のコイル塞栓術を追加した.最後に大腿−大. No. of patient. Total patient. 腿動脈バイパス術を追加し患側の下肢血流を確保した. %. 11. 100. 11. 100. 0. 0. Sex. (Figs. 1B,4A,B) .内腸骨動脈瘤に対しては,まず瘤. Male. 末梢の分枝のコイル塞栓術を行い,造影にて末梢への. Female. flowの消失を確認後,瘤の起始部のコイル塞栓術を施行. Age (y). 76.5앐4.4. した (Figs. 1C,3A,B,5A,B) .SGは,Spiral Z stentに. Rupture. 1. 9.1. UBE woven graft (宇部興産社製) を被覆した自作のtapered. Preoperative complication. type graftまたはPassager stent(Boston Scientific社製)を. Malignancy. 3. 27.3. 用いた.閉塞用コイルはCook社製ステンレスコイル. Previous cardiac operation. 3. 27.3. Previous abdominal operation. 3. 27.3. (0.035 inch),またはBoston Scientific社製プラチナコイ ル (0.035または0.016 inch) を使用した.SG挿入用シース は18∼22 Fr Cook社製あるいはメディキット社製のもの. Cerebral infarction. 1. 9.1. Chronic respiratory failure (HOT). 1. 9.1. HOT: home oxygen therapy.. を使用し,コイルの挿入は5 Frのカテーテルを使用し た.SG留置に関する除外項目としては,アプローチ血 管に閉塞や高度狭窄あるいは著明な屈曲・蛇行を認め. 認めた症例もなかった.3∼6 カ月ごとに施行した経過. た症例とした.. 観察のCTでは,endoleakやSGのmigration等の所見は認 めなかった.左総腸骨動脈瘤に対して患側のSG留置術. 結 果. を施行した症例において,術後 2 カ月目に血栓による. 手術死亡および遠隔期死亡例はなかった.破裂性右. SG閉塞を認め,緊急大腿−大腿動脈バイパス術を施行. 内腸骨動脈瘤に対し,緊急コイル塞栓術を施行した症. したが,その後の経過は良好であった.CTによる術後. 例においても,後腹膜血腫は次第に消退し,経過は良. の経過観察では,いずれの症例も瘤径は軽度縮小∼不. 好であった.手術時に開腹手術へ移行した症例はな. 変であり,瘤の拡大を認めた症例はなかった.また,. く,片側の内腸骨動脈閉塞に伴う下部消化管の虚血を. 術後に動脈瘤破裂をきたした症例もなかった (平均観察. Technique 1 Fig. 1. Technique 2. Technique 3. A Schematic figure of the operation. A: Technique 1. SG was placed in the ipsilateral iliac artery. B: Technique 2. SG (aortouniiliac endografting) was inserted distally from the abdominal aorta into the contralateral iliac artery in conjunction with femoro-femoral bypass. C: Technique 3. Internal iliac artery coil embolization was performed. SG: stent graft.. 12. B. C.
(3) 2005年 4 月. Fig. 2. 75. 迫ほか:孤立性腸骨動脈瘤に対する血管内治療. A: Case 3. Preoperative angiography. B: Case 3. Postoperative angiography (Fig. 1A).. A. B. Fig. 3. A: Case 6. Preoperative angiography. B: Case 6. Postoperative angiography (Fig. 1A, C).. A. B. Fig. 4. A: Case 5. Preoperative angiography. B: Case 5. Postoperative angiography (Fig. 1B).. A. B. 13.
(4) 76. Fig. 5. 日血外会誌 14巻 2 号. A: Case 9. Preoperative angiography. B: Case 9. Postoperative angiography (Fig. 1C).. A. 期間:27.0 앐 11.8カ月) (Table 2).. B. 点は,proximal landing zoneが十分に確保できない症例が 少なくない点であるが,このような症例に対しては下部. 考 察. 大動脈から対側総腸骨動脈へのSG留置(aortouniiliac. 孤立性腸骨動脈瘤は比較的稀な疾患であり,腹部大. endografting) を行い,大腿−大腿動脈バイパス術とコイ. 動脈瘤の 1∼6%と報告されている1∼6).しかしながら臨. ル塞栓術を組み合わせ瘤内の血流を途絶させることで. 床症状に乏しく,破裂により発見される例も多く,救. 対応した.しかしながら本法は下腸管膜動脈を温存す. 命率は満足のいくものではない4,5).自験例でも11例中. るような位置にグラフトを留置するため中枢側landing. 5 例は無症状で,検診等で発見されており,1 例は破裂. zoneがとりにくいこと,および中枢側 (abdominal aorta). 時に発見されたものであった.手術方法は開腹による. の径が大きくなることからendoleakが起きやすいと考. 1∼6). ,近年で. えられる.したがってlanding zoneが確保できる症例に. はSGによる治療も報告されつつある7∼9).SG留置術は. おいては,できるだけ患側(動脈瘤側)の総腸骨動脈か. 開腹を必要とせず,低侵襲であり,早期離床が可能な. ら外腸骨動脈にかけてSGを留置するのが望ましいと考. 瘤切除,人工血管置換術が一般的であるが. ことから有用な方法と考えられる.自験例では,平均. えられ(Fig. 1A),患側(動脈瘤側)への留置が困難な. 年齢76.5歳と高齢者が多く,担癌患者や開腹手術,心臓. (landing zoneが確保しにくい) 場合のみ本術式を施行する. 手術の既往を持つ患者がおのおの27.3%と高率で,慢性. こととしている (Fig. 1B) .自験例では遠隔期のendoleak. 呼吸不全の患者も認めたが,いずれも早期離床が可能. 出現は認めていないが,endoleak出現の際には,coil. であった.. embolizationやSG追加などが必要になると考える.. 腹部大動脈瘤に対するSG留置術の臨床報告例は多. また大腿−大腿動脈バイパス術を行うのであれば,. く,最近では良好な成績の報告も見られるが,周術期. 経後腹膜経路によるbypass血行再建と比較すると,手術. および遠隔期の合併症も報告されており,開腹手術の. 侵襲では遜色ないと思われ,遠隔期成績を考慮すると. 良好な成績から考えると,適応などに関して未だ議論. 経後腹膜経路によるbypass血行再建の方が長期安定性を. 10). の残るところである .一方,孤立性腸骨動脈瘤は頻. 期待できるため,症例に応じた適応を考慮する必要が. 度が少なく,SG留置術の臨床報告例は少ない.しかし. ある.自験例では 2 例中の 1 例は慢性呼吸不全の患者. ながら我々は,腹部大動脈瘤に比べ瘤径も小さく,また. で,また 2 例とも高齢者であったため,全身麻酔の必. アプローチの距離が短いために手技が比較的容易である. 要がない本法(意識下硬膜外麻酔にて施行)は低侵襲化. ことから,総腸骨動脈瘤に対しても積極的にSG留置術. に寄与できる術式と考えられた.. を行ってきた.総腸骨動脈瘤に対するSG留置術の問題. 全11例中,術後にendoleakやmigrationを認めた症例は. 14.
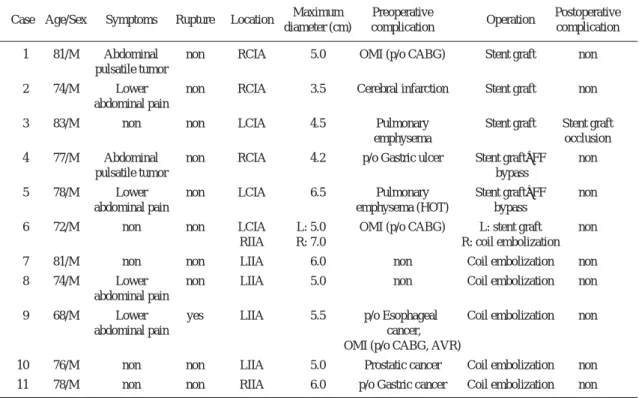
(5) 2005年 4 月. 77. 迫ほか:孤立性腸骨動脈瘤に対する血管内治療 Table 2 Summary of isolated iliac artery aneurysm. Case Age/Sex. Symptoms. Rupture. Location. Maximum diameter (cm). Preoperative complication. Operation. Postoperative complication. 1. 81/M. Abdominal pulsatile tumor. non. RCIA. 5.0. OMI (p/o CABG). Stent graft. non. 2. 74/M. Lower abdominal pain. non. RCIA. 3.5. Cerebral infarction. Stent graft. non. 3. 83/M. non. non. LCIA. 4.5. Pulmonary emphysema. Stent graft. Stent graft occlusion. 4. 77/M. Abdominal pulsatile tumor. non. RCIA. 4.2. p/o Gastric ulcer. Stent graft+FF bypass. non. 5. 78/M. Lower abdominal pain. non. LCIA. 6.5. Pulmonary emphysema (HOT). Stent graft+FF bypass. non. 6. 72/M. non. non. LCIA RIIA. L: 5.0 R: 7.0. OMI (p/o CABG). L: stent graft R: coil embolization. non. 7. 81/M. non. non. LIIA. 6.0. non. Coil embolization. non. 8. 74/M. Lower abdominal pain. non. LIIA. 5.0. non. Coil embolization. non. 9. 68/M. Lower abdominal pain. yes. LIIA. 5.5. p/o Esophageal Coil embolization cancer, OMI (p/o CABG, AVR). non. 10. 76/M. non. non. LIIA. 5.0. Prostatic cancer. Coil embolization. non. 11. 78/M. non. non. RIIA. 6.0. p/o Gastric cancer. Coil embolization. non. CIA: common iliac artery, IIA: internal iliac artery, R: right, L: left, FF: femorofemoral, p/o: post operation, CABG: coronary artery bypass grafting, HOT: home oxygen therapy, AVR: aortic valve replacement.. なかった.SG留置を行った 1 例で,術後 2 カ月目に血. 例に対する治療法に関しては,さらなる検討が必要と. 栓によるグラフト閉塞を認め,大腿−大腿動脈バイパ. 思われる.. ス術を必要とした.CT,腹部X-P上は明らかなグラフ. 孤立性腸骨動脈瘤を開腹手術にて治療する際には,. トの屈曲や末梢側遊走は認めなかった.ただし本症例は. 腹部大動脈まで人工血管で置換すべきか否か議論の分. landing zoneが短く,術中SG 1 本留置後中枢側endoleak. かれるところである.しかし,腸骨動脈瘤に対して血. を認めたため,中枢側にSGを 1 本追加挿入しendoleak. 管内治療を行った症例では,仮に残存腹部大動脈に瘤. を消失させた症例であった.その後のCT follow-up上は. 化を認めても開腹術や末梢吻合が容易であり,その点. endoleak出現を認めなかったが,2 本のSGを連結してい. においても本治療法の有用性は大きいと考える.. たため,グラフト内に血栓を生じやすかった可能性が. 結 語. 考えられた. 片側内腸骨動脈を閉塞させる点に関しては,原則と. 孤立性腸骨動脈瘤に対する血管内治療11例を経験し. して,術前に血管造影検査を行い,下腸間膜動脈およ. た.術後にSG内の血栓閉塞を認めた 1 例を除き,endoleak. び対側内腸骨動脈の開存を確認することとしている.. や瘤拡大,破裂等の合併症を認めず,良好な治療成績. 今回の症例においては,両側腸骨動脈瘤 (右内腸骨動脈. が得られた.低侵襲で,早期回復の可能な本治療法. 瘤,左総腸骨動脈瘤)1 例を認めたが,一側内腸骨動脈. は,今後,孤立性腸骨動脈瘤に対する有効な治療法に. は温存できており,両側内腸骨動脈を閉塞した症例は. なり得ると考えられた.. なく,術後の腸管虚血や臀筋虚血を認めた症例はな かった.両側内腸骨動脈瘤あるいは下腸間膜動脈閉塞. 15.
(6) 78. 日血外会誌 14巻 2 号. 文 献. の検討を含めて−.日血外会誌,12:663-667, 2003.. 1) 牧野信也,吉津 博,鳥羽信郎,他:孤立性腸骨動脈. 7) Sanchez, L. A., Patel, A. V., Ohki, T, et al.: Midterm expe-. 瘤手術症例の検討.日血外会誌,4:71-76,1995.. rience with the endovascular treatment of isolated iliac. 2) 佐久田斉,玉城 守,松原 忍,他:孤立性腸骨動脈. aneurysms. J. Vasc. Surg., 30: 907-914, 1999.. 瘤手術例の検討.日血外会誌,8:729-736,1999.. 8) Parsons, R. E., Marin, M. L., Veith, F. J., et al.: Midterm. 3) 辻 和宏,斉藤 誠,三谷英信:孤立性腸骨動脈瘤13. results of endovascular stented grafts for the treatment of. 例の検討.日血外会誌,11:575-579,2002.. isolated iliac artery aneurysms. J. Vasc. Surg., 30: 915-. 4) 戸部道雄,近藤治郎,井元清隆,他:破裂性孤立性腸骨. 921, 1999.. 動脈瘤の治療成績.日心外会誌,30:118-121,2001.. 9) Ricci, M. A., Najarian, K. and Healey, C. T.: Successful. 5) 大田 治,我部 敦,平良博史,他:水腎症・S状結. endovascular treatment of a ruptured internal iliac aneu-. 腸瘻を合併した孤立性内腸骨動脈瘤破裂の 1 治験例.. rysm. J. Vasc. Surg., 35: 1274-1276, 2002.. 日血外会誌,7:841-844,1998.. 10) 高橋昌一,高谷俊一,一関一行,他:腹部大動脈瘤に. 6) 高橋宏明,杉本貴樹,三村剛史,他:孤立性内腸骨動. 対するステントグラフト治療の初期および中期成績.. 脈瘤に対して瘤縫縮術を施行した 2 例−本邦報告例. 日心外会誌,32:224-229,2003.. Endovascular Treatment for Solitary Iliac Aneurysm Shiro Hazama1, Ichiro Sakamoto2, Shiro Yamachika1, Manabu Noguchi1, Tsuneo Ariyoshi1, Hideaki Takai1, Tomohiro Odate1, Seiji Matsukuma1 and Kiyoyuki Eishi1 1 Department of Cardiovascular Surgery, Nagasaki University School of Medicine 2 Department of Radiology, Nagasaki University School of Medicine Key words: Solitary iliac aneurysm, Endovascular treatment, Stent graft. Solitary iliac aneurysms were treated by endovascular therapy in 11 patients. All were men, with the average age being 76.5 앐 4.4 years. The site of the aneurysm was the common iliac artery in 5 patients, the internal iliac artery in 5 patients, and the common and internal iliac arteries in 1 patient. The aneurysm had ruptured in 1 patient, but not in the other 10 patients. In terms of surgical management, a stent graft (SG) was placed in the ipsilateral iliac artery in 3 patients; an SG (aortouniiliac endografting) was inserted distally from the abdominal aorta into the contralateral iliac artery in conjunction with femoro-femoral bypass in 3 patients; and internal iliac artery coil embolization was performed in 5 patients. No postoperative deaths occurred. In 1 patient who underwent stenting of the ipsilateral artery, thrombosis resulted in SG occlusion 2 months after surgery, and femoro-femoral bypass was consequently performed. In the other patients, the postoperative course was favorable, with no complications and neither endoleak nor SG migration being demonstrated on follow-up examination. Endovascular therapy appears to be an effective and minimally invasive technique for solitary iliac aneurysm. (Jpn. J. Vasc. Surg., 14: 73-78, 2005). 16.
(7)
図


関連したドキュメント
We also describe applications of this theorem in the study of the distribution of the signs in elliptic nets and generating elliptic nets using the denominators of the
В данной работе приводится алгоритм решения обратной динамической задачи сейсмики в частотной области для горизонтально-слоистой среды
We present sufficient conditions for the existence of solutions to Neu- mann and periodic boundary-value problems for some class of quasilinear ordinary differential equations.. We
In Section 13, we discuss flagged Schur polynomials, vexillary and dominant permutations, and give a simple formula for the polynomials D w , for 312-avoiding permutations.. In
Analogs of this theorem were proved by Roitberg for nonregular elliptic boundary- value problems and for general elliptic systems of differential equations, the mod- ified scale of
Then it follows immediately from a suitable version of “Hensel’s Lemma” [cf., e.g., the argument of [4], Lemma 2.1] that S may be obtained, as the notation suggests, as the m A
Definition An embeddable tiled surface is a tiled surface which is actually achieved as the graph of singular leaves of some embedded orientable surface with closed braid
Correspondingly, the limiting sequence of metric spaces has a surpris- ingly simple description as a collection of random real trees (given below) in which certain pairs of
