-\twza\
eg
22tsee
8
e
464
--
471
e
(1995
ff)
Report
TheEffectiveness
of
Neurodevelopmental
Treatment
for
Motor
Impaired
Children*
Meta-Amalysis
for
aRetrospective
Study
KoichiHIRAOKA**
Abstract
The
purpose of thisstudy was todetermine
the effectiveness ofNeurodevelopmental
Treat-ment
(NDT)
forchildren with motor disabilities.Meta-analysis was used toestirnate theeffec-tiveness through reviewing previous studies.
Meta-analysis
is
a reratively new statistical method that allows us tofind
out overall effectiveness of a therapeuticintervention
throughreviewing
previous
research articles thatrelates totheissue.
The
effectiveness of thetherapeu-tic
intervention
isrepTesentedby
the effect size thatisdefined
as thedifference
between
the means of the experimental and the control groupdivided
by
the contror group standarddevia-tion.
I
estimated the effect size of thelong
term treatment through experimental studies whichhad published between 1985 and 1994
(Study
1).Furthermore, the short term effectiveness ofNDT
was estimated through studies thathad
publishedbetween
1970 and 1994,dealtwithim-mecliate effectiveness of NDT after one treatment session
(Study
2).The effect size of the Study 1was-O,
21,and of theStudy
2 was O.69.The results suggested thatNDT intervention wasnot predominant against other control conditions while
the
changes of performancesduring
short termNDT
interventionwas obvious.Key words Neurodevelopmental Treatment
(NDT),
Meta-analysis,Developmentaldisability
Introduction
Neuro-developmental
Treatment(NDT)
has
been
ene of the most popular ways totreatchildren with
the problems of motor
development,
such ascere-brai
palsy. However, the effects of the treatmentare controversial.
Many
researchers have failedto*
gyme:wntts#61eeests\eciinuta)imR
Meta-AnalysiseMVhkNemS}st
" School
of Physical and OccupationalTherapy,Hakone National Hospital
ytmade
-
:Nittsasptngeera[nlngpt
v/N lfvi- y . y\
M
ve\tstaeFF(+
2soreAJI[fiylxWMrtIMza
412)(9NE
1995E2
fi
6fi1eeveE 1995fiE
11fi
25H)prove
its
eMcacybecause
of their poor methodologiesi}.Piper2)
suggested that most ofthose studies
had
methodological problems such as alack
of control groups, sample size, outcomemeasures, and sample population.
Because
of these conditions, the effectiveness of NDT for childrenwith physical
disabilities
has notbeen
establishedas yet.
Glass6)
has established a way tointegrate
studiescalled "meta-analysis".
This
analysis allows usto
estimate the raagnitude of effectiveness throughadding up the outcomes of
the
studies. HeJapanese Physical Therapy Association
JapanesePhysicalTherapy Association
The
a strong conclusion on meta-analysis. The analysis
gives us an index which
is
calted effect size,Effect
size issimply calculated by subtracting means of
control group from means of experimental group
divided
by
standarddeviation
of control group.
There
is
a research that has used meta-analysisto estimate effectiveness of
NDT
intervention.
OttenbacherB) attempted to
investigate
effectivenessof
NDT
throughintegrating
studies ofNDT
inter-vention that had beenpublished
by
1984
usingmeta-analysis. He showed a magnitude of difference
of outcome
between
NDT and otherinterventions
in
his
study. This isthe onty study that havees-timated effect size of
NDT
intervention.
Despite his study, there
is
no research ones-timating effect size on studies that
investigates
theimmediate effectiveness of an
NDT
intervention.
However, itisa factthat many therapistshave
im-pliedefiicacy of immediate effectiveness of
NDT
in-tervention intheirclinical experience9)iO). DeGaltgii}
suggested the usefulness of the measurement of the short term changes of theperformance toprove the effectiveness of
NDT.
In
thisreport,I
investigated
the efficacy ofNDT
through reviewing previous results of the studies
in
order to determine how much NDT intervention was effective. Meta-analysis was used fores-timating that.
I
designed
two studies.One
was the study thatinvestigated
long
term effectiveness ofNDT,
and the other was the study that addressedto
find
out short term effectiveness ofNDT.
Method
I
referredto
the
latestresearch articles thathad
been
published from 1985 to1994 forStudy 1,and1970
to1994
for
Study
2.
The
reason Ididn't
search articles published
before
1985 for Study 1was that a previous study
I
mentionedbefore
had existedS) for the articles. The ways to search thestudies were on-line computer searches on Medline,
Cumulative Index toNursing and AlliedHealth
Lit-erature, and manual search on Index Medicus.
Effectivenessof
Neurodevelopmentai
Treatment forMotor ImpairedChildren
465
1. Studyl
In
Study
1,
I
gathered articles which metthe
fol-lowing
criteria.Fjrst,
theyhad
tobe
the articles ofthe efficacy of
NDT
treatment thatincluded
NDT
intervention,
Secondly,
theyhad
to address thetreatment of children with some kinds of physical
disabilities
such as cerebral palsy or Down'sSyn-drome. Thirdly, they had to have at least two
groups, a control group
that
wastreated
by
NDT and ano,ther group thatwas not treatedby
NDT orby
a reducedin
intensity
of theNDT
intervention.
Fourthly,
theyhad
tomeasure the effectiveness ofthe accumulation of more than one therapeutic
in-tervention. Finally, they had to have dependent
variables of at ]eastmean and standard deviation,
or F,or tso thatIcould calculate "effect
size".
2.
Study2
In
Study
2,
I
gathered articles that met thefol-lowing criteria.
First,
theyhad
tobe the articles ofthe efficacy of
NDT
treatment thatincluded
NDT
intervention. Secondly, they might address the
treatment of children with some physical
dis-abilities such as cerebral palsy or
down
syndrome.Thirdly,
the articles had tocornpare thefunctional
status of pre-treatrnentand post-treatment
measur-ing
theimmediate
carry-over effects of single NDT session. Finally,theyhad
tohave dependentvaria-bles
of at leastrnean and standarddeviation
or For tvalues so thatIcan calculate `teffect
size".
3,
Hypothesis
I
established ahypothesis
for
Study
1
thatNDT
intervention
had
alarge
advantage over the othereonditions. Also I established a hypothesis that
there was a short
term
effectiveness ofNDT
inter-vention for Study 2. For these hypetheses, I
as-sumed
that
both estimated effect sizes shouldbe
large.
4. Analysis
AsI
mentionedbefore,
I
used rneta-analysis te466
eeIittstaY
tiveness of NDT.
Control
grQups' scores were usedas the control conditions of
Study
1.
Pretest
scores were used as scores of a control condition inStudy2
because
theydidn't
have
a control condition.Al-though the way in Study 2 isnot the formaf way
for meta-analysis, it ispermissible to use
meta-analysis for single or multiple subject designs that don't have control groups. Because Glassii)said
that
experimentsthat
comprjsed only pretestingand pesttesting
in
a single group of subjects mightbe included
if
the treated group's members' preteststatus was a good estimate of theirhypothetical
post treatment status
in
the absence of treatmenLBecause
of thiscondition, effect size ofStudy
2 is supposed toshow the differenceinperformancebe-tween pre-test and post-test of each subject within a short term.
In order toavoid biased estimate of effect size,
effect size was multiplied
by
correctedfactor,
Alsoinorder toavoid
bias
of homogeneity, pooledesti-mate of variance was used
for
population variance.Weighted
mean was estimated so as toestimate the overall mean effect sizei2).I
summarized anexam-ple of the procedure estimating the effect size on
Appendix.
Results
Between 1985 and 1994,
there
were 11 studies which had investigated effects of NDT on childrenwith physical
disabilities.
Out
of the 11 studies,there were
6
experimental designed studies. Twostudies were excluded
from
the studiesbecause
oflack
of control group, and a study was excludedbe-cause of
lack
of description of standard deviation.Therefore,therewere
3
studies thatmet thecriteriaI had established forStudy 1.
Between
1970
ancl1994,
there were 20 studies whichhad
investigated
effects ofNDT
for
childrenwith physical disabilities.
Out
of the 20 studies,there were
7
studies investigating the short termeffectiveness of NDT. One study was excluded from
the studies
because
oflack
of control group, andthree studies were excluded
because
of lack ofde-eg
22geg
8e
scription of standard
deviation.
Therefore,
therewere
3
studies that met the criteriaI
had
tabilishedfor
Study
2.Studies
I
referred werelisted
onTable
1.
Ilistedindividualeffect size on Table 2.0verall
mean effect size in Study 1
ivas
-O.21.
0verallmean effect size in
Study
2
was O,69,The summaryof information of thestudies were listedon Tables
2
and3.
Discussion
As
I mentioned above, the resultin
Study 1 showed-O.21
of effect size.The
effect size issidered as small effect size according to
Cohents
criteria27). Cohen suggested that
.2
was consideredas small effect size,
.5
was considered as mediumeffect size which was largeenough tobe visible to
thenaked eye, and
.8
was the largeeffect size.
Accordingly,
Iconcludedthat
NDT
approach wasnot predominant or slightly
detrimental
againstother conditions. Therefore, the
hypothesis
for
Study 1 was rejected. In
Ottenbacher's
study,he
showed effect size of
NDT
intervention
asO.31,
which was
interpreted
as children who hadceived NDT performed slighLly betterthan children who hadn'treceived NDT.
The difference between the results of
Ottenbacher's
study andthe
study presented heremay
be
caused by differenttrends of the outcomeof the studies, Thirty-sixpercent of thestudies
sented after 1984 showed positive effectiveness of
NDT
while 56 percent of the studies presentedtween
1970
and1984
showed positive effectivenessaccording tothe 20 articles referred to inStudy 2.
That
implies
more negative trendis
predominantin
the
later
studies.
As
theresult ofStudy
2,I
had
O.69 of effect sizewhich was considered as a
large
effect size
ing
toCohen's
criteria.The
effect size suggestedthat NDT intervention causes children to perform
much better than they
did
on pre-interventionwithin a short period,Therefore,the
hypothesis
forJapanese Physical Therapy Association
JapanesePhysicalTherapyAssociation
The Effectivenessof
Neurodevelopmental
Treatment forMotor ImpairedChildren
Table 1. Research articles
that
relateto
NDT outcorne foryouth population467
ResearchersStudy#Year Subjects ResearchDesign MeasurementTools Wrighti3) 1973cerebralpalsy Experiment originalscores
Carlseni4)
1975cerebralpalsyExperiment
BayleyScate,DDST
Norton15) 1975multiple Singlesubjectfrequencyofbehavior
Rothmani6)
41978cerebralpalsySinglesubjectVC,PVC,PPVC,FEV
Avignoni7)
1981riskinfantsExperiment
physicalexaminationHarris9)
1981Down'sSyndromeExperiment
BayieyScaLe,PeabodyScaleSommerfeld5)
1981cerebralpalsy
Experiment
Wilsondeyelopmental
RefiexTest
WCISDGrossMotorEvaluation
ROMJenkinsia)
1982developmental disability Experirnent PeabodyscaleDeGangii)
1983cerebralpalsy ExperimentADLtest
Goodman19) 31985riskinfant Experiment
GriMth'smentaldevelopment
scale
Piper2)
1986riskinfant
Experiment
WoianskiGrossMotorEvalua-tionWilsonDevelopmentalReflex
Profile
Milaniscreeningtest
Griffth'sMentalDevelopment
Scale
Herdon20) 1987cerebralpalsy
QuasiExperiment
movementpatternPalmer2i) 11988cerebralpalsy Experiment
BayleyScale
Piper2Z)
1988riskinfants
QuasiExperiment
neurologicalsymptomsEdwards23)
1989Down'sSyndromeSinglesubjectBayleyScale
Lillyle)
1989cerebralpalsy
SinglesubjectADLtest
Srnelt24)
1989cerebralpalsy
SinglesubjectROMhandsurfacearea
Kluzik25)
5'I990cerebralpaLsy
SinglesubjectMovementTime(MT)
MovementUnits(MUs)
PercentageofMTofFirstMUs
Mayo4)
21991cerebralpalsy
Experiment
BayleyScale
Chakerian26)
61993cerebralpalsy
Singlesubjecthandtracingarea
'The
study numbers correspond tothe study numbers on Tables2and 3.
suggested that
NDT
intervention
made alarge
change
irr
perforrnance within a short terrnal-though the
NDT
intervention
might
notbe
significantlydifferent
from
other conditionsin
terms of
long
term
effectiveness.I
suppose that the reasonsI have had Iargeeffect sizein
Study
2
are thelength
of the period of the468
Table 2.
ve\tante}g
eg
22tseg
se
Summary
Informatien
for
theStudy
1
Study# rnean(E)
SD(E)
N(E) mean(C)SD(C)N
(C)ESWeighted
Corrected CorrectedSp Factor ES 1111112333333
49.1
65.6
67,8
47.9
67
67.5173.498
102
101 10196
9511.616.3
1918,918.423.299.411
20 10 12 13 1325252525252517202020202020
58.I75.572.563.375,376.6159.5
98
10298
9695
97 1914.918.22215.318.382.3
13
18 11 1613
1823232323232312202020202020
・-o.-o.-o.-o.-o.-o.
o.
o,
o,o.-o.
58632575494315oe29350813
15.5815.6518,6220,4416.99
2192.8112.0419,0210.5114.14
13 15.7O.98O
98O.98O,98O,98O.98O.97O.98O.98O.98O.98O.98O.98
-o.-o.-o.-o.-o.-o.
o.
o, o.o.-o.
57622574484351oo28350812ES=effectsize.
(E)=Experimentgroup,
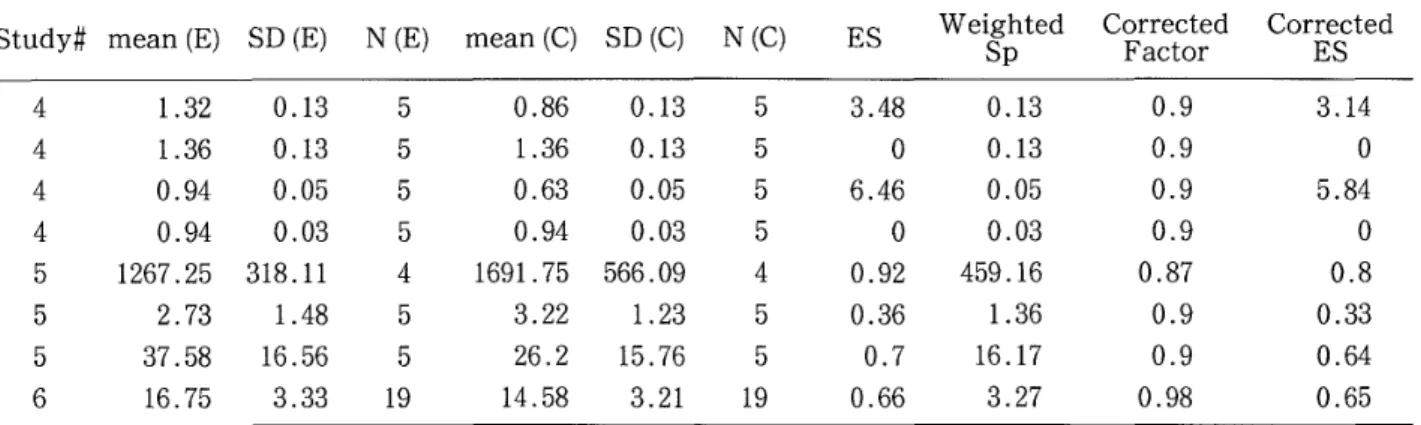
(C}=,-Controlgreup.N=Number ei samples,Table 3.Summary IRformation
for
theStudy
2Study#
rnean(E) SD(E) N(E) mean(C) SD(C)N(C)ESWeighted
Corrected
Corrected
Sp
Factor
ES
44445556 1.32 O.13 1.36O.13
O.94
O.05
O.94
O.03
1267,25
318.11
2.73 1.48 37.58 16.56 16.753.33
555545519 O.86O.13
1.36
O.13
O.63
O.05
O.94
O,03
1691.75 566,09 3.22 1.2326.2
15,7614.58
3.21
5555455193.48o6.46
oO.92O.36
O,7O.66 O,13O,13
O,05
O.03459.16
1,3616.17
3.27
O.9
O,9
O.9
O.9O,87 O.9O.9O.98
3,14
o5,84
o O.8O 33O.64O,65ES==effectsize.
(E)=Experiment
group.(C)=Control
group. "ESvalues in ES#5 and 6 are po$itivealthough means of
theexperimental groups subtracted by means of the centrol groups are negative. Becausethe negative values mean
posi-tiveresults inthose values.
can see on
Table
1,
100%
of studies that measure short Lerrn effectiveness ef NDT used evaluativemeasurements made
for
rneasuring the outcome oftreatments specifically. They measured
qualitative
changes of movements
based
on therapy's target specificity. Some therapists9)iO)haveproposed
utiliz-ing of measurement toolswhich are
based
onindi-vidual treatment goals.Parette28)said that a more
comprehensive assessment batteryadministered on
a pre-treatment/post-treatment
basis
may more ac-curately reflect the influence of therapeuticinter-vention. So,although there
is
no standardizedtest-ing to evaluate short term effectiveness of
treat-ment
for
children with cerebral palsy, measuringqualitativechanges of theirmovements must
be
a $ignificant way toevaluating the outcornes ofther-apeutlclnterventlon.
On
the otherhand,
other studies mainly useddi-agnostic measurernent tools,such as
Bayley
Scale
and
Peabody
scale, that may notbe
sensitiyeenough todetectthe outcomes of interventions.In
Study
1,67% of thestudies usedBayley
Scale
forthe assessment.
This
is
rnaclefor
discriminative
measure, and no responsiveness
data
has
been
pre-sented to establish the Bayley
Motor'
Scale
as an evaluative instrument29)30).stern3) said that theJapanese Physical Therapy Association
JapanesePhysicalTherapyAssociation
The Effectiyenessof
Neurodevelopmental
Treatmentfor
Motor ImpairedChildren
Table
4.The
Relationship
between
Opinions
on thestudy outcomesand the Length of the Intervention
469
<1 month1 <3 monthS-months3 monthsS <6 months6 monthsS PositiveEffectsNo
changes41
32
13 13 'Thenumerals intheblanksindicatethenumber ef research articles corresponding to thecolumns and thelines.
cause ef theobscure effectiveness of NDT
interven-tion is that rnost standardized scales, such as
Bayley
Scale,
didn'taccount forthe quality of themovement although measuring the qnality of
movement was the most
important
framework
in
determining
theimprovement
ot the motor per-formance. Lillyie)also said that the measurementcriteria used
in
those studies were not sensitiveenough to detect small changes occurring
due
toNDT,
Also,
length
of period of intervention isanimpor-tant
factor.
As you can see in Table 4, there isatrend that the results of
the
reports worsen asthe
length of period of treatment increases.Based on
that trend,Imay be able to
interpret
the result ofStudy 2 that I can see obvious predominancy of
NDT as lengthof periodof treatment
is
short.The limitationof thisstudy was small sample
size. Glassii}said that more studies are
better
thanfewer.
So,
the
number of studiesIreferred tofores-tirnationof effect size rnay weaken the conclusion
ofthisstudy.
APPENDIX
Showing an example of estimating effect size as follows,
The values described belowwas sited from the firstlineof
Table2.1.
Calculatingthe square root ef the weighted pooled
varlance i
(NE-1)SZ+(Nc-1)SZ
Weighted SP=V N,+Ncu2
v(25-1)IL62+(23-1)19.o2
25+23-2-15.58
2. Calculating theCorrectedFactor
3 CorrectedFactor=.'1-
--
4m-1 3 4(25+23-2)--1 =.O.98 'm=NE+Ncm2 3. CalculatingCorrectedEffectSizeEs=
g-:mC.
=
49.1-58.1=-o.ss
Sp 15.6CorrectedES
==
ES'Corrected Factor=:-O.58'O.98
==-O.57
References
1)DeGangi GA, Hurley L,et al,: Toward a methodology of the short-term effects of neurodevelopmental
rnent. Am JOccupTher 37
(7):
479-484. 1983,2)PiperMC, Kunos I,et aL: Early physical therapy
effects on the high-risk infact)A randomized trolledtriaLPediatrics78 (2):216-224, 1986.
3) Stern FM, Gorga D: Neurodevelopmentaltreatment
(NDT);
Therapeuticinterventionand itseMcacy.fantsand Young Children1
(1):
22-32,1988.4)Mayo NE: The effect of physicaltherapy for childre]
with motor delay and cerebral palsy; A randomized
clinical trial.Am jPhys Med Rehab 70
(5):
258-267,1991.
5)Sommerfeld D,FraserBA,etaL: Evaluationofphysical
therapy service for severely mentally impaired dents with cerebral palsy.Phys Ther 61
(3):
338-344,1981.
6)GlassGV: Meta-AnalysisinSocialResearch. Sage
lications,1981.
7)Thomas JR: RcsearchMethods in Physica} Activity.
Human KineticBeoks, 1990.
8)OttenbacherKJ,BioccaZ,et at.:Quantitativeanalysis
of the effectiveness of pediatrlctherapy; Emphasis en
the neurodevelopmental treatment approach. Phys
Ther 66 (7]:1095-1101,1986.
9)Harris RS: Effects of neurodeveloprnental therapy on motor performance of infantswith Down's syndrome.
Dev Med Child Neurol 23:477-q83, 1961.
10) LMy LA, Powell NJ: Measuring the effects of
neurodevelopmental treatment on the daily living
skills of 2 children with cerebral palsy. Am
J
OccupTher 44
<2):139-145,
1990.470
ve#tsza\
research. Review of Research in Education 5:351-379, 1977.
12) Themas JR,French KE: The use of meta-analysis in
exercise and sport] A tutorial.Res
Quart
ExerSport57(3):196-204, 1986.
13) Wright T, Nicholson J:Physiotherapy forthe spastic
ehild: an evaluation. Dev Med Child Neurol 15:
163,1973.
14) CarlsenPN: Comparison of two occupational therapy appreaches for treating the yeung cerebral palsied
child, Am JOccup Ther 29
{5):
267-272, 1975.15)NortenY:Neurodevelopment and sensory integratien. Am JOccup Ther29
(2):
93-100,1975.16)Rothman
JG:
Effectsof respiratory exercises on thevital capacity and forcedexpiratory volume in
dren with cerebral palsy,Phys Ther 58
{4):
421-525,1978.
17)Avignon M, Noren L,et al.: Earlyphysiotherapy Ad
Medum Veita or Bobath in infantswith suspected
neuromotor disturbance. Neuropediatr 12(3):232-241,
1981.
18)jenkinsRj:Effectsofdevelopmentaltherapy on rnotor impairedchildren. Phys Occup TherPediatr,2,4,1982, pp19-28.
19)Goodman M, Rothberg AD: Effect of early neurodevelopmental therapy in normal and aL risk survivors of neenatal intensivecare. Lancet14: 1330, 1985.
20)Herdon WA, Troup P,ei al.:Effects of mental treatrnent on movement patterns Df children with cerebral palsy.
J
PediatrOrthe 7(4):
395-400,1987.
21)Palmer FB,ShapjroBK,et al.: The effect$ of physical
therapy on cerebral palsy;A controlled trialin infants
ag
22
igee
8
-g
with spastic dip]egia.New Eng JMed 318
(13):
808,1988.22> Piper MC, Mazer B,et al.: Resolution of neurological symptoms in high-riskinfantsduring the firsttwo
years oflife.Dev Med ChildNeurol 30:26-35, 1988. 23) Edwards SJ,Yuen HK: An intervention program fora fraternaltwin with Down syndreme. Am
J
Occup Ther 44(5):
454--458,1990,24) Srne]tHR: Effect of an inhibitiveweight-bearing mitt on tene reducation and functionalperformance ina child with cerebral palsy.Phys Occup Ther Pediatr9
(2):
53--80,1989.25)Kluzik J:Quantificationof control; A preliminary
study of effects on neurodevelopmental treatment on reaching inchildren with spastic cerebral palsy.Phys
Ther 70
(2):
65--78,1990.26)ChakerianDL, LarsonMA: Effectsof upper-extremity
weight-bearing on hand-opening and prehension
terns inchildren with cerobral palsY.Dev Med Child
Neurol 35:216-229, 1993.
27)Cohen J:StatisticalPower AnalysisfortheBehavioral
Services.
Academic PressInc.1977.28)ParetteHP,Hourcade
JJ:
A review of therapeuticvention research on gross and finemotor progress in
young children withcerebral palsy,Am
J
Occup Ther38 (7):462-468, 1984.
29)Deyo RA: Teward cEinical apprications ef healthstatus measures: Sensitivity of scales toclinically important changes. Health ServiceResearch 19
{3)/
275-289,1984.
30) Rosenbaum PL, Russell DJ : Issues in measuring change in motor function in children with cerebral
palsy:A special communication. Phys Ther 70 (2)i125
Japanese Physical Therapy Association
Japanese Physioal Therapy Assooiation
The
Effectiveness
ofNeurodevelopmental
Treatment
for
Motor
Impaired
Children
471〈要 約 〉 運動障害児に対する神経 発 達 学的治療の効 果
一
Meta−Analysis
を用いた文 献 分 析一
平 岡 浩一
国立療 養所箱根 病院附属リハ ビ リテー
シ ョ ン学 院 理学 療法学 科 (〒250
神 奈川県小田原市風 祭412
) こ の研 究で は,
運 動 障 害 児に対する神 経 発 達 学 的 治 療 (NDT )の効 果につ い て検 討した。
過 去に発 表された神 経 発 達 学 的 治 療の効 果に関 する文 献 を もとに Meta−Analysis
を用い て全 体として の治 療 効 果の 大き さ を判定し た。 Meta−
Analysis は過去の研究論 文を 通し てある治療 介 人の効果を測定 する比 較的新しい統 計学的方法で ある。
その治 療 介 入の効 果は,
実 験群の 平均値か らコ ン トn一
ル群の 平均値 を減算し,
その値をコ ン トロー
ル 群の標 準偏差で除算し た数 値 (Effect
Size
)に よっ て表さ れ る。 1985年か ら1994年の間に発 表さ れ た 研究 論 文を も とにNDT
の 長 期 的 治 療 効 果 〔複 数 回 治 療の累 積 効 果 )にっ い て のEffect
Size
を算 出し た (研 究1
) 。 更にNDT
の短期的 治 療 効 果 (1
回 治療の直 接 効 果) にっい て 1970年か ら1994年の間に発 表さ れ た研 究 論 文を も とに Effect Sizeを算 出し た (研 究 2)。
研究1
お よび研 究2
の文献 採択 基準に合 致 する論 文 数は それぞれ 3であっ た。 長期 的 治療 効 果のEffect
Size
(研究 1)は一
〇.
21,
短 期 的治 療 効 果の Effect Size (研 究2)はO.
69であっ たQ 本研究の結果よ り, 運動障害児に対する神経発 達学的治療は
,
短 期 的 効 果は認め ら れ る が, 長期 的に は他の治療介 入と 比較して ほ ぼ同 等