年 月 日 年 月 日 円 自 年 月 日 年 月 日 至 年 月 日 年 月 日 日 間 年 月 日 被保険者 被扶養者 昭 平 令 〒 自 年 月 日 至 年 月 日 コルセット装着日 年 月 日 自 年 月 日 至 年 月 日 〒 印 (注意事項) 支 給 期 間 資 格 取 得 資 格 喪 失 支 払 年 月 日 受 付 年 月 日 決 裁 決 裁 年 月 日 理 事 長 常 務 理 事 事 務 長 担 当 者 支 給 額
海外療養費支給申請書
(第 回目) 被 保 険 者 証 の 記 号 ・ 番 号 被 保 険 者 が 勤 務 す る ( し て い た ) 事 業 所 の 名 称 第 号 所在地 入院期間 被保険者 との続柄 傷 病 名 発 病 又 は 負 傷 の 年 月 日 年 月 日 発 病 又 は 負 傷 の 原 因 傷 病 の 経 過 支 給 対 象 者 氏名 生年 月日 年 月 日 診 療 又 は 手 当 を 受 け た 医 療 機 関 の 名 称 ・ 所 在 地 及 び 医 師 の 氏 名 名称 所在地 及び電 話番号 氏名 診 療 又 は 手 当 の 内 容 委任欄 この保険給付金の受領方を事業主に委任します。 被保険者氏名 診 療 又 は 手 当 を 受 け た 期 間 日間 診 療 又 は 手 当 に 要 し た 費 用 の 額 金 円也 診 療 又 は 手 当 が 被 保 険 者 の 選 定 に 係 る 特 別 の 病 室 の 提 供 、 そ の 他 厚 生 大 臣 が 定 め る 療 養 を 含 む と き は そ の 旨 療 養 の 給 付 又 は 特 定 療 養 費 も し く は 家 族 療 養 費 の 支 給 を 受 け る こ と の で き な か っ た 理 由 第 三 者 の 行 為 に よ る 負 傷 で あ る と き その事実と 届出の有無 加害者の氏名 加害者の住所 上記のとおり申請します。 年 月 日 健康保険組合理事長 殿 〒 - 住所 氏名 印 被保険者の 明細書については、医師が診療内容を記載した明細等があれば添付は不要とします。 別添の明細書以外の明細書については、日本語に翻訳し、翻訳者の氏名および連絡先を記載してください。 ※の欄については、組合へ申出て傷病届の提出が必要となります。【別 紙】
Request to Attending Physician
担当医へのお願い
From A 1. This form is used for claiming the social insurance benefit.
様式 A この様式は社会保険の給付の申請に使用されます。
2. This form should be completed and signed by the attending physician この様式は担当医が書き、かつ署名してください。
3. One form for each month, one form for hospitalization / outpatient and home visit. 各月毎、入院・入院外毎に付この様式が1枚必要です。
Attending Physician's Statement
診療内容明細書
1. Name of patient (Last, First) Age (Date of Birth) Sex (Male・Female)
患 者 名 年令(生年月日) 性別(男・女)
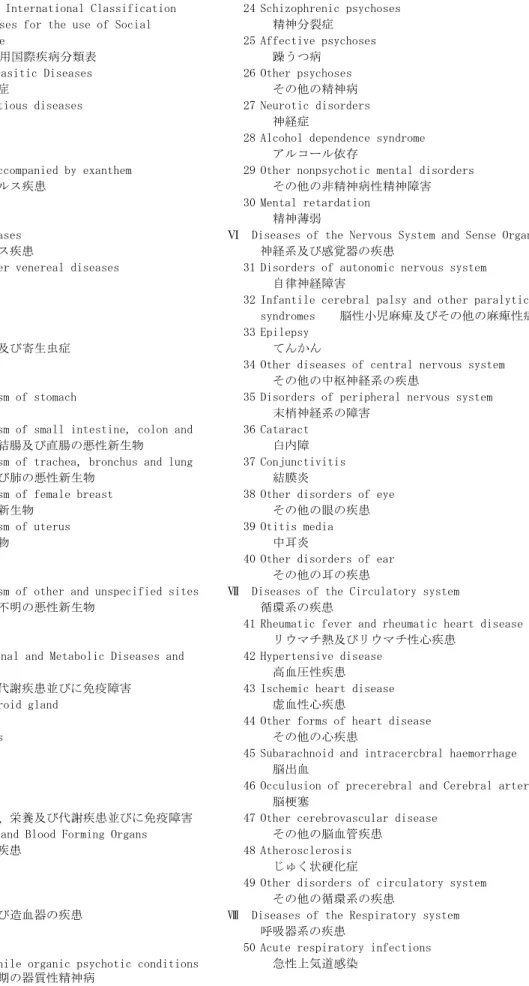
2. Name of Illness or Injury preferably with Number of International Classification of Diseases for the use of Social Insurance (See the other side of this form)
傷病名及び社会保険用国際疾病分類番号(裏面参照) 3. Date of First Diagnosis : ,
初 診 日
4. Days of Diagnosis and Treatment : days 診療日数
5. Type of Treatment 治療の分類
□ Hospitalization : From , to ( days)
入 院 自 至 ( 日間)
□ Outpatient or Home Visit : , ,
入 院 外 , ,
6. Nature and Condition of Illness or Injury (in brief) 症状の概要
7. Precription, Operation and any other treatments (in brief) 処方、手術その他の処置の概要
8. Was the treatment required as a result of an accidental injury? Yes □ No □
治療は事故の障害によるものですか。 はい いいえ
9. Itemized amounts paid to Hospital and / or Attending phyisician : Form B 治療実費 様式 B 10. Name and Address of Attending Physician
担当医の名前及び住所
Name 名前 : Last 姓 First 名 Title 称号
Address 住所 : Home 自宅 Phone 電話
Office 病院又は診療所 Phone 電話
Date 日付 Signature 署名
Attending Physician 担当医 Reference Number of your Medical Record (if applicable) 診療録の番号
(1/4ページ)
PAGE1/4PAGE2/4
Request to Attending Physician or Superintendent of Hospital / Clinic
担当医又は病院事務長へのお願い
From B 1. Please fill in this form so that the patient may claim the social insurance benefit.
様式 B この様式は患者の社会保険の給付の申請に必要ですので、証明をお願いします。
2. This form should be completed and signed by either the attending physician or the superintendent of a hospital / cl inic.
この様式は担当医又は病院の事務長が書き、かつ署名してください。
3. One form for each month and one form for hospitalization / outpatient (home visit) should be filled out.
各月毎、入院・入院外毎に付この様式1枚が必要です。 4. If not in dollars, please specify the unit used. ドル以外の貨幣の場合はその旨を書いてください。
Itemized Receipt
領収明細書
(1) Fee for Initial Office Visit 初 診 料 $ (2) Fee for Follow - up Office Visit 再 診 料 $
(3) Fee for Home Visit 往 診 料 $
(4) Fee for Hospital Visit 入 院 管 理 料 $
(5) Hospitalization 入 院 費 $ (6) Consultation 診 察 費 $ (7) Operation 手 術 費 $ (8) Professional Nursing 職 業 看 護 婦 費 $ (9) X - Ray Examinations X 線 検 査 費 $ (10) Laboratory Tests 諸 検 査 費 $ (11) Medicines 医 薬 費 $ (12) Surgical Dressing 包 帯 費 $ (13) Anesthetics 麻 酔 費 $
(14) Operating Room Charge 手 術 室 費 用 $
(15) The Others (Specify) その他(特記せよ) $ $
$ $
(16) Total 合 計 $
Important : Exclude the amount irrelevant to the treatment, i. e, payment for luxurious room charge.
注 意 : 高級室料等治療に直接関係のないものは除いてください。
Name and Address of Attending physician / Superintendent of Hospital or Clinic 担当医又は病院事務長の名前及び住所
Name : Last First Title
名前 姓 名 称号
Address : Home 自宅 Phone 電話
住所 Office 病院又は診療所 Phone 電話
Date Signature
PAGE3/4
Table of International Classification 24 Schizophrenic psychoses of Diseases for the use of Social 精神分裂症
Insurance 25 Affective psychoses
社会保険用国際疾病分類表 躁うつ病
Ⅰ Infectious and Parasitic Diseases 26 Other psychoses
感染症及び寄生虫症 その他の精神病
1 Intestinal infectious diseases 27 Neurotic disorders
腸管感染症 神経症
2 Tuberculosis 28 Alcohol dependence syndrome
結 核 アルコール依存
3 Viral diseases accompanied by exanthem 29 Other nonpsychotic mental disorders
発疹を伴うウイルス疾患 その他の非精神病性精神障害
4 Viral hepatitis 30 Mental retardation
ウイルス肝炎 精神薄弱
5 Other Viral diseases Ⅵ Diseases of the Nervous System and Sense Organs
その他のウイルス疾患 神経系及び感覚器の疾患
6 Syphilis and other venereal diseases 31 Disorders of autonomic nervous system
性 病 自律神経障害
7 Mycoses 32 Infantile cerebral palsy and other paralytic
真菌症 syndromes 脳性小児麻痺及びその他の麻痺性症候群
8 Others 33 Epilepsy
その他の感染症及び寄生虫症 てんかん
Ⅱ Neoplasms 34 Other diseases of central nervous system
新生物 その他の中枢神経系の疾患
9 Malignant neoplasm of stomach 35 Disorders of peripheral nervous system
胃の悪性新生物 末梢神経系の障害
10 Malignant neoplasm of small intestine, colon and 36 Cataract rectum 小腸、結腸及び直腸の悪性新生物 白内障 11 Malignant neoplasm of trachea, bronchus and lung 37 Conjunctivitis
気管、気管支及び肺の悪性新生物 結膜炎
12 Malignant neoplasm of female breast 38 Other disorders of eye
女性乳房の悪性新生物 その他の眼の疾患
13 Malignant neoplasm of uterus 39 Otitis media
子宮の悪性新生物 中耳炎
14 Leukaemia 40 Other disorders of ear
白血病 その他の耳の疾患
15 Malignant neoplasm of other and unspecified sites Ⅶ Diseases of the Circulatory system
その他及び部位不明の悪性新生物 循環系の疾患
16 Other neoplasm 41 Rheumatic fever and rheumatic heart disease
その他の新生物 リウマチ熱及びリウマチ性心疾患
Ⅲ Endocrine Nutritional and Metabolic Diseases and 42 Hypertensive disease
Immunity Disorders 高血圧性疾患
内分泌、栄養及び代謝疾患並びに免疫障害 43 Ischemic heart disease 17 Disorders of thyroid gland 虚血性心疾患
甲状腺の疾患 44 Other forms of heart disease 18 Diabetes mellitus その他の心疾患
糖尿病 45 Subarachnoid and intracercbral haemorrhage
19 Gout 脳出血
痛 風 46 Occulusion of precerebral and Cerebral arteries
20 Others 脳梗塞
その他の内分泌、栄養及び代謝疾患並びに免疫障害 47 Other cerebrovascular disease Ⅳ Diseases of Blood and Blood Forming Organs その他の脳血管疾患
血液及び造血器の疾患 48 Atherosclerosis
21 Anaemias じゅく状硬化症
貧 血 49 Other disorders of circulatory system
22 Others その他の循環系の疾患
その他の血液及び造血器の疾患 Ⅷ Diseases of the Respiratory system
Ⅴ Mental Disorders 呼吸器系の疾患
精神障害 50 Acute respiratory infections 23 Senile and presenile organic psychotic conditions 急性上気道感染
老年期及び初老期の器質性精神病
PAGE4/4
51 Acute bronchitis and bronchiolitis and bronchitis, 78 Hypertension complicating pregnancy and excessive not specified as acute or chronic vomiting in pregnancy 妊娠中毒症
急性及び詳細不明の気管支炎 ★ 79 Delivery in a completely normal case
52 Chronic sinusitis 正常分娩
慢性副鼻腔炎 80 Other
53 Allergic rhinitis その他の妊娠、分娩及び産じょくの合併症 アレルギー性鼻炎 XII Diseases of the skin and Subcutaneous Tissue
54 Pneumonia 皮膚及び皮下組織の疾患
肺 炎 81 Infections of skin and Subcutaneous tissue
55 Influenza 皮膚及び皮下組織の感染
インフルエンザ 82 Others
56 Chronic bronchitis その他の皮膚及び皮下組織の疾患
慢性気管支炎 XIII Diseases of the Musculoskeletal System and 57 Asthma Connective Tissue
喘 息 筋骨格系及び結合組織の疾患
58 Other diseases of respiratory system 83 Rheumatoid arthritis and other inflammatory その他の呼吸系の疾患 polyarthropathies 慢性関節リウマチ(脊髄を除く) Ⅸ Diseases of the Digestive System 84 Osteoarthrosis and allied disorders
消化系の疾患 変形性関節症及び類似症
59 Diseases of teeth and supporting structures 85 Disorder of back
歯及び歯の支持組織の疾患 腰痛症
60 Gastric and duodenal ulcer 86 Other dorsopathies
胃及び十二指腸潰瘍 その他の脊柱疾患
61 Gastritis and duodenitis 87 Peripheral enthesopathies and allied syndromes
胃炎及び十二指腸炎 肩の障害
62 Appendicitis 88 Others
虫垂炎 その他の筋骨格系及び結合組織の疾患
63 Hemia and intestinal obstruction XIV Congenital Anomalies
腸閉塞及びヘルニア 先天異常
64 Liver cirrhosis 89 Congenital anomalies of heart
肝硬変 心臓の先天異常
65 Chronic liver disease 90 Congenital musculoskeletal deformities
慢性肝炎 先天性股関節脱臼
66 Other disorders of liver 91 Others
その他の肝の疾患 その他の先天異常
67 Cholelithiasis and gallbladder XV Certain Conditions Originating in the perinatal 胆石症及び胆のう炎 period 周産期に発生した主要病態
68 Other diseases of digestive system 92 Slow fetal growth and fetal malnutrition and その他の消化系の疾患 disorders relating to short gestation and Ⅹ Diseases of the Genitourinary System unspecified low birth weight
泌尿生殖系の疾患 胎児発育遅延、胎児栄養失調及び未熟児
69 Nephritis and nephrosis 93 Others
腎炎及びネフローゼ その他の周産期に発生した主要病態
70 Renal failure XVI Symptoms, Signs and Ill - defined Conditions
腎不全 症状、徴候及び診断名不明確の状態
71 Calculus of urinary system 94 Symptoms, signs and ill - defined conditions
泌尿系の結石 症状、徴候及び診断名不明確の状態
72 Other diseases of urinary system XVII Injury and Poisoning
その他の泌尿系の疾患 損傷及び中毒
73 Hyperplasia of prostate 95 Fracture
前立腺肥大炎 骨 折
74 Other disorders of male genital organs 96 Intracranial injury, intemal injury and injury to その他の男性生殖器の障害 nerves and spinal cord 脊髄を含む頭蓋内及び内部損傷 75 Menopausal and postmenopuusal disorders 97 Burns
月経障害及び閉経期の障害 熱 傷
76 Other disorders of breast and female genital organs 98 Poisoning by drugs, medicaments and biological 乳房及びその他の女性生殖器の疾患 substances 化学物質の有害作用
XI Complications of Pregnancy, Childbirth and the 99 Others
Puerperium その他の損傷及び中毒
妊娠、分娩及び産じょくの合併症 Important : No.79 with asterisk is not covored by social 77 Pregnancy with abortive outcome insurance
1. This form is used for claiming the social insurance benefit.
この様式は社会保険の給付の申請に使用されます。
2. This form should be completed and signed by the attending physician
この様式は担当医が書き、かつ署名してください。
3. One form for each month, one form for hospitalization / outpatient and home visit.
各月毎、入院・入院外毎に付この様式が1枚必要です。
Name of patient Date of Birth Sex (Male・Female)
生年月日 性別(男・女)
Date of First Diagno Days of Diagnosis and Treatment :
診療日数 days
Permanent Tooth 永久歯 Milky Tooth 乳歯
8 7 6 5 4 3 2 1 1 2 3 4 5 6 7 8 E D C B A A B C D E
8 7 6 5 4 3 2 1 1 2 3 4 5 6 7 8 E D C B A A B C D E
Services Tooth No. Fee Services Tooth No. Fee
診療内容 歯式 料金 診療内容 歯式 料金
1. Examination 8. Filling Amal. 1 serf.
診察 アマルガム 2 serf.
2. X-ray Bite-wings × 3 serf.
レントゲン 咬翼型 Comp. 診断 複合レジン 1 serf. Periapical × 2 serf. 標準型 3 serf. Panoramic × 面 パノラマ 9. Inlay / Onlay Models インレー・アンレー スタディモデル 10.Amal./Comp./ Build-up 3. Medication yes no アマルガム・複合レジンによる支台築造 投薬 Post c Core 4. Prophylaxies / Scaling メタルコア
歯垢 ← 歯石除去 11. Crown Porcelain / Gold
Fluoride 冠 ポーセリン・金
フッ化物塗布 Silver Alloy
5. Extraction 銀合金
抜歯 Other
6. Periodontal Scaling / Root planing その他 歯肉下歯石除去・根面平滑化 12. Bridge Work Abut
Gingival Curettage ブリッジ 支台歯 盲嚢掻爬 Pontic 7. Pulp Cap ダミー 歯髄覆罩 13. Plate Denture Pulpotomy 有床義歯 歯髄切断・抜髄 14. Other
Root Canal Therapy その他
根管治療 1 Canal
2 Canal 3 Canal
根管
Name and Address of Dentist / Office
担当医の名前及び住所
Title 称号:
Date 日付: Signature 署名:
Request to Attending Physician
担当医へのお願い
Attending Dentist's Statement
歯科診療内容明細書 患者名 初診日 Tooth Number 歯式 充填 合計 Name 名前 Address 住所 : Total Fee