髄床底穿孔を生じた近心中央根管を有する下顎第一大臼歯に感染根管治療を行った一症例
6
0
0
全文
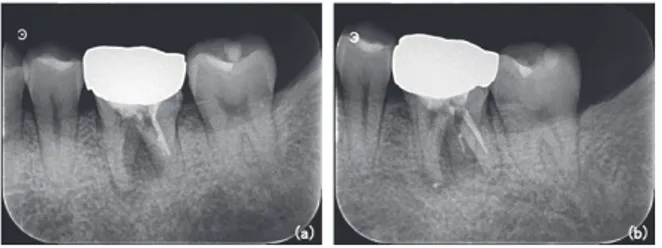
(2) 118 日歯内療誌 42(2):117~122,2021 付近での穿孔もしくは歯根縦破折の疑いと診断し,追 加情報を採取するために CBCT の撮影を行った. CBCT 画像上で根分岐部の穿孔と穿孔部に連続する骨 吸収像が確認されたため(図 2) ,保存の可否の診断的 治療もかねて感染根管治療を行うこととした.事前に ヘルシンキ宣言に基づき,口頭と書面で研究目的と内 容を説明して,研究に対する十分な理解を得たうえで 参加の同意を得た(東京歯科大学水道橋病院倫理委員 会 承認番号:SH‒41).. 経 過 浸潤麻酔を行い,補綴物とう蝕を除去した.コンポ. Fig. ₁ Pre‒treatment X‒ray of the mandibular left first molar (a)orthoradial,(b)eccentric projections 図 ₁ 術前下顎第一大臼歯デンタル X 線画像 (a)正放線,(b)偏近心. ジットレジンにて隔壁を作製してラバーダム防湿を 行った.歯面の清掃はポビドンヨードと過酸化水素水 で行い,根管治療は手術用顕微鏡を用いて開始した. メチレンブルーで歯質を染色して観察したところ,明 らかな歯根破折は認めないが,髄床底の遠心舌側根管 内湾側に,歯周ポケットと交通する直径 3 mm 程度の 穿孔を認めた(図 3‒a).また,根管探索時に,近心根 の頰側根管と舌側根管を結ぶ根管イスムスと,その部 位に MM 根管を確認した.保存可能と診断し治療を継 続することとした.すべての根管のネゴシエーション を行ったのち,電気的根管長測定を行った.測定した 根管長でファイル試適のデンタルエックス線写真を撮 影して,根管長に間違いがないか確認した(図 3‒b). 作業長を根管長から 0.5 mm 手前に設定し,根管拡大 は Ni‒Ti ロータリーファイルで MB 根管,ML 根管と MM 根管を#40/.04 まで拡大した.また遠心根管を #60/.04 まで拡大した.根管洗浄は 2.5%NaOCl と 17%EDTA を用いて,シリンジを用いた陰圧洗浄を行 い,超音波器具を併用して PUI を行った.穿孔部への 更なる感染を予防するために,最初に穿孔部の封鎖を 行うこととした.穿孔部から肉芽の侵入を認めたた め,肉芽をヒートプラガーにて焼結して除去し,0.5% NaOCl と 17%EDTA にて穿孔部を洗浄し,エピネフ リ ン 含 有 綿 球 に て 圧 迫 止 血 を 行 っ た. 他 の 根 管 に MTA セメントが入りこまないように,水酸化カルシ ウム製剤を貼薬した後に穿孔部を MTA セメントにて. Fig. ₂ Pre‒treatment X‒ray of the mandibular left first molar. CBCT coronal sectional image (a)coronal section,(b)sagittal section of M root,(c)sagittal section at the root furcation,(d)sagittal section of D root,(e)axial section of the root canal orifice, (f)axial section of the perforation,(g)axial section of the apical third 図 ₂ 術前下顎第一大臼歯 CBCT 画像 (a)冠状断,(b)M 根の矢状断, (c)歯根分岐部での矢状断, (d)D 根の矢状断, (e)根管口部での横断,(f)穿孔部での横断, (g)根尖側 ₃ mm での横断.
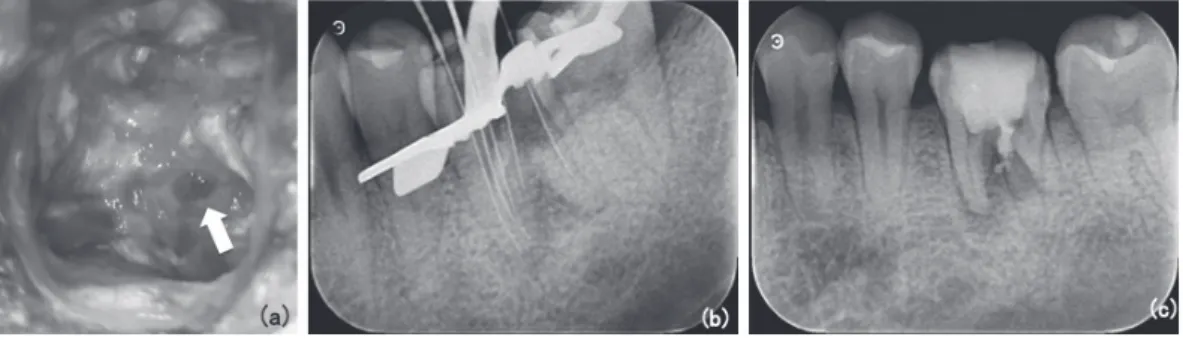
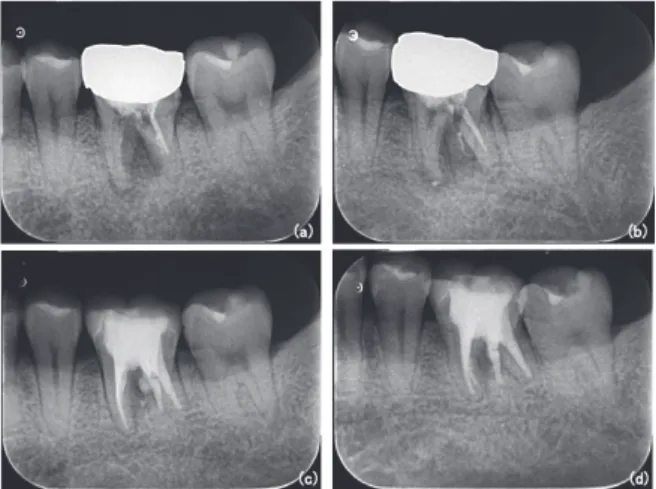
(3) 髄床底穿孔修復と MM 根管の感染根管治療 119. Fig. ₃ Intra‒operative images (a)microscopic images taken during perforation examination,(b)dental X‒ray image with a trial file at the root canal length,(c)dental X‒ray image after perforation repair 図 ₃ 術中の画像 (a)穿孔部確認時のマイクロスコープ像, (b)根管長でファイル試適時のデンタル X 線画像, (c)穿 孔修復直後の X 線画像. Fig. ₄ Images at the second visit (a)microscopic images taken during confirmation of sealing of the perforation repair part,(b) dental X‒ray with trial master point 図 ₄ ₂ 回目の受診時の画像 (a)穿孔修復部の硬化確認時のマイクロスコープ像, (b)GP のコーンフィット時. 封鎖し(図 3‒c) ,水硬性仮封材とグラスアイオノマー セメントにて二重仮封を行った.2 回目の来院時で垂 直打診痛は軽減していた.ラバーダム防湿を行い,歯 面清掃後に仮封を除去した.手術用顕微鏡下で MTA セメントの硬化と,穿孔部の封鎖が得られていること を確認できたため根管治療を開始した (図 4‒a).2.5% NaOCl と 17%EDTA を用いて根管の最終洗浄を行っ た.根管乾燥してガッタパーチャを根管内で試適し, デンタルエックス線画像を撮影して作業長が維持され ていることを確認した(図 4‒b) .CWCT 法にて根管 充塡を行った後に(図 5‒a,b) ,直接法で築造を行い, テンポラリークラウンを装着して,充塡状態の確認の ためデンタルエックス線画像を撮影した (図 5‒c,d) . 根管充塡後のデンタルエックス線画像で MB 根管と MM 根管は根尖部付近で合流していることが観察さ れた.. Fig. ₅ Images at root canals filling (a)microscopic images taken while the MM root canals filling,(b)microscopic images taken after the root canals filling. Dental X‒rays after root canal filling,(c)orthoradial and(d)eccentric projections 図 ₅ 根管充塡の画像 (a)MM 根管の根管充塡時のマイクロスコープ画像, (b)根管充塡直後のマイクロスコープ画像, (c)根管 充塡直後の正放線デンタル X 線画像,(d)偏近心デ ンタル X 線画像. 結 果 根管充塡後 3 カ月の経過観察時で臨床症状は消失 し,頰側の限局性の歯周ポケットは 3 mm 程度に改善 を認めた.デンタルエックス線画像で近心根と根分岐 部の透過像は縮小傾向を認め,機能的に問題を認めな.
(4) 120 日歯内療誌 42(2):117~122,2021 いため(図 6) ,治癒中と診断し歯冠修復を行った.1 年後の経過観察で臨床症状や著変はなく,機能的であ り,デンタルエックス線画像(図 7)と CBCT 画像(図 8)で,根尖部と根分岐部の透過像領域の縮小を認めた ため,良好な治癒が得られたと診断した.. 有する場合は 42%に低下することも報告されてい る4).一方,現在の手法や材料を用いた場合,89%と 従来より高い成功率が報告されている5).その理由と. 考 察 穿孔は根管治療の結果として 9.6%で生じるといわ れており3),従来からの手法や材料で行った場合の成 功率は 56%と報告されている1).さらに,根尖病変を. Fig. ₆ Post‒treatment X‒rays taken three months after root canal filling of the mandibular left first premolar Dental X‒rays in(a)orthoradial and(b)eccentric projections 図 ₆ 根管充塡後 ₃ カ月のデンタル X 線画像 (a)正放線,(b)偏近心. Fig. ₇ Comparison of X‒rays of the mandibular left first premolar before and after treatment Pre‒treatment dental X‒rays in(a)orthoradial and (b)eccentric projections. Post‒treatment dental X‒ rays taken one years after root canal filling in(c) orthoradial and(d)eccentric projections 図 ₇ 術前と術後のデンタル X 線画像写真の比較 (a)術前正放線, (b)術前偏近心, (c)根管充塡後 ₁ 年正 放線, (d)根管充塡後 ₁ 年偏近心. Fig. ₈ Post‒treatment X‒ray of the mandibular left first molar CBCT coronal sectional image (a)coronal section,(b)sagittal section of M root,(c)sagittal section at the root furcation,(d)sagittal section of D root,(e)axial section of the root canal orifice, (f)axial section of the perforation repaired area,(g)axial section of the apical third 図 ₈ 術後下顎第一大臼歯 CBCT 画像 (a) 冠 状 断,(b)M 根 の 矢 状 断, (c) 歯 根 分 岐 部 で の 矢 状 断,(d)D 根 の 矢 状 断, (e)根管口部での横断,(f)穿孔部修復部での横断, (g)根尖側 ₃ mm での横断.
(5) 髄床底穿孔修復と MM 根管の感染根管治療 121. しては,拡大視野にて穿孔部の術前処置と封鎖を確実 に行えることと,MTA セメントの高い生体親和性と 封鎖性に由来すると考えられる6).細菌感染を伴わな い穿孔部では,MTA セメントで修復した多くの場合 で,組織反応として炎症の抑制と新生セメント質の形 成を認め,感染を伴っている場合よりも治癒が良好で あったと報告されている7,8).しかし感染を有する場合 には,水酸化カルシウムを貼薬して細菌減少を期待し た後に MTA セメントで修復した場合でも,早期に MTA セメントで修復した場合も差異はないと報告さ れている.さらに穿孔窩洞内にデブリスや肉芽組織が 存在すると根尖周囲組織と MTA セメントの接触が妨 げられて,十分な治癒が得られない可能性も示唆され ており9),これらは良好な治癒の妨げの一因と考えら れる. また,MM 根管は,約 10~20%の発現率が報告され ており,比較的多く存在しその形態も分類されてい る2).本症例は,MB 根管と MM 根管が根尖付近で合 流している,分類における「confluent」であった.し かし,MM 根管のその位置的な問題や,今回のように 画像診断や CBCT で描出されないことも多い.CBCT での探索より,手術用顕微鏡下で探索したほうの検出 率が高いとも報告されており10),事前の検出は難し い.また,狭窄しているためにその拡大清掃も困難で あるが11),未治療のままで残ることは好ましくない. 感染した根管を見逃した場合に,通常の 4.38 倍や 6.25 倍の確率で根管治療後に根尖性歯周炎を伴うこ とが報告されていることからも,治療失敗の大きな要 因であると考えられる12,13). 本症例では,手術用顕微鏡を用いて拡大視野下で確 実 に, 窩 洞 内 の 異 物 と 肉 芽 組 織 を 十 分 に 除 去 し, MTA セメントにて比較的早期に穿孔修復を行えた. また手術用顕微鏡を用いることで MM 根管を検出で き,M 根の汚染された解剖学的構造物の細菌数を機械 的除去にて減少させて根管治療を行えた.以上より穿 孔部感染による骨欠損と,根尖性歯周炎由来の骨欠損 の良好な治癒が得られたと考えられた14).. 結 論 本症例では手術用顕微鏡を用いた拡大視野下で確実 な穿孔封鎖を行い,MM 根管と主根管を探索してデブ ライドメントすることで十分な感染源の除去が行えた ため,良好な治癒が得られた.以上より手術用顕微鏡 下での穿孔修復と MM 根管の治療は有用である. 本論文に関して開示すべき利益相反はない.. 文 献 1)Kvinnsland I, Oswald RJ, Halse A et al.:A clinical and roentgenological study of 55 cases of root perforation, Int Endod J, 22:75‒84, 1989. 2)Pomeranz HH, Eidelman DL, Goldberg MG: Treatment considerations of the middle mesial canal of mandibular first and second molars, J Endod, 7:565‒568, 1981. 3)Ingle JI:A standardized endodontic technique utilizing newly designed instruments and filling materials, Oral Surg Oral Med Oral Pathol, 14: 83‒91, 1961. 4)Farzaneh M, Abitbol S, Friedman S:Treatment outcome in endodontics:The Toronto study‒ phases Ⅰ and Ⅱ:Orthograde retreatment, J Endod, 30:627‒633, 2004. 5)Mente J, Hage N, Pfefferle T et al.:Treatment outcome of mineral trioxide aggregate:Repair of root perforations, J Endod, 36:208‒213, 2010. 6)Pace R, Giuliani V, Pagavino G:Mineral trioxide aggregate as repair material for furcal perforation:Case series, J Endod, 34:1130‒1133, 2008. 7)末原正崇,森永一喜,中川寛一:Mineral Trioxide Aggregate および強化型亜鉛華ユージノールセメ ントが髄床底穿孔部周囲の組織に及ぼす影響,日 歯保存誌,44:755‒775,2001. 8)Holland R, Filho JA, de Souza V et al.:Mineral trioxide aggregate repair of lateral root perforations, J Endod, 27:281‒284, 2001. 9)Holland R, Bisco Ferreira L, de Souza V et al.: Reaction of the lateral periodontium of dogs’ teeth to contaminated and noncontaminated perforations filled with mineral trioxide aggregate, J Endod, 33:1192‒1197, 2007. 10)Honap MN, Devadiga D, Hegde MN:To assess the occurrence of middle mesial canal using cone‒beam computed tomography and dental operating microscope:An in vitro study, J Conserv Dent, 23:51‒56. 2020. 11)Cunningham CJ, Senia ES:A three‒dimensional study of canal curvatures in the mesial roots of mandibular molars, J Endod, 18:294‒300, 1992. 12)Karabucak B, Bunes A, Chehoud C et al.:Prevalence of apical periodontitis in endodontically treated premolars and molars with untreated canal:A cone‒beam computed tomography study, J Endod, 42:538‒541, 2016..
(6) 122 日歯内療誌 42(2):117~122,2021 13)Costa FFNP, Pacheco‒Yanes J, Siqueira JF Jr et al.:Association between missed canals and apical periodontitis, Int Endod, 52:400‒406, 2019. 14)José F Siqueira Jr, Isabela N Rôças:Clinical implications and microbiology of bacterial persistence after treatment procedures, J Endod, 34: 1291‒1301, 2008.. 著者連絡先:山田雅司. 東京歯科大学歯内療法学講座 . 〒 101‒0061 東京都千代田区三崎町 2‒9‒18 TEL:03‒6380‒9136 E‒mail:[email protected].
(7)
図
関連したドキュメント
Laplacian on circle packing fractals invariant with respect to certain Kleinian groups (i.e., discrete groups of M¨ obius transformations on the Riemann sphere C b = C ∪ {∞}),
Eskandani, “Stability of a mixed additive and cubic functional equation in quasi- Banach spaces,” Journal of Mathematical Analysis and Applications, vol.. Eshaghi Gordji, “Stability
Finally, we give an example to show how the generalized zeta function can be applied to graphs to distinguish non-isomorphic graphs with the same Ihara-Selberg zeta
We show that a discrete fixed point theorem of Eilenberg is equivalent to the restriction of the contraction principle to the class of non-Archimedean bounded metric spaces.. We
「A 生活を支えるための感染対策」とその下の「チェックテスト」が一つのセットになってい ます。まず、「
It turns out that the symbol which is defined in a probabilistic way coincides with the analytic (in the sense of pseudo-differential operators) symbol for the class of Feller
We give a Dehn–Nielsen type theorem for the homology cobordism group of homol- ogy cylinders by considering its action on the acyclic closure, which was defined by Levine in [12]
In this work, our main purpose is to establish, via minimax methods, new versions of Rolle's Theorem, providing further sufficient conditions to ensure global
