Effect of lnjection Pressure of Subperiosteal
Infiltration Anesthesia on Local Anesthetic
Infiltration to the Jawbone
Division of Systemic Management,
Department of Oral Function,
Ohu University Graduate School of Dentistry
Kenji Yoshida
{Director Shinya Yamazaki)
骨 膜 下 浸 潤 麻 酔 の 注 入 圧 が
顎 骨 へ の 局 所 麻 酔 浸 潤 に 与 え る 影 響
奥 羽 大 学 大 学 院 歯 学 研 究 科 口 腔 機 能 学 領 域 生 体 管 理 学 専 攻
吉 田 健 司
指 導 教 員:山 崎 信 也
Abstract
To obtain a high infiltration anesthesia effect, concentration of local anesthetic in the jawbone must be increased. In dentistry however, low‑pressure injection is
recommended for subperiosteal infiltration anesthesia in order to reduce pain experienced by the patient. Currently, no studies regarding the injection pressure and infiltration anesthesia have been observed, and a standard injection pressure has not been clearly determined. Hence, the effect of injection pressure of subperiosteal infiltration anesthesia on local anesthetic infiltration to the jawbone was considered by directly measuring of lidocaine concentration in the jawbone.
Japanese white male rabbits were used as test animals. After inducing general anesthesia with oxygen and sevoflurane, cannulation to the femoral artery was
performed and arterial pressure was continuously recorded. Subperiosteal infiltration anesthesia was performed by injecting O.5 mL of 2% of lidocaine containing 1/80 ,000 adrenaline, and injection pressure was monitored by pressure transducer for 40 seconds.
After a specified time interval(10,20,30,40,50 and 60 minutes) , jawbone and blood samples were collected, and the concentration of lidocaine at each time interval was measured. The mean injection pressure was divided into four groups 100土50mmHg , 200土50mmHg, 300±50mmHg, and 400±50mmHg, and comparison statistical analysis was performed.
No significant change in blood pressure during infiltration anesthesia was observed in any of the four groups. Lidocaine concentration in blood and the jawbone was highest 10minutes after the infiltration anesthesia in all four groups, and decreased thereafter . Lidocaine concentration in the jawbone increased as injection pressure increased , while lidocaine concentration in blood showed a significantly lower value. This suggests that , when injection pressure of subperiosteal infiltration anesthesia is low, infiltration of local anesthetic to the jawbone may be more difficult, while transfer to oral mucosa and blood may be easier.
Key words : infiltration anesthesia, local anesthesia, jawbone, injection pressure , lidocaine concentration
和 文 抄 録
高 い 浸 潤 麻 酔 効 果 を 得 る た め に は,顎 骨 内 の 局 所 麻 酔 薬 の 濃 度 を 高 め る 必 要 が あ る 。 一 方 で,歯 科 に お け る 骨 膜 下 浸 潤 麻 酔 は,患 者 へ の 痛 み を 軽 減 さ せ る た め に,低 圧 注 入 が 推 奨 さ れ て い る が,注 入 圧 と 浸 潤 麻 酔 効 果 に 関 す る 研 究 が 認 め ら れ な い た め,注 入 圧 の 基 準 は 明 ら か に な っ て い な い 。 そ こ で,骨 膜 下 浸 潤 麻 酔 の 注 入 圧 が,局 所 麻 酔 薬 の 顎 骨 へ の 浸 潤 に ど の よ う な 影 響 を 与 え る か に つ い て,顎 骨 内 の リ ド カ イ ン 濃 度 を 直 接 定 量 す る こ と で 検 討 し た 。
実 験 動 物 と し て 日 本 白 色 系 雄 性 兎 を 用 い,酸 素,セ ボ フ ル ラ ン で 全 身 麻 酔 導 入 後,大 腿 動 脈 に カ ニ ュ レ ー シ ョ ン を 行 い,浸 潤 麻 酔 時 の 動 脈 圧 の 変 動 を 連 続 的 に 記 録 し た 。 下 顎 骨 に8万 倍 希 釈 ア ド レ ナ リ ン 添 加2%リ ド カ イ ン 0.5mLを 圧 ト ラ ン ス デ ュ ー サ ー に て 注 入 圧 を モ ニ タ ー し
な が ら40秒 間 で 骨 膜 下 浸 潤 麻 酔 を 行 っ た 。一 定 時 間(10, 20,30,40,50,60分)後 に 顎 骨 お よ び 血 液 を 採 取 し , そ れ ぞ れ の リ ド カ イ ン 濃 度 を 測 定 し た 。 平 均 注 入 圧 を 100±50mmHg, 200±50mmHg, 300±50mmHg, 400±50mmHg の4群 に 分 類 し 比 較 統 計 を 行 っ た 。
浸 潤 麻 酔 時 の 血 圧 変 動 は4群 と も に 有 意 差 は な か っ た ° 血 中 リ ド カ イ ン 濃 度 と 顎 骨 内 リ ド カ イ ン 濃 度 は4群 と も に 浸 潤 麻 酔10分 後 に 最 高 と な り,そ の 後 低 下 し た 。 注 入 圧 が 高 い 条 件 ほ ど,顎 骨 内 リ ド カ イ ン 濃 度 は 有 意 に 高 く, 逆 に,血 中 リ ド カ イ ン 濃 度 は 有 意 に 低 い 値 を 示 し た 。 骨 膜 下 浸 潤 麻 酔 の 注 入 圧 が 低 い 場 合,局 所 麻 酔 薬 は 顎 骨 内 に 浸 潤 し に く く,口 腔 粘 膜 や 血 中 へ 移 行 し や す い 可 能 性 が 示 唆 さ れ た 。
キ ー ワー ド:浸 潤 麻 酔,局 所 麻 酔,顎 骨,注 入圧,リ ドカ イ ン濃 度
Introduction
To obtain a high infiltration anesthesia effect, concentration of local anesthesia in the jawbone must be increased1). In dentistry however, low‑pressure injection is recommended for subperiosteal infiltration anesthesia in order to reduce pain experienced by the patient2). In clinically performed dental and oral surgical treatment including the removal of impacted teeth and oral implant surgery, surgery is performed by elevating the periosteum and washing it with saline. The effective clinical infiltration anesthesia time in such surgery has been reported to be short3). Even in experiments on rabbits, the effect of infiltration anesthesia and local anesthetic concentration in the
jawbone has been reported to be significantly impaired when the periosteum is elevated and washed with saline in comparison to cases where the periosteum is not elevated4) Consequently, a higher infiltration anesthesia effect is needed during surgery on the
jawbone, and there are some studies on infiltration of local anesthetic to the jawbone. In experiments on rabbits, infiltration anesthesia to attached gingiva, rather than alveolar mucosa, has been reported to have more significant infiltration of local anesfihesia to
jawbone, higher analgesic effect, and a longer effective duration5). For oral implant placement surgery commonly performed on aged persons with hypertension, etc., a stronger local anesthetic effect and longer effective duration would be safer and more advantageous6,7). While there are some studieson injection pressure of subperiosteal infiltration anesthesia to jawbone focus on injection and pain , which report that low
pressure injection is recommended to reduce patient pain2), studies on injection pressure and infiltration anesthesia have not been observed. As a result, a standard injection
pressure for infiltration anesthesia has not been clearly determined. Hence, this study considered the effect of injection pressure of subperiosteal infiltration anesthesia on lidocaine concentration in the jawbone.
Materials and Methods 1.Animals
Japanese white rabbits(n=144, body weight:2.66±0.3 kg,16 weeks of age, male) (Nippon Bio‑Supp. Center, Tokyo, Japan)were used. Animals were kept in a controlled
animal room at 23°C and 60%humidity, and given free access to pellets(MF , Oriental Yeast, Tokyo, Japan)and drinking tap water until the experiment day . This study was
performed in accordance with the Animal Experiment Regulations of Ohu University (Permit No.2013‑52,2014‑28}.
2.General anesthesia and experimental model
General anesthesia was induced by oxygen SL/minute and 5%sevoflurane using anesthesia equipment for small animals(Soft Lander, Shin‑Ei Industries , Tokyo, Japan), and then a tracheotomy was performed, after which general anesthesia was maintained at oxygen 3 L/minute and 3%sevoflurane. A cannula was inserted into the femoral artery, and arterial pressure was continuously recorded throughout the experiment using a polygraph(Sanei Sokki, Tokyo, Japan)and a pressure transducer
(Nihon Kohden, Tokyo, Japan)(Figure 1).
3.Infiltration anesthetic injection and excision of jawbone
Under general anesthesia, using quantitative electric injector (Cartri‑Ace, Dentronics, Tokyo, Japan)with injection needle(27G,0.40×19)(TERUMO NEEDLE , TERUMO, Tokyo, Japan),0.5 mL of 2%of lidocaine containing 1/80,000 adrenaline
(dental xylocaine cartridge containing 1/80,000 adrenaline, Dentsply Sankin, Tokyo, Japan)was injected into the right maxillae, for 40 seconds. Injection pressure was measured using a pressure transducer by connecting Terufusion , a T shape stopcock
{TERUMO Corporation, Tokyo)between Cartri‑Ace, an electric inj ector for dental anesthesia, and the injection needle. Subperiosteal infiltration anesthesia was determined to be performed with the gingivobuccal fold of the molar buccal region side of the right lower jawbone set as the injection site by attaching the needle tip to the
jawbone(Figure 2). Next, after a specified time interval(10,20,30,40,50 and 60 minutes), the periosteum was elevated, and the jawbone was removed using bone cutting forceps. The collected bone was preserved frozen at‑80°C .
4.Measurement of the mean arterial pressure before and after injection of local anesthesia
Since arterial blood pressure changes due to pain and adrenaline contained in local anesthesia, even while under general anesthesia8), change in blood pressure during
infiltration anesthesia was measured. Arterial blood pressure was recorded by polygraph , through cannulation of femoral artery via pressure transducer . From the polygraphic arterial pressure data,1/3 pulse pressure added diastolic arterial pressure was calculated as the mean arterial pressure(MAP), and changes in arterial pressure were assessed 10 and 20 seconds after infiltration anesthesia of 2%lidocaine with 1:80 ,000 adrenaline.
5.Measurement of the blood lidocaine concentration
Subperiosteal infiltration anesthesia was performed, and 3mL blood sample was collected after the specified time interval(10,20,30,40 ,50 and 60 minutes). The sample was separated into individual plasma components by centrifuge , and blood lidocaine concentration was measured by the enzyme multiplied immunoassay technique(EMIT)method9‑1 1).
6.Measurement of lidocaine concentration in the jawbone
Bone and mucosa samples which were frozen were ground using a bone mill (TK‑CM20S, Tokken, Tokyo, Japan), suspended with O.01 M boric acid at pH 9.18, and homogenized for 2 minutes using a homogenizer(POLYTRON PT2100
, Kinematica, Switzerland). The supernatant(0.5 mL)was combined with 100オL mexiletine(10オg/mL)and then 5 mL of chloroform:methanol(8:2) . After mixing, the solution was centrifuged at 3,000 rpm(1,000 G}for 10 minutes , and 3 mL of the organic layer was collected and dried under a reduced pressure at 40°C for 60 minutes using a rotary evaporator(EYELA, Tokyo Rikakikai, Tokyo , Japan). The sample was then dissolved in 250オL of the mobile phase(50 mM KH2PO4:CH3CN=4:1) , stirred using a mixer, filtered, and applied to high‑performance liquid chromatography
(HPLC}(Jasco PU‑2080 Plus, JASCO, Tokyo, Japan}to measure the jawbone lidocaine level12). Detailed HPLC conditions by Morota's report5)is sh。wn in Table 1. The typical chromatograms of lidocaine from rabbit bone sample are shown in Figure 3 . Tissue lidocaine data were converted to lidocaine level per gram(g)jawbone .
7.Comparison statistics of data
Comparison statistical analysis on MAP, blood lidocaine, and lidocaine concentration in the jawbone was performed on the four groups(100±5OmmHg , 200±50mmHg,300±50mmHg and 400±50mmHg). Kruskal Wallis H‑test was used for
the statistical analysis, and Mann‑Whitney U‑test with Bonferroni correction was
performed with multiple comparisons. The statistical significance level of all cases was determined to be P<0.05.
Results
1.Fluctuation in MAP due to infiltration anesthesia(Figure 4)
MAP of the four groups is shown before inj ection, after 10 seconds, and after 20 seconds, respectively, as follows.
In the lOO±50mmHg group, MAP was 97±1.08mmHg, 94±2.04mmHg and 98±0.86mmHg. In the 200±50mmHg group, 97±1.29mmHg , 95±1.87mmHg and 99±0.82mmHg. In the 300±50mmHg group, 97±0.82mmHg , 95土0.43mmHg and 98±0.43mmHg. In the 400±50mmHg group, 97±0.70mmHg, 96±0 .82mmHg and 98±0.86mmHg, respectively.
No significant fluctuation in blood pressure was observed in any group, and no significant difference between four group s was detected.
2.Blood lidocaine concentration(Figure 5)
Blood lidocaine concentration of the four groups is shown at 10min,20 min,30 min;
40min,50 min and 60 min after the infltration anesthesia, respectively , as follows.
In the 100±50mmHg group, blood iidocaine concentration was 1.38±0.12μg/mL, 1.13±0.11μg/mL, 0.97±0.13μg/mL, 0.87±0.17μg/mL, 0.69±0 .12μg/mL and O59±0.09μg/mL In the 200±50mmHg group,1.09±0.06オg/mL,0 .95士0.09μg/mL, 0.79±0.12μg/mL,0.67±0.17オg/mL,0.60±0.16μg/mL and 0.53±0 .15μg/mL. In the 300±50mmHg group, 0.88土0.06μg/mL , 0.72±0.03オg/mL, 0.60±0.03μg/mL,
0.55±:0.03μg/mL,0.50±0.04μg/mL and 0.41±0.03オg/mL. In the 400±50mmHg group , 0.79±0.03μg/mL, 0.69±0.04μg/mL, 0 .59±0.05μg/mL, 053±0.04μg/mL, 0.49±0.06μg/mL and 0.40±0.04μg/mL, respectively .
For all groups, the highest value was obtained at 10 minutes after infiltration anesthesia, and concentration decreased thereafter. For all time intervals , cases of lower injection pressure had significantly higher blood lidocaine concentrations . Moreover, blood lidocaine concentration for the 400±50mmHg group at all time intervals was
significantly lower than that for the 100±50mmHg group. In the 200±50mmHg group , significant difference was no longer observed after 30 minutes. In the 300±50mmHg
group, significant difference was no longer observed after 50 minutes.
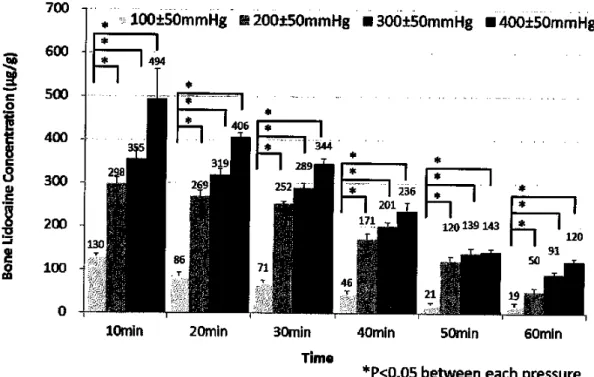
3.Lidocaine concentration in the j awbone(Figure 6)
Lidocaine concentration in the jawbone of the four groups is shown at 10 min,20 min,30 min,40 min,50 min and 60 min after the infiltration anesthe sia, re spectively , as follows.
In the 100f50mmHg group, lidocaine concentration in the j awbone was 130±4オg/g, 86±7オg/g,71±4μg/g,46±6μg/g,21±4μg/gand 19±5μg/g. In the 200±50mmHg group , 298±15μg/g,269±14μg/g,252±7μg/g,171±13μg/g,120±10μg/gand 50±8μg/g . In the
300±50mmHg group,355±23μg/g,319±14μg/g,289±10μg/g,201±9μg/g,139±11μg/g and 91±6μg/g. In the 400±50mmHg group,494±68μg/g,406±8μg/g,344±12オg/g, 236±19オg/g,143±6μg/gand 120±7μg/g, respectively.
The highest value was obtained at 10 minutes after infiltration anesthesia for all groups, and concentration decreased thereafter. Groups with a higher inj ection pressure had signifcantly higher lidocaine concentration in the jawbone at all time intervals .
Discussion
1.Fluctuation in MAP due to infiltration anesthesia
Although no significant difference was observed in fluctuation in MAP before and after infiltration anesthesia, atendency towardstemporary decrease was observed in all
groups after infiltration anesthesia. Decrease in MAP due to a temporary reduction in vascular resistance of skeletal muscle caused by adrenalineβ2 reaction , and a return to levels before injection due to peripheral vasoconstriction by α1 reaction , have been reported 13,14).Furthermore, cardiac output is increased by adrenaline , and total
peripheral resistance is reduced. However, it is reported that blood pressure does not increase significantly by just one or two cartridges of 2% ofl idocaine with 1/80,000 adrenaline, in the clinical use dosage for a healthy adultl3).Hence, the amount of lidocaine and adrenaline used on rabbits in this study is considered to be within the range of clinical use dosage.
There are some reports that anxiety and pain at the beginning of injection can be controlled with a lower injection pressure. However, other reports on studies of injection pressure and pain show that in cases of a higher injection pressure of SOOmmHg, pain does not significantly increase due to blocking pain by local anesthetic infltration, and nerve transient ischemia by pressure 1,15,16) Moreover , greater fluctuation of MAP with the increase of pain has also been reported , showing a positive correlation in general anesthesia experiment of rabbits8). This result suggests that a significant difference of a pain will not be observed in the each condition of inj ection
pressure range, since no significant difference was observed for the fluctuation range of MAP at infiltration anesthesia between groups.
2.Blood lidocaine concentration
Blood lidocaine concentration increased as injection pressure decreased at each time interval. Generally, local anesthesia is injected under the periosteum and filtrated into the bone through the cortical bone, reaching the bone marrow, and absorbed from the blood capillaries18). Although lidocaine has high tissue permeability , infltration into bone tissue is considered more difficult than that into soft tissue 18, 19) On the other hand , oral soft tissue has denser blood vessels and greater blood flow volume than bone3) . Consequently, local anesthesia in oral soft tissue with denser blood vessels and greater blood flow was transferred more quickly to blood vessels, rather than jawbone . Since the results findings showed a faster increase of blood lidocaine concentration at a lower injection pressure, the possibility that local anesthesia does not infiltrate into the
jawbone, but is transferred to the oral soft tissue and vessels at a lower injection pressure, was indicated.
3.Inj ection pressure and lidocaine concentration in the jawbone
Since lidocaine concentration in the jawbone significantly increased as injection pressure increased, greater infiltration of local anesthesia into the jawbone due to the increased injection pressure of subperiosteal infiltration anesthesia was indicated . Moreover, this result is strongly supported by the results of blood lidocaine concentration in this study.
As reported by Morota et al.5), in experiments comparing insertion to attached
gingiva and insertion to alveolar mucosa, infiltration anesthesia to attached gingiva was performed at a higher injection pressure, with increased lidocaine concentration in the jawbone. Hochman et al.18) alsohas reported that greater infiltration to tissue at a higher
injection pressure could be achieved for attached gingiva than for alveolar mucosa . Results obtained by Tateno et al.19) using rats showed that local anesthesia injected into alveolar mucosa widely spread to soft tissue. These reports also support the results of this study, namely that as injection pressure increases, infltration of local anesthesia
into the jawbone becomes easier. However, in these reports, the possibility that differences between injection sites influence the degree of infiltration of local anesthesia cannot be ruled out. In this regard, as subperiosteal infiltration anesthesia was given to the same site under the same conditions and then classified into four groups according to the mean injection pressure, consideration only of injection pressure, rather than differences between sites, was possible in this study. In surgeries clinically performed on the jawbone, obtaining a higher infiltration anesthesia effect for a longer period of time is considered attainable by avoiding a lower inj ection pressure, then searching for the point to gain a higher injection pressure at which to perform injection. Furthermore , in subperiosteal infiltration anesthesia at a higher injection pre ssure, reducing injection volume of local anesthetic is also considered possible.
Conclusion
The effect of injection pressure of subperiosteal infiltration on local anesthetic infiltration was considered by directly measuring the lidocaine concentration. As a result, as inj ection pressure increases, subperiosteal infiltration anesthesia also increases, the effect of lidocaine concentration in jawbone becomes stronger while a low blood lidocaine concentration could be maintained.
Acknowledgements
In conclusion, the authors would like to express their heartfelt gratitude to Prof.
Shinya Yamazaki and Associate Prof. Hiroyoshi Kawaai, Division of Systemic Management, Department of Oral Function, Ohu University Graduate School of
Dentistry, for their supervision. The authors also would like to thank the staffs from the Division of Dental Anesthesiology, Department of Oral Surgery, School of Dentistry, Ohu University, and Prof. Norifumi Yonehara and other staffs from Division of Dental Pharmacology, Department of Oral Pathobiological Science, School of Dentistry, Ohu University, for their cooperation.
References
1)Ohkado, S., Ichinohe, T., Kaneko, Y.,:Comparative study on ane sthetic potency
depending on concentrrations of lidocaine and epinephrine;Assessment of dental local
anesthetics using the jaw‑opening reflex. Anesth Progress 41;16‑20 2001.
2)Kudo, M., Ohke, H., Kawai, T., Kokubu , M., Shinya, N.:Effects of inj ection
pressure and injection speed on anxiety and pain during gingival submucosal infiltration
anesthesia. Anesthesia Progress 32;49‑54 2004.
3)Shinya, Y., Hiroaki, S., Sachie, O., Hiroshi,1, and Hiroyoshi, K.:Elevation of a
periosteal flap with irrigation of the bone for minor oral surgery reduces the duration of
action of infiltration anesthesia. Anesthesia Progress 53;8‑12 2006.
4)Ogawa, S., Watanabe, T., Kawaai, H., Tada, H., Yamazaki , S. Lidocaine
concentration in mandibular bone after subperiosteal infiltration anesthesia decreases
with elevation of periosteal flap and irrigation with saline. Anesthesia Progress 61;
53‑62 2014.
5)Morota, T.,Kawaai,H., Yamazaki, S.:Difference of injection point for local
anesthesia in alveolar bone affects infiltration and action of anesthesia. Ohu Univ . Dent.
J.41;29‑38 2014.
6)Nagao, H., Munakata, M., Tachikawa, N., Shiota, M., Kasugai, S.:Clinical study of risk management for dental implant treatment:Changes of blood pressure and pulse rate during implant surgery under local anesthesia. J. Stomatol . Soc. Jpn.69;27‑33 2002.
7)Ishihara, Y., Kikutani, T., Inaba, S.:A study of circadian blood pressure variability and local anesthesia procedure:Comparison between elderly dental outpatients and
young subjects. Japanese Journal of Applied Physiology.32;139‑145 2002.
8)Ma, D., Chakrabarti, M.K., Whitwam, J.G.:The combined effects of sevoflurane and remifentanil on central respiratory activity and nociceptive cardiovascular responses in anesthetized rabbits. Anesth. Analg.89;453‑461 1999.
9)Beach, C.L., Ludden, T.M., Clementi, W.A., Allexheiligen , S.R.:Measurement of lidocaine free concentration. Ther Drug Monit.8;326‑330 1986 .
10)Parish, R.C., Gotz, V.P., Lopez, L.M., Curry, S.H.:Improved EMIT analysis for lidocaine. Clin Chem.31;1920‑1921 1985.
11)Oellerich, M.:Enzyme immunoassays in clinical chemistry:present status and trends. J CIin Chem Clin Biochem.18;197‑208 1980 .
12)Piwowalska, J., Kuczynska, J., Pachecka , J.:Liquid chromatographic method for the determination of lidocaine and monoethylglycine xylidide in human serum
コ
containing various concentrations of bilirubin for the assessment of liver function . J Chromatogr B Analyt Technol Biomed Life Sci .805;1‑5 2004.
13)Ichinohe, T., Kaneko, Y., Nakakuki, T.:The effect of epinephrine on circulation and respiration‑investigation with epinephrine infusion technique‑ .J. Jpn, Dent. Soc.
Anesthesiol.18;477‑497 1990.
14)Troullos, E.S., Goldstein, D.S., Hargreaves , K.M., Dionne, R.A. Plasma epinephrine levels and cardiovascular response to high administered doses of epinephrine contained in local anesthesia. Anesthesia Progress 34;10‑13 1987 .
15)Birchfield, J., Rosenberg, P.A.:Role of the anesthetic solution in intrapulpal anesthe sia. J Endodontics.1;26‑27 1975.
16)Hirvonen, T., Virtansen, A., Narity, M., Huopaniall , T.:Effect of adrenalin on responses of intradental nerve fiber units. Proc Finn Dent Soc .78;110‑115 1982.
17)Ishikawa, M., Momota, Y., Kotani, J.:Effects of adrenalin and the sedative agent
on the systemic vascular absorption of lidocaine after local infiltration anesthesia . J. Jpn.
Dent. Soc. Anesthesiol.35;649‑654 2007.
18)Hochman, M.N., Friedman, M.J., Williams, W., Hochman , C.B.:Interstitial tissue
pressure associated with dental injections:aclinical study. Quintessence Int.37;
469‑476 2006.
19)Tateno, K., Inoue, K., Sato, T., Fukayama , H.:Differences in the degree of infltration of local anesthesia according to the site of injection in rats . Oral Surg Oral Med Oral Pathol Oral Radiol Endod.106;6‑10 2008 .
Figure legends
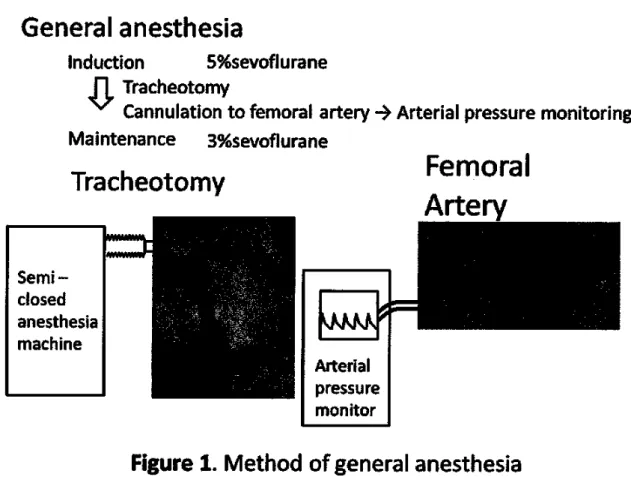
Figure 1.Method of general anesthesia
General anesthesia was induced by oxygen 5L/minute and 5%sevoflurane, and then a tracheotomy was performed, after which general anesthesia was maintained at oxygen 3L/minute and 3%sevoflurane. A cannula was inserted into the femoral artery, and arterial pressure was continuously recorded throughout the experiment using a
polygraph and a pressure transducer.
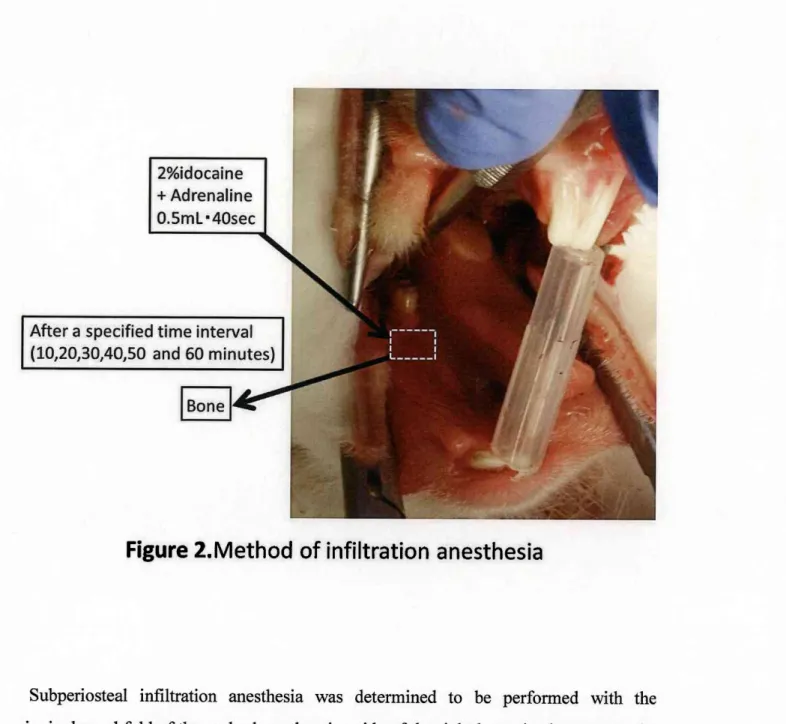
Figure 2. Method of infiltration anesthesia
Subperiosteal infiltration anesthesia was determined to be performed with the
gingivobuccal fold of the molar buccal region side of the right lower jawbone set as the injection site by attaching the needle tip to the jawbone. Next, after a specified time interval(10,20,30,40,50 and 60 minutes), the periosteum was elevated, and the
jawbone was removed using bone cutting forceps.
Table 1.Condition for HPLC analysis of lidocaine
Figure 3. Chromatogram of Iidocaine from tissue in rabbit
The typical chromatograms of lidocaine from rabbit bone sample are shown. Tissue lidocaine data were converted to lidocaine level per gram(g)tissue.
Figure 4. Change ofmean arterial pressure before and after infiltration anesthesia
No significant fluctuation in blood pressure was observed in any group, and no significant difference between four groups was detected.
Figure 5. Change of blood lidocaine concentration after infiltration anesthesia
For all groups, the highest value was obtained at 10 minutes, after infiltration anesthesia, and concentration decreased thereafter. For all time intervals , cases of lower injection pressure had significantly higher blood lidocaine concentrations. Moreover, blood lidocaine concentration for the 400±50mmHg group at all time interva1s was
signifcantly lower than that for the 100±50mmHg group and in the 200±50mmHg
group, significant difference was no longer observed after 30 minutes. In the 300±50mmHg group, significant difference was no longer observed after 50 minutes . Figure 6. Change of jawb one lidocaine concentration after infiltration anesthesia
The highest value was obtained at 10minutes after infiltration ae sthesia for all groups,
and concentration decreased thereafter. Groups with a higher inj ection pressure had significantly higher lidocaine concentration in the jawbone at all time intervals.
Figure 1. Method of general anesthesia
General anesthesia was induced by oxygen 5L/minute and 5%sevoflurane, and then a tracheotomy was performed, after which general anesthe sia was maintained at oxygen 3L/minute and 3%sevoflurane. A cannul a was inserted into the femoral artery, and arterial pressure was continuously recorded throughout the experiment using a
polygraph and a pressure transducer.
Figure 2.Method of infiltration anesthesia
Subperiosteal infiltration anesthesia was determined to be performed with the
gingivobuccal fold of the molar buccal region side of the right lower jawbone set as the injection site by attaching the needle tip to the jawbone. Next, after a specified time interval(10,20,30,40,50 and 60 minutes), the periosteum was elevated , and the
jawbone was removed using bone cutting forceps.
Table 1。 Condition for HPLCanalysis of lidocaine
Punp
Flow rate
Detector
Wave length
Sensitivlty Column
Column oven
Column temperature
Degasser
Mobile phase
Jasco PU‑2080 Plus
1.0mL/min
jasco UV‑2075 Plug
205nm 0.001AUFS
TOSOH TSK‑GELODS‑100V 15cm×4.6mm
Sugai V‑630
40°C
AZZOTA AG‑12
50mM KH2PO4:CH3CN=4:1
Figure 3. Chromatogram of lidocaine from tissue in rabbit
The typical chomatograms of lidocaine from rabbit bone sample are shown. Tissue lidocaine data were converted to lidocaine level per gram(g)tissue.
Figure 4. Change of mean arterial pressure before and after infiltration anesthesia
No significant fluctuation in blood pressure was observed in any group, and no significant difference between four groups was detected,
Figure 5. Change of blood lidocaine concentration after infiltration anesthesia
For all groups, the highest value was obtained at 10 minutes after infltration anesthesia, and concentration decreased thereafter. For all time intervals, cases of lower injection pressure had significantly higher blood lidocaine concentrations. Moreover, blood lidocaine concentration for the 400±50mmHg group at all time intervals was
significantly Iower than that for the 100±50mmHg group and in the 200±50mmHg
group, significant difference was no longer observed after 30 minutes. In the 300±50mmHg group, significant difference was no longer observed after 50 minute s.
Figure 6. Change of jawbone lidocaine concentration after infiltration anesthesia
The highest value was obtained at 10minutes after infiltration aesthesia for all groups, and concentration decreased thereafter. Groups with a higher injection pressuxe had significantly higher lidocaine concentration in the jawbone at all time intervals .