第 79 回日本感染症学会総会学術講演会座長推薦論文
侵襲性肺炎球菌感染症の小児から分離された Streptococcus pneumoniae の血清型と耐性遺伝子の検討
1)旭川厚生病院小児科,2)北里大学北里生命科学研究所感染情報学研究室
坂田 宏
1)生方 公子
2)千葉菜穂子
2)(平成 17 年 9 月 22 日受付)
(平成 17 年 11 月 16 日受理)
Key words : Streptococcus pneumoniae , invasive infection, serotype, child
要 旨
1998 年 8 月から 2005 年 7 月までの 7 年間に,侵襲性肺炎球菌感染症の小児の血液または髄液培養から検
出された Streptococcus pneumoniae 46 株について血清型と耐性遺伝子を検討した.患者の年齢は生後 2 カ月
から 9 歳の範囲で 1 歳以下の児は 36 名(78.3%)であった.臨床診断名は肺炎が 16 名(34.8%),occult bac- teremia が 15 名(32.6%),髄膜炎が 8 名(17.4%),上気道炎が 6 名(13.0%),関節炎が 1 名(2.2%)であっ た.最も多い血清型は 6B で 18 株(39.1%),ついで 23F が 8 株(17.4%),6A と 19F が 4 株(8.7%)であっ た.7 価の肺炎球菌ワクチンに含まれる血清型は 70% 以上を占めていた.
耐性遺伝子 1 個所に変異があるのは 15 株(32.6%),2 個所に変異があるのは 10 株(21.7%),3 個所に変 異がある,いわゆる penicillin resistant S. pneumoniae(PRSP)は 18 株(39.1%)であった.PRSP は 6B,
23F,6A の 3 つの血清型で認められ,それぞれの血清型の 55.6%,62.5%,75.0% であった.
〔感染症誌 80:91〜96,2006〕
はじめに
Streptococcus pneumoniae は小児において髄膜炎,
肺炎,中耳炎などの疾患の主要な原因菌である.中で も,髄膜炎,菌血症,肺炎,関節炎,腹膜炎は侵襲性 肺炎球菌感染症(invasive pneumococcal infection,
IPI)として一つの疾患単位としてまとめられること が多い.近年は,従来抗菌活性を有していた penicillin 系あるいは cephem 系抗菌薬に感受性が低下した S.
pneumoniae が著しく増加し,臨床の場で大きな問題
になっている.米国では本菌による感染症の発症を抑 制するために,S. pneumoniae に対するワクチンを接 種している.主に小児に対して用いられるのは 4,6B,
9V,18C,19F,22,23F の 7 種の血清型に対するワ クチン(7-valent pneumococcal conjugate vaccine,
PCV7)である.本邦では,現在このワクチンの小児 における臨床試験が進行中であり,早期の導入が期待 されている状況にある.著者は以前に,北海道道北地 区の IPI の発生頻度を人口 10 万人あたり 5 歳未満で
35.5,2 歳未満では 61.4 で,米国より低いがほぼヨー ロッパ諸国と同程度と推測している
1)が,PCV7 の導 入前の状況として,IPI の児から分離された菌の血清 型と耐性遺伝子を疫学的に調査しておく必要性を感じ たの,当院で保存していた株を用いて検討したので報 告する.
対象及び方法
1998 年 8 月 か ら 2005 年 7 月 ま で の 7 年 間 に,IPI の小児の血液または髄液培養から検出された S. pneu-
moniae 46 株を対象とした.46 株のうち当院に入院し
た患者から分離された菌が 21 株,北海道内の 9 つの 小児科施設から送っていただいた菌が 25 株であっ た.これらの株は検査まで凍結乾燥保存していた.
ペニシリン結合蛋白(penicillin binding protein,
PBP)遺伝子は PCR キットであるペニシリン耐性肺 炎球菌遺伝子検出試薬(湧永製薬)で解析を行った.
その結果に基づいて生方らの分類
2)により penicillin resistant S. pneumoniae(PRSP),penicillin interme- diate-resistant S. pneumoniae(PISP),penicillin sus- ceptible S. pneumoniae(PSSP)に分類した.以下の
原 著別刷請求先:(〒078―8211)旭川市 1 条通24 丁目
旭川厚生病院小児科 坂田 宏
Fig.1 Relationship between age and clinicaldiagnosis in patients with an invasive pneumo- coccalinfection
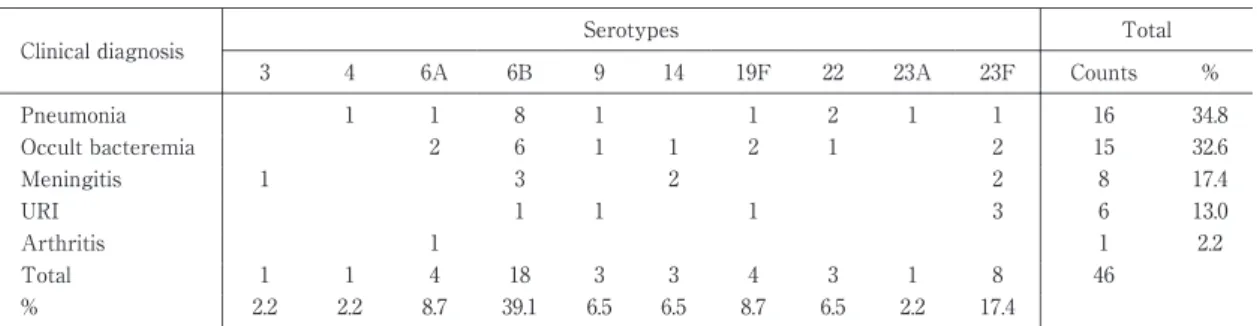
Table 1 Relationship between serotypes and invasive pneumococcalinfectious disease Total Serotypes
Clinicaldiagnosis
% Counts 23F
23A 22 19F 14 9 6B 6A 4 3
34.8 16
1 1 2 1 1
8 1 1 Pneumonia
32.6 15
2 1
2 1 1 6 2 Occult bacteremia
17.4 8
2 2
3 1
Meningitis
13.0 6
3 1
1 1 URI
2.2 1
1 Arthritis
46 8
1 3 4 3 3 18 4 1 1 Total
17.4 2.2 6.5 8.7 6.5 6.5 39.1 8.7 2.2 2.2
%
Table 2 Relationship between serotypes and mutation ofpbpgenes
Total Serotypes
Abnormalpbpgene
% Counts 23F
23A 22 19F 14 9 6B 6A 4 3
39.1 18
5 10
3 1a,2x,2b
6.5 3
1 2
1a,2x
15.2 7
3 1 1
2 2x,2b
32.6 15
3 3 1 2 4 1 1
2x
6.5 3
1 1 1
normal
Table 3 Relationship between serotypes and macrolide resistance genes
Total Serotypes
Macroride resistance
genes 3 4 6A 6B 9 14 19F 22 23A 23F Counts %
2.2 1
1 mefA,ermB
26.1 12
1 3
1 3
3 mefA
30.4 14
1 1
3 9 1
ermB
41.3 19
6 3
1 1 6
1 1 none
文中では遺伝子解析により耐性を判定した株は(g)
を略称の後に記した.血清型は Pneumococcal antisera
(Statens Serum Institute,Copenhagen,Denmark)
で判定した.なお 1998 年から 2001 年の株の一部は既 報
3)で血清型を報告したが,その際の血清型は肺炎球
て判別しており,6A と 6B などの分類ができていな かったので,今回あらためて再検査を行い成績に加え た.
成 績
46 株を分離した患者の年齢と疾患をFig. 1に示し
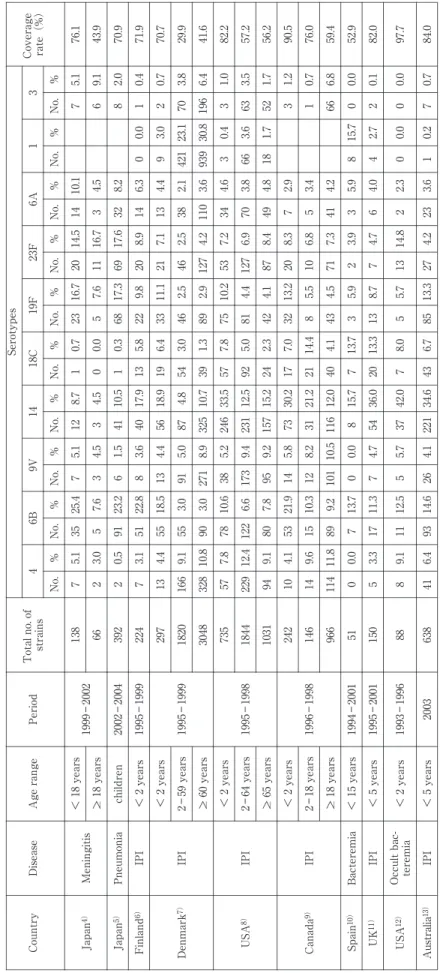
Table 4 Main studies of serotype and invasive pneumococcal infectious disease Coverage rate(%)
Serotypes Total no. of strainsPeriodAge rangeDiseaseCountry316A23F19F18C149V6B4 %No.%No.%No.%No.%No.%No.%No.%No.%No.%No. 76.15.1710.11414.52016.7230.718.7125.1725.4355.17138 1999―2002<18 years MeningitisJapan4) 43.99.164.5316.7117.650.004.534.537.653.0266>_ 18 years 70.92.088.23217.66917.3680.3110.5411.5623.2910.523922002―2004childrenPneumoniaJapan5) 71.90.410.006.3148.9209.8225.81317.9403.6822.8513.172241995―1999<2 yearsIPIFinland6) 70.70.723.094.4137.12111.1336.41918.9564.41318.5554.413297 1995―1999
<2 years IPIDenmark7)29.93.87023.14212.1382.5462.5463.0544.8875.0913.0559.116618202―59 years 41.66.419630.89393.61104.21272.9891.33910.73258.92713.09010.83283048>_ 60 years 82.21.030.434.6347.25310.2757.85733.52465.23810.6787.857735 1995―1998
<2 years IPIUSA8)57.23.5633.6663.8706.91274.4815.09212.52319.41736.612212.422918442―64 years 56.21.7521.7184.8498.4874.1422.32415.21579.2957.8809.1941031>_ 65 years 90.51.232.978.32013.2327.01730.2735.81421.9534.110242 1996―1998
<2 years IPICanada9)76.00.713.456.8105.5814.42121.2318.21210.3159.6141462―18 years 59.46.8664.2417.3714.5434.14012.011610.51019.28911.8114966>_ 18 years 52.90.0015.785.933.925.9313.7715.780.0013.770.00511994―2001< 15 yearsBacteremiaSpain10) 82.00.122.744.064.778.71313.32036.0544.7711.3173.351501995―2001<5 yearsIPIUK11) 97.70.000.002.3214.8135.758.0742.0375.7512.5119.18881993―1996<2 yearsOccult bac- teremiaUSA12) 84.00.770.213.6234.22713.3856.74334.62214.12614.6936.4416382003<5 yearsIPIAustralia13) IPI:invasive pneumococcal infection Blank:no description in report
歳 が 14 名(30.4%)で あ り,1 歳 以 下 の 児 は 36 名
(78.3%)であった.最年少は生後 2 カ月,最年長は 9 歳であった.臨床診断名は肺炎が 16 名(34.8%)(中 耳炎の合併 3 名を含む),occult bacteremia が 15 名
(32.6%),髄膜炎が 8 名(17.4%),咽頭・扁桃炎が 6 名(13.0%)(中耳炎の合併 2 名を含む),関節炎が 1 名(2.2%)であった.
Table 1に疾患と血清型を示したが,最も多い血清 型 は 6B で 18 株(39.1%),つ い で 23F が 8 株
(17.4%),6A と 19F が 4 株(8.7%)ず つ,3,9,22 が 3 株(6.5%)ずつであった.血清型と疾患との間に関 連性は得られなかった.
Table 2に pbp 遺伝子変異と血清型を示した.1 個 所に変異がある PISP(g)は 15 株(32.6%),2 個所 に変異がある PISP(g)は 10 株(21.7%),PRSP(g)
は 18 株(39.1%)であり,変異がな い PSSP(g)は 3 株(6.5%)にすぎなかった.PRSP(g)は 6B,23F,6 A の 3 つの血清型で認められ,それぞれの血清型の 55.6%,62.5%,75.0% を占めていた.Table 3に Maclo- ride 耐性を示したが,mefA と ermB 両者を保有する 株 が 1 株(2.2%),mefA が 11 株(23.9%),ermB が 15 株(32.6%)であった.
考 案
S. pneumoniae の血清型は 90 種類に達するが,IPI を起こす血清型はその半数以下に限られている.Ta- ble 4に 6 型を PCV7 に含まれる 6B と含まれていない 6A に 分 け て 血 清 を ま と め て い る 2001 年 以 降 の 報
告
4)〜13)を示した.デンマーク
7),米国
8),カナダ
9)から
の報告は年齢別でも検討しているが,小児と成人では 血清型の頻度は大きく異なっていた.本邦でも Ubu- kata ら
4)は小児の髄膜炎では 6B,19F,23F,6A,14 が多く,成人では 23F,22,3,10,6B,19F が多かっ たとしている.米国
8),カナダ
9),オーストラリア
13)の 成績では小児は 14 がほぼ 3 分の 1 を占めて最も多い が,本邦
4)5)やフィンランド
6)では 10 から 20% 程度と やや少なく 6B が最も多いというように国によって多 少の差が認められた.小児における IPI の原因である S. pneumoniae の血清型における PCV7 に含まれる型 の比率(cover 率)は,例数が少ないスペイン
10)を除 いて,各国とも 2 歳未満では 70% 以上に達していた.
成人
7)〜9)では,原因菌の血清型の頻度は小児とは異な
るため,cover 率は 60% 以下であった.著者の成績 では,9 の 3 株が 9V かどうか判定できなかったので,
3 株すべてが 9V とすると cover 率は 80.4%,すべて が異なっていれば 73.9% となり,Ubukata らの報告
4)5)と同程度であった.
PCV7 導入後の疫学的調査効果として米国では 2 歳
入前の 1998 から 1999 年までの平均が 188.0 であった のに対し,導入後の 2001 年には 5.0 まで有意に低下 した
14).PCV7 に含まれている 7 つの血清 型 に 限 る と,導入前が 156.1 であったのが導入後には 33.6 まで 低下し,個々の血清型すべてで有意に発生率は減少し ていた.PCV7 には含まれていないが 6A や 9A など 関連した型では導入前に 19.6 であったのが導入後に は 9.8 と同様に低下しており,これらの型にもワクチ ンは有効と考えられた.ワクチンに含まれていない血 清型では反対に導入前 12.4 から導入後 15.7 に増加し ていた.別の報告
15)では導入前の 1994 年から 2000 年 までの生後 24 カ月以下の IPI の発生率が,2001 年で は 58%,2002 年 で は 66% 減 少,血 清 型 で は PCV7 に含まれる株では 2001 年に 63%,2002 年に 77% 減 少したが,含まれていない型で 2001 年 28%,2002 年 66% 増加していて,血清型としては 3,15,33 で増 加が顕著であった.
PCV7 を接種した児における IPI の発生率を Hsu
16)が報告している.67 名の 2 歳未満の IPI の小児の中 で,PCV7 に含まれている血清型によるものは 15 名 おり,5 名がワクチンを 3 回以上接種していた児で,
10 名が不完全接種か接種していない児であった.ワ クチンに含まれていない型によるものは 38 名で,う ち 30 名がワクチンを 3 回以上接種していた.母集団 が不明なので,ワクチンの vaccine failure の比率は 算定できないが,他のワクチン同様,血清型が合致し ていても failure はある程度起こりうることが示され ている.PC7 を 3 回以上接種しても IPI に至った 5 名 のうち 2 名は呼吸疾患や心疾患という基礎疾患があっ た児で,基礎疾患のある児で vaccine failure の可能 性が高いことが推測された.
血清型と耐性遺伝子の関係では,Ubukata ら
3)は,
血清型によって耐性遺伝子の保有率には差が認めら れ,10 株以上検出された血清型の中で 19F はすべて PRSP(g),6A は 42.9%,6B は 45.8%,23F は 70.0%
と高かった.著者の成績でも,PRSP(g)は 6B,6A,23 F の 3 種の血清型のみで認められていた.6B と 23F は PCV7 に含まれている型であり,治療に難渋する 事が多い PRSP(g)による IPI が PCV7 接種によっ て減少できれば,その恩恵は大きいと考えられる.ま
た,S. pneumoniae による市中感染の多発例の報告も
認められるが,血清型は 4 や 14 が多く
17),この点か らも PCV7 の有用性が期待される.
なお,本論文の内容の一部は,第 79 回日本感染症学会
(2005 年,名古屋)にて口演した.
謝辞:S.
pneumoniae
の株を提供していただいた当院を はじめ千歳市立病院,函館赤十字病院,札幌徳洲会病院,紋別病院,市立稚内病院,赤平市立病院の各病院の小児科 医師および細菌検査技師の皆様に深謝いたします.
文 献
1)坂田 宏:小児にお け る
Streptococcus pneumo- niae
菌血症の臨床疫学的検討.感染症誌 2005;79:1―6.
2)生方公子,小林玲子,千葉菜穂子,長谷川恵子,
紺野昌俊:本邦において 1998 年から 2000 年の 間に分離された
Streptococcus pneumoniae
の分子 疫学解析 肺炎球菌等による市中感染症研究会 収集株のまとめ.日化療会誌 2003;51:60―70.3)坂 田 宏:小 児 の 髄 液・血 液 か ら 分 離 さ れ た
Streptcoccus pneumoniae
の penicillin 結合蛋白遺 伝子変異と薬剤感受性.日化療会誌 2002;50:143―6.
4)Ubukata K, Chiba N, Hasegawa K, Kobayashi R, Iwata S, Sunakawa K:Antibiotic susceptibility in relation to penicillin-binding protein genes and serotype distribution of
Streptococcus pneu- moniae
strains responsible for meningitis in Ja- pan, 1999 to 2002. Antimicrob Agents Che- mother 2004;48:1488―94.5)Chiba N, Kobayshi R, Hasegawa K, Morozumi M, Nakayama E, Tajima T,
et al.:Antibiotic su-
sceptibility according to genotype of penicillin- binding protein and macrolide resistance genes, and serotype ofStreptococcus pneumoniae
iso- lates from community-acquired pneumonia in children. J Antimicrob Chemother 2005;56:756―60.
6)Hanage WP, Kaijalainen TH, Syrjanen RK, Au- ranen K, Leinonen M, Makela PH,
et al.:Inva-
siveness of serotypes and clones ofStreptococcus pneumoniae
among children in Finland. Infect Immun 2005;73:431―5.7)Konradsen HB, Kaltoft MS:Invasive pneumoc- occal infections in Denmark from 1995 to 1998 : epidemiology, serotypes, and resistance. Clin Di- agn Lab Immunol 2002;9:358―65.
8)Robinson KA, Baughman W, Rothrock G, Bar- rett NL, Pass M, Lexau C,
et al.:Epidemiology
of invasiveStreptococcus pneumoniae
infections in the United States, 1995-1998. Opportunities for prevention in the conjugate vaccine era.JAMA 2001;285:1729―35.
9)Jette LP, Delage G, Ringuette L, Allard R, De Wals P, Lamothe F,
et al.:Surveiilance of inva-
sive
Streptococcus pneumoniae
infection in the province of Quebec, Canada, from 1996 to 1998:Serotype distribution, antimicrobial sus- ceptibility, and clinical characteristics. J Clin Mi- crobiol 2001;39:733―7.10)Perez A, Sala P, Gimenez M, Sierra M, Esteve A, Alonso A,
et al.:Pneumococcal
bacteremia in children : an 8-year review in two hospitals in Barcelona. Eur J Clin Microbiol Infect Dis 2004;23:677―81.11)Brueggemann AB, Griffiths DT, Meats E, Peto T, Crook DW, Spratt BG:Clonal relationship between invasive and carriage
Streptococcus pneumoniae
and serotype-and clone-specific dif- ferences in invasive disease potential. J Infect Dis 2003;187:1424―32.12)Alpern ER, Alessandrini EA, McGowan KL, Bell LM, Shaw KN:Serotype prevalence of occult pneumococcal bacteremia. Pediatrics 2001;
108:E23.
13)Watson M, Roche P, Bayley K, Bell JM, Colli- gnon P, Gilbert GL,
et al.:Laboratory surveilla-
nce of invasive pneumococcal disease in Austra- lia, 2003-predicting the future impact of the uni- versal childhood conjugate vaccine program.Commun Dis Intell 2004;28:455―64.
14)Whitney CG, Farley MM, Hadler J, Harrison LH, Bennett NM, Lynfield R,
et al.:Decline in inva-
sive pneumococcal disease after the introduc- tion of protein-polysaccharide conjugate vaccine.N Engl J Med 2003;348:1737―46.
15)Kaplan SL, EO Mason Jr, Wald ER, Shutze GE, Gradley JS, Tan TQ,
et al.:Decrease of invasive
Pneumococcal infections in children among 8 childrenʼs hospitals in the United States after the introduction of the 7-valent pneumococcal conjugate vaccine. Pediatrics 2004;113:443―9.
16)Hsu K, Pelton S, Karumuri S, Heisey-Grove D, Klein J, Massachusetts Department of Public Health Epidemiologists:Population-based sur- veillance for children invasive Pneumococcal disease in the era of conjugate vaccine. Pediatr Infect Dis J 2005;24:17―23.
17)Hausdorff W, Feikin DR, Klugman K:Epidemi- ological differences among pneumococcal sero- types. Lancet Infect Dis 2005;5:83―93.
Serotype Distribution and Penicillin-Binding Protein Genes of Streptococcus pneumoniae in Children with Invasive Pneumococcal Infection
Hiroshi SAKATA
1), Kimiko UBUKATA
2)& Naoko CHIBA
2)1)Department of Pediatrics, Asahikawa Kosei Hospital,2)Kitasato Institute for Life Science and Graduate School of Infection Control Science, Kitasato University