Clinical, cytogenetic and molecular analyses of 17 neonates with transient abnormal myelopoiesis and non-constitutional trisomy 21
Ҳգࠐਹҡଁ৫Νͪ͢ඉඬ६ܗ 'RZQ ޫ܊ਫ਼ࣉ ྭྡজ
దٶ;ࢢࡋ๖Ҫఽָదմੵ
ਅ੧ं ߄ָָӅҫָݜڂՌ
үՌָҮ ঘࣉබସָ
ࢱ໌ ౮ୖ ݊ଢ
ࢨگद ґ౽ ӽ࿗
Keywords
Down syndrome, trisomy 21, transient abnormal myelopoiesis, myeloid leukemia, GATA1
Abstract
Background: Transient abnormal myelopoiesis (TAM) is a unique myeloproliferative disorder that occurs in neonates with constitutional trisomy 21/Down syndrome (DS).
Although TAM also develops in neonates without constitutional trisomy 21, the clinical, cytogenetic and molecular characteristics of those patients are not fully understood.
Procedure: We retrospectively evaluated the clinical and cytogenetic findings and GATA1 mutation status of 17 neonates with TAM and non-constitutional trisomy 21 tested for GATA1 mutations at our institute, and compared the findings with those of 64 neonates with TAM and constitutional trisomy 21/DS.
Results: DS clinical features were observed in 5 of the 17 (29%) patients. In all patients, both trisomy 21 and GATA1 mutations were detected in diagnostic samples.
Over a median follow-up of 33 (range, 0–139) months, early death (<6 months of age) occurred in four patients (24%). Overall and event-free survivals were not significantly different between the patients with TAM and non-constitutional trisomy 21 and those
with TAM and constitutional trisomy 21/DS (5-year overall survival: 76 ± 10% vs. 53 ± 13%, P = 0.40; 5-year event-free survival: 55 ± 13% vs. 48 ± 12%, P = 0.90). The 5- year cumulative incidence of progression to myeloid leukemia of DS was also similar between the groups (21% vs. 24%, P = 0.80).
Conclusions: Patients with TAM and non-constitutional trisomy 21 exhibited similar biology and outcomes to those with TAM and constitutional trisomy 21/DS. The possibility of TAM should be considered even in phenotypically normal neonates with TAM symptoms, for appropriate management.
INTRODUCTION
Transient abnormal myelopoiesis (TAM) is a unique myeloproliferative disorder that occurs in 5–10% of neonates with constitutional trisomy 21/Down syndrome (DS).1-3 Most cases resolve spontaneously within 3 months. However, approximately 20% of patients with TAM die from organ failure including liver failure, and 20–30% of surviving patients subsequently develop myeloid leukemia of DS (ML-DS) during the first 4 years of life.4-7 Germline trisomy 21 and prenatally acquired GATA1 mutations cooperatively contribute to the development of TAM.8-13 TAM also develops in neonates without constitutional trisomy 21, and there have been several case reports on neonates with TAM and non-constitutional trisomy 21, some of which include literature
reviews.14-19 However, the clinical, cytogenetic and molecular characteristics of these patients are not fully understood. To define the characteristics of neonates with TAM and non-constitutional trisomy 21, we retrospectively evaluated the clinical and cytogenetic findings and GATA1 mutation status of 17 neonates with TAM and non- constitutional trisomy 21 who had undergone GATA1 mutation testing at our institute. In addition, we compared the findings with those of 64 neonates with TAM and
constitutional trisomy 21/DS.
PATIENTS AND METHODS Patients
This study was approved by the Ethics Committee of Hirosaki University Graduate School of Medicine. All clinical samples were evaluated after obtaining informed consent from the patients’ guardians in accordance with the Declaration of Helsinki.
Between April 2003 and March 2019, 335 patients with TAM were analyzed for GATA1 mutations at Hirosaki University upon request from referring hospitals. Patients
enrolled in the Japanese Pediatric Leukemia/Lymphoma Study Group, TAM-10 study were not included in this study.
We collected the following clinical data: sex, gestational age, birth weight, age at diagnosis of TAM, clinical features of DS, and clinical symptoms at diagnosis including effusions, bleeding diathesis, hepatomegaly, splenomegaly and jaundice. The following laboratory data at diagnosis were also obtained: white blood cell count, percentage of blasts, hemoglobin level, platelet count, levels of aspartate aminotransaminase (AST), alanine aminotransferase and total and direct bilirubin, and cytogenetic findings of diagnostic samples.
Twenty-five neonates were suspected of having TAM and non-constitutional trisomy 21 according to their clinical and/or cytogenetic findings at diagnosis, and
cytogenetic data from germline samples were collected by a standardized questionnaire.
The sources of the germline samples were variable among the patients and included peripheral blood, bone marrow, buccal mucosa and skin fibroblasts. If disomy 21 cells were detected in the diagnostic and/or germline samples by G-banding and/or
fluorescence in situ hybridization, the patient was considered to have non-constitutional trisomy 21.
GATA1 mutation analysis
GATA1 mutations were analyzed by Sanger sequencing using genomic DNA and complementary DNA prepared from peripheral blood at diagnosis of TAM as described previously.20 For patients in whom GATA1 mutations were not detected by Sanger sequencing, targeted next-generation sequencing was performed. 20
Statistical analysis
Clinical parameters were compared between patients with TAM and non-constitutional trisomy 21 and those with TAM and constitutional trisomy 21/DS who had undergone GATA1 mutation testing at our institute during the same period. Differences in the distribution of individual parameters between the two groups were analyzed using
Fisher’s exact test for categorical variables and the Mann–Whitney U test for
continuous variables. The Kaplan–Meier method was used to calculate overall survival (OS) and event-free survival (EFS), which were compared between groups by the log- rank test. OS was defined as the time from diagnosis to death from any cause, and EFS was defined as the time from diagnosis to progression to ML-DS or death from any cause. The cumulative incidence of progression to ML-DS was analyzed using the Gray test. A P-value < 0.05 was considered statistically significant. Early death was defined as death from any cause within the first 6 months of life.
RESULTS
Patient characteristics
Seventeen neonates were confirmed to have TAM and non-constitutional trisomy 21 based on the cytogenetic findings at diagnosis and/or during remission of TAM. Their clinical and cytogenetic findings and GATA1 mutation status are summarized in Table 1 and Supplementary Table S1. In all 17 patients, trisomy 21 was detected in the
diagnostic samples. Cytogenetic findings in germline samples during remission were available in 11 patients. The facial features of DS and/or congenital heart disease were observed in 5 of 17 (29%) patients. Other anomalies were not seen in any patients.
GATA1 mutations were successfully identified in leukemic blasts in all 17 patients. Nine patients (53%) were treated with low-dose cytarabine. Over a median follow-up of 33 months (range, 0–139 months), early death occurred in four patients (24%), all of whom died of hepatic failure. Of the 13 patients without early death, 3 (23%) subsequently developed ML-DS at the age of 7, 17 and 10 months, respectively. Two of these patients (patient # 3 and #10) had available paired TAM and ML-DS samples, and the same GATA1 mutations were identified in both sample types in both patients (c.129_148dup and c.167_174dup, respectively). All three patients were treated with chemotherapy and remained in continuous complete remission at the time of analysis.
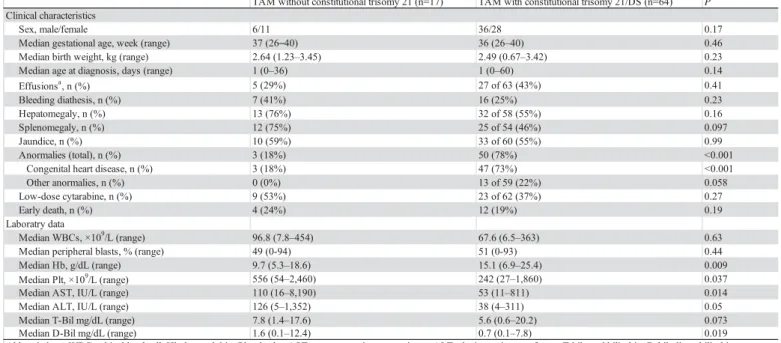
Comparison of the clinical characteristics between patients with TAM and non- constitutional trisomy 21 and those with TAM and constitutional trisomy 21/DS The 64 patients with TAM and constitutional trisomy 21/DS had sufficient clinical data (Supplementary Table S2), which were compared with those of the 17 patients with TAM and non-constitutional trisomy 21. There were no differences in most of the clinical characteristics, including sex, gestational age, birth weight, age at diagnosis and clinical symptoms, between patients with TAM and non-constitutional trisomy 21 and those with TAM and constitutional trisomy 21/DS (Table 2). As expected, the former
were significantly less likely than the latter to have any anomalies (18% vs. 78%, P <
0.001). Although the median white blood cell count was higher in the patients with TAM and non-constitutional trisomy 21, the difference between the groups was not significant (96.8 vs. 67.6 × 109/L, P = 0.63). There was also no difference in the percentage of blasts between the two groups (49% vs. 51%, P = 0.44). However, the patients with TAM and non-constitutional trisomy 21 had a significantly lower hemoglobin level and higher platelet count than those in the patients with TAM and constitutional trisomy 21/DS (P = 0.009 and 0.037, respectively). The levels of AST and direct bilirubin were significantly higher in the former than the latter group (P = 0.014 and 0.019, respectively).
The OS rate was higher in the patients with TAM and non-constitutional trisomy 21 than in those with TAM and constitutional trisomy 21/DS, but the difference was not significant (5-year OS, 76 ± 10% vs. 53 ± 13%, P = 0.40; Figure 1A). The EFS rate and cumulative incidence rate of progression to ML-DS were also not significantly different between the two groups (5-year EFS: 55 ± 13% vs. 48 ± 12%, P = 0.90; 5-year
cumulative incidence of ML-DS: 21% vs. 24%, P = 0.80; Figure 1B and 1C).
DISCUSSION
GATA1 mutation testing was not routinely conducted in previously reported neonates with TAM and non-constitutional trisomy 21.14-19 Rozen et al. performed a literature review of 14 patients with TAM that was not associated with DS and reported that GATA1 mutations were analyzed in only 8 patients, all of whom had GATA1 mutations as well as trisomy 21 in leukemic blasts, indicating that the biology of TAM without constitutional trisomy 21 was similar to that of TAM with constitutional trisomy 21/DS.19 After the report of Rozen et al, there have also been several case reports of TAM without constitutional trisomy 21 but harboring both trisomy 21 and GATA1 mutations in leukemic blasts.21-24 Here, we present the cytogenetic findings and GATA1 mutation status of a series of 17 patients with TAM and non-constitutional trisomy 21 who had been tested for GATA1 mutations at a single institute. All 17 patients harbored both trisomy 21 and GATA1 mutations in leukemic blasts, clearly showing that the molecular pathogenesis is common between TAM with and without constitutional trisomy 21.
In this study, the incidences of early death and progression to ML-DS in patients with TAM and non-constitutional trisomy 21 were 24% and 23%, respectively, which were similar to those found in larger clinical studies on patients with TAM and mainly constitutional trisomy 21/DS.4-7 There was also no significant difference in OS, EFS or
incidence of progression to ML-DS between our patients with TAM and non-
constitutional trisomy 21 and those with TAM and constitutional trisomy 21/DS who had also been tested for GATA1 mutations at our institute. Phenotypically normal neonates with TAM can be misdiagnosed with congenital acute myeloid leukemia and treated with intensified chemotherapy. The possibility of TAM should be considered in all neonates who present with symptoms consistent with TAM to avoid overtreatment. It is also indicated that patients with TAM and non-constitutional trisomy 21 need to be followed and monitored for the development of ML-DS in the same way as those with TAM and constitutional trisomy 21/DS.
Although the outcomes were similar between the two groups, it should be noted that three patients died after the age of 6 months in the group of TAM with
constitutional trisomy 21/DS in contrast to no deaths in the group of TAM without constitutional trisomy 21. The causes of death of the three patients were respiratory syncytial virus infection during chemotherapy for ML-DS, hematemesis of unknown origin, and ML-DS, respectively. Because patients with constitutional trisomy 21/DS are more likely to have significant congenital abnormalities such as congenital heart disease, gastrointestinal anomalies and immunodeficiencies, death from non-
hematological causes might be more common in this population than in patients with
TAM and non-constitutional trisomy 21.
Although there were no differences in most of the clinical characteristics between the two groups, the hemoglobin level was significantly lower and platelet count higher in patients with TAM and non-constitutional trisomy 21 than in those with TAM and constitutional trisomy 21/DS. Higher hemoglobin levels and lower platelet counts have been reported in DS neonates compared with non-DS neonates. 25,26 Although the exact reasons are unclear, the differences in the hemoglobin level and platelet count might reflect the nature of background hematopoietic cells with different cytogenetics
(constitutional trisomy 21/DS, trisomy 21; non-constitutional trisomy 21, disomy 21 or mixture of disomy and trisomy 21).
The main limitations of this study were the small number of patients and
retrospective nature. Because patients with TAM and non-constitutional trisomy 21 are very rare, long-term nationwide or international studies are warranted to determine the exact characteristics of these patients.
In conclusion, we retrospectively evaluated the clinical and cytogenetic findings and GATA1 mutation status of 17 patients with TAM and non-constitutional trisomy 21, who had similar biology and outcomes to those of patients with TAM and constitutional trisomy 21/DS. The possibility of TAM should be considered even in phenotypically
normal neonates who present with symptoms consistent with TAM to manage them appropriately. Compared with patients with TAM and constitutional trisomy 21/DS, those with TAM and non-constitutional trisomy 21 had a significantly lower
hemoglobin level, higher platelet count and higher levels of AST and direct bilirubin, although the number of the latter patients was small. More patients need to be evaluated to define the clinical, cytogenetic and molecular characteristics of patients with TAM and non-constitutional trisomy 21 more precisely.
CONFLICT OF INTEREST
The authors declare no conflicts of interest.
ACKNOWLEDGMENTS
The authors thank Shingo Morinaga (National Hospital Organization Kumamoto Medical Center), Rintaro Ono (St. Luke’s International Hospital), Takahiro Ueda
(Nippon Medical School Hospital), Tsuyako Iwai (Shikoku Medical Center for Children and Adults), Rie Kuroda (Kanazawa University), Kazuhiro Kogawa (National Defense Medical College), Yuko Cho (Hokkaido University Hospital), Yuko Nomura (Fukuoka University Hospital), Yasushi Ishida (Ehime Prefectural Central Hospital), Atsushi
Nakao (Japanese Red Cross Medical Center), Keigo Hamahata (Japanese Red Cross Society Wakayama Medical Center), Miyuki Tanaka (Shinshu University), Daichi Sajiki (Japanese Red Cross Nagoya First Hospital), Mitsutaka Shiota (Kitano Hospital), Maho Sato (Osaka Women’s and Children’s Hospital), Keita Igarashi (Sapporo Medical University), Yuya Sato (Dokkyo Medical University) and Genichiro Sotodate (Iwate Medical University) for providing the patient samples and data. We also thank H. Kudo, Y. Kudo and A. Mikami for their technical assistance with the GATA1 mutation analysis.
This work was supported by JSPS KAKENHI (grant numbers JP26253061, JP18H04039 and JP18K07810) and the Project for Cancer Research and Therapeutic Evolution (JP18cm0106407) from the Japan Agency for Medical Research and Development (AMED).
REFERENCES
1. Lange B. The management of neoplastic disorders of haematopoiesis in children with Down’s syndrome. Br J Haematol 2000;110:512-524.
2. Zipursky A. Transient leukaemia - a benign form of leukaemia in newborn infants with trisomy 21. Br J Haematol 2003;120:930-938.
3. Pine SR, Guo Q, Yin C, et al. Incidence and clinical implications of GATA1 mutations in newborns with Down syndrome. Blood 2007;110:2128-2131.
4. Massey GV, Zipursky A, Chang MN, et al. A prospective study of the natural history of transient leukemia (TL) in neonates with Down syndrome (DS):
Children’s Oncology Group (COG) study POG-9481. Blood 2006;107(12):4606- 4613.
5. Klusmann JH, Creutzig U, Zimmermann M, et al. Treatment and prognostic impact of transient leukemia in neonates with Down syndrome. Blood 2008;111:2991- 2998.
6. Muramatsu H, Kato K, Watanabe N, et al. Risk factors for early death in neonates with Down syndrome and transient leukaemia. Br J Haematol 2008;142:610-615.
7. Gamis AS, Alonzo TA, Gerbing RB, et al. Natural history of transient
myeloproliferative disorder clinically diagnosed in Down syndrome neonates: a
report from the Children's Oncology Group Study A2971. Blood 2011;118:6752- 6759.
8. Wechsler J, Greene M, McDevitt MA, et al. Acquired mutations in GATA1 in the megakaryoblastic leukemia of Down syndrome. Nat Genet 2002;32:148-152.
9. Mundschau G, Gurbuxani S, Gamis AS, Greene ME, Arceci RJ, Crispino JD.
Mutagenesis of GATA1 is an initiating event in Down syndrome leukemogenesis.
Blood 2003;101:4298-4300.
10. Hitzler JK, Cheung J, Li Y, Scherer SW, Zipursky A. GATA1 mutations in transient leukemia and acute megakaryoblastic leukemia of Down syndrome. Blood
2003;101:4301-4304.
11. Rainis L, Bercovich D, Strehl S, et al. Mutations in exon 2 of GATA1 are early events in megakaryocytic malignancies associated with trisomy 21. Blood 2003;102:981-986.
12. Groet J, McElwaine S, Spinelli M, et al. Acquired mutations in GATA1 in neonates with Down's syndrome with transient myeloid disorder. Lancet 2003;361:1617- 1620.
13. Xu G, Nagano M, Kanezaki R, et al. Frequent mutations in the GATA-1 gene in the transient myeloproliferative disorder of Down syndrome. Blood 2003;102:2960-
2968.
14. Polski JM, Galambos C, Gale GB, et al. Acute megakaryoblastic leukemia after transient myeloproliferative disorder with clonal karyotype evolution in a phenotypically normal neonate. J Pediatr Hematol Oncol 2002;24:50-54.
15. Sandoval C, Pine SR, Guo Q, et al. Tetrasomy 21 transient leukemia with a GATA1 mutation in a phenotypically normal trisomy 21 mosaic infant: case report and review of the literature. Pediatr Blood Cancer 2005;44:85-91.
16. Magalhães IQ, Splendore A, Emerenciano M, et al. Transient neonatal
myeloproliferative disorder without Down syndrome and detection of GATA1 mutation. J Pediatr Hematol Oncol 2005;27:50-52.
17. Apollonsky N, Shende A, Ouansafi I, et al. Transient myeloproliferative disorder in neonates with and without Down syndrome: a tale of 2 syndromes. J Pediatr
Hematol Oncol 2008;30:860-864.
18. Kawase K, Azuma E, Ohshita H, et al. Risk factors for early death in transient myeloproliferative disorder without phenotypic features of Down syndrome: a case report and literature review. J Pediatr Hematol Oncol 2012;34:475-479.
19. Rozen L, Huybrechts S, Dedeken L, et al. Transient leukemia in a newborn without Down syndrome: case report and review of the literature. Eur J Pediatr
2014;173:1643-1647.
20. Terui K, Toki T, Taga T, et al. Highly sensitive detection of GATA1 mutations in patients with myeloid leukemia associated with Down syndrome by combining Sanger and targeted next generation sequencing. Genes Chromosomes Cancer 2019 Oct 13. doi: 10.1002/gcc.22816. [Epub ahead of print]
21. Corazza F, Astolfi A, Libri V, et al. Transient abnormal myelopoiesis in a phenotypically normal newborn with polyclonal trisomy 21. Int J Hematol 2014;99:794-797.
22. Ono R, Hasegawa D, Hirabayashi S, et al. Acute megakaryoblastic leukemia with acquired trisomy 21 and GATA1 mutations in phenotypically normal children. Eur J Pediatr 2015;174:525-531.
23. Ohkawa T, Miyamoto S, Sugie M, et al. Transient abnormal myelopoiesis in non- Down syndrome neonate. Pediatr Int 2015;57:e14-17.
24. Salvatori G, Foligno S, Sirleto P, et al. Sometimes it is better to wait: First Italian case of a newborn with transient abnormal myelopoiesis and a favorable prognosis.
Oncol Lett 2017;13:191-195.
25. Henry E, Walker D, Wiedmeier SE, et al. Hematological abnormalities during the first week of life among neonates with down syndrome. Am J Med Genet A
2007;143A:42-50.
26. Roberts I, Alford K, Hall G, et al. GATA1-mutant clones are frequent and often unsuspected in babies with Down syndrome: identification of a population at risk of leukemia. Blood 2013;122:3908-3917.
TABLE 1 Clinical, cytogenetic and molecular characteristics of 17 neonates with TAM and non-constitutional trisomy 21 Patient
no. Sex
Age at diagnosis
(days) Facial features
of DS
Congenital heart disease
Cytogenetics at diagnosis (samples and methods)
Cytogenetics during remission
(samples and methods) GATA1 mutation Low-dose cytarabine EFS
(months) OS (months)
Outcome (cause of death)
1 F 36 No No 47,XX,+21[18]/46,XX[2] (PB, G-banding) Trisomy 21 5-6% (PB, FISH) c.-19-53_76del148 No 56+ 56+ CCR
2 F 22 Yes No 47,XX,+21[5],46,XX[15] (PB, G-banding, PHA+) NA c.2T>C No 33+ 33+ CCR
3 M 13 No No 48,XY,+21,+mar[19] (PB, G-banding, PHA-)
48,XY,+21,+mar[19] (BM, G-banding, PHA-) 46,XY[20] (PB, G-banding, PHA+)
Disomy 21 100/100 (Buccala, FISH) 46,XY[20] (BM, G-banding, PHA-)
c.129_148dup No 7+ 139+ Progression to ML-DS
4 F 0 No No Trisomy 21 97% (PB, FISH) Disomy 21 100/100 (PB, FISH) c.1A>C Yes 18+ 18+ CCR
5 M 1 No No 47,XY,inv(2)(p11.2;q13),+21 (PB, G-banding) Disomy 21 99/100, trisomy 21 1/100
(Buccal, FISH)
c.231_232dup Yes 0 0 Early death (liver failure)
6 M 1 No No 46,XY,i(21)(q10)/46,XY(18/21) (PB, G-banding, PHA+) NA c.4G>T Yes 5 5 Early death (liver failure)
7 F 1 No No 47,XX,+21 [20/20] (PB, G-banding)
Disomy 21 27.5%, trisomy 21 72.5% (PB, FISH)
Trisomy 21 0% (PB, FISH) c.4G>T Yes 115+ 115+ CCR
8 F 3 No No 47,XX,+21 (PB, G-banding) Trisomy 21 0/75 (Buccal, FISH) c.219A>C Yes 3+ 3+ CCR
9 F 17 No No 47,XX,+21[15/20]/46,XX [5/20] (BM, G-banding, PHA-) NA c.183_184insTAG No 13+ 13+ CCR
10 F 0 No No 47,XX,+21[14/20]/46,XX[6/20] (BM, G-banding) 46,XX (PB, G-banding, PHA+)
Disomy 21 100/100 (Buccal, FISH)
c.167_174dup No 17+ 72+ Progression to ML-DS
11 F 4 No No 47,XX,+21[15/20]/46,XX[5/20] (BM, G-banding) 46,XY (PB, FISH) c.1A>C No 47+ 47+ CCR
12 F 0 Yes VSD 47,XX,+21[27]/46,XX[23] (PB, Gbanding, PHA+) NA c.3G>A Yes 1 1 Early death (liver failure)
13 M 0 Yes No 47,XY,+21[20/20] (PB, G-banding) Disomy 21 99/100, trisomy 21 1/100
(Buccal, FISH)
c.1A>G Yes 47+ 47+ CCR
14 F 0 No No 47,XX,+21(PB, G-banding)
Trisomy 21 36/100, disomy 21 64/100 (PB, FISH)
Trisomy 21 0/100 (Buccal, FISH) Trisomy 21 2/100 (PB, FISH)
c.85G>T Yes 45+ 45+ CCR
15 M 7 Yes ASD 47,XX,+21[15/20]/46,XX [5/20] (PB, G-banding, PHA+) NA c.-19-1G>A No 10+ 34+ Progression to ML-DS
16 M 1 No AVSD 47,XY,+21[16]/46,XY[14] (PB, G-banding, PHA+) NA c.174_175insTGGCTGCAGCTGCG No 2 2 Early death (liver failure)
17 F 1 No No 47,XX,+21[26/50]/46,XX[24/50] (PB, G-banding, PHA+)
47,XX,+21[20]䠄BM, G-banding, PHA-䠅 46,XX[30/30] (Skinb, G-banding, PHA+) Trisomy 21 0/1000 (Skin, FISH)
c.220G>A Yes 11+ 11+ CCR
aBuccal, buccal mucosa.
bSkin, skin fibroblasts.
Abbreviations: M, male; F, female; ASD, atrial septal defect; AVSD, atrioventricular septal defect; VSD, ventricular septal defect; PB, peripheral blood; BM, bone marrow; FISH, fluorescence in situ hybridization; PHA, phytohemagglutinin; NA, not available; ND, not determined; EFS, event-free survival; OS, overall survival; CCR, continuous complete remission; ML-DS, myeloid leukemia of Down syndrome.
TABLE 2 Comparison of the clinical characteristics between patients with TAM and non-constitutional trisomy 21 and those with TAM and constitutional trisomy 21/DS TAM without constitutional trisomy 21 (n=17) TAM with constitutional trisomy 21/DS (n=64) P Clinical characteristics
Sex, male/female 6/11 36/28 0.17
Median gestational age, week (range) 37 (26–40) 36 (26–40) 0.46
Median birth weight, kg (range) 2.64 (1.23–3.45) 2.49 (0.67–3.42) 0.23
Median age at diagnosis, days (range) 1 (0–36) 1 (0–60) 0.14
Effusionsa, n (%) 5 (29%) 27 of 63 (43%) 0.41
Bleeding diathesis, n (%) 7 (41%) 16 (25%) 0.23
Hepatomegaly, n (%) 13 (76%) 32 of 58 (55%) 0.16
Splenomegaly, n (%) 12 (75%) 25 of 54 (46%) 0.097
Jaundice, n (%) 10 (59%) 33 of 60 (55%) 0.99
Anormalies (total), n (%) 3 (18%) 50 (78%) <0.001
Congenital heart disease, n (%) 3 (18%) 47 (73%) <0.001
Other anormalies, n (%) 0 (0%) 13 of 59 (22%) 0.058
Low-dose cytarabine, n (%) 9 (53%) 23 of 62 (37%) 0.27
Early death, n (%) 4 (24%) 12 (19%) 0.19
Laboratry data
Median WBCs, ×109/L (range) 96.8 (7.8–454) 67.6 (6.5–363) 0.63
Median peripheral blasts, % (range) 49 (0-94) 51 (0-93) 0.44
Median Hb, g/dL (range) 9.7 (5.3–18.6) 15.1 (6.9–25.4) 0.009
Median Plt, ×109/L (range) 556 (54–2,460) 242 (27–1,860) 0.037
Median AST, IU/L (range) 110 (16–8,190) 53 (11–811) 0.014
Median ALT, IU/L (range) 126 (5–1,352) 38 (4–311) 0.05
Median T-Bil mg/dL (range) 7.8 (1.4–17.6) 5.6 (0.6–20.2) 0.073
Median D-Bil mg/dL (range) 1.6 (0.1–12.4) 0.7 (0.1–7.8) 0.019
aEffusions include ascites, pleural effusion, pericardial effusion, anasarca and fetal hydrops.
Abbreviations: WBC, white blood cell; Hb, hemoglobin; Plt, platelet; AST, aspartate aminotransaminase; ALT, alanine aminotransferase; T-bil, total bilirubin; D-bil, direct-bilirubin.
Supplementary Table S1 Clinical and laboratory findings of 17 neonates with TAM and non-constitutional trisomy 21 Patient
no.
GA (week)
Birth weight
(kg) Effusionsa Bleeding
diathesis Hepatomegaly Splenomegaly Jaundice WBC (×109/L) Blast (%) Hb (g/dL) Plt (×109/L) AST (IU/L) ALT (IU/L) T-bil (mg/dL) D-bil (mg/dL)
1 37 2.5 - - + + + 34.6 48 7.1 579 64 47 7.4 4.7
2 38 3.1 - - + + + 7.8 0 7.3 195 68 39 5.7 3.6
3 40 3.5 - + - - - 11.6 37 12.4 54 16 12 3.3 0.6
4 40 3.1 - - + + + 119.0 94 12.2 556 501 231 5.8 0.7
5 34 2.0 - - + + + 316.6 90 7.0 183 8,190 1,352 3.7 NA
6 38 2.6 - + + + + 105.5 72 8.5 944 3,866 473 16.5 5.5
7 39 2.8 + + + + + 98.3 60 11.1 1,068 4,341 653 4.3 1.9
8 37 2.6 - + + + + 356.9 85 7.1 873 356 407 9.7 6.9
9 36 2.5 - - + + - 15.0 18 6.7 234 29 9 5.8 2.2
10 26 1.2 + + - - - 47.6 34 5.3 247 4,393 717 7.8 2.9
11 37 2.6 - - - - + 35.2 17 14.3 1,260 72 72 14.5 1.0
12 35 3.1 + + + + + 96.8 49 14.0 2,460 4,949 1,154 17.6 12.4
13 36 2.4 + - + + - 434.8 92 9.7 361 86 126 13.9 1.1
14 31 1.9 + + + + - 454.0 75 6.3 206 110 11 1.4 0.2
15 36 3.0 - - - - - 51.4 37 18.6 587 27 5 12.5 0.6
16 36 3.4 - - + - + 32.6 14 13.8 108 493 191 9.6 1.2
17 34 2.3 - - + - - 103.0 79 18.0 938 43 9 8.0 0.1
Abbreviations: GA, gestational age; WBC, white blood cell count; Hb, hemoglobin; Plt, platelet count; AST, aspartate aminotransaminase; ALT,alanine aminotransferase; T-bil, total bilirubin; D-bil, direct-bilirubin; NA, not available
aEffusions include asites, pleural effusion, pericardial effusion, anasarca and fetal hydrops.
Supplementary Table S2 Clinical and laboratory findings of 64 neonates with TAM and constitutional trisomy 21/DS Patient
no. Sex Age at diagnosis (days)
GA (week) Birth weight (kg)
Effusionsa Bleeding
diathesis Hepatomegaly Splenomegaly Jaundice Congenital
heart disease Other anomalies WBC (×109/L) Blast (%) Hb (g/dL) Plt (×109/L) AST (IU/L) ALT (IU/L) T-bil (mg/dL) D-bil (mg/dL) Low-dose cytarabine
EFS (months)
OS (months)
Outcome (cause of death)
1 F 2 39 3.3 - - + - + PDA NA 49.9 30 14.1 676 35 24 15.3 0.9 No 68+ 68+ CCR
2 F 9 37 2.8 - - - - - No - 10.5 4 20.3 92 49 11 8.8 0.6 No 42+ 42+ CCR
3 F 1 37 2.9 - - + - NA No - 244.0 66 15.8 1,860 153 81 6.5 0.5 No 13 55+ Progression to ML-DS
4 F 3 34 2.4 + - - - + ASD - 38.3 24 16.4 623 53 76 2.4 0.7 No 2+ 2+ NA
5 F 0 37 3.1 - - + + + PS, VSD + 221.0 91 16.0 631 80 26 6.7 0.6 Yes 51+ 51+ CCR
6 M 2 38 2.8 + - + + + PDA, VSD - 149.7 86 15.5 400 80 82 2.2 0.1 Yes 52+ 52+ CCR
7 M 1 38 2.5 - - - - NA PDA, VSD NA 132.3 58 17.7 198 68 96 5.0 1.4 No 18 28 Progression to ML-DS (RSV infection)
8 F 1 36 2.1 + + + + NA PDA, VSD NA 220.0 86 11.8 317 197 40 2.4 0.4 No 0 0 Early death (heart failure)
9 M 0 32 1.9 + + + + + PDA - 166.0 93 11.6 391 455 198 5.0 0.5 No 0 0 Early death (liver failure)
10 M 2 36 2.7 + - + + + PDA - 93.3 60 18.9 404 81 131 13.5 0.7 Yes 1 1 Early death (NA)
11 M 2 NA 2.6 + + + NA + ASD + 363.2 50 14.5 94 229 157 18.3 2.3 Yes 35+ 35+ NA
12 M 0 33 1.7 - - - - - PDA - 290.8 92 12.2 133 49 8 2.4 0.3 Yes 1 1 Early death (liver failure)
13 M 0 37 2.4 + - + + + No - 136.6 69 10.3 302 77 41 4.5 1.6 Yes 1 1 Early death (liver failure)
14 M 0 34 2.1 + + + + + VSD + 33.1 8 9.1 149 42 7 2.7 0.6 Yes 3 3 Early death (liver failure)
15 M 1 34 1.4 - - - - + VSD - 9.0 5 15.6 58 18 6 6.6 0.7 No 20+ 20+ CCR
16 F 2 38 3.0 - - + + + No - 33.3 17 12.7 151 31 55 10.2 2.4 No 17+ 17+ CCR
17 F 1 38 2.0 - - NA NA - PDA, VSD - 53.3 66 19.7 109 62 94 5.6 0.8 No 16+ 16+ CCR
18 M 2 37 2.5 - - - - + CoA, VSD + 33.0 15 17.9 71 51 8 5.9 0.6 No 0+ 0+ CCR
19 M 0 31 1.6 + - + + - No - 178.2 NA 11.8 97 NA NA NA NA No 0 0 Early death (heart failure)
20 F 0 39 2.7 - - + NA - ASD, VSD - 73.6 5 23.2 388 78 91 6.7 NA No 10+ 10+ CCR
21 F 1 37 2.2 - - - - + AVSD, CoA + 12.9 9 15.4 27 60 13 5.8 NA No 12+ 12+ CCR
22 M 0 37 3.4 - - - - + PDA - 117.2 72 10.3 711 52 76 2.6 1.3 No 12+ 12+ CCR
23 M 11 36 2.9 - - - - + AVSD, PDA - 13.0 25 20.7 72 17 4 20.2 1.5 No 13+ 13+ CCR
24 F 4 33 2.1 - - - - - No + 6.5 3 12.9 122 11 7 3.0 0.7 Yes 4 4 Early death (liver failure)
25 M 1 35 2.1 - - - - + No - 81.1 60 15.3 959 170 311 14.9 1.9 Yes 34+ 34+ NA
26 M 60 31 1.9 - - - - - VSD - 120.2 63 7.4 1,222 33 46 0.6 0.1 Yes 2+ 2+ NA
27 F 0 36 NA + - + + - No - 32.4 18 NA NA 34 30 0.8 0.1 NA 4+ 4+ CCR
28 M 0 30 1.8 + + + + + PDA, VSD + 69.4 23 11.3 190 69 41 6.3 1.0 Yes 1 1 Early death (liver failure)
29 F 0 36 3.1 + - + + - ASD - 133.8 91 8.3 242 63 32 1.5 0.6 Yes 0+ 0+ NA
30 F 0 36 2.8 - + + + + PDS, VSD NA 54.5 55 12.4 422 75 209 2.9 1.1 No 0 0 Early death (multiple organ failure)
31 M 5 36 2.2 - - - - - ASD - 65.8 82 14.9 37 41 12 8.3 0.5 No 1+ 1+ CCR
32 M 14 39 3.2 - - NA NA - No - 13.2 6 16.0 610 32 21 10.8 NA No 0+ 0+ NA
33 M 0 39 3.2 - - + + - ASD, PDA, VSD + 71.6 60 17.8 826 48 23 0.8 0.3 Yes 3+ 3+ NA
34 M 0 36 2.1 + + + - + No + 19.9 84 12.2 73 51 73 9.4 4.0 Yes 16+ 16+ CCR
35 F 0 33 2.0 + + + + - VSD - 325.7 90 10.3 246 110 232 3.4 NA Yes 12 14+ Progression to ML-DS
36 M 0 35 2.1 + + + + + AVSD, PDA - 71.7 53 12.0 264 83 35 2.9 1.4 No 1 1 Early death (multiple organ failure)
37 M 0 36 1.9 + - + + - AVSD - 25.7 35 16.0 100 52 18 2.4 1.0 No 13 13 CCR (hematemesis of unknown origin)
38 M 0 38 3.3 - - - - - PDA + 74.1 36 14.7 162 45 34 4.6 1.8 No 34 40 Progression to ML-DS (ML-DS-related death)
39 M 1 36 2.3 + + + + - ASD - 156.5 81 10.6 177 811 200 6.5 1.5 Yes 7+ 7+ CCR
40 M 0 37 2.5 - - + NA - ASD, PDA, VSD NA 222.4 92 9.3 584 141 110 2.8 0.8 Yes 0+ 0+ NA
41 F 0 38 2.7 - - NA NA + No - 37.9 47 15.8 159 52 72 4.7 0.7 No 2+ 2+ CCR
42 F 0 33 1.9 + - + - - No + 35.8 47 6.9 384 28 14 2.1 1.0 No 0 0 Early death (lung bleeding)
43 F 9 36 2.7 + + + + + VSD - 356.7 88 14.3 295 47 7 17.5 1.0 Yes 2+ 2+ NA
44 F 1 40 3.3 - - NA NA + AVSD + 84.0 24 23.9 572 410 120 7.9 0.5 No 0+ 0+ NA
45 M 23 37 2.4 - - - - - TOF + 24.0 4 25.4 54 112 23 7.1 0.1 No 0+ 0+ CCR
46 F 0 35 1.9 - - - - - VSD - 56.2 67 16.4 623 61 34 2.3 0.6 No 2+ 2+ CCR
47 M 2 37 2.9 - - - - - No - 61.8 63 16.8 153 40 10 3.1 0.5 No 0+ 0+ NA
48 M 15 33 1.6 - - NA NA - No - 29.2 1 16.4 242 50 30 9.9 0.7 No 1+ 1+ CCR
49 M NA 26 0.7 + + - - + AVSD - 8.6 0 10.4 50 115 38 10.1 7.8 No 3+ 3+ NA
50 F 0 36 2.9 + - - - - No - 84.1 43 16.4 669 52 93 2.4 0.7 No 13+ 13+ CCR
51 F 4 39 2.5 + - - - + ASD, VSD - 41.2 40 19.5 426 51 31 11.5 0.6 Yes 8+ 8+ NA
52 F 0 30 1.5 NA + NA NA + ASD, PDA, VSD - 53.9 12 14.2 263 107 45 3.8 NA No 17+ 17+ CCR
53 M 0 32 1.6 + + + + + No - 155.4 88 9.5 133 34 60 2.8 1.0 Yes 9+ 9+ CCR
54 M 1 36 3.1 - - - - + VSD - 6.5 5 8.7 75 72 75 5.9 3.1 No 1+ 1+ NA
55 F 1 38 3.0 - - - - - PDA - 12.6 NA 18.9 115 45 10 13.8 0.6 No 1+ 1+ CCR
56 M 0 31 1.7 + + - - + PDA - 141.4 76 13.6 127 100 68 5.7 1.0 Yes 6+ 6+ NA
57 F 0 35 2.4 + + + + + PDA, VSD - 186.4 60 8.6 1,041 243 83 3.5 0.8 No 0+ 0+ NA
58 M 8 37 2.9 - - + + NA VSD - 17.1 15 16.6 63 26 12 14.4 0.1 No 0+ 0+ CCR
59 M 5 37 2.7 - - - - + ASD - 24.0 33 18.2 126 21 8 16.6 1.0 No 8+ 8+ CCR
60 M 1 37 2.7 - - + + + PDA - 108.0 63 16.2 817 210 182 8.7 1.1 NA 0+ 0+ NA
61 F 3 38 2.7 - - + + - ASD, VSD - 28.0 3 17.4 111 20 14 13.1 0.7 No 2+ 2+ CCR
62 F 0 35 2.3 + - - - - PDA - 251.4 78 12.0 288 55 81 3.3 NA Yes 0+ 0+ NA
63 F 0 39 3.0 + - + - - ASD, VSD - 177.5 77 15.1 424 69 37 2.2 1.0 Yes 10+ 10+ CCR
64 M 0 37 2.8 - - - + + No - 16.1 0 15.2 635 19 10 2.4 NA No 0+ 0+ NA
aEffusions include asites, pleural effusion, pericardial effusion, anasarca and fetal hydrops.
Abbreviations: GA, gestational age; WBC, white blood cell count; Hb, hemoglobin; Plt, platelet count; AST, aspartate aminotransaminase; ALT,alanine aminotransferase; T-bil, total bilirubin; D-bil, direct-bilirubin; EFS, event-free survival; OS, overall survival; M, male; F, female; NA, not available; ASD, atrial septal defect; AVSD, atrioventricular septal defect; CoA, coarctation of the aorta; PDA arteriosus; PS, pulmonary stenosis; TOF, tetralogy of Fallot; VSD, ventricular septal defect; CCR, continuous complete remission; ML-DS, myeloid leukemia of Down syndrome; RSV, respiratory syncytial virus.
Figure Legends
FIGURE 1. Outcome of patients with TAM and non-constitutional trisomy 21 compared with those with TAM and constitutional trisomy 21/DS. (A) Overall survival. (B) Event- free survival. (C) Cumulative incidence of progression to ML-DS.