*1大阪大学医学部附属病院集中治療部(〒565-0871 大阪府吹田市山田丘2-15) 受付日2017年12月11日 *2 Keenan Research Centre, Li Ka Shing Knowledge Institute, St. Michael’s Hospital 採択日2018年 1 月 5 日 (30 Bond street Toronto, ON, M5B IW8, Canada) *3 Interdepartmental Division of Critical Care Medicine, University of Toronto (190 Elizabeth street R. Fraser Elliott Building, 3-805 Tronto, ON M5G 2C4, Canada) *4大阪大学大学院医学系研究科麻酔・集中治療医学講座(〒565-0871 大阪府吹田市山田丘2-2) 要約:人工呼吸中に自発呼吸を温存することは,背側肺領域優位の換気を促し,低い気道内 圧(プラトー圧)でも呼気終末肺容量が比較的保たれ,酸素感も改善することから,最も侵襲 性の低い肺リクルートメント療法であると考えられている。しかし,急性呼吸窮迫症候群の 重症例など呼吸努力の特に強い症例では,肺保護換気戦略に則ってプラトー圧を制限したと しても経肺圧が増加し,人工呼吸器関連肺傷害の危険因子となり得ることが多数報告されて いる。また,そのような症例に対し,肺保護換気戦略に従って1回換気量を制限したとしても, pendelluft現象により肺局所の過伸展から肺損傷を引き起こす可能性がある。呼吸努力を最小 限に抑えた自発呼吸の温存または,筋弛緩によるfull supportは症例ごとの呼吸状態を慎重に 見極めることで,一連の管理方法となり得ると考える。 Key words: ①spontaneous breathing, ②mechanical ventilation, ③acute respiratory distress syndrome, ④ventilator-induced lung injury
人工呼吸管理中の自発呼吸の功罪
海老島宏典
*1吉田 健史
*2, 3内山 昭則
*4Ⅰ.はじめに
1950年代に陽圧換気用人工呼吸器が開発され,呼吸
不全患者に対する機械的人工呼吸法の適応は急速に拡
大した。陽圧人工呼吸下では人工呼吸器関連肺傷害な
ど呼吸器関連合併症の予防に焦点をあてた肺保護換気
戦略が主流となっており
1)〜4),人工呼吸中の自発呼吸
の温存は肺機能の改善や呼吸筋の廃用症候群などの合
併症の予防に有益と考えられてきた
5)〜8)。
Ⅱ.人工呼吸管理中に肺にかかる
stress
人工呼吸器による陽圧の気道内圧は,肺胞と胸郭の
両方を拡張させることにより1回換気量が確保され
る。つまり,人工呼吸管理中に肺胞が伸展/虚脱する
ためにかかるstressは肺胞内圧から胸膜圧を引いた経
肺胞圧が最も適切な生理学的用語となる。気流がない
状態では気道抵抗に対する圧がゼロとなり経肺胞圧は
経肺圧(=気道内圧-胸膜圧)と等しくなることから,
人工呼吸管理中の肺の伸展/虚脱に作用するstressは
経肺圧で評価することができる
9)。2010年Brielらに
より重症急性呼吸窮迫症候群(acute respiratory
distress syndrome, ARDS)患者では高いPEEP設定が
院内死亡率を低下させることが報告され
10),個々の症
例に適したPEEP設定の重要性が再認識された。前述
の式に従えば,適切な呼吸器設定の決定に際し,症例
ごとの胸膜圧の同定が重要となる。胸膜圧の測定方法
では,1949年にBuytendijkは食道内圧が胸膜圧の代
用になり得ることを初めて報告した
11)。その後,呼
吸生理学的研究分野において,食道内圧は胸膜圧の代
替として長きにわたり頻用されてきた。しかし,食道
内圧の測定には専用の食道内バルーンの挿入が必要で
あり,留置位置の調節など手技の煩雑さなどから,臨
床現場ではほとんど使用されていなかった。近年,
Prof. Laurent Brochardを中心としたworking group
(PLeUral pressure working Group, PLUG)が,ベッ
ドサイドでの正確な食道内圧測定の普及に努めてい
る
12)。
Ⅲ.人工呼吸管理中の自発呼吸が及ぼす生理
的変化
1
)
経肺圧の上昇
自発呼吸がなければ気道内圧の陽圧の一部は胸郭の
伸展に消費されるため,経肺圧が気道内圧を上回るこ
とはない。肺保護戦略の観点に立てば,気道内圧(プ
ラトー圧)の制限によって経肺圧が下がり,肺損傷の
riskを回避することが可能となる。しかし,人工呼吸
管理中に自発呼吸努力が生じると,横隔膜をはじめと
した呼吸筋の能動的な収縮により胸郭は自発的に拡が
るため,胸膜圧は陰性化し経肺圧は上昇する
12)〜14)(Fig. 1)。
2
)
Pendelluft
現象
正常肺では人工呼吸器や自発呼吸により発生した陽
性または陰性の胸膜圧変化は瞬時に肺表面全体に均一
に伝播され,肺尖部,腹側肺,背側肺,それぞれの部位
での変化値は等しくなることが多くの肺生理学実験で
示されている(肺のfluid-like behavior)。一方,ブタ
の急性肺傷害モデルでは,肺局所表面の胸膜圧変化は
不均一であることが示された
15),16)(Fig. 2)。すなわち,
急性肺傷害モデルでは,人工呼吸管理中の自発呼吸に
より横隔膜周囲で発生した陰圧の胸膜圧は背側領域に
より重点的に伝播され,背側と腹側の肺領域に非常に
大きな胸膜圧の圧較差を生じていた(胸膜圧変化値の
背側領域 vs. 腹側領域;-13±4.0 cmH
2O vs. -6.4
±3.8 cmH
2O)
16)。これは,肺血流の増加した部位
(dependent lung)や浸出液・炎症細胞で肺胞が満た
された部位では胸膜圧変化の伝播様式が固体様に変化
することを意味している(肺のsolid-like behavior)。
肺領域間での胸膜圧変化の不均衡は,吸気フローの不
均衡(胸膜圧の低い背側肺に吸気フローが流入する)
だ け で な く,腹 側 肺 か ら 背 側 肺 へ の 空 気 の 移 動
(pendelluft現象)を引き起こす。これにより吸気相に
腹側肺が虚脱,背側肺は過膨張することになる。
3
)
肺循環血液量の増加
自発呼吸により生じる胸腔内の陰圧は,静脈還流の
増加と肺血管の拡張による前負荷の増大と後負荷の軽
Fig. 1 Spontaneous effort and transpulmonary and transvascular pressures During a mechanical breath(a), the transpulmonary pressure(Paw- Ppl= PL)distending the lung is + 20(30-10); the pulmonary blood vessels are compressed by the positive-pressure breath and the transvascular pressure(Pcap-Ppl)is low(assume 12-10=2). When spontaneous effort is added(b),the PL(30+20=+50)is greater, thereby increasing the VT and causing lung injury. In addition, the
negative Ppl(-20)distends the pulmonary blood vessels and increases perfusion; the transvascular
pressure is greater(assume 8--20=+28), increasing fluid shift to the interstitium. In the presence of injury, permeability(and therefore propensity to alveolar edema)is increased.
Paw, airway pressure; Pcap, capillary hydrostatic pressure; Ppl, pleural pressure.
Reprinted with permission of the American Thoracic Society. Copyright © 2017 American Thoracic Society.
Cite: Yoshida T, Fujino Y, Amato MB, Kavanagh BP/ 2017 /Fifty Years of Research in ARDS. Spontaneous Breathing during Mechanical Ventilation. Risks, Mechanisms, and Management./ Am J Respir Crit Care Med. / 195 / 985-992. Ppl +10 Ppl -20 Interstitial fluid Paw +30 Paw +30 PCap +12 PCap +8 (a) (b)
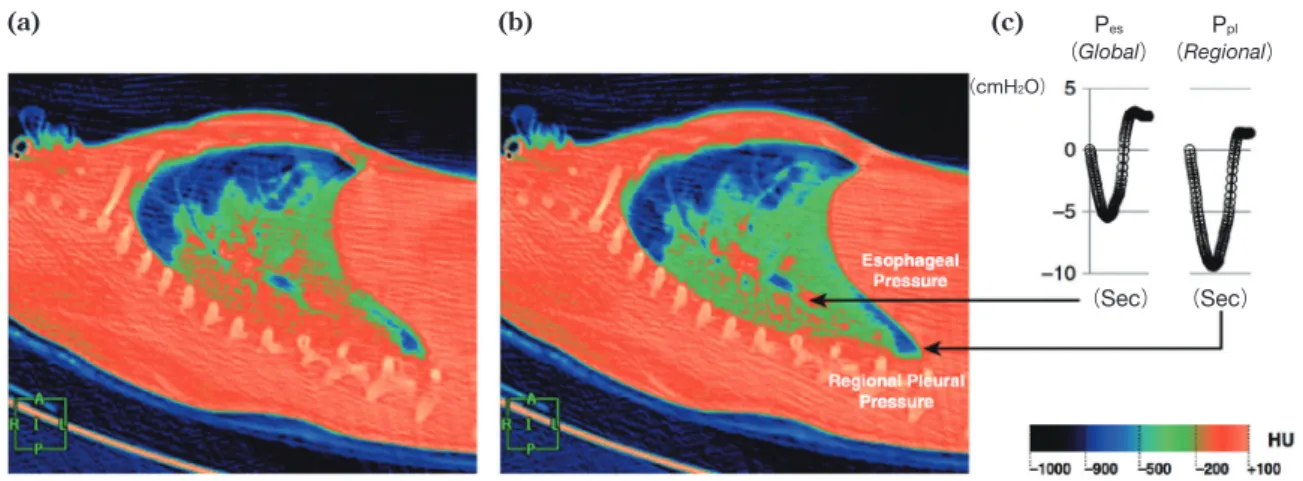
Fig. 2 Spontaneous effort and distribution of regional ventilation and pleural pressure
Dynamic computed tomographic scan in end-expiration(a)demonstrates that the aerated lung(blue)is nondepen-dent, while the dependent lung is densely atelectatic(red). At end-inspiration during a spontaneous breath(b), there is little change in the nondependent aerated lung(blue); the dependent lung, previously densely atelectatic (red), is now partially aerated(green/red)(i.e., tidal recruitment). The inspiratory pleural pressure traces(c),
measured at the arrow tips, show the negative deflections(“swings”)in regional Ppl and global Pes
during inspira-tion. However, the “swing” in regional Ppl is greater(by twofold)than the “swing” in Pes, indicating that
diaphragm contraction results in greater distending pressure applied to the regional lung near the diaphragm, compared with the pressure transmitted to the remainder of the lung(i.e., Pes).
A, anterior; HU, Hounsfield units; I, inferior; L, left; P, posterior; Pes, esophageal pressure; Ppl, pleural pressure; R,
right.
Reprinted with permission of the American Thoracic Society. Copyright © 2017 American Thoracic Society. Cite: Yoshida T, Fujino Y, Amato MB, Kavanagh BP/ 2017 /Fifty Years of Research in ARDS. Spontaneous
Breathing during Mechanical Ventilation. Risks, Mechanisms, and Management./ Am J Respir Crit Care Med. / 195 / 985-992.
減により肺循環血液量は増加する
17),18)。
Ⅳ.自発呼吸を温存するメリットとデメリット
1
)
メリット
呼吸筋の活動により生じた陰圧の胸膜圧は均一に肺
表面に伝播し,経肺圧を増加させる。このため,低い
気道内圧で肺リクルートメントを促すことが可能とな
り,呼気終末肺容量の維持,すなわち無気肺の予防に
効果的である
19)。また,横隔膜の筋緊張は腹圧によ
る胸腔(呼吸器系)への圧迫を軽減する。このように
自発呼吸を温存した人工呼吸管理は最も侵襲性の低い
肺 リ ク ル ー ト メ ン ト と な る
19)。 横 隔 膜 の 収 縮 は
dependent lungである背側領域優位の換気を促すた
め,換気血流ミスマッチ(V
・/Q
・ミスマッチ)の改善に
も寄与する。同時に肺血流量増加も促すため酸素化の
改善に大きく貢献する
5),6)。また,呼吸筋の周期的な
緊張と弛緩は,呼吸筋の機能不全や廃用症候群の予防
となる。これらの理由により,人工呼吸中に自発呼吸
を温存することは古くから推奨されてきた
5),6),8),20)。
例えばmild〜moderate ARDSでは自発呼吸を温存す
ることで,ガス交換と含気分布が改善すると多数報告
されている
6),13),15),21),22)。2001年にPutensenらは急性
肺損傷症例において,自発呼吸を温存した人工呼吸群
でICU滞在日数も短縮することを報告している
6)。し
たがって,正常〜重症度の高くない肺傷害症例では自
発呼吸は温存されるべきである。しかし,これまで報
告された基礎および臨床研究の多くは,重症肺傷害の
症例を除外していることに留意する必要がある。
2
)
デメリット
人工呼吸管理中の自発呼吸の存在は前述の通り,肺
コンプライアンスを改善させる。しかし,重症肺傷害
症例では自発呼吸努力の存在は必ずしもメリットとは
ならない。重症肺傷害症例において肺保護換気戦略に
則って気道内圧(プラトー圧)を低く管理していたと
しても,呼吸困難感などにより強い呼吸努力から胸膜
圧に過度な陰性変化が生じた場合,経肺圧は非常に高
くなり肺損傷が悪化する可能性がある
13),23)。過剰な
呼吸努力は,CO
2貯留,アシドーシス,低酸素血症,痛
み,発熱,全身または肺血管の炎症などの際に認めや
すく,臨床的にはsevere ARDSの病態を呈している
ことが多い。YoshidaらはウサギARDSモデルを用い
て人工呼吸中の気道内圧(プラトー圧)を制限しても,
強い自発呼吸によって病理組織学的肺損傷の悪化と
Pes (Global) (cmH2O) (Sec) (Sec) Ppl (Regional) (a) (b) (c)CT画像によるconsolidationの増加を認めたと報告し
ている
13),23)。
さらに肺保護換気戦略に従って1回換気量を制限し
た場合,人工呼吸管理中の自発呼吸努力はpendelluft
現象を惹起するため,肺局所の過伸展が生じる可能性
がある
16)。Pendelluft現象はブタを用いた実験だけで
なく,術後ARDS患者においても確認されているが,
pendelluft現象が肺傷害の直接の誘引となることは未
だ証明されていない。しかし,短時間で虚脱と過伸展
が入れ替わることは肺に悪影響を及ぼしているものと
推察される。
最後に過剰な呼吸努力は,吸気筋だけでなく呼気筋
にも過剰収縮をもたらす。この結果,呼気時に横隔膜
の頭側シフトと胸膜圧の上昇が生じ,呼気時経肺圧は
低下する。この結果,呼気時肺容量の減少すなわち肺
胞の虚脱や低酸素血症が起こる可能性がある
24)。こ
れらの理由から,人工呼吸管理中は過度な自発呼吸努
力を避けることが,人工呼吸器関連肺傷害の予防,す
なわち肺保護換気戦略に効果的な方法となる。
Ⅴ.人工呼吸器設定に関する推奨方法
人工呼吸管理中の自発呼吸努力が強くなるほど,肺
損傷の危険性は高まる。つまり,肺損傷を予防する最
善の方法は呼吸努力の強度を最小限に抑えることであ
る。そして,過度な自発呼吸努力が存在する場合に筋
弛緩により自発呼吸を抑えることは,肺保護換気戦略
に最適な方法となる。2010年にPapazianらは,重症
ARDS症例(PaO
2/F
IO
2<120 mmHg)の早期に48時
間筋弛緩薬を投与した群では非投与群と比較して生存
率が13.8%上昇しただけでなく,圧損傷の発生頻度も
低下したと報告している
25)。十分な鎮静と鎮痛,CO
2の貯留を防ぎ,アシドーシスを補正することによって
も呼吸努力は軽減される。
1回換気量を制限することは必ずしも推奨しない。
なぜなら1回換気量の減少は,特に従量式呼吸器設定
の場合には,呼吸努力の強度を上げる可能性があるか
らである。過度の呼吸努力はpendelluft現象を増悪し,
局所の圧損傷を引き起こすだけではなく,含気肺から
背側の無気肺領域へのガス移動に伴い,肺野全体とし
ては1回換気量が減少する可能性もある。
患者と人工呼吸器の同調性を保つことは,非常に重
要である。従量式(volume control)換気では自発呼吸
と人工呼吸器が非同期を生じやすく,呼吸努力が過度
となりダブルトリガ(double triggering)を起こしや
すくなる。鎮静や鎮痛を増やすよりも呼吸器設定を見
直して,従圧式(pressure control)または圧補助
(pressure support)モードに切り替えるほうが,ダブ
ルトリガの予防に有効な場合もある
26)〜28)。
最後に,肺リクルートメントと十分なPEEPは肺コ
ンプライアンスを改善し,呼吸努力の強度を低下させ
る可能性がある
15)。コンプライアンスの改善は肺の
solid-like behavior軽減をもたらし,呼吸努力強度の低
下やpendelluft現象の抑制にも効果があると考えられ
る
16)。また,肺リクルートメントによって機能的残
気量を増やすことができれば,横隔膜の形態は平坦に
近づき,横隔膜の筋繊維長が短縮し収縮力は減弱す
る
29)ため,胸膜圧を減弱しpendelluft現象を緩和する
可能性がある
15)。
Ⅵ.結 語
人工呼吸管理中の自発呼吸の存在には一長一短があ
るが,自発呼吸を温存するpartial ventilatory support
と筋弛緩により自発呼吸を完全に抑制するfull
venti-latory supportは決して相反する治療法ではなく,
ARDSの重症度と肺保護換気戦略に基づいてどちらも
選択され得る呼吸管理である。人工呼吸管理中の自発
呼 吸 温 存 の 問 題 点 は,自 発 呼 吸 の 強 度,経 肺 圧,
pendelluft現象の発生の有無など通常のモニターでは
予測困難なものであるため,過剰な自発呼吸努力の発
生を避けた人工呼吸器管理を目指す必要がある。
利益相反の開示吉田健史はSociety of Emergency and Critical Care MedicineおよびTaiwan Society of Critical Care Medicine より講演料を得ている。また,Restracompより研究費を得 ている。その他の著者には規定された利益相反(conflict of interest, COI)はない。 文 献 1) Brower RG, Fessler HE. Mechanical ventilation in acute lung injury and acute respiratory distress syndrome. Clin Chest Med 2000;21:491-510viii. 2) Brower RG, Ware LB, Berthiaume Y, et al. Treatment of ARDS. Chest 2001;120:1347-67.
3) Amato MB, Barbas CS, Medeiros DM, et al. Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome. N Engl J Med 1998;338: 347-54.
4) Acute Respiratory Distress Syndrome Network, Brower RG, Matthay MA, et al. Ventilation with lower tidal volumes compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000;342:1301-8.
5) Stock MC, Downs JB, Frolicher DA. Airway pressure release ventilation. Crit Care Med 1987;15:462-6.
6) Putensen C, Zech S, Wrigge H, et al. Long-term effects of spontaneous breathing during ventilatory support in patients with acute lung injury. Am J Respir Crit Care Med 2001;164:43-9.
7) Levine S, Nguyen T, Taylor N, et al. Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. N Engl J Med 2008;358:1327-35.
8) Esteban A, Frutos-Vivar F, Muriel A, et al. Evolution of mortality over time in patients receiving mechanical ventilation. Am J Respir Crit Care Med 2013;188:220-30. 9) Talmor D, Sarge T, O’Donnell CR, et al. Esophageal and
transpulmonary pressures in acute respiratory failure. Crit Care Med 2006;34:1389-94.
10) Briel M, Meade M, Mercat A, et al. Higher vs lower positive end-expiratory pressure in patients with acute lung injury and acute respiratory distress syndrome: systematic review and meta-analysis. JAMA 2010;303: 865-73.
11) Buytendijk JH. Intraesophageal pressure and lung elasticity [thesis]. Groningen, the Netherlands: University of Groningen; 1949.
12) Akoumianaki E, Maggiore SM, Valenza F, et al; PLUG Working Group (Acute Respiratory Failure Section of the European Society of Intensive Care Medicine). The appli-cation of esophageal pressure measurement in patients with respiratory failure. Am J Respir Crit Care Med 2014;189:520-31.
13) Yoshida T, Uchiyama A, Matsuura N, et al. Spontaneous breathing during lung-protective ventilation in an experi-mental acute lung injury model: high transpulmonary pressure associated with strong spontaneous breathing effort may worsen lung injury. Crit Care Med 2012;40: 1578-85.
14) Yoshida T, Uchiyama A, Fujino Y. The role of sponta-neous effort during mechanical ventilation: normal lung versus injured lung. J Intensive Care 2015;3:18.
15) Yoshida T, Roldan R, Beraldo MA, et al. Spontaneous effort during mechanical ventilation: maximal injury with less positive end-expiratory pressure. Crit Care Med 2016;44:e678-88.
16) Yoshida T, Torsani V, Gomes S, et al. Spontaneous effort causes occult pendelluft during mechanical ventilation. Am J Respir Crit Care Med 2013;188:1420-7.
17) Mauri T, Yoshida T, Bellani G, et al; PLeUral pressure
working Group (PLUG--Acute Respiratory Failure section of the European Society of Intensive Care Medicine). Esophageal and transpulmonary pressure in the clinical setting: meaning, usefulness and perspectives. Intensive Care Med 2016;42:1360-73.
18) Eckstein JW, Hamilton WK. Changes in transmural central venous pressure in man during hyperventilation. J Clin Invest 1958;37:1537-41.
19) Keenan JC, Formenti P, Marini JJ. Lung recruitment in acute respiratory distress syndrome: what is the best strategy?. Curr Opin Crit Care 2014;20:63-8.
20) Marini JJ. Spontaneously regulated vs. controlled venti-lation of acute lung injury/acute respiratory distress syndrome. Curr Opin Crit Care 2011;17:24-9.
21) Wrigge H, Zinserling J, Neumann P, et al. Spontaneous breathing improves lung aeration in oleic acid-induced lung injury. Anesthesiology 2003;99:376-84.
22) Hering R, Peters D, Zinserling J, et al. Effects of sponta-neous breathing during airway pressure release venti-lation on renal perfusion and function in patients with acute lung injury. Intensive Care Med 2002;28:1426-33. 23) Yoshida T, Uchiyama A, Matsuura N, et al. The
comparison of spontaneous breathing and muscle paralysis in two different severities of experimental lung injury. Crit Care Med 2013;41:536-45.
24) Coggeshall JW, Marini JJ, Newman JH. Improved oxygenation after muscle relaxation in adult respiratory distress syndrome. Arch Intern Med 1985;145:1718-20. 25) Papazian L, Forel JM, Gacouin A, et al; ACURASYS
Study Investigators. Neuromuscular blockers in early acute respiratory distress syndrome. N Engl J Med 2010;363:1107-16.
26) Kallet RH, Alonso JA, Luce JM, et al. Exacerbation of acute pulmonary edema during assisted mechanical ventilation using a low-tidal volume, lung-protective ventilator strategy. Chest 1999;116:1826-32.
27) Pohlman MC, McCallister KE, Schweickert WD, et al. Excessive tidal volume from breath stacking during lung-protective ventilation for acute lung injury. Crit Care Med 2008;36:3019-23.
28) Chanques G, Kress JP, Pohlman A, et al. Impact of venti-lator adjustment and sedation-analgesia practices on severe asynchrony in patients ventilated in assist-control mode. Crit Care Med 2013;41:2177-87.
29) Pengelly LD, Alderson AM, Milic-Emili J. Mechanics of the diaphragm. J Appl Physiol 1971;30:797-805.
Abstract
Pro and Cons of spontaneous breathing during mechanical ventilation
Hironori Ebishima
*1, Takeshi Yoshida
*2, 3, Akinori Uchiyama
*4*1 Intensive Care Unit, Osaka University Hospital *2 Keenan Research Centre, Li Ka Shing Knowledge Institute, St. Michael’s Hospital *3 Interdepartmental Division of Critical Care Medicine, University of Toronto *4 Department of Anesthesiology and Intensive Care Medicine, Osaka University Graduate School of Medicine *1 2-15 Yamadaoka, Suita, Osaka 565-0871, Japan *2 30 Bond street Toronto, ON, M5B IW8, Canada *3 190 Elizabeth street R. Fraser Elliott Building, 3-805 Tronto, ON M5G 2C4, Canada *4 2-2 Yamadaoka, Suita, Osaka 565-0871, Japan
Spontaneous breathing during mechanical ventilation has long been recognized as beneficial, since spontaneous breathing increases aeration and oxygenation and preserves diaphragmatic muscle function. Spontaneous effort also reduces the pleural pressure and increases the transpulmonary pressure. Unlike the situation in normal lungs, however, the change in transpulmonary pressure is not uniformly transmitted in injured lungs, resulting in the pendelluft phenomenon. Clinical data suggest that the vigorous effort of spontaneous breathing may cause or worsen acute lung injury by increasing the transpulmonary pressure and pendelluft phenomenon. Ventilator strategies for patients with acute respiratory distress syndrome with and without spontaneous breathing should not be conflicting, but rather compatible, if spontaneous effort is adequately controlled.
Key words: ① spontaneous breathing, ② mechanical ventilation, ③ acute respiratory distress syndrome, ④ ventilator-induced lung injury