Abstract
Purpose: To determine the impact of experimentally preformed
peri-implant crater-shaped bone defects on the evolution of in situ microbiota and development of bone defects compared to those induced over time by ligature placement only.
Methods: Implants were installed in the mandibles of eight dogs.
Standard-ized bone defects were preformed in four test animals but not in the other four control animals, prior to implant (3.3 mm × 8 mm) installation. After 2 months of healing, peri-implantitis was induced with silk ligatures in both groups for 2 months. Microbial samples were obtained from implants and teeth for analysis at three time points (qPCR), and the average depths of the bone defects were measured.
Results: At the baseline, the total marker load of periodontal-pathogenic
bacteria (TML) for teeth accounted for 5.2% (0-17.4%). After implant heal-ing, TMLs for implants and teeth were comparable (7.1% [0.3-17.4%]). The TML of both groups was 3.5%, 2 months after ligature placement. Bone defects had a mean depth of 1.84 mm at preformed defects and 1.64 mm at control sites (P > 0.05).
Conclusion: Preformed defects in the test group showed comparable
results to the control group in terms of TML, the incidence of periodontal-pathogenic bacteria, and bone defect depth.
Keywords: animal experiment, bacteria, bone defect, dental implant, polymerase chain reaction (PCR)
Introduction
Dental implants have become a valid treatment option for replacement of missing teeth, and high success rates of 97% and 75% over periods of 10 [1] and 20 [2] years, respectively, have been reported. However, biological complications can occur, and these may lead to peri-implant inflammation with concomitant inflammation of the mucosa and progressive marginal bone loss [3], also known as peri-implantitis, representing the main cause of late implant failure [4,5]. Derks et al. [6] conducted a meta-analysis showing that 22% of all implants in patients are affected by peri-implan-titis to varying degrees. The clinical symptoms of peri-implanperi-implan-titis, such as bleeding on probing of the adjacent gingiva/mucosa, pain, suppuration, increased probing depth, radiographic bone loss, and the presence of abun-dant perio-pathogen bacteria, which colonize non-shedding surfaces in biofilms, are similar to those of periodontitis affecting natural teeth [7,8]. Peri-implantitis—like periodontitis—is induced by biofilm and associated with similar microbiota [7]. Dental implants affected by peri-implantitis can be treated using different approaches. However, no specific treatment pro-tocol has been shown to be particularly advantageous, suggesting the need for further research on the pathogenesis and treatment of peri-implantitis
[8]. In 1966, Rovin et al. [9] described the use of animal models to study the pathogenesis and possible treatment of periodontitis. This research model was adopted for peri-implantitis research in the early 1990s [10,11], and still remains in common use [12]. In these models, ligatures made of cotton are placed submarginally around healthy implants, allowing biofilm to accumulate and induce inflammation-related tissue breakdown [10]. Schwarz et al. [13] reported that the most commonly encountered defect was a saucer-shaped circumferential defect (Class -Ie), with incidences of 55% and 85% in humans and animals, respectively.
Regarding the microbiome associated with peri-implantitis, an experi-mental microbiological study conducted in dogs in 1992 linked the shift from aerobic to anaerobic flora around implants to pathologic conditions [14]. Porphyromonas gingivalis, Prevotella intermedia, and Tannerella forsythia have higher populations in both peri-implant inflammation and periodontal defects [12]. More recently, ligatures have been used in these models to promote tissue breakdown within shorter periods than was the case in earlier models, which were prepared over periods of years [15]. A recently published study has described a canine model in which circum-ferential defects are preformed around implants, followed by induction of peri-implantitis with ligatures [16]. In the present canine study, a similar peri-implant model was adopted and crater-shaped defects were preformed with saucer-shaped burs before ligature placement. The aim was to deter-mine the impact of pre-existing peri-implant crater-shaped bone defects on the evolution of the in situ microbiome and the progression of defects, relative to those induced over time by ligature placement only.
Materials and Methods
The study was approved by the Ethics Committee for Animal Research at the University of Murcia (Spain). The study protocol followed guidelines established by the European Union Council Directive of February 1, 2013 (R.D. 53/2013), and was registered with the Ministry of Animal Health (Murcia Regional Government; Reg. no. A1320141102). Eight Beagle dogs were purchased, aged approximately 1.5 years, from a licensed vendor in Murcia (Spain) for the study. Upon clinical assessment, the dogs were in good general health and showed no signs of oral viral or fungal lesions. No dog presented with any occlusal trauma. Animals were quarantined for vaccination with anti-rabies vaccine and administration of vitamins. Pre- and postoperatively, the animals were kept in individual cages. After three days, they received appropriate veterinary care with unrestricted access to water and standard laboratory nutritional support throughout the treatment period. All animals presented with intact dental arches without any oral viral or fungal lesions. This study followed the Animal Research: Report-ing of In Vivo Experiments (ARRIVE) guidelines [17]. The timeline of the study is outlined in Fig. 1.
Anesthesia protocol
Acepromazine 0.12-0.25 mg/kg, buprenorphine 0.01 mg/kg, medetomi-dine 35 mg/kg with 10% zolazepam at 0.10 mg/kg, acepromazine maleate 0.12-0.25 mg/kg (Calmo-Neosan, Pfizer, Madrid, Spain), and medeto-midine 35 mg/kg (Medetor 1 mg, Virbac, CP-Pharma GmbH, Burgdorf, Germany) were administered to pre-anesthetize the animals. The mixture was injected intramuscularly in the femoral quadriceps. General anesthesia was administered through an intravenous catheter (diameter: 22/20 G) in
Original article
Influence of preformed bone defects on key pathogens and bone loss during experimental
peri-implantitis formation in a canine model
Alex Solderer
1), Benjamin Pippenger
1,2), Yann Gager
3), Kai Fischer
1,4), and Patrick R. Schmidlin
1) 1) Center of Dental Medicine, University of Zurich, Zurich, Switzerland2) Preclinical and Translational Research, Institute Straumann AG, Basel, Switzerland 3) Genolytic GmbH, Leipzig, Germany
4) Private practice, Wurzburg, Germany
(Received August 29, 2020; Accepted December 4, 2020)
Correspondence to Dr. Alex Solderer, Center of Dental Medicine, University of Zurich, Plattenstrasse 11, Zurich 8032, Switzerland
Fax: +41-44-634-4308 Email: [email protected] J-STAGE Advance Publication: February 17, 2021 Color figures can be viewed in the online issue at J-STAGE. doi.org/10.2334/josnusd.20-0444
the cephalic vein with propofol at a slow constant infusion rate of 0.4 mg/ kg/min. Conventional dental infiltration anesthesia ([articaine 40/0.0005 mg/mL; 1% epinephrine] [Articaine, Inibsa, Barcelona, Spain]) was administered at the surgical sites. All procedures were performed under the supervision of a veterinary physician.
Surgical procedure
Sixty-four teeth from eight dogs were removed. Following two implanta-tion protocols after tooth extracimplanta-tion and healing, six implants (three per side) were installed in the mandibles of these dogs. The dogs were divided into two treatment groups of four dogs each: a “non-preformed” group (no preformed defects [n = 24]) and a “preformed” group (standardized marginal bone defects in the implantation bed [n = 24]). Bone defects were formed using a specially designed 2.8 mm-deep and 7-mm-wide bur with a saucer-shaped profile (Straumann, Switzerland). In both groups, identical implants (3.3 mm × 8 mm, BLT, Straumann, Switzerland), which healed in 2 months, were installed. Next, experimental peri-implantitis was induced with silk ligatures in both groups for another 2 months (Fig. 2). Ligatures were placed in the marginal part of the implants in both groups in order to facilitate plaque accumulation, without forced advancement of the liga-tures into the preformed defects.
Data acquisition
The data were collected during the three sampling sessions: March (Baseline-BL), May (T1), and July 2018 (T2) (Fig. 3). The time differences between the baseline and T1 and T2 were 84 and 54 days, respectively. During the first session, two teeth (one from each side) from a selection of four dogs (n = 8) were sampled at the baseline. The sampling procedure was performed using a sterile paper point inserted between the tooth and the gum. At the baseline, eight teeth from each dog (anterior, middle, and posterior teeth from each side) were extracted for implant installation. In general, six implants and two control teeth (one from each side) from all dogs were sampled with a sterile paper point at T1 and T2. As an excep-tion, dogs 1034 and 9581 could not be sampled respectively for one and two implants. Periapical X-ray images were taken at the baseline and T2 to illustrate and measure the defect depths after 2 months of ligature placement. At the end of this study, the dogs were not sacrificed to obtain histological data because this study was part of two other ongoing studies, which used the two different defect models.
Microbiological analysis
The sterile paper points were analyzed using a standard microbiological kit, iai PadoTest (Institut für Angewandte Immunologie IAI AG, Zuchwil, Switzerland). This kit relies on quantitative PCR (qPCR) to determine the total population of bacteria and the quantities of six key bacteria involved in periodontitis and peri-implantitis: Aggregatibacter actinomycetemcomi-tans, Filifactor alocis, Porphyromonas gingivalis, Prevotella intermedia, Tannerella forsythia, and Treponema denticola. The microbiological test provided information about the total quantity of bacteria (total bacterial load, TBL) and quantities of each of the six key bacteria and their sum (total marker load, TML).
Bone defect analysis
Bone defect depths were assessed radiologically after implant installa-tion and 2 months of ligature-induced peri-implantitis formainstalla-tion (Fig. 4). Defect depths were measured on periapical radiographs (Fiji, Image J) from the apical point of the defect to the implant shoulder by a calibrated and blinded examiner.
The average defect depth for each implant (mesial and distal measure-ments) and each dog was calculated to obtain separate data for each group (the “preformed” and “non-preformed” defect groups). The threads on each radiograph were used for calibration of the individual radiographs.
Data analysis
Means, standard deviations, medians, and interquartile ranges (IQR) were calculated for defect depths, and means for TBL and TML. TBL, TML, and bacterial load for each of the five key bacteria identified in this study were compared between the “preformed” and “non-preformed” groups at baseline (BL), T1, and T2. To determine whether extreme values were outliers, the Cook’s D was calculated. Values with a Cook’s D > 4/n were used as the cut-off.
Using the Mann-Whitney U-test for independent samples, the bacte-rial loads and defect depths of the treatment groups were compared. When comparing outcomes at the different time points, the Wilcoxon signed-rank test for dependent samples was used. Mixed linear regression models were used to examine the influence of different factors on the outcomes, with the advantage that the effect of the animal could be taken into account. The model included a point in time, tooth/implant position of the implant in the mandible, side of the mandible, and bacterial load (when considered as a Fig. 1 Flow chart of the experimental procedures and timeline
Fig. 2 Surgical and post-surgical procedures. A, preformation of saucer-shaped defects (Test); B, implants after insertion with preformed defects and healing caps (test); C, D, bone-level implant placement without any crestal bone modifications (control); E, sites after 2 months of ligature-induced peri-implantitis; F, sampling after abutment removal with sterile paper points
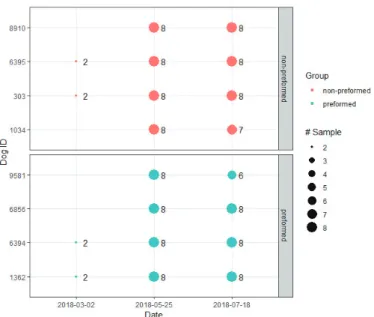
Fig. 3 Sampling design for eight dogs over three sampling sessions between BL and T2. BL (2018-03-02) consisted of sampling two control teeth in four dogs (“baseline” group). T1 and T2 sampling dates (2018-05-25 and 2018-07-18) consisted of two control teeth and six implants in eight dogs. As an exception, dogs 1034 and 9581 could not be sampled for one and two implants, respectively. These were divided into two groups: “non-preformed” (control), where no defects were preformed (four dogs) and “preformed” (test), where the implantation bed received standardized marginal bone defects (four dogs).
factor) as fixed effects, as well as the dog as a random effect. The Dunnett-Hsu method was used to adjust for multiple comparisons. All statistical analyses were performed using the statistical software, R version 3.4.3 (R Core Team 2018, Vienna). The significance level was set to an alpha level of P = 0.05.
Results
In general, the surgical procedures and healing were uneventful, except for one tooth and two implants. Microbiological sampling could not be performed for one control tooth in one dog at T2; i.e. two implants could not be measured at T2, because the radiographic data were unreadable. Further data for one implant in the test group were omitted from statistical analysis of bone defect depths due to complete bone loss.
Total Bacterial Load
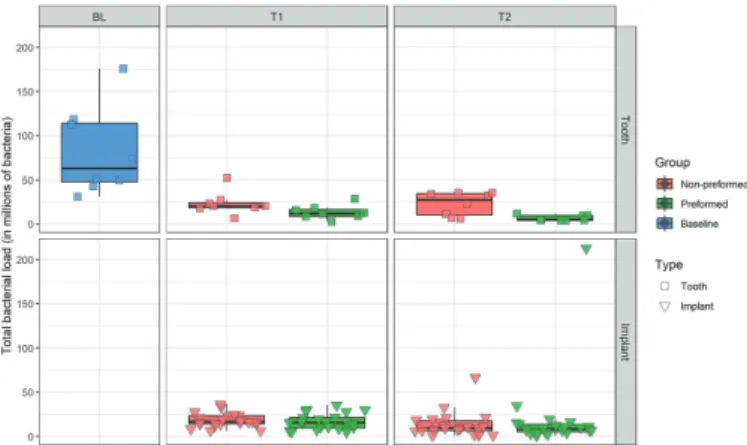
TBL values ranged widely between 0.9 million and 212.8 million bacteria (Fig. 5). Authors observed a decrease in TBL at T1 and T2 for both “pre-formed” (test) and “non-pre“pre-formed” (control) from the TBL measured at the baseline in all eight animals. Before therapy, the mean TBL for teeth was 82 million bacteria (range = 31-175.8 million). After implant instal-lation and 2 months of healing, decreased but comparable mean values of TBL were found for the teeth (x̄ for the control group = 23.3 million; x̄ for the test group = 13.3 million) and the implants (x̄ for the control group = 18.4 million; x̄ for the test group = 16.3 million). Mean values of TBL 2 months after ligature placement remained relatively consistent for the teeth ( x̄ for the control group = 23 million; x̄ for the test group = 6.6 million) and implants (x̄ for the control group = 13.3 million; x̄ for the control group = 19.1 million). The increase in mean TBL at T2 for implants in the “preformed” group was largely due to the presence of an outlier (TBL = 212.8 million).
Total Marker Load
TML was based on five bacterial species because A. actinomycetemcomi-tans was not detected. The TML showed values ranging between 0 and 7.3 million (Fig. 6). There was a slow but continuous decrease in the TML over the three sampling sessions. Before therapy, the mean TML for the teeth was 2.7 million bacteria (range = 0.7-7.3 million). After implant installa-tion and 2 months of healing, decreased mean values of TML for the teeth (x̄ for control group = 1.9 million; x̄ for the test group = 0.9 million) and the implants (x̄ for the control group = 1.4 million; x̄ for the test group = 1.3 million) were recorded. Mean values of TML 2 months after ligature placement remained relatively consistent around teeth (x̄ for the control group = 0.7 million; x̄ for the test group = 0.1 million) and implants (x̄ for control group = 0.6 million; x̄ for the test group = 0.4 million). The differ-ence between TBL and TML for all samples showed that bacteria, with an average of 19.6 million bacteria (range = 0.9-212.1 million), were present other than the five key species.
Specific periopathogens
Two of the six bacterial species investigated—P. gingivalis and T. dentic-ola—were detected in 100% of the teeth and implants sampled. Three other bacterial species were detected only in a fraction of the samples: 99.2% of samples for T. forsythia, 95.5% for F. alocis, and 35.3% for P. intermedia. The sixth bacterial species—A. actinomycetemcomitans—remained sys-tematically undetected. Follow-up of the control teeth (Table 1) revealed that P. gingivalis had the highest mean bacterial count, followed in order by
T. forsythia, T. denticola, F. alocis, and P. intermedia. Only at the baseline did P. intermedia have a larger population than F. alocis, which remained undetected. Furthermore, the control group showed quasi-systematically higher mean bacterial counts than those from the test group. The follow-up of implants (Table 2) revealed a similar pattern as that for the control teeth, with P. gingivalis showing the highest mean bacterial count, followed in order by T. forsythia, T. denticola, F. alocis, and P. intermedia. The mean counts of the five bacteria were comparable between the control and test groups at both sampling points (T1 and T2).
Comparison of defect depths between the preformed and non-preformed groups
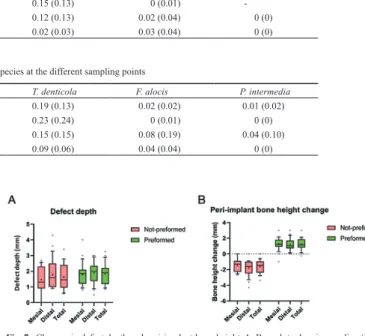
At the time of implant installation, the defects had a depth of 2.8 mm. After 2 months of peri-implantitis induction, the depth in preformed defects was 1.84 mm, compared with 1.64 mm in the control group (Table 3). Figure 3 shows the median (IQR) defect depths for mesial and distal sites, as well as for the test and control groups. A two-sample t-test comparing the two treatments yielded no statistically significant difference (P = 0.34). Figure 7 shows the change in peri-implant bone height in the test and control groups during ligature placement; a positive bone height change in the test group was observed relative to the control group.
Discussion
This study using a canine model was conducted to assess the influence of preformed saucer-shaped peri-implant defects on key pathogens and the development of bone defects in the early stage of peri-implantitis, com-pared to those induced solely by ligature placement.
After ligature placement, deep pocketing, suppuration, and loss of alveolar bone were observed. This animal model has been widely chosen in studies evaluating the pathogenesis and treatment of peri-implantitis [10]. Although the tissue breakdown induced by ligatures does not reflect the natural development and progression rate in humans, the defect sizes Fig. 5 Follow-up of total bacterial load (in millions of bacteria) of teeth and implants for each group (“baseline”, “not-preformed”, and “preformed”)
Fig. 6 Follow-up of total marker load (in millions of bacteria) of teeth and implants for each group (“baseline”, “not-preformed”, and “preformed”)
Fig.4 Representative radiographs of the “preformed” group. Images show the situation of two neighboring implants after defect formation and implant placement (left) and 4 months later after peri-implantitis induction (right: healing abutments removed)
and shapes seem to resemble those occurring naturally in humans [18]. In 2006, Schwarz et al. [13] compared experimentally induced peri-implantitis defects in dogs with defects in humans. They concluded that the configuration and size of experimental ligature-induced defects seemed to follow those of naturally occurring defects. The authors further considered that circumferential crater-shaped bone loss without any dehiscence was the defect most often observed in humans (55.3%) and dogs (86.6%). That study, similar to the one published by Seong et al. [16] in 2019, involved a peri-implantitis model where direct acute trauma led to circumferential defects. This type of defect initiation doubtless does not represent the condition generally observed in a clinical setting. Nevertheless, upon comparison of microbiological data and defect depths, the authors found no significant difference between the “newly” proposed and conventional peri-implantitis models.
Some authors have expressed concerns about spontaneous regression in peri-implant defects caused by acute trauma [16]. The findings of the present study were consistent with these results. At the time of implant installation, preformed defects showed a standardized defect depth of 2.8 mm and a width of 7 mm. At the end of the study, preformed defects had an average depth of 1.84 mm, showing regression of bone defect depth after traumatic induction of peri-implant defects (Fig. 7). As no X-ray plates or measurements were obtained at T1, the extent to which preformed defects showed regression during 2 months of healing after implant installation or during active ligature-induced peri-implantitis (2 months) remained unclear. However, there is a need for caution when implementing this model in studies assessing regenerative processes in peri-implantitis defects, as the results could be biased by spontaneous regression.
As the difference in depths between the control and treatment groups was not statistically significant (less depth for the control than for treat-ment), the statistical power of the study to confirm that the treatment was not inferior, considering a tolerance range of 0.4 mm as clinically insig-nificant, was post-calculated. The power of the study with four animals per group was 0.76, compared with 0.89 for six animals per group. This indicates that our study was under-powered.
Nevertheless, comparing the depths of non-preformed and preformed defects, the latter were observed to result in a more homogenous and predictable defect size (Fig. 6). Clarification of the predictability and uniformity of defect sizes would be helpful for future studies designed to investigate and compare preclinical peri-implantitis treatments.
With regard to study design, the present study was part of two other ongoing studies that used these two different defect models. Therefore, no split-mouth design was appropriate. The authors consider these cir-cumstances to be an advantage, rather than a shortcoming, in terms of the 3Rs in animal research (Replacement, Reduction and Refinement). Fur-thermore, no specimens for further histological analysis could have been retrieved for this reason.
Microbiological studies revealed similar findings with respect to the TML for the “non-preformed” and “preformed” groups, showing an initial increase at T1, followed by a decrease at T2. A decrease in TBL was observed at T1 and T2 in both groups, from the TBL recorded at the baseline.
As the TBL represents all bacteria present, this observation might be due to a decrease in abundant symbiotic bacteria with a shift to dysbio-sis [19]. Although a minimal decrease in TML was observed at different time points (baseline, T1, and T2), the mean TML of the different groups remained comparable.
In this study, the silk ligatures induced peri-implantitis in 2 months (8 weeks). Charalampakis et al. [20], in a similar canine study, described the application of silk ligatures for 10 weeks followed by a period of 25 weeks of plaque accumulation after ligature removal. During the 25-week period of plaque accumulation, the subgingival bacterial load increased significantly over time. A longer study period, as well as ligature removal, might have led to an increase in TBL/TML of the implants.
A. actinomycetemcomitans was never detected, which indicates that this bacterium at least did not play a major role in peri-implantitis in this study. P. intermedia was found only in a fraction of the samples, whereas P. gingivalis showed the highest counts, followed in order by T. forsythia, T. denticola, F. alocis, and P. intermedia. Thus, three Gram-negative bacte-rial species (P. gingivalis, T. forsythia, and T. denticola) were found in higher amounts than the Gram-positive F. alocis and Gram-negative P. intermedia.
Data and opinions regarding peri-implantitis-associated bacteria have been mostly inconsistent. A systematic review from 2016 supported a direct association between peri-implantitis and the periopathogen red cluster bacteria, P. gingivalis, T. denticola, and T. forsythia, and the orange cluster bacteria, P. intermedia and Campylobacter rectus. P. gingivalis and T. forsythia were the most common bacterial species. Although less studied, C. rectus has also been reported to be associated with periodontitis
BL Baseline 1.88 (2.3) 0.50 (0.33) 0.29 (0.19) 0 (0) 0.07 (0.11)
T1 ControlTest 0.92 (0.92)0.45 (0.40) 0.81 (0.58)0.31 (0.24) 0.13 (0.05)0.15 (0.13) 0.03 (0.04)0 (0.01) - -T2 ControlTest 0.29 (0.38)0.09 (0.11) 0.27 (0.23)0.07 (0.07) 0.12 (0.13)0.02 (0.03) 0.02 (0.04)0.03 (0.04) 0 (0)0 (0)
Table 3 Mean defect depths (mm) of ligature-induced peri-implantitis in the preformed (test) and non-preformed (control) bone defects after 2 months
Group Dog (no. of implants) Mean defect depth (mm)
No defect (control) 1 (5) 1.91
2 (6) 0.71
3 (6) 1.45
4 (6) 2.48
Average (SD) 1.64 (0.75)
Preformed defect (test) 1 (5) 2.02
2 (5) 1.73
3 (6) 2.08
4 (6) 1.54
Average (SD) 1.84 (0.22)
Table 2 Mean (standard deviation) populations (in millions) of the five key bacterial species at the different sampling points
Date Group P. gingivalis T. forsythia T. denticola F. alocis P. intermedia
T1 ControlTest 0.68 (0.63)0.75 (1.01) 0.49 (0.47)0.39 (0.45) 0.19 (0.13)0.23 (0.24) 0.02 (0.02)0 (0.01) 0.01 (0.02)0 (0) T2 ControlTest 0.21 (0.28)0.16 (0.17) 0.19 (0.28)0.16 (0.13) 0.15 (0.15)0.09 (0.06) 0.08 (0.19)0.04 (0.04) 0.04 (0.10)0 (0)
Fig. 7 Changes in defect depth and peri-implant bone height. A, Box-plots showing median (IQR) for mesial sites, distal sites, and total in the non-preformed and preformed groups; B, Box-plots showing the change in peri-implant bone height after ligature placement
Furthermore, in a recent canine study, an early increase in the T. for-sythia population after ligature placement was associated with an increase in the pocket probing depth (PPD) [22]. These findings are consistent with the present observations.
In contrast, Dabdoub et al. [23], in 2013, found in a representative cohort in which peri-implantitis-infected implants showed perio-patho-genic bacteria at only 37% of the sites examined. These observations were partially corroborated by a systematic review in 2017, which – on the one hand – described periodontitis and peri-implantitis as different entities in terms of microbial composition, peri-implantitis showing a more hetero-geneous and complex microbiome than periodontitis predominated by non-culturable Gram-negative species. On the other hand, red and orange complex bacteria, i.e. P. gingivalis and P. intermedia, are encountered more frequently in peri-implant inflammation than in healthy gums [24]. Consequently, the authors indicated the need for more research.
In the present study, the patterns of perio-pathogenic bacteria, in terms of distribution and amount, found in “preformed” defects mirrored those formed in “non-preformed” defects after ligature-induced inflammation and tissue breakdown. A comparison between the two groups sampled during the same experimental period revealed that most implants (85.2%) showed a general overlap of their bacterial compositions. The detec-tion rate of P. intermedia was only 39.7% and only small numbers were present, suggesting a limited role of this bacterium in peri-implantitis. A comparison of TML values at the different sampling points revealed a general decrease around implants and apparently around control teeth. The TML values for the “non-preformed” and “preformed” groups at T1 were similar, suggesting that the tapered drill did not influence the control mark-ers. TML values were comparably decreased in the “non-preformed” and “preformed” groups, suggesting an immune reaction and a reduction in the extent of the peri-implantitis.
In conclusion, preformed peri-implant crater-shaped bone defects showed comparable results in terms of TML, the incidence of periodontal pathogenic bacteria, and defect depth after 2 months of ligature-induced peri-implantitis in this canine model. These results suggest that the protocol used in the present peri-implantitis model does not create any differences in defect size or microbial composition.
Acknowledgments
We would like to thank Aline Memmel from Genolytic Co. for supervising the laboratory work. We also thank Leticia Grize and Daniel Wiedemeier for support with the statistical analysis. This study was part of two other studies, which were funded by the University of Zurich and, in part, by Straumann (Basel, Switzerland) and EMS (Nyon, Switzerland).
Conflict of interest
Yann Gager is an employee at Genolytic Co., which supervised the labora-tory work and analysis using the microbiological kit iai Padotest. Benjamin Pippenger works at Institut Straumann AG, which provided the materials for this study.
1. Buser D, Janner SF, Wittneben JG, Brägger U, Ramseier CA, Salvi GE (2012) 10-year survival and success rates of 511 titanium implants with a sandblasted and acid-etched surface: a retrospective study in 303 partially edentulous patients. Clin Implant Dent Relat Res 14, 839-851.
2. Chappuis V, Buser R, Brägger U, Bornstein MM, Salvi GE, Buser D (2013) Long-term outcomes of dental implants with a titanium plasma-sprayed surface: a 20-year prospective case series study in partially edentulous patients. Clin Implant Dent Relat Res 15, 780-790. 3. Schwarz F, Derks J, Monje A, Wang HL (2018) Peri-implantitis. J Clin Periodontol 45,
S246-S266.
4. Manor Y, Chaushu G, Lorean A, Mijiritzky E (2015) A retrospective analysis of dental implants replacing failed implants in grafted maxillary sinus: a case series. Int J Oral Max-illofac Implants 30, 1156-1160.
5. Anitua E, Piñas L, Begoña L, Alkhraisat MH (2017) Prognosis of dental implants imme-diately placed in sockets affected by peri-implantitis: a retrospective pilot study. Int J Periodontics Restorative Dent 37, 713-719.
6. Derks J, Tomasi C (2015) Peri-implant health and disease. A systematic review of current epidemiology. J Clin Periodontol 42 Suppl 16, S158-S171.
7. Mombelli A (2002) Microbiology and antimicrobial therapy of peri-implantitis. Periodon-tol 2000 28, 177-189.
8. Esposito M, Grusovin MG, Worthington HV (2012) Treatment of peri-implantitis: what interventions are effective? A Cochrane systematic review. Eur J Oral Implantol 5 Suppl, S21-S41.
9. Rovin S, Costich ER, Gordon HA (1966) The influence of bacteria and irritation in the initiation of periodontal disease in germfree and conventional rats. J Periodontal Res 1, 193-204.
10. Lindhe J, Berglundh T, Ericsson I, Liljenberg B, Marinello C (1992) Experimental break-down of peri-implant and periodontal tissues. A study in the beagle dog. Clin Oral Implants Res 3, 9-16.
11. Zitzmann NU, Berglundh T, Ericsson I, Lindhe J (2004) Spontaneous progression of experimentally induced periimplantitis. J Clin Periodontol 31, 845-849.
12. Schwarz F, Sculean A, Engebretson SP, Becker J, Sager M (2015) Animal models for peri-implant mucositis and peri-peri-implantitis. Periodont 2000 68, 168-181.
13. Schwarz F, Herten M, Sager M, Bieling K, Sculean A, Becker J 2007. Comparison of naturally occurring and ligature-induced peri-implantitis bone defects in humans and dogs. Clin Oral Implants Res 18, 161-170.
14. Leonhardt A, Berglundh T, Ericsson I, Dahlén G (1992) Putative periodontal pathogens on titanium implants and teeth in experimental gingivitis and periodontitis in beagle dogs. Clin Oral Implants Res 3, 112-119.
15. Lindhe J, Hamp SE, Loe H (1973) Experimental periodontitis in the beagle dog. Int Dent J 23, 432-437.
16. Seong WJ, Kotsakis G, Huh JK, Jeong SC, Nam KY, Kim JR et al. (2019) Clinical and microbiologic investigation of an expedited peri-implantitis dog model: an animal study. BMC Oral Health 19, 150.
17. Kilkenny C, Browne WJ, Cuthill IC, Emerson M, Altman DG (2010) Improving bioscience research reporting: the ARRIVE guidelines for reporting animal research. PLoS Biol 8, e1000412.
18. Berglundh T, Zitzmann NU, Donati M (2011) Are peri-implantitis lesions different from periodontitis lesions. J Clin Periodontol 38 Suppl 11, 188-202.
19. Yu XL, Chan Y, Zhuang L, Lai HC, Lang NP, Keung Leung W, Watt RM (2019) Intra-oral single-site comparisons of periodontal and peri-implant microbiota in health and disease. Clin Oral Implants Res 30, 760-776.
20. Charalampakis G, Abrahamsson I, Carcuac O, Dahlen G, Berglundh T (2014) Microbiota in experimental periodontitis and peri-implantitis in dogs. Clin Oral Implants Res 25, 1094-1098.
21. Pérez-Chaparro PJ, Duarte PM, Shibli JA, Montenegro S, Lacerda Heluy S, Figueiredo LC et al. (2016) The current weight of evidence of the microbiologic profile associated with peri-implantitis: a systematic review. J Periodontol 87, 1295-1304.
22. Zhu B, Meng H, Huang B, Chen Z, Lu R (2019) Detection of T. forsythia and other impor-tant bacteria in crestal and subcrestal implants with ligature-induced peri-implant infection in dogs. J Periodontol 90, 306-313.
23. Dabdoub SM, Tsigarida AA, Kumar PS (2013) Patient-specific analysis of periodontal and peri-implant microbiomes. J Dent Res 92, 168S-175S.
24. Lafaurie GI, Sabogal MA, Castillo DM, Rincón MV, Gómez LA, Lesmes YA et al. (2017) Microbiome and microbial biofilm profiles of peri-implantitis: a systematic review. J Peri-odontol 88, 1066-1089.