Low
-dose radioiodine ablation of remnant thyroid in high
-risk differentiated thyroid carcinoma
Kunihito SUZUKI, Mana YOSHIMURA and Koichi TOKUUYE
Department of Radiology, Tokyo Medical University
Abstract
Recently, the potential of remnant thyroid ablation using 1,110 MBq 131I has been established, albeit under certain limitations, and guidelines have been issued on its use as an outpatient procedure in Japan. The aims of this study were to calculate the success rate of remnant thyroid ablation with 1,110 MBq as an outpatient proce- dure in high-risk differentiated thyroid carcinoma (DTC) patients and explore the relationship between successful outcome and patient-/disease-related factors. Fifty high-risk patients with DTC underwent remnant thyroid abla- tion with 1,110 MBq 131I on an outpatient basis between January 2009 and March 2011 at Tokyo Medical Univer- sity Hospital. The ablation success rate was evaluated using a whole body scan (WBS) performed at 4-33 months (mean, 7 months) post-
successful outcome was obtained in 41 patients, with a success rate of 82.0%, which was in agreement with that any patient-/disease-related factor. We believe that remnant ablation with 1,110 MBq 131I in high-risk DTC ablation with low-dose (1,110 MBq) 131I in high-risk DTC patients.
Received October 15, 2013, Accepted January 6, 2014
Key words: radioiodine therapy, thyroid ablation, differentiated thyroid carcinoma, thyroid carcinoma
Corresponding author: Kunihito Suzuki, Department of Radiology, Tokyo Medical University, 6-7-1 Nishi-Shinjuku, Shinjuku-ku, Tokyo 160-0023, Japan
TEL : +81-(0)3-3342-6111 ext.5818 FAX : +81-(0)3-3348-6314 E-mail : [email protected] Educator name : Mana YOSHIMURA
Introduction
Patients with high
-risk differentiated thyroid carci- noma (DTC) are typically treated with total thyroidec- tomy (TT) followed by
131I ablation of the post
-surgical thyroid remnant in accordance with the Japanese clinical guidelines
1). Ablation of remnant thyroid tissue is also recommended by international consensus in high
-risk patients
2)3). The purpose of this procedure is to remove completely any remaining thyroid tissue following TT.
This has been reported to improve disease
-free survival and local control rate in high
-risk patients
4). The level of iodine in the Japanese diet differs from that found in Europe or the United States, resulting in a higher rate of occurrence of papillary carcinoma. Therefore, surgery involves neck lymph node dissection due to the greater
number of lymph node metastases. However, fewer
distant metastases occur with this disease than usually
found with follicular carcinoma. Some studies have
noted that there is a lack of hospital wards and beds
available for non
-sealed radioiodine therapy
5)6). Based
on these two points, remnant thyroid ablation has often
been avoided in some DTC patients in Japan for a long
time. Recently, guidelines have been established on
remnant thyroid ablation as an outpatient procedure, with
ablation using 1,110 MBq
131I becoming possible, albeit
under certain limitations
7)8). The aims of this study were
to calculate the success rate of remnant thyroid ablation
with 1,110 MBq as an outpatient procedure in high
-risk
DTC patients and explore the relationship between suc-
cessful outcome and patient
-/disease
-related factors (age,
sex, pT stage, presence of lymph node metastasis, dura-
J. Tokyo Med. Univ., 72 2 : 141-147, 2014tion from TT to ablation). To our knowledge, this is the
Materials and Methods 1. Patients
Fifty high
-risk patients with DTC underwent remnant thyroid ablation with 1,110 MBq
131I on an outpatient basis between January 2009 and March 2011 at Tokyo Medical University Hospital. Patient characteristics are shown in Table 1. All patients underwent TT as radical surgery and comprised 36 female and 14 male, with a mean age at ablation of 53.9 years. The diagnosis was - cation of pT2 in 1 patient, pT3 in 33, and pT4 in 16.
Among 40 cases of lymph node metastasis, 38 were pN1b and 2 were pN1a. The mean duration from TT to ablation was 245.5 days (range 53
-1327 days). High risk was defined according to the following criteria : tumor size larger than 5 cm ; lymph node metastasis larger than 3 cm ; lymph node metastasis extending to the internal jugular vein, carotid artery, or major nerves such as the recurrent laryngeal nerve or pre
-vertebral fascia ; multiple and intensely swollen lymph node metastases ; or extra
-thyroid extension to the trachea or esophageal mucosa
1). Exclusion criteria were the pres- ence of distant metastases (e.g., lung or bone) or a treat- ment history of
131I thyroid ablation.
2. Radioiodine ablation of remnant thyroid All patients underwent remnant thyroid ablation with 1,110 MBq
131I. Administration of levothyroxine was withdrawn for 4 weeks and replaced with triiodothyro- preparation for the procedure. The patients were instructed to follow a low
-iodine diet for 2 weeks prior to surgery until the 4
-5th day after ablation. No recom- binant human TSH (rhTSH) was used for the ablation.
The TSH and serum Tg values were measured in all patients at ablation. Four days after oral administration
-
camera equipped with high
-resolution parallel
-hole collimator (E.CAM, Siemens, Erlangen, Germany). Whole body planar images and spot views of the neck were acquired in ante- rior and posterior projections on a photo peak of 365 keV with a 15% window.
3. Evaluation
Post
-ablation WBS was performed at 4
-33 (mean, 7 months) months after the ablation. WBS and serum Tg value measurement were performed either thyroid hor- mone withdrawal (THW) or rhTSH
-aided
9). WBS by THW was obtained on the fourth day with 481
-1,110 MBq of
131I with measurement of Tg value on the first day. On the other hand, by rhTSH
-aided protocol, rhTSH was given at a dose of 0.9 mg intramuscularly on
day 1, and day 2. On the day 3, 185
-1,110 MBq of
131I was administered. On day 5 or 6, WBS was performed of ablation was negative of WBS.
4. Statistical analysis (multiple logistec-regression analysis)
For statistical analysis, we used SPSS version 17.0 for Windows (SPSS Inc, Chicago, Illinois, USA). The quantitative data (continuous parameters) were analyzed using the forward selection method of likelihood ratio test. We selected as variable factors of age, gender, pT stage, presence of lymph node metastasis, duration from difference was considered when
p value of <0.05 wasconsidered to indicate a statistically significant differ- ence.
Results
The success rate of remnant thyroid ablation was 82%
in 41 of 50 patients (Fig. 1). The procedure was deemed to have failed in the remaining 9 patients based on their post
-ablation WBS results (Fig. 2). The presence of thyroid tissue in the thyroid bed was indicated in these patients and additional ablation therapy administered.
There were no cases of local recurrence or cancer death during the study period. On the other hand, a high Tg value (ranging from 20 to 210 ng/ml) was observed in 7 patients during the post
-ablation follow
-up and cervical lymph node and/or pulmonary metastases confirmed, indicating the need for additional treatment.
In the multiple logistic
--
cant correlation was observed between the success of remnant thyroid ablation and age, sex, pT stage, lymph node metastases, or duration from TT to ablation (Table 2). The goodness
-of
-fit in this model was verified by the Hosmer
-Lemeshow test (p=0.671).
Discussion
Differentiated thyroid carcinoma is the most common endocrine malignancy. The 10
-year survival rate is reported to be 93% in papillary carcinoma and 85% in follicular carcinoma according to a large cohort study in the USA
10). The diagnosis in patients with DTC is also good. For high
-risk DTC, TT is recommended under the Japanese guidelines
1). A multivariate analysis of over 50,000 patients with papillary thyroid carcinoma revealed that TT significantly improved recurrence and survival rates for tumors >1.0 cm
11). Remnant thyroid ablation increases the rates of local control and cause
-specific survival rates, especially in high
-risk patients undergoing TT
4).
Thyroid tissue remains in approximately 90% of
patients undergoing TT, but is often impossible to detect
by various imaging modalities such as ultrasonography
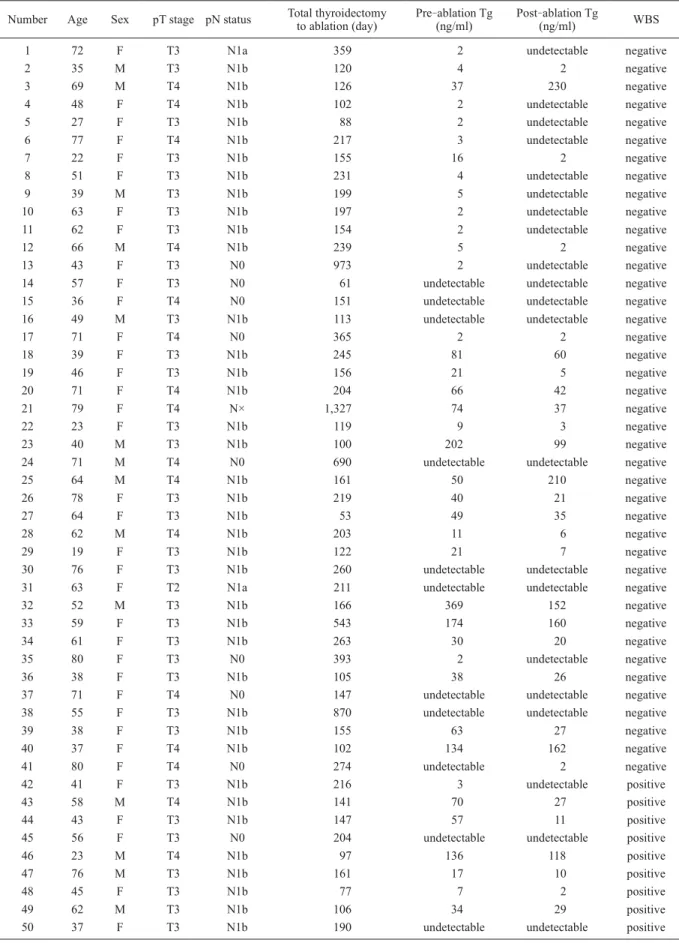
Table 1 Patient characteristics and clinical data Number Age Sex pT stage pN status Total thyroidectomy
to ablation (day) Pre-ablation Tg
(ng/ml) Post-ablation Tg
(ng/ml) WBS
1 72 F T3 N1a 359 2 undetectable negative
2 35 M T3 N1b 120 4 2 negative
3 69 M T4 N1b 126 37 230 negative
4 48 F T4 N1b 102 2 undetectable negative
5 27 F T3 N1b 88 2 undetectable negative
6 77 F T4 N1b 217 3 undetectable negative
7 22 F T3 N1b 155 16 2 negative
8 51 F T3 N1b 231 4 undetectable negative
9 39 M T3 N1b 199 5 undetectable negative
10 63 F T3 N1b 197 2 undetectable negative
11 62 F T3 N1b 154 2 undetectable negative
12 66 M T4 N1b 239 5 2 negative
13 43 F T3 N0 973 2 undetectable negative
14 57 F T3 N0 61 undetectable undetectable negative
15 36 F T4 N0 151 undetectable undetectable negative
16 49 M T3 N1b 113 undetectable undetectable negative
17 71 F T4 N0 365 2 2 negative
18 39 F T3 N1b 245 81 60 negative
19 46 F T3 N1b 156 21 5 negative
20 71 F T4 N1b 204 66 42 negative
21 79 F T4 N× 1,327 74 37 negative
22 23 F T3 N1b 119 9 3 negative
23 40 M T3 N1b 100 202 99 negative
24 71 M T4 N0 690 undetectable undetectable negative
25 64 M T4 N1b 161 50 210 negative
26 78 F T3 N1b 219 40 21 negative
27 64 F T3 N1b 53 49 35 negative
28 62 M T4 N1b 203 11 6 negative
29 19 F T3 N1b 122 21 7 negative
30 76 F T3 N1b 260 undetectable undetectable negative
31 63 F T2 N1a 211 undetectable undetectable negative
32 52 M T3 N1b 166 369 152 negative
33 59 F T3 N1b 543 174 160 negative
34 61 F T3 N1b 263 30 20 negative
35 80 F T3 N0 393 2 undetectable negative
36 38 F T3 N1b 105 38 26 negative
37 71 F T4 N0 147 undetectable undetectable negative
38 55 F T3 N1b 870 undetectable undetectable negative
39 38 F T3 N1b 155 63 27 negative
40 37 F T4 N1b 102 134 162 negative
41 80 F T4 N0 274 undetectable 2 negative
42 41 F T3 N1b 216 3 undetectable positive
43 58 M T4 N1b 141 70 27 positive
44 43 F T3 N1b 147 57 11 positive
45 56 F T3 N0 204 undetectable undetectable positive
46 23 M T4 N1b 97 136 118 positive
47 76 M T3 N1b 161 17 10 positive
48 45 F T3 N1b 77 7 2 positive
49 62 M T3 N1b 106 34 29 positive
50 37 F T3 N1b 190 undetectable undetectable positive
*Tg undetectable mean <1 ng/ml
and CT scans. Ablation with
131I offers an effective method of destroying remnant thyroid tissue, reducing the possibility of local recurrence. Moreover, this method is more suitable than other procedures as it is convenient for use during post
-surgical follow
-up. The
serum Tg value is a good marker of recurrence and dis- tant metastases during post
-surgical follow
-up in DTC patients as it does not require anti
-thyroglobulin anti- body. However, the serum Tg value cannot be deter- mined if thyroid tissue remains. As ablation erases Tg
Table 2 Patient characteristics and multiple logistic-regression analysis of predictive factors for successful ablationSucccess Failure P value
Sex 0.243
Male 10 4
Female 31 5
Age 0.364
Mean (range 55.0 (19.0-80.0) 49.0 (23.0-76.0)
p Tstage* 0.46
T3 26 7
T4 14 2
Presence of lymph node metastases** 0.444
N0 8 1
N1a-b 32 8
Total thyroidectomy to ablation (day) 0.18
Mean (SD) 258.5±266.8 148.8±46.1
Range 53.0-1,327.0 77.0-216.0
Quantitative data (continuous parameters) were analyzed using forward selection method of likelihood ratio test. No lymph node metastases, or duration from TT to ablation.
*Excluding one case of T2
**Excluding one case of Nx
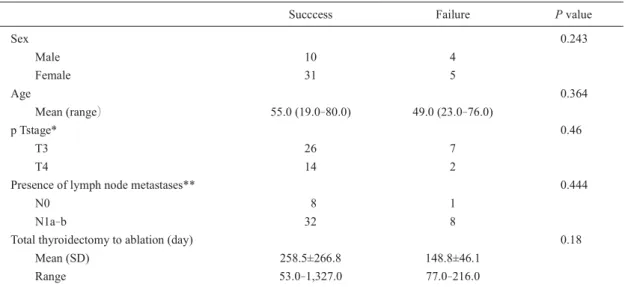
Fig. 1. Successful case (Case 8 in Table 1)
a : WBS on 5th day of ablation. Intense uptake of 131I in center of neck, indicating thyroid bed accumulation.
b : Post-ablation WBS using 1,110 MBq 131I performed at 20 months after ablation. There was no accumulation in thyroid bed. Tg value decreased from 4 to undetectable level after ablation. This case was considered to be successful.
a b
from remnant thyroid tissue, its serum values can serve as a good marker of post
-surgical recurrence or metasta- sis. Therefore, it is important for patients at high risk of post
-surgical recurrence or metastasis to undergo abla- tion
12-16).
Even allowing for differences in high
-risk patients or dosage of
131I, the success rate of ablation is approxi- mately 70%
-95%
17)18). Zidan et al. reported the ablation success rate as 94% in 238 patients receiving 1,110
-3,145 MBq. Bal et al. reported the success rate as 72.8% in 149 patients receiving 1,110
-5,735 MBq. In the present study, remnant thyroid ablation with 1,110 MBq in high
-risk patients yielded an equivalent therapeutic result to as a negative WBS result, as the purpose of remnant thy- roid ablation is to destroy the remnant thyroid bed.
After TT and ablation, the serum Tg value is normally
-
presence of remnant thyroid tissue and investigate metastatic or recurrent lesions. A high Tg value with negative neck accumulation is thought to suggest microscopic metasta- ses in extra
-thyroid lesions. During observation, cervi- cal lymph node and/or pulmonary metastases were found in 7 patients with high a Tg value by chest CT or neck ultrasonography. There is a real potential of local recur- rence or metastasis, so careful diagnostic imaging and observation are needed. If local recurrence or distant
metastases actually occur, then additional therapy is needed. There is no effective chemotherapy for local recurrent or distant metastases in DTC patients. It is difficult to control tangible local recurrences or lymph node metastases detected on imaging studies, so surgical treatment is the most appropriate response
19).
Recently, few studies have reported any difference in the ablation success rate between low
-dose (1,110 MBq) and high
-dose (3,700 MBq)
131I
20-22). In this study, we administered 1,110 MBq on the basis of the established guidelines for outpatient treatment. We believe that the present results obtained with a low dose are of particular interest.
We analyzed the relationship between patient
-/dis- ease
-related factors and ablation success. No signifi- cant correlation was observed between the success of remnant thyroid ablation and age, sex, pT stage, or pres- ence of lymph node metastasis. No correlation was observed between ablation success and the duration from TT to ablation. To our knowledge, no studies to date have established the appropriate duration from TT to remnant thyroid ablation. However, the risk of death in patients undergoing initial radioiodine therapy at more than 180 days after TT is reported to be 4.22 times higher than that in those treated within 180 days in metastatic DTC
23).
There was small number of failure cases in this study.
a b
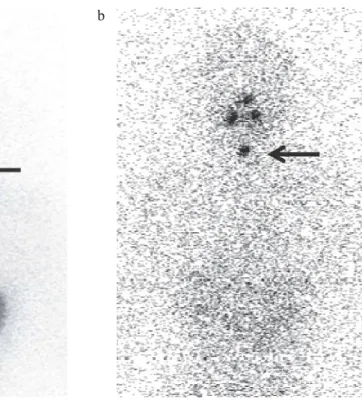
Fig. 2. Failure case (Case 48 in Table 1)
a : WBS on 5th of ablation. Intense uptake of 131I in center of neck, indicating thyroid bed accumulation.
b : Post-ablation WBS using 1,110 MBq 131I performed at 6 months after ablation.
Neck accumulation remained. Presence of thyroid tissue in thyroid bed was suggested.
Further study is needed to elucidate the relationship between the success of ablation and such factors in larger samples of patients.
Conclusion
The success rate of remnant thyroid ablation was 82%
in 41 of 50 patients, which is in agreement with rates reported in earlier studies. The present results suggest that the success of remnant thyroid ablation is indepen- dent of age, sex, pT stage, presence of lymph node metastases, or duration from TT to ablation.
Acknowledgements
We are indebted to Professor Jeremy Williams, Chair- man of the Department of International Medical Commu- nications at Tokyo Medical University, for his review of the English of the manuscript.
References
1) Takami T, Ito Y, Noguchi Y, Yoshida A, Okamoto T : Treatment of Thyroid Tumor/Japanese Clinical Guidelines
2) David S. Cooper, Gerard M. Doherty, Bryan R. Hau- gen, Richard T. Kloos, Stephanie L. Lee, Susan J.
Mandel, Ernest L. Mazzaferri, Bryan McIver, Furio Pacini, Martin Schlumberger, Steven I. Sherman, David L. Steward, R. Michael Tuttle : Revised Amer- ican Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer/The American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer. THYROID 19: 1167-1214, 2009
3) Pacini F, Schlumberger M, Dralle H, Rossella E, Johannes W, Wilmar W : European consensus for the management of patients with differentiated thyroid carcinoma of the follicular epithelium. Eur J Endo- crinol 154: 787-803, 2006
4) Jonklaas J, Sarlis N, Litofsky D, Ain K, Bigos S, Bri- erley J, Cooper D, Haugen B, Ladenson P, Magner J, Robbins J, Ross D, Skarulis M, Maxon H, Sherman S : Outcomes of patients with differentiated thyroid carcinoma following initial therapy. Thyroid 16: 1229-1242, 2006
5) Kusakabe K, Ito K, Shibuya H, Kinuya S, Ito M, Yokoyama K, Azuma T, Togawa T, Koizumi K, Yoshimura M, Uchiyama M, Okamoto T, Kanaya S, Kanaya K, Yoneyama T : The surveillance report on the actual operational status of medical ward environ- ment for radioactive iodine therapy of differentiated thyroid cancers in Japan (In Japanese with English abstract). Isotope News 672: 25-29, 2010
6) Koizumi K, Kusakabe K, Okamoto T, Kanaya S, Kanaya K, Ito K, Shibuya H, Uchiyama M, Kinuya S, Yoneyama T, Yokoyama K, Azuma T, Togawa T, Ito M, Yoshimura M, Uchida K : The second surveil-
lance report on the actual operational status of medi- cal ward environment for radioactive iodine therapy of differentiated thyroid cancers in Japan (the second survey in 2010) (In Japanese with English abstract).
Kaku Igaku 48: 15-17, 2011
7) Guidelines of outpatient treatment I-131(1,110 MBq) for the purpose of remnant thyroid ablation. (In Jap- anese with English abstract) : http://www.jsnm.org/
files/pdf/guideline/2012/i-131_jisshiyoukou_2012.
02.14.pdf
8) Higashi T, Kudo T, Kinuya S : Radioactive iodine (131I) therapy for differentiated thyroid cancer in Japan : current issues with historical review and future perspective. Ann Nucl Med 26: 99-112, 2012
9) Khan M, Nawaz M, Shah M, Syed A, Khan A : Judicious use of recombinant TSH in the management of differentiated thyroid carcinoma. Ann Nucl Med 24: 609-615, 2010
10) Hundahl S, Fleming I, Fremgen A, Menck H : A National Cancer Data Base report on 53,856 cases of thyroid carcinoma treated in the U.S. Cancer 83: 2638-2648, 1998
11) Bilimoria K, Bentrem D, Ko C, Stewart A, Win- chester D, Talamonti M : Sturgeon C Extent of sur- gery affects survival for papillary thyroid cancer.
Ann Surg 246: 375-381, 2007
12) Mazzaferri E, Jhiang S : Long-term impact of initial surgical and medical therapy on papillary and follicu- lar thyroid cancer. Am J Med 97: 418-428, 1994 13) Sawka A, Thephamongkhol K, Brouwers M, Thabane
L, Browman G, Gerstein H : a systematic review and metaanalysis of the effectiveness of radioactive iodine remnant ablation for well-differentiated thyroid can- cer. J Clin Endocrinol Metab 89: 3668-3676, 2004 14) Sawka A, Brierley J, Tsang R, Thabane L, Rotstein L,
Gafni A, Straus S, Goldstein D : An updated system- atic review and commentary examining the effective- ness of radioactive iodine remnant ablation in well- differentiated thyroid cancer : Endocrinol Metab Clin North Am 37: 457-480, 2008
15) Mazzaferri E : An overview of the management of papillary and follicular thyroid carcinoma. Thyroid 9: 421-427, 1999
16) Mazzaferri E, Kloos R : current approaches to pri- mary therapy for papillary and follicular thyroid can- cer. J clin Endocrinol Metab 86: 1447-1463, 2001 17) Bal C, Kumar A, Pant G : Radioiodine dose for rem-
nant ablation in differentiated thyroid carcinoma : a randomized clinical trial in 509 patients. J Clin Endocrinol Metab 89: 1666-1673, 2004
18) Zidan J, Hefer E, Iosilevski G, Drumea K, Stein ME, using different doses as determined by postoperative thyroid scan uptake in patients with differentiated thyroid cancer. Int J Radiat Oncol Biol Phys 59: 1330-1336, 2004
19) Schlumberger M : Papillary and follicular thyroid carcinoma. N Engl J Med 338: 297-306, 1998 20) Bal C, Pa dhy AK, Jana S , Gauri P, Basu A :
Prospective randomized clinical trial to evaluate the optimal dose of 131I for remnant ablation in patients with differentiated thyroid carcinoma. Cancer 77: 2574-2580, 1996
21) Creutzig H : High or low dose radioiodine ablation of thyroid remnants? Eur J Nucl Med 12: 500-502, 1987
22) Johansen K, Woodhouse N, Odugbesan O : Com pari-
son of 1073 MBq and 3700 MBq iodine-131 in post- operative ablation of residual thyroid tissue in patients with differentiated thyroid cancer. J Nucl Med 32: 252-254, 1991
23) Higashi T, Nishii R, Yamada S, Nakamoto Y, Ishizu K, Kawase S, Togashi K, Itasaka S, Hiraoka M, Misaki T, Konishi J : Delayed initial radioactive iodine ther- apy resulted in poor survival in patients with meta- static differentiated thyroid carcinoma : a retrospec- tive statistical analysis of 198 cases. J Nucl Med 52: 683-689, 2011
131I 1,110 MBq
2009 1 2011 3
1,110 MBq 131I 50
131I Whole body scan
41 82.0%
131I 1,110 MBq