依 頼 総 説
慢性疼痛患者の認知的側面にどのように対応するか
大久保昌和
1),和嶋浩一
2)1)日本大学松戸歯学部有床義歯補綴学講座
2)慶應義塾大学医学部歯科・口腔外科学教室
抄 録
本教育講演では慢性疼痛患者の認知的側面を理解するために,外傷後有痛性三叉神経ニューロパシーの 薬物療法の現状を知り,口腔顔面痛患者の脳イメージング研究のメタ分析から明らかにされた,脳の機能 的あるいは形態的変化について,そして,慢性疼痛患者の情動・認知的側面への補完代替医療の介入が疼 痛緩和に有効であるとする最近の総説を解説し,今後の慢性疼痛患者管理の方向性について述べる.慢性 口腔顔面痛“患者”の管理には痛みの感覚的,情動的,認知的側面を熟知しておく必要があり,それには 患者を知るための医療面接技法の習得や質問票の活用が勧められる.外傷後有痛性三叉神経ニューロパ シー“患者”の薬物療法の結果は必ずしも思わしくなく,生物心理社会的アプローチを併用することや有 効で安全な薬の開発が望まれる.ほとんどの慢性疼痛状態は痛みの中枢化と呼ぶことができる,脳の機能 的,形態的,あるいは化学的変化を惹き起こし,fMRI は客観的診断への可能性を有している.補完医療の 慢性疼痛“患者”の認知的側面への介入は有効かもしれず,口腔顔面痛歯科医は薬物療法に加えて神経学 や精神医学に関する知識の習得と専門家との連携,そして,補完医療の可能性についても考慮する必要が ある. キーワード:慢性口腔顔面痛,痛みの認知的側面,ニューロイメージング,認知行動療法,補完医療 はじめに 痛みは実質的あるいは潜在的な組織損傷に結びつく, あるいはそのような損傷を表す言葉によって述べられ る不快な感覚,情動体験である(IASP, 1979).口腔顔 面痛の痛覚伝導路をみても,三叉神経視床路は外側系 と内側系にわかれ,それぞれ痛みの感覚・識別的側面 と情動・認知的側面 に関わっており,これらは双方向 的に影響するばかりでなく,さらに多くの神経機構を 巻き込んでいることが理解できる.本教育講演では慢 性疼痛患者の認知的側面を理解するために,外傷後有 痛性三叉神経ニューロパシーの薬物療法の現状を知り, 痛みの中枢化と口腔顔面痛患者の脳イメージング研究 のメタ分析から明らかにされた,脳の機能的あるいは 形態的変化について,そして,慢性疼痛患者の情動・ 認知的側面への補完代替医療の介入が疼痛緩和に有効 であるとする最近の総説を解説し,今後の慢性疼痛患 者管理の方向性について述べる. 外傷後有痛性三叉神経ニューロパシーの 薬物療法の有効性 口腔顔面領域の神経障害性疼痛に関する最近の研究1) は,国際頭痛分類第3 版β版の診断基準2)(表)に従 大久保昌和 〒271-8587 千葉県松戸市栄町西 2-870-1 日本大学松戸歯学部有床義歯補綴学講座い外傷後有痛性三叉神経ニューロパシーと診断した 91 人の患者に対する,ガイドラインの推奨に従った薬 物療法を行い,コントロールとした典型的三叉神経痛 患者に対する薬物療法は74.1%が有効であったのに対 し,疼痛強度に50%以上の改善が見られたのはほんの 11%に過ぎなかったと報告した.この結果は,現在使 用可能な薬剤が限られていることや薬剤の限定的な効 果や有害反応を反映しており,治療のプロトコールを 見直す必要があることや薬物療法に加えて生物心理社 会的あるいは補完医療的アプローチによる検討が必要 であることを示唆している. 表 外傷後有痛性三叉神経ニューロパシーの診断基準 (ICHD-3β, 13.1.2.3) 片側顔面あるいは口部の痛みが三叉神経の外傷によってお こり,痛み以外に三叉神経障害の症状や臨床徴候を伴う, 診断基準 A 片側顔面あるいは口部の痛みで,基準 C を満たす, B 三叉神経に対する外傷が明確で,三叉神経の臨床的に明 らかな陽 性症状(痛覚過敏,アロディニア)あるいは 陰性症状(感覚低下,痛覚鈍麻)を伴う, C 下記の両方の因果関係が認められる 1 外傷を受けた三叉神経支配領域の同じ領域に痛みがある 2 三叉神経外傷から 3‐6 ヶ月以内に痛みが発症している D 他に最適な ICHD-3 の診断がない 注記 三叉神経に対する外傷は,機械的,化学的,温度的, あるいは放射線による障害を含む. 痛みの中枢化と三叉神経領域の慢性疼痛患者の 脳の機能的,形態的変化 ほ と ん ど の 慢 性 疼 痛 状 態 は , 痛 み の 中 枢 化 ” centralization of pain”と呼ぶことができる,脳の機能的, 形態的,さらに化学的な変化を惹き起こし3),患者の 遺伝的な要因に加えて,いかなる環境要因への暴露が 患者の痛みの慢性化につながるのかも研究課題となっ ている.Lin4)は PRISMA のガイドラインに従い, PubMed を用いて,過去 10 年間(1994 年 1 月 1 日から 2013 年 8 月 31 日)に出版された患者を対象にした三 叉神経系あるいはTMD による疼痛に焦点をあてた研 究で,脳の機能的あるいは構造的変化をMRI により測 灰白質)における機能的(活動性の上昇あるいは低下) あるいは構造的(灰白質の厚さ)変化について,質的 メタアナリシスを行った.その結果,陽性の機能的変 化が認められた関心領域については神経障害性疼痛と TMD の間に相関がみられた,すなわち疼痛処理に関わ る領域に違いがなかったが,陰性の構造的変化(灰白 質の厚さの減少)については両者に相関は見られず, 神経障害性疼痛でより大きな変化が認められている. (図1) 図1 三叉神経障害性疼痛と TMD との間の脳活動性パター ンの比較(Lin CS, 2014 から引用) 痛みの認知的・情動的コントロールと 慢性疼痛におけるその混乱 NIH(米国国立衛生研究所)の一部門として設立さ れた補完代替医療センターでは,これまで研究が不足 していた補完医療あるいは代替医療の科学的評価をす
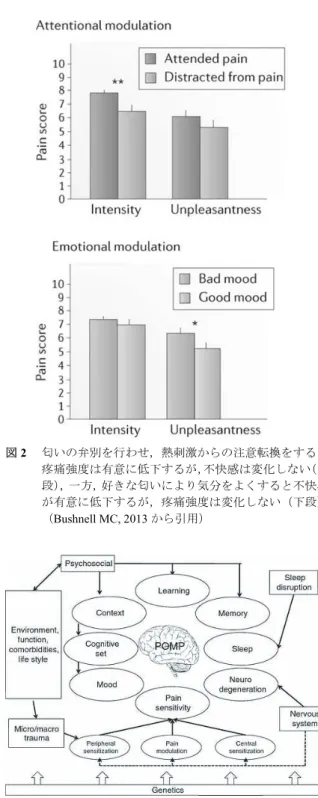
線維筋痛症患者に認知行動療法(CBT)を行った際 の圧刺激による脳の機能的変化についてfMRI を用い て検討したランダム化比較試験5)は,CBT 前後で前頭 前皮質背外側部(DLPFC)における活動が増加するこ とを初めて明らかにした.また,禅の瞑想者を対象と して,熱刺激とfMRI を用いて脳の機能的変化を調べ た他の研究6)は,禅の瞑想はACC の処理が増加してい るにもかかわらず,DLPFC の活動性が低下する状態, あたかも痛みを無視できると考えられる脳の活動性を 検出している.Bushnell ら7,8)はまた,熱刺激と匂いを 用いて興味深い研究を行っている.熱刺激を与えなが ら匂いの弁別を行わせたり,心地よい匂いと不快な匂 いを嗅がせたりして(換言すれば,注意あるいは注意 転換と快あるいは不快による)疼痛強度(図2)と fMRI による脳活動部位を比較した結果,認知と情動は異な る経路により痛みを調節しているようだと結論付けて いる.さらにBingel ら9)は,期待とオピオイドの効果 についてfMRI を用いて検討し,純粋なオピオイドの 効果(投与を知らせない)と比較し正の期待(positive expectation,痛みが減ると知らせる)は DLPFC と CC (anterior)そして PAG の機能的変化を通じてオピオ イドの効果を増強する,一方,負の期待(negative expectation,痛みがひどくなると知らせる)は海馬の 機能的変化を通じてオピオイドの効果を完全に無効に するということを論証している.これらの研究から, 痛みの認知的側面には DLPFC が重要な役割を演じて いると考えられる. 最後に,口腔顔面痛のエキスパートグループにより すでに提唱されている,Persistent orofacial muscle pain
の複雑な病態モデル(図 3)を参照いただきたい.患 者の遺伝的な背景に,疼痛感受性,そして心理社会的 因子,外傷などの身体的影響,学習,記憶,睡眠,そ して事情,認知,気分などの様々な環境因子など,さ らには性別や民族性が複雑に関わりあうことが理解で きるモデルとなっている10). 図2 匂いの弁別を行わせ,熱刺激からの注意転換をすると 疼痛強度は有意に低下するが,不快感は変化しない(上 段),一方,好きな匂いにより気分をよくすると不快感 が有意に低下するが,疼痛強度は変化しない(下段), (Bushnell MC, 2013 から引用)
図3 Persistent orofacial muscle pain の複雑な病態モデル
まとめ これまで述べてきたように,慢性口腔顔面痛“患者” の管理には痛みの感覚的,情動的,認知的側面を熟知 しておく必要がある.それには患者を知るための医療 面接技法の習得や質問票の活用が勧められる.外傷後 有痛性三叉神経ニューロパシー“患者”の薬物療法の 結果は必ずしも思わしくなく,生物心理社会的アプ ローチを併用することや有効で安全な薬の開発が望ま れる.慢性口腔顔面痛“患者”の脳では機能的,形態 的,(あるいは化学的変化)が起こっており,fMRI は 客観的診断への可能性を有している.補完医療の慢性 疼痛“患者”の認知的側面への介入は有効かもしれず, 口腔顔面痛歯科医は薬物療法に加えて神経学や精神医 学に関する知識の習得と専門家との連携,そして,補 完医療の可能性についても考慮する必要がある. 稿を終えるにあたり,大雑把な内容の記載にとどま り説明不足があることをお詫びする.どうか詳細につ いては原著を参照されたい. 謝辞 本講演は科学研究費助成事業(基盤研究C25463265) の補助を受けた。 文献
1. Haviv Y, Zadik Y, Sharav Y, Benoliel R. Painful traumatic trigeminal neuropathy: an open study on the pharmacotherapeutic response to stepped treatment. J Oral Facial Pain Headache. 28:52-60, 2014.
2. Headache Classification Committee of the
International Headache Society (IHS) (2013) The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 33:629-808. (日本頭痛学会・国際頭痛分類委員会.国際頭痛 分類第3 版 beta 版.医学書院.東京.1-256,2014.) 3. Borsook D. A future without chronic pain:
neuroscience and clinical research. Cerebrum. 2012 May; 2012:7. Epub 2012 Jun 27.
4. Bushnell MC, Ceko M, Low LA. Cognitive and emotional control of pain and its disruption in chronic pain. Nat Rev Neurosci. 14:502-11, 2013.
5. Lin CS. Brain signature of chronic orofacial pain: a systematic review and meta-analysis on neuroimaging research of trigeminal neuropathic pain and temporomandibular joint disorders. PLoS One. 9: e94300, 2014.
6. Jensen KB, Kosek E, Wicksell R, Kemani M, Olsson G, Merle JV, Kadetoff D, Ingvar M. Cognitive Behavioral Therapy increases pain-evoked activation of the prefrontal cortex in patients with fibromyalgia. Pain. 153:1495-503, 2012.
7. Grant JA, Courtemanche J, Rainville P. A non-elaborative mental stance and decoupling of executive and pain-related cortices predicts low pain sensitivity in Zen meditators. Pain. 152:150-6, 2011. 8. Villemure C, Bushnell MC. Mood influences
supraspinal pain processing separately from attention. J Neurosci. 29:705-15, 2009.
9. Bingel U, Tracey I, Wiech K. Neuroimaging as a tool to investigate how cognitive factors influence analgesic drug outcomes. Neurosci Lett. 520:149-55, 2012.
10. Benoliel R, Svensson P, Heir GM, Sirois D, Zakrzewska J, Oke-Nwosu J, Torres SR, Greenberg MS, Klasser GD, Katz J, Eliav E. Persistent orofacial muscle pain. Oral Dis. Suppl 1:23-41, 2011.
Management Strategy against Cognitive Aspects of Chronic Pain
Patients.
Masakazu Okubo
1),Koichi Wajima
2)1)