5-アミノレブリン酸(5-ALA)を利用した
光線力学的胸腔鏡下蛍光 navigation 手術の試み
坂尾幸則
1,2;黒田浩章
1;谷田部恭
3要約 ━━ 背景. 5-アミノレブリン酸(5-ALA)の蛍光ナビゲーション手術の新たな可能性を検討した.症例.60 歳代,
男性.左 S1+2,左 S5に 2 cm 大の結節を認め,大動脈下リンパ節が 3 cm 大に腫大していた.Positron emission
tomogra-phy(PET)CT では 3 病変ともにフルオロデオキシグルコース(FDG)の集積を認めた.治療方針決定のため 3 病変 を胸腔鏡下に生検(肺部分切除 2 カ所,リンパ節針生検)した.手術 3 時間前に 5-ALA を 20 mg/kg 内服し,3 ports 鏡視下手術を実施した.結果.胸腔内観察では S1+2病変には強い赤色蛍光を認めた.大動脈下リンパ節と S5病変では 明らかな赤色蛍光を認めなかった.それぞれの病変の病理は S1+2は大細胞癌,S5は肉芽腫,リンパ節は上皮性悪性腫 瘍の転移を認めた.本例では肺病変に関しては,非腫瘍性腫瘤と腫瘍との鑑別に有用である可能性が示唆された.一方 リンパ節に関しては,bulky な転移であったにも関わらず蛍光はほとんど観察されなかった.原因としては,viable な腫瘍細胞が観察面に乏しかった可能性がある.結論.5-ALA 利用の胸腔鏡下での蛍光観察は病変の腫瘍性変化と炎症 性変化を鑑別できる可能性が示唆された. (気管支学.2019;41:417-421) 索引用語 ━━ 5-アミノレブリン酸,胸腔鏡手術,光線力学診断
背 景
我 が 国 の 光 線 力 学 診 断(photodynamic diagnosis: PDD)の歴史は 1978 年,Dougherty と東京医大との共同 研究に始まる.臨床応用としては 1979 年 11 月肺癌の診 断的蛍光観察(PDD),1980 年 3 月に早期肺癌の光線力学 治療(PDT)が施行されている.現在では,光過敏症な どの副作用の少ない 5-アミノレブリン酸(5-ALA)を使 用した PDD が脳腫瘍や膀胱腫瘍を中心に普及してきて いる1.5-ALA はヘム代謝の中間基質で患者に経口投与, 吸収されると正常細胞では蛍光を認めないヘムに速やか に代謝されるが,癌細胞では porphobilinogendeaminase の活性が高く,ferrochelatase の活性が低いため,プロト ポルフィリン IX(PpIX)が選択的に蓄積される2-4.PpIX は蛍光物質であり,これを検出して癌の診断を行うこと が可能となる.術野に波長 405 nm の半導体レーザー光 を照射し,420 nm 以下をカットするフィルターを通して 観察すると,腫瘍部では PpIX による赤色蛍光が観察さ れる.既に脳神経外科領域,泌尿器科領域においてはそ の術中蛍光診断の有効性が報告されている1.特に高悪性 度脳腫瘍である悪性神経膠腫の腫瘍摘出術に際しては, 白色光下での完全切除率が 36% であったのに対して 5-ALA 投与後の蛍光観察下では 65% と腫瘍摘出率の向 上,6 カ月無増悪期間の延長が示されている5.呼吸器外 科領域においては,微小胸膜播種,胸膜浸潤の診断に有 効である可能性が報告されている6が,肺癌の局在や炎 症腫瘤との鑑別における有効性は未だ報告されていな い.我々は 5-ALA の蛍光 navigation 手術の有用性を検 討すべく,臨床試験(愛知県がんセンター中央病院倫理 審査委員会:2016-1-37)を開始した.症 例
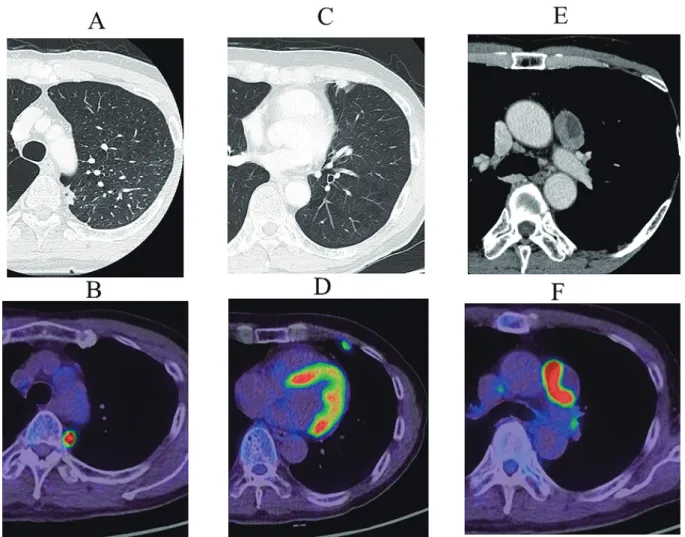
60 歳代,男性. 20XX 年に検診胸部エックス線写真で異常を指摘され 受診. CT では左 S1+2,左 S5に 2 cm 大の結節を認め,大動脈 下リンパ節に 3 cm 大のリンパ節腫大も認めた.Positron emission tomography(PET)CT では 3 病変ともにフル オロデオキシグルコース(FDG)の集積を認めた(stan-dardized uptake value(SUV)max;S1+2:27.4,舌区:4.8, 大動脈下リンパ節:38.6).S5病変にも集積があり,転 移や多重癌,炎症が鑑別であった(Figure 1).3 病変の
TECHNICAL REPORT
1愛知県がんセンター中央病院呼吸器外科;2帝京大学外科学講座・呼吸器外科;3愛知県がんセンター中央病院遺伝子病理診断部. 著者連絡先:坂尾幸則,帝京大学外科学講座・呼吸器外科,〒173-8605 東京都板橋区加賀 2-11-1(e-mail: [email protected]). 受付日:2019 年 1 月 15 日,採択日:2019 年 3 月 11 日.Figure 1. Computed tomography (CT) and fluorodeoxyglucose (FDG) positron emission tomography-CT findings. A: A 2-cm nodule with an irregular shape is noted in the S1+2 regions. B: The nodule has a standardized uptake val-ue (SUV) max of 27.4. C: A 2-cm nodule with an irregular shape is noted in the S5 region. D: The nodule has an SUV max of 4.8. E: A 3-cm subaortic lymph node with a low-density lesion. F: The lymph node has an SUV max of 38.6, and the low-density lesion shows no accumulation of FDG.
病理所見とその関連性によって治療方針が異なるため, まず 3 病変を胸腔鏡下に生検(肺部分切除 2 カ所,リン パ節針生検 1 カ所)する方針とした.
5-ALA 蛍光観察の方法
1.投与方法 胸腔鏡下肺手術の 3 時間前に 5-ALA を 20 mg/kg 内 服する.その後,胸腔鏡蛍光画像システムで病変を観察 して視認性を評価する.リンパ節の観察も併せて施行す る. 2.使用器材(STORZ 社製撮像システム) 撮像スコープ:K26003AIA,内視鏡光源:D-ライト C with SCB,カメラヘッド:IMAGE 1 SPICES FI,カメラ コントロールユニット IMAGE 1 CONNECT/LINK. 波長 405 nm の半導体レーザー 光 を 照 射 し,420 nm 以下をカットするフィルターを通して観察する.結 果
3 ports 鏡視下手術とした(Figure 2).胸腔内観察では S1+2病変には強い赤色蛍光を認めた.大動脈下リンパ節 と S5病変では明らかな赤色蛍光を認めなかった.それぞ れの肺病変を部分切除,リンパ節は針生検を施行して, 手術は終了した. 病理では S1+2は大細胞癌,S5は肉芽腫(Figure 3A, 3B),リンパ節には細胞診で上皮性悪性腫瘍の転移を認 めた.以上から,左上葉肺癌(大細胞癌)cT1cN2M0-IIIA と判断した.リンパ節は 2.5 cm 大で,bulky single N2 の判断で導入化学療法とした.CDDP/VDS を 2 コース 行い,根治手術(左上葉切除及び ND2a-1)を行い,大動 脈下リンパ節のみに転移を認める skip single N2 症例でThoracoscopic Photodynamic Diagnosis Using 5-Aminolevulinic Acid in Lung Cancer―Sakao et al
Figure 2. Findings of thoracoscopic observation. A: A 2-cm nodule with an irregular shape is detected with white
light in the S1+2 regions. B: The nodule shows a high level of red fluorescence. C: A 3-cm consolidated lesion is de-tected with white light in the S5 region. D: Red fluorescence is not observed. E: A 3-cm subaortic lymph node is de-tected with white light. F: Red fluorescence is not observed.
あった(Figure 3C).その後,術後 1 年半の経過で現在ま で再発を認めていない.
考 察
5-ALA 利用の蛍光観察は,呼吸器外科領域において本 邦では未だ保険適用ではないが,微小胸膜播種,胸膜浸 潤の診断に有効である可能性が報告されている6.その報 告では肺癌症例において赤色蛍光が確認された割合は 53.5%,特に病理学的胸膜浸潤陽性例では 100% で,腫瘍 の存在診断に有効であるとしている. 他方,現時点で術中・術前に肺結節やリンパ節におけ る炎症性変化と腫瘍病変との有用な鑑別方法がない.基 本的に病理学的検索(迅速組織診断)を実施する以外に 方法がないのが現状である. 5-ALA の蛍光機序からは, 理論的に本法が炎症と腫瘍の鑑別に有用である可能性が 期待される.すなわち,炎症では腫瘍同様の代謝異常が 生 じ な い と 考 え ら れ る た め 5-ALA が protoporphyrin IX(PpIX)として細胞内に蓄積される機序は働かず, FDG-PET のような炎症部への集積は認めないと予想さ れる3,4,7.本例では肺病変に関しては,非腫瘍性病変(炎 症性腫瘤)と腫瘍との鑑別に有用である可能性が示唆さ れた.一方リンパ節に関しては,本例では bulky な転移 であったにも関わらず蛍光がほとんど観察されなかっ た.その要因のひとつとしては,腫大した大動脈下リン パ節の外側領域が造影 CT で広範な低吸収域を示してお り(Figure 1C),FDG 集積も同領域に乏しかったことか ら(Figure 2C),viable な腫瘍細胞が蛍光観察面(リンパ 節の外側表層近く)に乏しかったことなどが考えられる. なお,導入化学療法後に切除した大動脈下リンパ節の組 織所見では,CT の低吸収領域と一致して広範な壊死と 線維化を認めた(最大面の約 30∼40%:Ef.1b)(Figure 3E).化学療法後の変化を考慮すべきではあるが,化学療 法前に施行した画像診断所見(Figure 1C,2C)とも矛盾 しない所見であった. 今後の大きな課題としては,現時点では蛍光について の定量的な測定法・評価法がなく,視認するのみである. 病変,観察組織,病理所見,腫瘍細胞量などにより,異 なる蛍光強度が観察されることが予想されるため,今後 は定量的測定法・蛍光程度の客観的評価法の確立,病理 所見との対比が必要と考えている. 現在,上記の問題点を念頭にさらに症例の蓄積を図り 検証を進めている.今回は 1 例での所見であり,特に肺Figure 3. Pathological findings. A: A 2-cm nodule with a round shape is detected in the S1+2 regions. B: The tu-mor cells are round and have large nuclei and have much mitosis and form like sheet structure without gland for-mation or keratinization. Neuroendocrine markers are not detected by any immunohistochemical analyses. The pathological diagnosis is large cell carcinoma. C: The nodule consists of several small round areas in the S5 region. D: Many Langhans giant cells are observed and no tumor cell is found. The pathological diagnosis is granuloma. Final-ly, no microorganism including mycobacterium or fungus is detected. E: A 3-cm subaortic lymph node. Most of the lateral part of the lymph node shows necrosis and fibrosis. The effect of chemotherapy is evaluated as Ef.1b. F: In the medial part of the lymph node, viable tumor cells are observed. The tumor cells form patchy structures, and the cells are round and have large nuclei.
病変の炎症性腫瘤と腫瘍との鑑別に有用である可能性が 示唆されたため,テクニカルレポートとして報告した.
結 論
5-ALA 利用の胸腔鏡下での蛍光観察には,病変の腫瘍 性変化と炎症変化を鑑別できる可能性が示唆された. 本論文に関連する開示すべき利益相反関係にある企業 等はない. 謝辞:本研究において,技術協力していただいた水野鉄也先 生,坂倉範昭先生,有村隆明先生に深謝申し上げます. REFERENCES1.Inoue K, Anai S, Fujimoto K, et al. Oral 5-aminolevulinic acid mediated photodynamic diagnosis using fluores-cence cystoscopy for non-muscle-invasive bladder can-cer: A randomized, double-blind, multicentre phase II/ III study. Photodiagnosis Photodyn Ther. 2015;12:193-200.
2.Dailey HA, Smith A. Differential interaction of porphy-rins used in photoradiation therapy with ferrochelatase. Biochem J.1984;223:441-445.
3.Schoenfeld N, Epstein O, Lahav M, et al. The heme bio-synthetic pathway in lymphocytes of patients with ma-lignant lymphoproliferative disorders. Cancer Lett. 1988; 43:43-48.
4.Kennedy JC, Pottier RH. Endogenous protoporphyrin IX, a clinically useful photosensitizer for photodynamic therapy. J Photochem Photobiol B. 1992;14:275-292.
5.Stummer W, Pichlmeier U, Meinel T, et al. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma : a randomised controlled multicentre phase III trial. Lancet Oncol. 2006; 7:392-401.
6.Kitada M, Ohsaki Y, Matsuda Y, et al. Photodynamic di-agnosis of pleural malignant lesions with a combination of 5-aminolevulinic acid and intrinsic fluorescence ob-servation systems. BMC Cancer. 2015;15:174.
7.Peng Q, Warloe T, Berg K, et al. 5-Aminolevulinic acid-based photodynamic therapy. Clinical research and fu-ture challenges. Cancer. 1997;79:2282-2308.
Thoracoscopic Photodynamic Diagnosis Using 5-Aminolevulinic Acid in Lung Cancer―Sakao et al
Thoracoscopic Photodynamic Diagnosis Using 5-Aminolevulinic Acid
(5-ALA) in Lung Cancer
Yukinori Sakao
1,2; Hiroaki Kuroda
1; Yasushi Yatabe
3ABSTRACT━━ Background. A new fluorescent diagnostic modality involving the use of 5-aminolevulinic acid (5-ALA) for intrathoracic malignant lesions has been developed. Here we present the case of a patient with lung cancer who underwent photodynamic diagnosis using this modality. Case. A male patient was aged around 60-year-old with pulmonary nodules measuring 2 cm in the left S1+2and S5regions. In addition, he had a mediastinal mass measuring
3 cm on computed tomography (CT). Positron emission tomography/CT demonstrated standardized uptake value (SUV) max levels of 27.4, 4.8, and 38.6 for the S1+2, S5, and mediastinal masses, respectively. The patient received
5-ALA (20 mg/kg) orally 3 hours before surgery, and the intrathoracic space was viewed using an auto-fluorescence imaging system. Results. A high level of red fluorescence was observed in the S1+2nodule. However, red
fluores-cence was not observed for the S5nodule and subaortic lymph node. Pathological findings indicated large-cell
carci-noma in S1+2, granuloma in S5, and metastatic cancer with necrosis in the subaortic lymph node. Conclusion. This
fluorescent system involving the use of 5-ALA may distinguish viable malignant lesions from inflammatory lesions, suggesting that it could be applicable to the photodynamic diagnosis of lung nodules and hilar and mediastinal lymph node swellings.
(JJSRE. 2019;41:417-421)
KEY WORDS━━ 5-aminolevulinic acid, Thoracoscopic surgery, Photodynamic diagnosis
1Department of Thoracic Surgery, Aichi Cancer Center Hospital, Japan;2Department of Surgery, Teikyo University School of Medicine,
Japan;3Department of Pathology, Aichi Cancer Center Hospital, Japan.
Correspondence: Yukinori Sakao, Department of Surgery, Teikyo University School of Medicine, 2-11-1 Kaga, Itabashi-ku, Tokyo 173-8605, Japan (e-mail: [email protected]).