Original Article J Clin Med Res. 2015;7(7):545-550
Association Between Visit-to-Visit Variability in Blood Pressure and Cardiovascular Events in Hypertensive Patients After
Successful Percutaneous Coronary Intervention
Kouki Gondo
a, Shin-ichiro Miura
a, b, d, Yasunori Suematsu
a, Yuhei Shiga
a, Takashi Kuwano
a, Makoto Sugihara
a, Amane Ike
a, Atsushi Iwata
a, Kota Motozato
a, c, Takaaki Kusumoto
c, Hiroaki Nishikawa
a,
Keijiro Saku
a, bAbstract
Background: Visit-to-visit variability (VVV) in blood pressure (BP) in addition to high BP has been shown to be a strong predictor of coronary events and stroke. Therefore, we investigated the associa- tions between VVV in BP or BP levels and cardiovascular events after successful percutaneous coronary intervention (PCI).
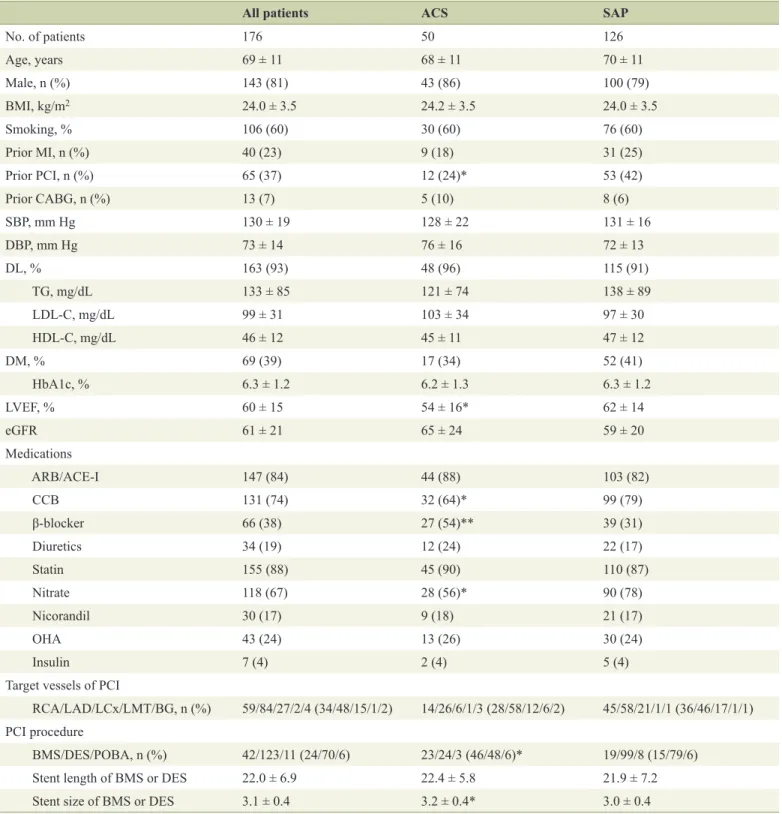
Methods: We enrolled 176 hypertensive patients who had undergone successful PCI and who had four clinic visits to measure BP until fol- low-up coronary angiography (CAG) at 6 - 9 months after PCI. The patients were divided into those with acute coronary syndrome (ACS group; n = 50) and those with stable angina pectoris (SAP group; n
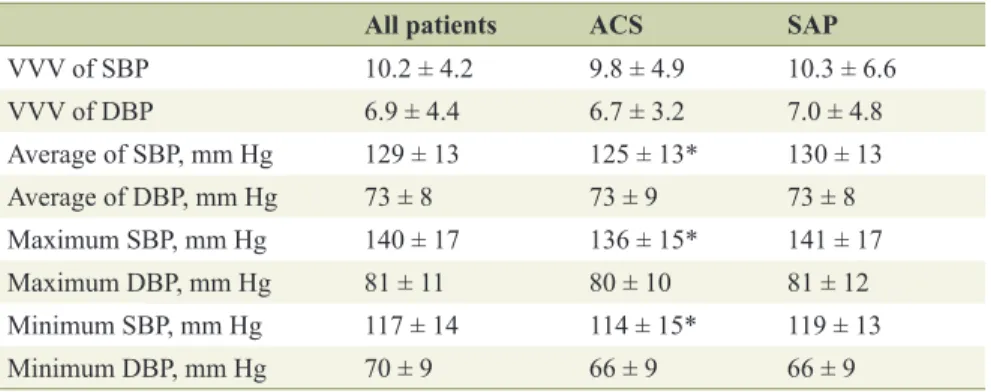
= 126). We determined VVV in BP expressed as the standard devia- tion (SD) of average BP, average, and the maximum and minimum BP during the follow-up period. Major adverse cardiovascular events (MACEs) (myocardial infarction (MI), target lesion revascularization (TLR) and all-cause death) were also analyzed.
Results: There were no significant differences in VVV in BP, average BP or maximum or minimum BP between the patients with and with- out MACE in all patients, the ACS and SAP groups. Interestingly, in the ACS group, VVV in SBP and maximum SBP in patients with MI were significantly higher than those in patients without MI. The cut- off levels for VVV in BP and maximum SBP that gave the greatest sensitivity and specificity for MI in the ACS group were 15.1 and 138 mm Hg, respectively.
Conclusion: Higher VVV in SBP and maximum SBP in patients with ACS after successful PCI were associated with the onset of MI.
Keywords: Visit-to-visit variability in blood pressure; Percutaneous
coronary intervention; Major adverse cardiovascular events; Myocar- dial infarction; Acute coronary syndrome
Introduction
High blood pressure (BP) is a major risk factor for the onset and progression of cardiovascular disease (CVD) and stroke.
Recently, visit-to-visit variability (VVV) in BP has also been shown to be a strong predictor of CVD, stroke and mortality independent of BP [1-4], although there is some controversy [5, 6]. The most noteworthy report was a systematic review and meta-analysis published in Hypertension in 2014 [4]. Diaz et al stated that modest associations between VVV in BP and CVD and all-cause mortality were present in many published studies. An increase in VVV in BP may be explained by arte- rial stiffness and abnormal autonomic function [7, 8]. Further- more, heart rate variability, a measure of autonomic dysfunc- tion, has been associated with an increased risk of myocardial ischemia in CVD patients [9]. Thus, VVV in BP is probably associated with CV events due to severe arterial stiffness and abnormal autonomic function.
According to the Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH2014), the target in BP control should be < 140/90 mm Hg [10]. When patients have multiple coronary risk factors, JSH2014 recom- mends a lower BP level (< 130/80 mm Hg) in the absence of significant coronary artery stenosis [10]. Although this point is still controversial, a decrease in BP causes a reduction in the diastolic coronary perfusion pressure and induces myocardial ischemia, which worsens the prognosis (J-shaped curve phe- nomenon) [11-13]. Nonetheless, there is no recommendation regarding the optimal lowest level or VVV in BP in patients with CVD.
To prevent the occurrence and progression of CVD, it may be important to manage both VVV in BP in addition to opti- mal BP in hypertensive patients with successful percutaneous coronary intervention (PCI), and we hypothesized that VVV in BP in hypertensive patients associates with major adverse cardiovascular events (MACEs) after PCI. Therefore, we in- vestigated the associations between VVV in BP or BP levels and MACE after successful PCI.
Manuscript accepted for publication April 10, 2015
a
Department of Cardiology, Fukuoka University School of Medicine, Fukuo- ka, Japan
b
Department of Molecular Cardiovascular Therapeutics, Fukuoka University School of Medicine, Fukuoka, Japan
c
Division of Cardiology, Izumi General Medical Center, Kagoshima, Japan
d