はじめに 外傷急性期における凝固障害は大量出血の原因 となり,重症外傷患者の予後を悪化させる1)︲5). 外傷急性期の凝固障害は,組織損傷と組織低灌流 (ショック)を原因とした消費性凝固障害と線溶 亢進が主体の線溶亢進型 DIC(disseminated intra-vascular coagulation,以下 DIC)である1),6)︲9).
外傷急性期において,フィブリノゲン(fibrino-重症外傷患者における搬入時の D︲dimer 高値は
フィブリノゲン値に関係なく予後不良を示唆する
北海道大学病院先進急性期医療センター1)・東北大学大学院医学系研究科外科病態学講座救急医学分野2) 独立行政法人国立国際医療研究センター救急科3)・防衛医科大学校防衛医学研究センター外傷研究部門4) 慶應義塾大学医学部救急医学5)・大阪大学大学院医学系研究科救急医学6) 地方独立行政法人りんくう総合医療センター大阪府泉州救命救急センター7)・近畿大学医学部附属病院救命救急センター8) 横浜市立大学大学院医学研究科救急医学9)・福岡大学医学部救命救急医学講座10)・東京女子医科大学救急医学11) 深谷赤十字病院12)・独立行政法人国立病院機構災害医療センター救命救急センター13) 東京医科歯科大学大学院救急災害医学分野14)・日本医科大学大学院医学研究科外科系救急医学分野15) 久留米大学医学部救急医学講座16)・順天堂大学医学部附属浦安病院救急診療科17)早 川 峰 司
1)前 川 邦 彦
1)久志本 成樹
2)萩 原 章 嘉
3)齋 藤 大 蔵
4)佐々木 淳一
5)小 倉 裕 司
6)松 岡 哲 也
7)植 嶋 利 文
8)森 村 尚 登
9)石 倉 宏 恭
10)武 田 宗 和
11)金 子 直 之
12)加 藤 宏
13)大 友 康 裕
14)横 田 裕 行
15)坂 本 照 夫
16)田 中 裕
17)白 石 淳
14)工 藤 大 介
2)金 村 剛 宗
3)渋 沢 崇 行
4)萩 原 靖
6)古郡 慎太郎
8)仲 村 佳 彦
9)村 田 希 吉
14)真 山 剛
10)矢 口 有 乃
11)金 史 英
15)高 須 修
16)西 山 和 孝
17) 目的:外傷急性期におけるフィブリノゲン(fibrinogen,以下 Fbg)低値は予後 不良を示唆する.D︲dimer は線溶亢進の指標であり外傷重症度を反映するが,予後 予測における Fbg との関係は明らかにされていない.今回,搬入時の D︲dimer 高 値が Fbg 値に関係なく予後不良を示唆する可能性を検証した.方法:Japanese Observational Study for Coagulation and Thrombolysis in Early Trauma(J︲OCTET) データベースを用いて,来院24時間以内における10単位以上の赤血球輸血,もしく は24時間以内の死亡を転帰不良と定義した.ROC 曲線を用いて,搬入時の Fbg 値 と D︲dimer 値の転帰不良に対する閾値を求め,その閾値に基づいた群分けを行い 比較した.結果:転帰不良に対する閾値は Fbg=190 mg/dL と D︲dimer=38 mg/L であった.この閾値に基づき,①D︲dimer 低値 /Fbg 高値,②D︲dimer 低値 /Fbg 低 値,③D︲dimer 高値 /Fbg 高値,④D︲dimer 高値 /Fbg 低値の ₄ 群に分けた.④群の 生存率は他の ₃ 群よりも有意に低値であった.③群の生存率は,①群および②群の 生存率よりも有意に低値であった.結語:ISS16以上の成人重症外傷においては, 搬入時の D︲dimer 高値は,Fbg 値に関係なく,予後不良の予測因子である. 索引用語:線溶,大量出血,組織損傷日本外傷学会将来計画委員会報告:J-OCTET
統計解析
すべての変数は,中央値(第 ₁︲第 ₃ 四分位点) もしくは実数(パーセント)で表示した. ₂ 群間 の比較は,Mann︲Whitney U︲test もしくはχ2 test を用いた. ₃ 群以上の比較は,Bonferroni 補正を 用いた Kruskal︲Wallis test を利用した. ₂ 群間の 単変量比較により統計学的な有意差を認めた変数 を独立変数とし,予後不良を従属変数としたス テップワイズロジスティック回帰分析(尤度比変 数増加法)による解析を行った.ロジスティック 回帰分析で統計学的な有意差を示した変数を ROC 曲線解析に投入し,予後不良に対する閾値 を Youden Index を用いて求めた.群間の生存時 間を比較するための Kaplan︲Meier 分析では log︲ rank test を用いた.すべての統計解析は,SPSS 15.0J(SPSS Inc., Chicago, IL, USA)を用いて行い, P<0.05を統計学的な有意差であるとした. 結 果 15施設が参加し,J︲OCTET データベースに重 症外傷患者796例が登録された.そのうち,164名 が予後不良群,632名が予後良好群であった.患 者背景をTable 1 に示した.予後不良群では,解 剖学的,生理学的,血液学的に予後良好群よりも 重篤であった. ロジスティック回帰分析 予後良好群,不良群の ₂ 群間で,性別,ISS, 胸部・腹部・四肢の abbreviated injury scores(以 下 AIS),revised trauma score,搬入時心拍数, 搬入時収縮期血圧,搬入時呼吸数,搬入時体温, pH,base deficit,乳酸値,すべての搬入時血液検 査登録項目で統計学的な有意差を認めた(Table 1).これらの ₂ 群間で差を認めた変数を独立変数, 複合転帰を従属変数としたステップワイズロジス ティック回帰分析を実施した(Table 2).欠損値 のため340症例が解析から除外された.Fbg,D︲ dimer のいずれも,予後不良を予測する因子とし て統計学的な有意差を示していた. D-dimer と Fbg による群分け Fbg と D︲dimer の予後不良に対する ROC 曲線 と,その結果を示した(Figure 1,Table 3).予 後不良に対する閾値は,それぞれ Fbg=190 mg/ dL と D︲dimer=38 mg/L であった.この閾値に 基づき,患者を以下の ₄ 群に分けた.①D︲dimer 低 値(<38mg/dL)/Fbg 高 値(>190mg/dL),② D︲dimer 低値/Fbg 低値(≦190mg/dL),③D︲dimer gen, 以下 Fbg)は止血血栓形成のために重要な役 割を担っている10)11).そのため,Fbg の低下は止 血機能障害や大量出血と密接に関係し,予後不良 を示唆する因子であると多くの報告で示されてい る8),12)︲17).さらには,外傷急性期の Fbg は,消費 と線溶亢進のため,その経過中に急速に低下する ことも明らかにされている6)︲8),13)14),18)︲21). 搬入時の D︲dimer 高値は組織損傷の重症度と 相関し22︲25),予後不良を示唆する所見であること が報告されている6)︲8),26).また,搬入時の D︲dimer 高値は線溶亢進の所見でもあり,大量出血と急性 期死亡を予測する因子であることが報告されてい るが6)︲8),予後予測における Fbg との関係は明ら かにされていない. 今回,我々は,搬入時の D︲dimer 高値は,Fbg 値とは関係なく,外傷急性期の凝固障害や予後不 良を予測する因子であるとの仮設を立て,検証し た. 対象と方法 この研究は,日本外傷学会倫理委員会およびす べての参加施設倫理委員会により承認されたもの である. 日本外傷学会将来計画委員会は,「外傷急性期 凝固線溶動態に関する多施設共同後向き研究」 (Japanese Observational Study for Coagulation and
Thrombolysis in Early Trauma, 以 下 J︲OCTET) を計画し,データベースの作成を行った.データ ベース作成前に,委員会は研究の目的に相応しい と思われる項目を,過去の論文報告と臨床医学的 見地から,一患者あたり117項目を選択した.こ のデータベースの対象患者は,2012年 ₁ 月~12月 に各委員施設へ入院した年齢18歳以上かつ,injury severity score(ISS)≧16の外傷症例である.心 停止,熱傷,軽微な外傷による頚髄損傷,妊娠, 肝硬変を合併している患者は除外した. 外傷急性期の凝固障害は大量出血を来たし,早 期の死亡原因となる1)︲5).しかし,頭部外傷症例 では,外傷急性期の凝固障害は大量出血とは関係 なく早期死亡を来たしうる27)28).このため,我々は, 24時間以内の10単位以上の赤血球輸血,もしくは 24時間以内の死亡を転帰不良と定義し,それ以外 を転帰良好とした.ROC 曲線解析を用いて求め た転帰不良に対する Fbg と D︲dimer の閾値に基 づき,患者を ₄ 群に分け,輸血投与量,止血処置 の頻度,生命予後を比較した.
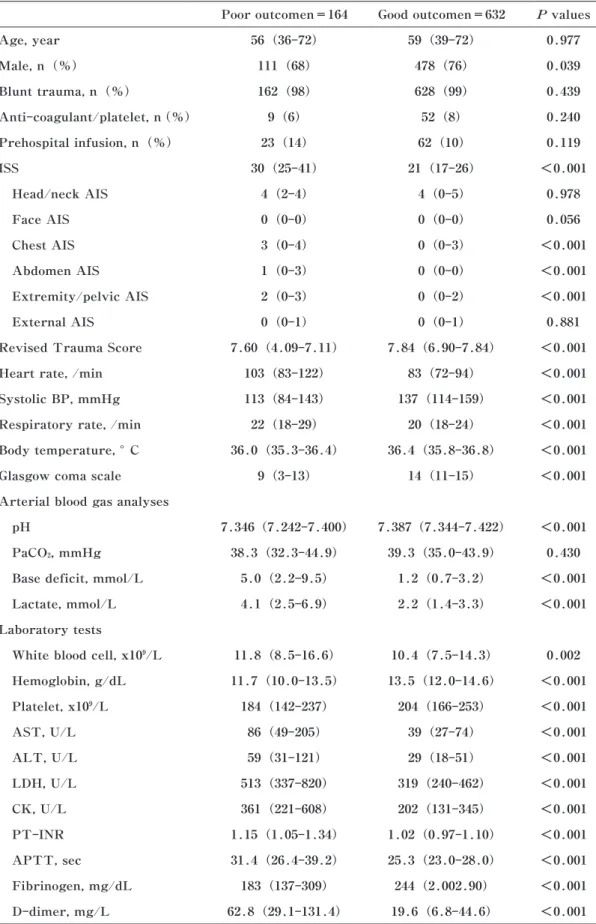
Table 1 Patient characteristics
Poor outcomen=164 Good outcomen=632 P values
Age, year 56(36-72) 59(39-72) 0.977 Male, n(%) 111(68) 478(76) 0.039 Blunt trauma, n(%) 162(98) 628(99) 0.439 Anti-coagulant/platelet, n(%) 9(6) 52(8) 0.240 Prehospital infusion, n(%) 23(14) 62(10) 0.119 ISS 30(25-41) 21(17-26) <0.001 Head/neck AIS 4(2-4) 4(0-5) 0.978 Face AIS 0(0-0) 0(0-0) 0.056 Chest AIS 3(0-4) 0(0-3) <0.001 Abdomen AIS 1(0-3) 0(0-0) <0.001 Extremity/pelvic AIS 2(0-3) 0(0-2) <0.001 External AIS 0(0-1) 0(0-1) 0.881
Revised Trauma Score 7.60(4.09-7.11) 7.84(6.90-7.84) <0.001
Heart rate, /min 103(83-122) 83(72-94) <0.001
Systolic BP, mmHg 113(84-143) 137(114-159) <0.001
Respiratory rate, /min 22(18-29) 20(18-24) <0.001
Body temperature, °C 36.0(35.3-36.4) 36.4(35.8-36.8) <0.001
Glasgow coma scale 9(3-13) 14(11-15) <0.001
Arterial blood gas analyses
pH 7.346(7.242-7.400) 7.387(7.344-7.422) <0.001
PaCO2, mmHg 38.3(32.3-44.9) 39.3(35.0-43.9) 0.430
Base deficit, mmol/L 5.0(2.2-9.5) 1.2(0.7-3.2) <0.001
Lactate, mmol/L 4.1(2.5-6.9) 2.2(1.4-3.3) <0.001
Laboratory tests
White blood cell, x109/L 11.8(8.5-16.6) 10.4(7.5-14.3) 0.002
Hemoglobin, g/dL 11.7(10.0-13.5) 13.5(12.0-14.6) <0.001 Platelet, x109/L 184(142-237) 204(166-253) <0.001 AST, U/L 86(49-205) 39(27-74) <0.001 ALT, U/L 59(31-121) 29(18-51) <0.001 LDH, U/L 513(337-820) 319(240-462) <0.001 CK, U/L 361(221-608) 202(131-345) <0.001 PT-INR 1.15(1.05-1.34) 1.02(0.97-1.10) <0.001 APTT, sec 31.4(26.4-39.2) 25.3(23.0-28.0) <0.001 Fibrinogen, mg/dL 183(137-309) 244(2.002.90) <0.001 D-dimer, mg/L 62.8(29.1-131.4) 19.6(6.8-44.6) <0.001
ISS, injury severity score;AIS, abbreviated injury score;BP, blood pressure;AST, aspartate aminotrans-ferase;ALT, alanine aminotransferase;LDH, lactate dehydrogenase;CK, creatine kinase;PT-INR, pro-thrombin time-International normalized ratio;APTT, activated partial thromboplastin time.
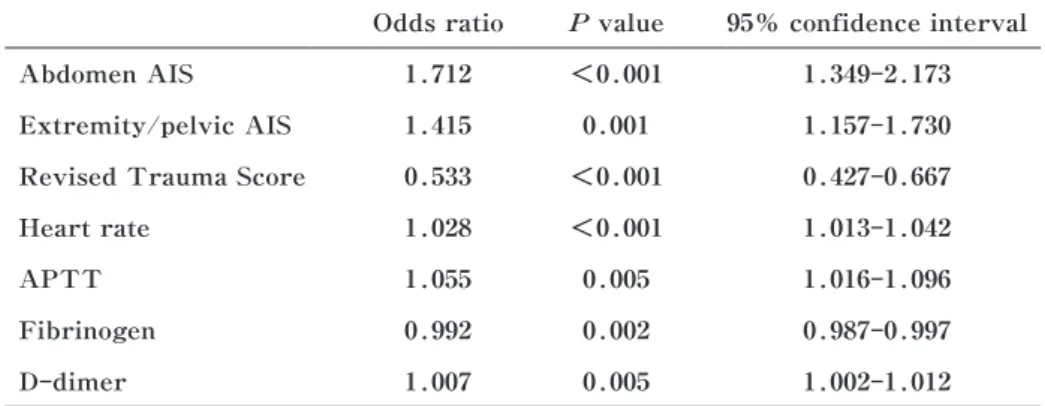
Table 2 Results of stepwise logistic regression analysis for predicting a poor outcome
Odds ratio P value 95% confidence interval
Abdomen AIS 1.712 <0.001 1.349-2.173
Extremity/pelvic AIS 1.415 0.001 1.157-1.730
Revised Trauma Score 0.533 <0.001 0.427-0.667
Heart rate 1.028 <0.001 1.013-1.042
APTT 1.055 0.005 1.016-1.096
Fibrinogen 0.992 0.002 0.987-0.997
D-dimer 1.007 0.005 1.002-1.012
AIS, abbreviated injury score;APTT, activated partial thromboplastin time
Figure 1 Receiver operating characteristic(ROC)curves for predicting a poor outcome based on fibrinogen and D-dimer levels.
Dotted line, D-dimer;Solid line, fibrinogen
Table 3 The receiver operating characteristic(ROC)curve analysis of fibrinolytic variables
AUC 95% confidence interval P value Cutoff value
lower upper
Fibrinogen 0.702 0.649 0.755 <0.001 190 mg/dL
D-dimer 0.757 0.707 0.807 <0.001 38 mg/L
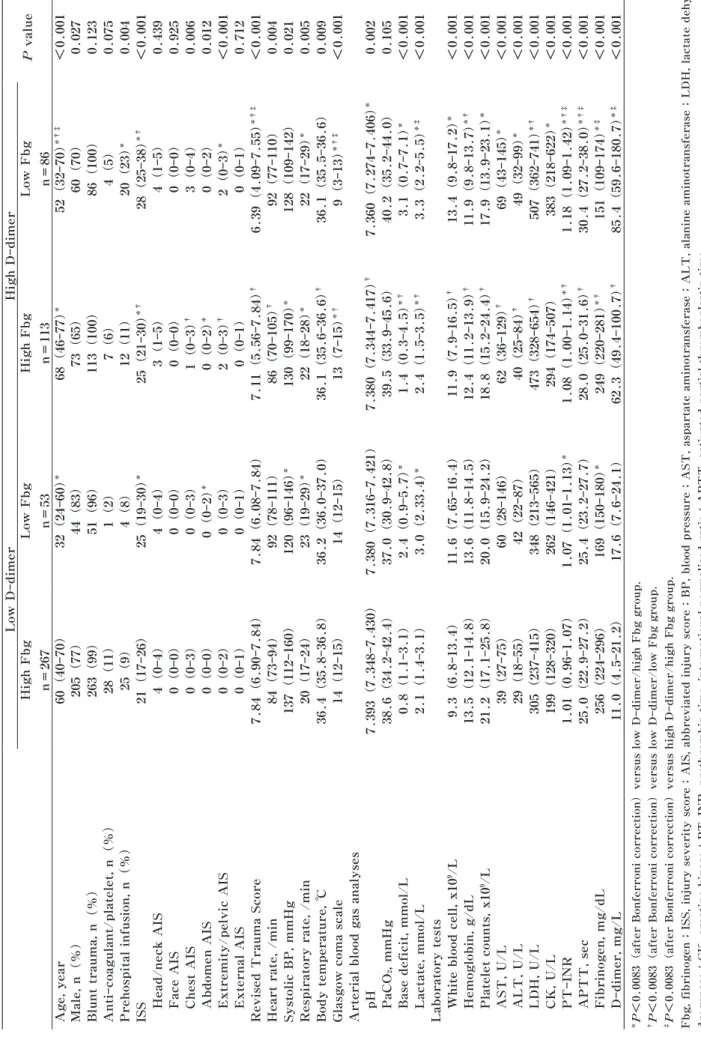
Table 4 Patient characteristics Low D-dimer High D-dimer P value High Fbg n=267 Low Fbg n=53 High Fbg n=113 Low Fbg n=86 Age, year 60(40-70) 32(24-60) * 68(46-77) * 52(32-70) *†‡ <0.001 Male, n(%) 205(77) 44(83) 73(65) 60(70) 0.027 Blunt trauma, n(%) 263(99) 51(96) 113(100) 86(100) 0.123 Anti-coagulant/platelet, n(%) 28(11) 1(2) 7(6) 4(5) 0.075 Prehospital infusion, n(%) 25(9) 4(8) 12(11) 20(23) * 0.004 ISS 21(17-26) 25(19-30) * 25(21-30) *† 28(25-38) *† <0.001 Head/neck AIS 4(0-4) 4(0-4) 3(1-5) 4(1-5) 0.439 Face AIS 0(0-0) 0(0-0) 0(0-0) 0(0-0) 0.925 Chest AIS 0(0-3) 0(0-3) 1(0-3) † 3(0-4) 0.006 Abdomen AIS 0(0-0) 0(0-2) * 0(0-2) * 0(0-2) 0.012 Extremity/pelvic AIS 0(0-2) 0(0-3) 2(0-3) † 2(0-3) * <0.001 External AIS 0(0-1) 0(0-1) 0(0-1) 0(0-1) 0.712
Revised Trauma Score
7.84(6.90-7.84) 7.84(6.08-7.84) 7.11(5.56-7.84) † 6.39(4.09-7.55) *†‡ <0.001
Heart rate, /min
84(73-94) 92(78-111) 86(70-105) † 92(77-110) 0.004 Systolic BP, mmHg 137(112-160) 120(96-146) * 130(99-170) * 128(109-142) 0.021
Respiratory rate, /min
20(17-24) 23(19-29) * 22(18-28) * 22(17-29) * 0.005 Body temperature, ℃ 36.4(35.8-36.8) 36.2(36.0-37.0) 36.1(35.6-36.6) † 36.1(35.5-36.6) 0.009
Glasgow coma scale
14(12-15) 14(12-15) 13(7-15) *† 9(3-13) *†‡ <0.001
Arterial blood gas analyses pH
7.393(7.348-7.430) 7.380(7.316-7.421) 7.380(7.344-7.417) † 7.360(7.274-7.406) * 0.002 PaCO 2 , mmHg 38.6(34.2-42.4) 37.0(30.9-42.8) 39.5(33.9-45.6) 40.2(35.2-44.0) 0.105
Base deficit, mmol/L
0.8(1.1-3.1) 2.4(0.9-5.7) * 1.4(0.3-4.5) *† 3.1(0.7-7.1) * <0.001 Lactate, mmol/L 2.1(1.4-3.1) 3.0(2.33.4) * 2.4(1.5-3.5) *† 3.3(2.2-5.5) *‡ <0.001
Laboratory tests White blood cell, x10 9/L 9.3(6.8-13.4) 11.6(7.65-16.4) 11.9(7.9-16.5) † 13.4(9.8-17.2) * <0.001 Hemoglobin, g/dL 13.5(12.1-14.8) 13.6(11.8-14.5) 12.4(11.2-13.9) † 11.9(9.8-13.7) *† <0.001 Platelet counts, x10 9/L 21.2(17.1-25.8) 20.0(15.9-24.2) 18.8(15.2-24.4) † 17.9(13.9-23.1) * <0.001 AST, U/L 39(27-75) 60(28-146) 62(36-129) † 69(43-145) * <0.001 ALT, U/L 29(18-55) 42(22-87) 40(25-84) † 49(32-99) * <0.001 LDH, U/L 305(237-415) 348(213-565) 473(328-654) † 507(362-741) *† <0.001 CK, U/L 199(128-320) 262(146-421) 294(174-507) 383(218-622) * <0.001 PT-INR 1.01(0.96-1.07) 1.07(1.01-1.13) * 1.08(1.00-1.14) *† 1.18(1.09-1.42) *†‡ <0.001 APTT, sec 25.0(22.9-27.2) 25.4(23.2-27.7) 28.0(25.0-31.6) † 30.4(27.2-38.0) *†‡ <0.001 Fibrinogen, mg/dL 256(224-296) 169(150-180) * 249(220-281) *† 151(109-174) *‡ <0.001 D-dimer, mg/L 11.0(4.5-21.2) 17.6(7.6-24.1) 62.3(49.4-100.7) † 85.4(59.6-180.7) *‡ <0.001
*P<0.0083(after Bonferroni correction)versus low D-dimer/high Fbg group. †P<0.0083(after Bonferroni correction)versus low D-dimer/low Fbg group. ‡P<0.0083(after Bonferroni correction)versus high D-dimer/high Fbg group. Fbg,
fibrinogen;ISS, injury severity score;AIS, abbreviated injury score;BP, blood pressure;AST, aspartate aminotransferase;ALT, alanine aminotransferase;LDH, lactate dehy
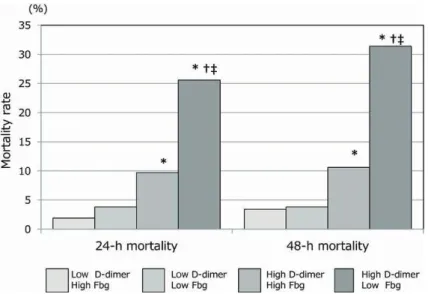
ogen activator の放出が原因であるとされる1)2)31). 一方,D︲dimer 高値で示される線溶亢進は throm-boelastometry で示される線溶亢進とは異なるも のである.Thromboelastometry で線溶亢進を指 摘された外傷患者では,D︲dimer は高値であるこ とが多いが30)32)33),D︲dimer 高値を示す外傷患者 で thromboelastometry による線溶亢進を示すとは 限らない30).D︲dimer はフィブリン形成の後の線 溶状態を反映する指標であり34),D︲dimer 高値は, 線溶亢進だけではなく凝固活性化も反映している 包括的な指標と言える. 頭部外傷患者において,搬入時の D︲dimer 高 値は予後不良と密接に関係していることが報告さ れている23)︲26).しかし,D︲dimer 高値は,頭部外 傷合併とは関係なく,すべての外傷患者で予後不 良の因子であるの報告もある6)︲8),30)32)33).本研究で は,搬入時の意識レベルが ₄ 群間で異なっていた が,頭部外傷の解剖学的な重症度(AIS)には差 を認めなかった(Table 4).頭部外傷ではなく, 循環不全などの生理学的な因子が搬入時の意識レ ベルに影響した可能性がある. フィブリン/フィブリノゲン分解産物(fibrin/fi-brinogen degradation products, 以下 FDP)と予後 高 値(≧38mg/dL)/Fbg 高 値,④D︲dimer 高 値/ Fbg 低値. ₄ 群の患者背景を Table 4 に示した. 各群の止血処置の頻度と輸血量を Table 5 に示し た.止血処置の頻度と搬入後 ₆ 時間および24時間 以内の輸血量は,①群から④群にかけて増加して いた.さらには,死亡率も①群から④群にかけて 増加していた(Figure 2).各群の Kaplan︲Meier 生存曲線を Figure 3 に示した.④群の生存率は 他の ₃ 群よりも低く(P<0.001 vs. ①群,P<0.001 vs. ②群,P=0.011 vs. ③群),③群の生存率は, ①群と②群よりも低かった(P<0.001 vs. ①群, P=0.007 vs. ②群). 考 察 本研究では,D︲dimer 高値/Fbg 低値の患者の 予後が最も不良であった.さらには,D︲dimer 高 値の患者は,搬入時に Fbg 低値を伴っていなく ても予後不良であることを明らかにした. ROTEM®な ど の thromboelastometry で 示 さ れ る線溶亢進は,外傷直後の凝固障害で中心的役割 を担っており,患者の予後不良と関連することが 多くの報告で述べられている20)21)29)30).この throm-boelastometry で示される線溶亢進は,組織低灌 流による血管内皮細胞からの tissue
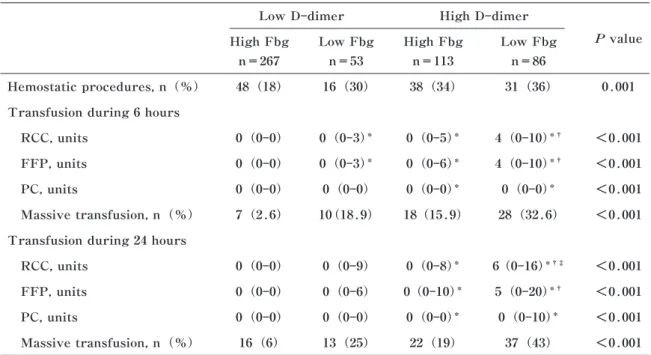
type︲plasmin-Table 5 Hemostatic procedures and transfusions
Low D-dimer High D-dimer
P value High Fbg n=267 Low Fbg n=53 High Fbg n=113 Low Fbg n=86 Hemostatic procedures, n(%) 48(18) 16(30) 38(34) 31(36) 0.001 Transfusion during 6 hours
RCC, units 0(0-0) 0(0-3)* 0(0-5)* 4(0-10)*† <0.001
FFP, units 0(0-0) 0(0-3)* 0(0-6)* 4(0-10)*† <0.001
PC, units 0(0-0) 0(0-0) 0(0-0)* 0(0-0)* <0.001
Massive transfusion, n(%) 7(2.6) 10(18.9) 18(15.9) 28(32.6) <0.001 Transfusion during 24 hours
RCC, units 0(0-0) 0(0-9) 0(0-8)* 6(0-16)*†‡ <0.001
FFP, units 0(0-0) 0(0-6) 0(0-10)* 5(0-20)*† <0.001
PC, units 0(0-0) 0(0-0) 0(0-0)* 0(0-10)* <0.001
Massive transfusion, n(%) 16(6) 13(25) 22(19) 37(43) <0.001
Massive transfusion was defined as over 10 units of red cell concentrate transfusion during the first 24 hours.
*P<0.0083(after Bonferroni correction)versus low D-dimer/high Fbg group. †P<0.0083(after Bonferroni correction)versus low D-dimer/low Fbg group. ‡P<0.0083(after Bonferroni correction)versus high D-dimer/high Fbg group.
Figure 3 Kaplan-Meier survival curves
The survival rate in the(4)high D-dimer/low fibrinogen group was lower than that in the other three groups( <0.001 vs.(1), <0.001 vs.(2), and =0.011 vs.(3)by the log-rank tests). The survival rate in the(3)high D-dimer/high fibrinogen group was lower than that in(1)and(2)groups( <0.001 and =0.007, respectively by the log-rank tests). Fbg, fibrinogen.
Low D-dimer and High D-dimer are indicated respectively<38 mg/L and≥ 38 mg/L in D-dimer levels on arrival at emergency department. Low Fbg and High Fbg are indicat-ed respectively≤ 1.9 mg/dL and>1.9 mg/dL in fibrinogen levels on arrival at emergen-cy department.
Figure 2 Mortality rate 24 and 48 hours after arrival at the emergency department The mortality rate 24 and 48 hours after arrival at the emergency department was statis-tically different among the groups(P<0.001 and<0.001, respectively). Low and high D-dimer levels were defined a<38 mg/L and≥ 38 mg/L, respectively, on arrival at the emergency department. Low and high fibrinogen levels were defined as≤ 1.9 mg/dL and>1.9 mg/dL, respectively, on arrival at the emergency department. Fbg, fibrinogen
* <0.0083(after Bonferroni correction)versus the low D-dimer/high fibrinogen group. † <0.0083(after Bonferroni correction)versus low D-dimer/low fibrinogen group. ‡ <0.0083(after Bonferroni correction)versus high D-dimer/high fibrinogen group.
7) Hayakawa M, Sawamura A, Gando S, et al:Dis-seminated intravascular coagulation at an early phase of trauma is associated with consumption co-agulopathy and excessive fibrinolysis both by plas-min and neutrophil elastase. Surgery 2011;149: 221︲230.
8) Sawamura A, Hayakawa M, Gando S, et al:Dis-seminated intravascular coagulation with a fibrino-lytic phenotype at an early phase of trauma predicts mortality. Thromb Res 2009;124:608︲613. 9) Gando S:Disseminated intravascular coagulation in
trauma patients. Semin Thromb Hemost 2001; 27:585︲592.
10) Fries D, Martini WZ:Role of fibrinogen in trauma︲ induced coagulopathy. Br J Anaesth 2010;105: 116︲121.
11) Schlimp CJ, Schochl H:The role of fibrinogen in trauma︲induced coagulopathy. Hamostaseologie 2013;34:29︲39.
12) Schochl H, Cotton B, Inaba K, et al:FIBTEM pro-vides early prediction of massive transfusion in trauma. Crit Care 2011;15:R265.
13) Kushimoto S, Shibata Y, Yamamoto Y:Implications of fibrinogenolysis in patients with closed head inju-ry. J Neurotrauma 2003;20:357︲363.
14) Chambers LA, Chow SJ, Shaffer LE:Frequency and characteristics of coagulopathy in trauma pa-tients treated with a low︲or high︲plasma︲content massive transfusion protocol. Am J Clin Pathol 2011;136:364︲370.
15) Inaba K, Karamanos E, Lustenberger T, et al:Im-pact of fibrinogen levels on outcomes after acute injury in patients requiring a massive transfusion. J Am Coll Surg 2013;216:290︲297.
16) Schochl H, Solomon C, Traintinger S, et al:Throm-boelastometric(ROTEM)findings in patients suf-fering from isolated severe traumatic brain injury. J Neurotrauma 2011;28:2033︲2041.
17) Goodnight SH, Kenoyer G, Rapaport SI, et al:Defi-brination after brain︲tissue destruction:A serious complication of head injury. N Engl J Med 1974; 290:1043︲1047.
18) Hayakawa M, Gando S, Ono S, et al:Fibrinogen level deteriorates before other haemostatic variables and massive transfusion in the early phase of severe trauma:A retrospective observational study. Semin Thromb Hemost 2014;41:35︲42.
19) Hiippala S:Replacement of massive blood loss. Vox Sang 1998;74 Suppl 2:399︲407.
20) Theusinger OM, Wanner GA, Emmert MY, et al: Hyperfibrinolysis diagnosed by rotational thrombo-elastometry(ROTEM)is associated with higher mortality in patients with severe trauma. Anesth Analg 2011;113:1003︲1012.
21) Kashuk JL, Moore EE, Sawyer M, et al:Primary fibrinolysis is integral in the pathogenesis of the acute coagulopathy of trauma. Ann Surg 2010; の関係を検討した報告がある6)︲8).D︲dimer はフィ ブリンの分解産物であるが,FDP にはフィブリ ンだけではなくフィブリノゲンの分解産物も含ま れる34).そのため,外傷急性期における線溶亢進 の指標として D︲dimer よりも FDP のほうが望ま しい可能性がある.しかし,今回の多施設共同研 究では,多くの患者で FDP が測定されておらず 検討することが不可能であった. J︲OCTET データベースには796名の重症外傷患 者が登録されたが,搬入時に Fbg や D︲dimer が 測定されていなかったため,227名の患者が ₄ 群 の比較検討から除外されている.また,受傷から 搬入時採血のタイミングは各患者間で一定ではな く,これらは本研究の検討結果に影響を与えた可 能性がある. 結 語 重症外傷患者における搬入時の D︲dimer 高値 は,Fbg 値とは関係なく早期死亡や大量輸血など の強い予測因子である.搬入時の D︲dimer に着 目することにより,より適切な止血戦略の展開が 可能となるかもしれない. すべての著者に開示すべき利益相反はない. 文 献
1) Gando S, Wada H, Thachil J:Differentiating disseminated intravascular coagulation(DIC)with the fibrinolytic phenotype from coagulopathy of trauma and acute coagulopathy of trauma︲shock (COT/ACOTS). J Thromb Haemost 2013;11: 826︲835.
2) Knight DJ, Gardiner D, Banks A, et al:Effect of synbiotic therapy on the incidence of ventilator as-sociated pneumonia in critically ill patients:a ran-domised, double︲blind, placebo︲controlled trial. Intensive Care Med 2009;35:854︲861.
3) Spahn DR, Bouillon B, Cerny V, et al:Management of bleeding and coagulopathy following major trauma:an updated European guideline. Crit Care 2013;17:R76.
4) Frith D, Brohi K:The pathophysiology of trauma︲ induced coagulopathy. Curr Opin Crit Care 2012; 18:631︲636.
5) Davenport R:Pathogenesis of acute traumatic co-agulopathy. Transfusion 2013;53 Suppl 1:23S︲ 27S.
6) Oshiro A, Yanagida Y, Gando S, et al:Hemostasis during the early stages of trauma:comparison with disseminated intravascular coagulation. Crit Care 2014;18:R61.
traumatic coagulopathy in the setting of isolated traumatic brain injury:a systematic review and meta︲analysis. Injury 2014;45:819︲824.
29) Schochl H, Frietsch T, Pavelka M, et al:Hyperfibri-nolysis after major trauma:differential diagnosis of lysis patterns and prognostic value of thrombelas-tometry. J Trauma 2009;67:125︲131.
30) Raza I, Davenport R, Rourke C, et al:The inci-dence and magnitude of fibrinolytic activation in trauma patients. J Thromb Haemost 2013;11: 307︲314.
31) Rijken DC, Lijnen HR:New insights into the molec-ular mechanisms of the fibrinolytic system. J Thromb Haemost 2009;7:4︲13.
32) Kutcher ME, Cripps MW, McCreery RC, et al:Cri-teria for empiric treatment of hyperfibrinolysis after trauma. J Trauma Acute Care Surg 2012;73:87︲ 93.
33) Ostrowski SR, Sorensen AM, Larsen CF, et al: Thrombelastography and biomarker profiles in acute coagulopathy of trauma:a prospective study. Scand J Trauma Resusc Emerg Med 2011;19:64. 34) Wada H, Sakuragawa N:Are fibrin︲related mark-ers useful for the diagnosis of thrombosis? Semin Thromb Hemost 2008;34:33︲38.
252:434︲442.
22) Hagiwara S, Oshima K, Aoki M, et al:Usefulness of fibrin degradation products and d︲dimer levels as biomarkers that reflect the severity of trauma. J Trauma Acute Care Surg 2013;74:1275︲1278. 23) Tian HL, Chen H, Wu BS, et al:D︲dimer as a
pre-dictor of progressive hemorrhagic injury in patients with traumatic brain injury:analysis of 194 cases. Neurosurg Rev 2010;33:359︲365.
24) Tong WS, Zheng P, Zeng JS, et al:Prognosis analy-sis and risk factors related to progressive intracra-nial haemorrhage in patients with acute traumatic brain injury. Brain Inj 2012;26:1136︲1142. 25) Tian HL, Chen H, Wu BS, et al:D︲dimer as a
pre-dictor of progressive hemorrhagic injury in patients with traumatic brain injury:analysis of 194 cases. Neurosurg Rev 2010;33:359︲365.
26) Yuan F, Ding J, Chen H, et al L:Predicting out-comes after traumatic brain injury:the develop-ment and validation of prognostic models based on admission characteristics. J Trauma Acute Care Surg 2012;73:137︲145.
27) Wafaisade A, Lefering R, Tjardes T, et al:Acute coagulopathy in isolated blunt traumatic brain injury. Neurocrit Care 2010;12:211︲219.
HIGH D︲DIMER LEVELS PREDICT A POOR OUTCOME IN PATIENTS WITH SEVERE TRAUMA
REGARDLESS OF FIBRINOGEN LEVELS:A RETROSPECTIVE COHORT STUDY
Mineji HAYAKAWA1), Kunihiko MAEKAWA1), Shigeki KUSHIMOTO2), Akiyoshi HAGIWARA3), Daizoh SAITOH4),
Junichi SASAKI5), Hiroshi OGURA6), Tetsuya MATSUOKA7), Toshifumi UEJIMA8), Naoto MORIMURA9),
Hiroyasu ISHIKURA10), Munekazu TAKEDA11), Naoyuki KANEKO12), Hiroshi KATO13), Yasuhiro OTOMO14),
Hiroyuki YOKOTA15), Teruo SAKAMOTO16), Hiroshi TANAKA17), Atsushi SHIRAISHI14), Daisuke KUDO2),
Takashi KANEMURA3), Takayuki SHIBUSAWA4), Yasushi HAGIWARA6), Shintaro FURUGORI8),
Yoshihiko NAKAMURA9), Kiyoshi MURATA14), Gou MAYAMA10), Arino YAGUCHI11), Shiei KIM15),
Osamu TAKASU16) and Kazutaka NISHIYAMA17)
Emergency and Critical Care Center, Hokkaido University Hospital1)
Division of Emergency and Critical Care Medicine, Tohoku University Graduate School of Medicine2)
Department of Emergency Medicine and Critical Care, National Center For Global Health and Medicine3)
Division of Traumatology, Research Institute, National Defense Medical College4)
Department of Emergency & Critical Care Medicine, School of Medicine, Keio University5)
Department of Traumatology and Acute Critical Medicine, Osaka University Graduate School of Medicine6)
Senshu Trauma and Critical Care Center, Rinku General Medical Center7)
Department of Emergency and Critical Care Medicine, Kinki University Faculty of Medicine8)
Department of Emergency Medicine, Yokohama City University Graduate School of Medicine9)
Department of Emergency and Critical Care Medicine, Faculty of Medicine, Fukuoka University10)
Department of Critical Care and Emergency Medicine, Tokyo Women's Medical University11)
Emergency and Critical Care Center, Fukaya Red Cross Hospital12)
Department of Critical Care and Traumatology, National Hospital Organization Disaster Medical Center13)
Trauma and Acute Critical Care Medical Center, Tokyo Medical and Dental University Hospital of Medicine14)
Department of Emergency & Critical Care Medicine, Nippon Medical School15)
Department of Emergency and Critical Care Medicine, Kurume University School of Medicine16)
Department of Emergency and Critical Care Medicine, Juntendo University Urayasu Hospital17)
Introduction:Elevated D︲dimer levels in trauma patients are one of indicators of hyperfibrinolysis during the early phase of trauma. We hypothesized that high D︲dimer levels would predict a poor outcome in severe trauma patients regard-less of fibrinogen levels on arrival. Methods:Patients with more than 10 units of red cell concentrate transfusion and/or death during the first 24 hours were classified with a poor outcome. Based on cut︲off values for fibrinogen and D︲dimer to differentiate the outcomes were compared. Results:In a stepwise logistic regression analysis, fibrinogen and D︲dimer levels were statistically significant predictors of a poor outcome. Optimal cut︲off values for fibrinogen and D︲dimer of 190 mg/dL and 38 mg/L, respectively. Based on these values, patients were divided into four groups:low D︲dimer/high fibrinogen, low D︲dimer/low fibrinogen, high D︲dimer/high fibrinogen, and high D︲dimer/low fibrinogen. The survival rate in the high D︲dimer/low fibrinogen group was lower than in the other three groups. Moreover, the survival rate in the high D︲dimer/ high fibrinogen group was statistically lower than that in the low D︲dimer/high fibrinogen and low D︲dimer/low fibrinogen groups. Conclusions:High D︲dimer levels on arrival are a strong predictor of poor outcome in severe trauma patients, re-gardless of fibrinogen levels.