Abstract. Biomarkers that can accurately predict treatment response are required for indicating optimal neoadjuvant treatments. The current study assessed the predictive value of secreted protein acidic and rich in cysteine (SPARC) mRNA expression for the response to neoadjuvant nab‑paclitaxel (nab‑PTX) therapy in patients with breast cancer. It was hypothesized that SPARC expression can affect the response to albumin‑bound taxanes, including nab‑PTX since SPARC binds albumin with a high affinity. Pre‑therapeutic specimens of core needle biopsies were analyzed from 50 patients in a phase II trial of neoadjuvant nab‑PTX and the factors that were associated with a pathological complete response (pCR) were assessed. The pre‑therapeutic tumor mRNA levels of chemo‑
therapy‑related proteins were quantified, including SPARC, and the correlations with post‑therapeutic clinicopatho‑
logical factors were assessed, including with pCR. The results demonstrated that pre‑therapeutic SPARC mRNA expression
was significantly higher in non‑pCR patients compared with patients with pCR (92.37±55.33 vs. 56.53±30.19; P=0.027).
A cutoff point of 48.5 was determined using receiver oper‑
ating characteristic (ROC) curve analysis (sensitivity, 83.3%;
specificity, 50.0%), and patients were classified into low and high SPARC expression groups. High SPARC expression was associated with histological grade (P=0.035), estrogen receptor expression (P=0.037), and progesterone receptor expression (P=0.002) but not with HER2 (P=0.895), and Ki‑67 LI (P=0.743) expression. The results of the current study indicated that a high SPARC mRNA expression was a nega‑
tive predictor of pCR following neoadjuvant nab‑PTX therapy regardless of breast cancer subtype. The phase II study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the National Hospital Organization Takasaki General Medical Center (Registration nos. H23‑9 and H23‑33).
Introduction
Breast cancer is the most common cancer in women and is a leading cause of mortality worldwide (1). Treatment strate‑
gies have been constantly evolving and chemotherapy has shifted from postoperative administration to preoperative therapy, or neoadjuvant therapy. Good response to neoadjuvant therapy allows patients to be treated using breast‑conserving surgery rather than using mastectomy (2). Furthermore, a pathological complete response (pCR) after neoadjuvant therapy improves survival (3), particularly in subtypes such as triple‑negative breast cancer (4). Breast cancer subtypes have different molecular profiles and biological behaviours and, thus, require individualized therapies (5). Patients who do not receive optimal chemotherapy suffer unnecessary toxic side effects. Therefore, pre‑therapeutic biomarkers that can adequately predict treatment response, particularly of pCR, are necessary for selecting the most adequate neoadjuvant chemotherapy for each patient. So far, several biomarkers, such as thymidylate synthase (TS) (6), dihydropyrimidine
The pathological complete response and secreted protein acidic and rich in cysteine expression in patients with breast cancer
receiving neoadjuvant nab‑paclitaxel chemotherapy
YUKO NAKAZAWA1‑3, SESHIRU NAKAZAWA1, SASAGU KUROZUMI1, MISATO OGINO1,2, YUKIO KOIBUCHI2, HIROKI ODAWARA4, TETSUNARI OYAMA3, JUN HORIGUCHI5, TAKAAKI FUJII1 and KEN SHIRABE1
1Department of General Surgical Science, Gunma University Graduate School of Medicine, Maebashi, Gunma 371‑8511;
2Department of Breast and Endocrine Surgery, National Hospital Organization Takasaki General Medical Center, Takasaki, Gunma 370‑0829; 3Department of Diagnostic Pathology, Gunma University Graduate School of Medicine, Maebashi, Gunma 371‑8511; 4Department of Surgery, Toho Hospital, Midori, Gunma 376‑0121; 5Department of Breast Surgery,
International University of Health and Welfare, Chiba 286‑8686, Japan Received July 21, 2019; Accepted December 3, 2019
DOI: 10.3892/ol.2020.11354
Correspondence to: Professor Takaaki Fujii, Department of General Surgical Science, Gunma University Graduate School of Medicine, 3‑39‑22 Showa‑machi, Maebashi, Gunma 371‑8511, Japan E‑mail: ftakaaki@gunma‑u.ac.jp
Abbreviations: SPARC, secreted protein acidic and rich in cysteine; nab‑PTX, nab‑paclitaxel; pCR, pathological complete response; HER2, human epidermal growth factor receptor 2; IHC, immunohistochemistry; ER, estrogen receptor; PgR, progesterone receptor; AST, aspartate aminotransferase; ULN, upper limit of normal; ALT, alanine aminotransferase; FISH, fluorescence in situ hybridization; RT‑qPCR, quantitative reverse‑transcription PCR;
LI, labeling index; FFPE, formalin‑fixed, paraffin‑embedded; FEC, 5‑FU, epirubicin and cyclophosphamide; HER, trastuzumab Key words: secreted protein acidic and rich in cysteine, nab‑paclitaxel, breast cancer, pathological complete response, neoadjuvant therapy
tion and cell migration, and its overexpression is associated with tumor growth, metastasis, and aggressiveness (12‑19).
Studies have revealed the association of high SPARC expres‑
sion with poor prognosis and treatment response in breast cancer (12,19‑21). A high SPARC expression evaluated by IHC has been reported to be associated with a high treatment response (20), whereas a high SPARC expression assessed by mRNA levels has been reported to be associated with low treatment response in breast cancer (21). The role of SPARC in breast cancer has not yet been established and a more focused analysis between SPARC expression and response to specific treatments is necessary to use SPARC as a biomarker.
In this study, we focused on the predictive role of SPARC in response to neoadjuvant treatment with nab‑paclitaxel (nab‑PTX), which is a nanoparticle albumin‑bound taxane drug used as neoadjuvant treatment for breast cancer. We analyzed the pre‑treatment specimens of a phase II trial of neoadjuvant nab‑PTX chemotherapy for breast cancer. A previous study that compared treatment with nab‑PTX and docetaxel has shown a higher therapy response and prolonged progression free survival for patients treated with nab‑PTX (22). Also, ongoing trials, such as the phase III GeparSepto trial, have shown that a regimen including nab‑PTX achieves higher pCR rates than a regimen with solvent‑based PTX (23). Since SPARC binds albumin with high affinity, we hypothesized that SPARC expression levels can affect the response to albumin‑bound taxanes such as nab‑PTX.
The purpose of our study was to evaluate the predictive value of SPARC mRNA expression for the response to neoad‑
juvant nab‑PTX therapy in breast cancer patients. We analyzed patient specimens from a phase II trial involving nab‑PTX and evaluated the association of pre‑treatment SPARC mRNA expression with the response to neoadjuvant nab‑PTX treat‑
ment. Our results suggested that SPARC mRNA expression in breast cancer is a negative predictor of treatment response to neoadjuvant nab‑PTX therapy.
Materials and methods
Patients and data. We retrospectively analyzed data from a total of 50 consecutive patients who were enrolled in a single center phase II trial of neoadjuvant nab‑PTX therapy (National Hospital Organization Takasaki General Medical Center, Takasaki, Japan) between May 2011 and September 2013. We collected the clinicopathological data such as age, tumor subtype, tumor staging (based on the Union for International Cancer Control TNM classification, 7th edition).
Immunohistochemistry (IHC) analysis of hormone receptors [estrogen (ER) or progesterone (PgR)], HER2 score, and Ki67 expression of the primary tumor was assessed via our staining
HER2‑negative breast cancer patients, neoadjuvant chemo‑
therapy comprised the administration of nab‑PTX, followed by the administration of 5‑FU, epirubicin, and cyclophospha‑
mide. For HER2‑positive breast cancer patients, neoadjuvant chemotherapy comprised the concurrent administration of nab‑PTX and trastuzumab, followed by surgery and post‑oper‑
ative administration of trastuzumab for one year. Surgery was performed 6 months after treatment initiation, and the opera‑
tive method (mastectomy or breast‑conserving surgery) was selected based on the post‑treatment tumor size and patient's preference. Sentinel lymph node dissection was performed for patients who were preoperatively diagnosed as negative for lymph node metastasis, and axillary lymph node dissection was performed for all patients who were suspected or diagnosed as positive for lymph node metastases. We enrolled patients with cytologically or histologically confirmed unilateral primary breast cancer, aged between 20 and 75 years, with an ECOG performance status of grade 0 or 1, and without any prior breast cancer treatment. Further eligibility criteria were: No severe comorbidities such as uncontrollable diabetes, infection, cardiac disease, or psychological symptoms; no interstitial lung disease confirmed on chest radiography; no brain metastases;
no history of severe drug allergy; no concurrent malignant disease; no history of inflammatory breast cancer; and no pregnancy. Laboratory requirements included white blood cell counts ≥4.0x103 cells per mm3, neutrophil counts ≥2.0x103 cells per mm3, platelets ≥100x103 cells per mm3, hemoglobin level
≥9.0 g/dl, aspartate aminotransferase (AST) level ≤2.5x upper limit of normal (ULN), alanine aminotransferase (ALT) level
≤2.5xULN, total bilirubin level ≤1.5 mg/dl, and creatinine level
≤1.5 mg/dl. Additional requirement for HER2‑positivity were 3+ HER2 by IHC or 2+ by IHC and positive by fluorescence in situ hybridization (FISH) and only tumors with a diameter of
>1 cm were included for HER2‑positive breast cancer. Informed consent was obtained from all patients prior to enrollment in the study. The phase II study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the National Hospital Organization Takasaki General Medical Center (Registration numbers:
H23‑9 and H23‑33).
Macro‑dissection and analysis of mRNA expression. We performed macro‑dissection of tumor cells in core needle biopsy specimens to exclude the influence from stromal tissue contamination and quantified the expression levels of chemotherapy‑related factors using RT‑qPCR. A pathologist reviewed representative hematoxylin and eosin‑stained slides from formalin‑fixed, paraffin‑embedded (FFPE) core needle biopsy specimens. Tumor tissue was selected and dissected via manual macro‑dissection (Fig. S1).
RNA was isolated from the tumor tissues using the RNeasy FFPE Kit (Qiagen). cDNA was prepared using High Capacity Reverse Transcription kit (Life Technologies) according to the manufacturer's instructions. SPARC, TS, DPD, MDR1, MRP1, and Topo IIα expression levels were determined using TaqMan real‑time PCR (TaqMan array card; Life Technologies) after TaqMan assay‑based pre‑amplification. Briefly, 2.5 µl cDNA was pre‑amplified using the TaqMan PreAmp Master Mix (2x) and a pool of TaqMan® Gene Expression Assays (0.2x) in a 10‑µl PCR reaction. The pre‑amplification cycling conditions included 95˚C for 10 min followed by 14 cycles of 95˚C for 15 sec and 60˚C for 4 min. Each amplified cDNA sample was diluted 20 times in TE buffer. Amplified cDNA (25 µl) was added to 25 µl RNase‑free water and 50 µL of 2x TaqMan Gene Expression Master Mix. The mixture was then transferred to a loading port for the TaqMan array card.
The array card was centrifuged twice and sealed, and PCR was performed using the Applied Biosystems Prism 7900HT Sequence Detection system (Life Technologies). The ther‑
mocycler protocol included the following conditions: 50˚C for 2 min and 94.5˚C for 10 min, followed by 40 cycles of 97˚C for 30 sec and 59.7˚C for 1 min. Beta‑actin was used as an internal standard for normalization. The gene expression (relative mRNA) levels were expressed as ratios (differences between the Ct values) between the gene of interest and the reference gene. The assay IDs used in the array card are shown in Table SI.
Immunohistochemical evaluation and subtype classification.
IHC analysis was performed using the core needle biopsy samples. A pathologist assessed the expressions of hormone receptors (ER and PgR), HER2, and Ki67 in all the speci‑
mens. ER and PgR expression levels were scored from 0 to 8 according to the Allred score (25) and expression was clas‑
sified as negative from 0 to 3 and positive from 4 to 8. HER2 expression was positive if the results were 3+ or 2+ by IHC and positive by FISH. The Ki67 score was calculated at hot spots and classified as low if ≤30% and as high if >30%. To assess the correlation of SPARC mRNA expression with its protein expression, IHC staining of SPARC was performed (n=10). The cytoplasmic expression of SPARC was classified as low, medium, or high (Fig. 2). The antibodies used were anti‑ER (SP1; Ventana Medical Systems), anti‑PgR (1E2;
Ventana Medical Systems), anti‑HER2 (4B5; Ventana Medical Systems), anti‑Ki‑67 (30‑9; Ventana Medical Systems), and anti‑SPARC (ON1‑1; Thermo Fisher Scientific). Breast cancer subtypes were defined according to the IHC results as luminal type (ER‑positive, HER2‑negative), luminal‑HER2 type (ER‑positive and HER2‑positive), HER2 type (ER‑negative and HER2‑positive), and triple‑negative (ER‑negative and HER2‑negative) breast cancer.
Statistical analysis. Statistical analysis was performed using Mann‑Whitney's U test and Kruskal‑Wallis test for continuous variables and chi‑square test for categorical variables. ROC curve analysis was used to assess the cutoff point of mRNA SPARC expression between pCR and non‑pCR. P<0.05 was considered to indicate a statistically significant difference.
All statistical analyses were performed using the IBM SPSS Statistics software (v24, IBM Corp.).
Results
Patient characteristics. The median age of patients was 55 years (range, 30‑75 years). We found 30.0% luminal type, 18.0% luminal‑HER2 type, 22.0% HER2 type, and 30.0%
triple‑negative breast cancer patients. All patients with luminal type breast cancer enrolled in the phase II trial had lymph node metastasis. ER, PgR, and HER2 expressions were positive in 48.0, 36.0, and 40.0% of patients, respectively. The mean score of Ki67 was 48.2±33.2%, with 36.0% of patients exhibiting low Ki‑67 expression and 64.0% high Ki‑67 expression.
Fourteen (28.0%) patients achieved pCR after neoadjuvant therapy including nab‑PTX.
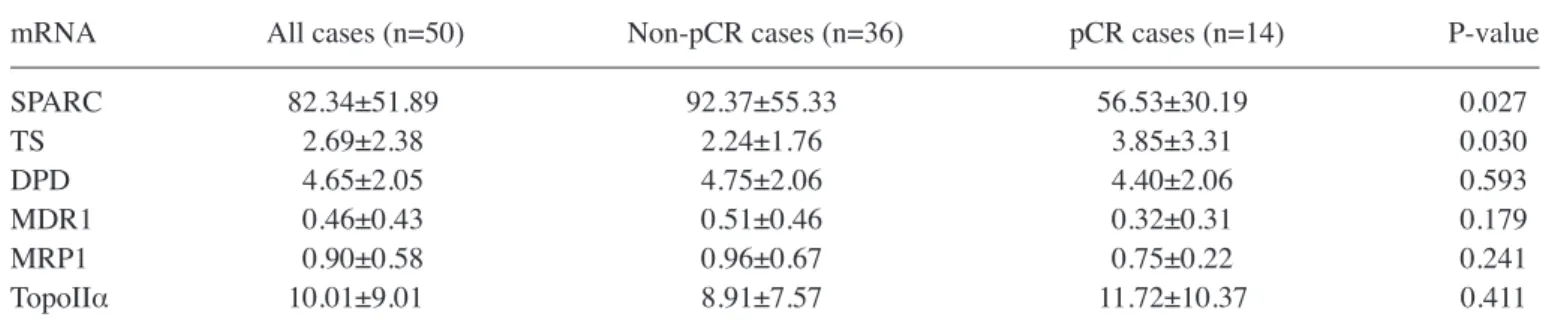
Intra‑tumor mRNA expression of chemotherapy‑related proteins. The correlations between the intra‑tumor mRNA levels of SPARC, TS, DPD, MDR1, MRP1, and Topo IIα and the treatment response were assessed (Table I). SPARC mRNA expression was significantly higher in the non‑pCR group (P=0.027). Also, TS mRNA expression was signifi‑
cantly higher in the pCR group (P=0.030). However, other markers as DPD, MDR1, MRP1, and Topo IIα were not the significant predictive markers of pCR. The intensity of SPARC expression detected by IHC correlated with SPARC mRNA expression levels (P=0.043; Fig. 3).
Figure 1. Treatment protocol of phase II trial of neoadjuvant nab‑paclitaxel. For patients that are HER2‑negative, nab‑PTX (260 mg/m2) was administered every 3 weeks for 4 courses, followed by administration of FEC (500 mg/m2 5‑FU, 100 mg/m2 epirubicin and 500 mg/m2 cyclophosphamide) every 3 weeks for 4 courses. For HER2‑positive patients, nab‑PTX (260 mg/m2) and trastuzumab (initial dose 8 mg/kg, sequential dose 6 mg/kg) was administered every 3 weeks for 4 courses. HER2, human epidermal growth factor receptor 2; nab‑PTX, nab‑paclitaxel; FEC, 5‑FU, epirubicin and cyclophosphamide; HER, trastuzumab.
Analysis according to SPARC expression. The ROC curve for the relative mRNA SPARC expression between pCR and non‑pCR is shown in Fig. S2. The area under the curve was 0.700, and the cutoff point was set at 48.5 (sensitivity, 83.3%;
specificity, 50.0%). Patients were classified into low and high SPARC expression groups (Table II). Patients in the low SPARC expression group had significantly higher pCR rates (P=0.029). We found no differences in the mean age (P=0.467) and tumor staging (P=0.507) between patients in the two groups. However, patients with low SPARC mRNA expres‑
sion had a significantly higher histological grade (P=0.035), lower ER expression (P=0.037), and lower PgR expression (P=0.002) in core needle biopsy specimen. In contrast, there were no significant differences in the HER2 (P=0.895), and Ki‑67 LI (P=0.285) expressions.
Discussion
Our study revealed that the pre‑therapeutic SPARC mRNA expression was significantly higher in the non‑pCR patients than in the pCR patients after neoadjuvant nab‑PTX therapy.
Conclusively, our results suggested that the relative SPARC mRNA expression level predicts the treatment response to neoadjuvant nab‑PTX therapy in breast cancer patients.
SPARC is a multifunctional matricellular glycoprotein that controls physiological and pathological processes, such as cellular differentiation, development, remodeling, cell
turnover, and tissue repair (12‑18). It is highly expressed in several types of tumors, such as melanoma (26), glioblas‑
toma (27), prostate (28), colorectal (29), pancreatic (30), and gastric (31) cancers. This overexpression in tumors suggests
Figure 2. Immunohistochemistry analysis of cytoplasmic SPARC expression in breast cancer specimens. (A) Low SPARC expression (magnification, x200).
(B) Medium SPARC expression (magnification, x200). (C) High SPARC expression (magnification, x200). SPARC, secreted protein acidic and rich in cysteine.
Figure 3. Correlation between SPARC mRNA values and IHC expression.
Expression of SPARC mRNA indicated a significant difference between low (n=3), medium (n=4) and high SPARC expression groups (n=3) detected using IHC (P=0.043). The x‑axis represents expression of SPARC classified according to IHC and the y‑axis represents the mRNA expression assessed using RT‑qPCR. *P<0.05; SPARC, secreted protein acidic and rich in cysteine; IHC, immunohistochemistry.
All values are mean ± SE. pCR, pathological complete response; SPARC, secreted protein acidic and rich in cysteine; TS, thymidylate synthase;
DPD, dihydropyrimidine dehydrogenase; MDR1, ATP‑binding cassette, sub‑family B, member 1; MRP1, ATP‑binding cassette, sub‑family C, member 1; Topo IIα, Topoisomerase (DNA) II alpha.
that SPARC promotes tumor development and is a potential treatment target. Although the association of high SPARC expression with some cancers remains controversial (32), several studies have reported high SPARC expressions in breast cancers (19‑21). Moreover, SPARC is reportedly expressed in the juxta‑tumoral stromal cells, indicating its possible role in breast cancer invasion (33). Yet, its prognostic role in breast cancer remains indeterminate, and the reports have been contradictory. Some studies have found that high SPARC expression is associated with low overall survival (19‑21), whereas others have reported that low SPARC expression is associated with low disease‑free and overall survival (34).
Moreover, the association of SPARC expression with breast cancer subtypes also varies between studies. It has also been frequently expressed in triple‑negative breast cancer (35) or has shown an inverse correlation with ER expression, thereby associating with less differentiated and more aggressive tumors (36).
An important advance resulting from our study is the finding that low SPARC mRNA expression is associated with higher pCR rates after neoadjuvant nab‑PTX therapy. Thus far, the prognostic value of SPARC expression as a marker of treatment response remains controversial. For example, a previous study has reported an association of high SPARC expression with low pCR rates in HER2‑type breast cancer patients (21), whereas another study has reported no asso‑
ciation of SPARC expression with the response to nab‑PTX therapy in metastatic breast cancer patients (35). In addition, high SPARC expression has been reported to be associated with a high pCR rate after treatment including docetaxel, doxorubicin, and cyclophosphamide (36). These conflicting results may be caused by differences in treatment protocol, ratio of breast cancer subtypes enrolled in the study, and methods used for sample analysis (19‑21,34‑36). Thus, for overcoming the difference in treatment protocol, our study focused on patients who were enrolled in a study on phase II neoadjuvant nab‑PTX therapy study within a single institute.
In theory, because SPARC is an albumin‑binding protein, its high expression in cancer cells and the surrounding stroma would increase the accumulation of albumin‑bound drugs in the tumor, thereby leading to a higher efficiency and less side effects (37). Therefore, the initial hypothesis was that tumors with high SPARC expression would show better treatment response to nab‑PTX therapy (38). However, our results were contrary to this hypothesis, and the low SPARC expression group showed higher pCR rates to nab‑PTX therapy.
Perou et al initially suggested a molecular classification as the intrinsic subtypes for breast cancer (39,40). Response to specific treatments may vary according to breast cancer subtype. For example, triple‑negative breast cancer patients showed an increased pCR rate in response to neoadjuvant chemotherapy with nab‑PTX in the GeparSepto‑GBG 69 study (23). The relation between SPARC expression and breast cancer subtypes is inconsistent between studies (21,23,36,41).
We showed here that SPARC expression was associated with high PgR and ER expression. PgR is known to be induced by ER and acts as a key factor in induction, progression and maintenance of the neoplastic phenotype of ER‑positive breast cancer (42,43). Also, recent clinical findings demonstrated that the PgR status is associated with low response to neoadjuvant Table II. Association between SPARC mRNA expression and
clinicopathological features.
SPARC expression ‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑‑
Low High expression expression Characteristics (n=13) (n=37) P‑value
Age (years) 0.467
Mean ± SE 57.5±12.4 54.7±12.2
Range 36‑72 30‑75
Stage 0.507
I 2 6
II 10 23
III 1 8
Tumor size (cm) 0.545
Mean ± SE 3.0±1.1 2.8±1.4
Range 1.8‑5.7 1.1‑7.8
Histological grade 0.035
Grade 1‑2 2 18
Grade 3 11 19
Nodal status 0.191
Negative 8 15
Positive 5 22
ER 0.037
Negative 10 16
Positive 3 21
PgR 0.002
Negative 13 19
Positive 0 18
HER2 0.895
Negative 8 22
Positive 5 15
Ki‑67 labeling 0.285
index (%)
Mean ± SE 56.69±34.69 44.53±33.00
Range 9‑99 3‑98
Ki‑67 0.743
Low (≤30%) 4 14
High (30%<) 9 22
Missing 0 1
IHC based subtypes 0.219
Luminal 2 13
Luminal‑HER2 1 8
HER2 4 7
Triple‑negative 6 9
pCR 0.029
No 6 30
Yes 7 7
SPARC, secreted protein acidic and rich in cysteine; NG, nuclear grade; ER, estrogen receptor; PgR, progesterone receptor; HER2, human epidermal growth factor receptor 2; pCR, pathological complete response.
For example, a high SPARC expression evaluated by IHC has been reported to be associated with a high pCR rate (20), whereas a high SPARC expression assessed by mRNA levels has been reported to be associated with low pCR rate (21). In the present study, we focused on tumor‑specific expression using macro‑dissection to extract tumor mRNA. Also, we evaluated expression of target proteins by RT‑qPCR. SPARC is a secreted protein and, extracellularly secreted proteins cannot be intracellularly detected by IHC unless secretion is inhibited (45). Moreover, SPARC expression also exists in the stromal tissues and inclusion of stromal components can falsely elevate true SPARC expression levels in tumor cells. Indeed, a study on colorectal cancers has shown a decrease in SPARC expression after the microdissection of tumor components compared with the initial expression analyzed in the bulk undissected tumor (46). Previously, a study on ovarian cancers has reported that the use of different SPARC antibodies can result in inconsistencies in the SPARC expression patterns (32). We confirmed the positive correlation between mRNA and protein expressions of SPARC in a small cohort. To be reliable and represent‑
able for SPARC‑IHC scoring, further analysis regarding the inter‑observer and inter‑institutional variability with a larger cohort is warrant.
In our patient cohort, ER, PgR, and HER2 expressions were positive in 48.0, 36.0, and 40.0% of patients, respectively, and triple‑negative breast cancer patients were 30.0%. Our present translational research is based on a phase II trial of neoadjuvant nab‑PTX chemotherapy including all breast cancer subtypes.
The evaluation of the pathological response of neoadjuvant chemotherapy have mainly been determined based on the results of NSABP protocol B‑18 (47) and B‑27 (48). These studies confirmed the utility of pCR as a prognositic surro‑
gator for breast cancer patient with neoadjuvant chemotherapy.
However, von Minckwitz G et al (4) suggested that pCR is a potent surrogate marker to predict the prognosis in most patients with breast cancer, but not in patients with ER‑positive tumors. However, they also demonstrated that pCR was predic‑
tive of good survival rate in ER‑positive tumors with high tumour proliferation (49). Therefore, ER‑positive early‑stage breast cancer patients with low tumour proliferation usually undergo surgery at first and thus do not meet the eligibility criteria of our phase II trial. This might be a reason why our study population had low rate of breast cancer with hormone receptor expression and a high rate of triple‑negative breast cancer patients.
We recognize several limitations to our study. First, this study is a part of a phase II trial conducted at a single institu‑
tion, and its small sample size may have influenced the results.
Further large‑scale studies will be necessary to validate our
needed to explore the effects of SPARC mRNA expression in stromal cells in response to nab‑PTX therapy.
In conclusion, we found that high SPARC mRNA expres‑
sion was a negative predictor of pCR after neoadjuvant nab‑PTX therapy. The pre‑therapeutic analysis of SPARC mRNA expression in core needle biopsy specimens may be valuable for selecting the optimal patients for neoadjuvant nab‑PTX therapy regardless of their breast cancer subtype.
Our results suggest that a high SPARC expression in tumor cells indicates that regimens other than nab‑PTX should be selected. A preoperative panel of tumor‑specific mRNAs including SPARC may lead to a more tailored selection of neoadjuvant treatment regimen for each patient.
Acknowledgements
The authors would like to thank Ms. Fumie Takada and Ms.
Harumi Kanai (Department of General Surgical Science, Gunma University Graduate School of Medicine) for their secretarial assistance.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present study are available from the corresponding author on reasonable request.
Authors' contributions
YN and SN analyzed data and wrote the initial draft of the manuscript. YN, SN, MO, HO and YK collected data and were involved in the initial study conception and design. TO contributed to the analysis and assessment of pathological data.
SN, SK, MO, YK, TO, TF, JH and KS interpreted the results and were involved in drafting the manuscript and revising the manuscript critically for important intellectual content. TF gave final approval of the version to be published. All authors have read and approved the final manuscript.
Ethics approval and consent to participate
The present study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the National Hospital Organization Takasaki General Medical Center (registration nos. H23‑9 and H23‑33). Written informed consent was obtained from all patients prior to enrollment in the study.
Patient consent for publication Not applicable.
Competing interests
The authors declare that they have no competing interests.
References
1. Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D and Bray F: Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer 136: E359‑E386, 2015.
2. Early Breast Cancer Trialists' Collaborative Group (EBCTCG):
Long‑term outcomes for neoadjuvant versus adjuvant chemo‑
therapy in early breast cancer: Meta‑analysis of individual patient data from ten randomised trials. Lancet Oncol 19: 27‑39, 2018.
3. Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N, Bonnefoi H, Cameron D, Gianni L, Valagussa P, et al:
Pathological complete response and long‑term clinical benefit in breast cancer: The CTNeoBC pooled analysis. Lancet 384:
164‑172, 2014.
4. von Minckwitz G, Untch M, Blohmer JU, Costa SD, Eidtmann H, Fasching PA, Gerber B, Eiermann W, Hilfrich J, Huober J, et al:
Definition and impact of pathologic complete response on prog‑
nosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J Clin Oncol 30: 1796‑1804, 2012.
5. Esserman LJ, Berry DA, Cheang MC, Yau C, Perou CM, Carey L, DeMichele A, Gray JW, Conway‑Dorsey K, Lenburg ME, et al:
Chemotherapy response and recurrence‑free survival in neoad‑
juvant breast cancer depends on biomarker profiles: Results from the I‑SPY 1 TRIAL (CALGB 150007/150012; ACRIN 6657).
Breast Cancer Res Treat 132: 1049‑1062, 2012.
6. Foekens JA, Romain S, Look MP, Martin PM and Klijn JG:
Thymidine kinase and thymidylate synthase in advanced breast cancer: Response to tamoxifen and chemotherapy. Cancer Res 61: 1421‑1425, 2001.
7. Yu Z, Yang Q, Sun J and Zhen J: Dihydropyrimidine dehydro‑
genase activity correlates with fluorouracil sensitivity in breast cancer. Exp Oncol 29: 192‑196, 2007.
8. Trock BJ, Leonessa F and Clarke R: Multidrug resistance in breast cancer: A meta‑analysis of MDR1/gp170 expression and its possible functional significance. J Natl Cancer Inst 89:
917‑931, 1997.
9. Taheri M and Mahjoubi F: MRP1 but not MDR1 is associated with response to neoadjuvant chemotherapy in breast cancer patients. Dis Markers 34: 387‑393, 2013.
10. Du Y, Zhou Q, Yin W, Zhou L, Di G, Shen Z, Shao Z and Lu J:
The role of topoisomerase IIα in predicting sensitivity to anthra‑
cyclines in breast cancer patients: A meta‑analysis of published literatures. Breast Cancer Res Treat 129: 839‑848, 2011.
11. Tokiniwa H, Horiguchi J, Takata D, Kikuchi M, Rokutanda N, Nagaoka R, Sato A, Odawara H, Tozuka K, Oyama T and Takeyoshi I: Topoisomerase II alpha expression and the Ki‑67 labeling index correlate with prognostic factors in estrogen receptor‑positive and human epidermal growth factor type‑2‑negative breast cancer. Breast Cancer 19: 309‑314, 2012.
12. Zhu A, Yuan P, Du F, Hong R, Ding X, Shi X, Fan Y, Wang J, Luo Y, Ma F, et al: SPARC overexpression in primary tumors correlates with disease recurrence and overall survival in patients with triple negative breast cancer. Oncotarget 7: 76628‑76634, 2016.
13. Framson PE and Sage EH: SPARC and tumor growth: Where the seed meets the soil? J Cell Biochem 92: 679‑690, 2004.
14. Brekken RA and Sage EH: SPARC, a matricellular protein: At the crossroads of cell‑matrix communication. Matrix Biol 19:
816‑287, 2001.
15. Arnold SA and Brekken RA: SPARC: A matricellular regulator of tumorigenesis. J Cell Commun Signal 3: 255‑273, 2009.
16. Podhajcer OL, Benedetti LG, Girotti MR, Prada F, Salvatierra E and Llera AS: The role of the matricellular protein SPARC in the dynamic interaction between the tumor and the host. Cancer Metastasis Rev 27: 691‑705, 2008.
17. Yan Q and Sage EH: SPARC, a matricellular glycoprotein with important biological functions. J Histochem Cytochem 47:
1495‑1506, 1999.
18. Bradshaw AD and Sage EH: SPARC, a matricellular protein that functions in cellular differentiation and tissue response to injury.
J Clin Invest 107: 1049‑1054, 2001.
19. Helleman J, Jansen MP, Ruigrok‑Ritstier K, van Staveren IL, Look MP, Meijer‑van Gelder ME, Sieuwerts AM, Klijn JG, Sleijfer S, Foekens JA and Berns EM: Association of an extra‑
cellular matrix gene cluster with breast cancer prognosis and endocrine therapy response. Clin Cancer Res 14: 5555‑5564, 2008.
20. Hsiao YH, Lien HC, Hwa HL, Kuo WH, Chang KJ and Hsieh FJ:
SPARC (osteonectin) in breast tumors of different histologic types and its role in the outcome of invasive ductal carcinoma.
Breast J 16: 305‑308, 2010.
21. Azim HA Jr, Singhal S, Ignatiadis M, Desmedt C, Fumagalli D, Veys I, Larsimont D, Piccart M, Michiels S and Sotiriou C:
Association between SPARC mrna expression, prognosis and response to neoadjuvant chemotherapy in early breast cancer: A pooled in‑silico analysis. PLoS One 8: e62451, 2013.
22. Gradishar WJ, Krasnojon D, Cheporov S, Makhson AN, Manikhas GM, Clawson A and Bhar P: Significantly longer progression‑free survival with nab‑paclitaxel compared with docetaxel as first‑line therapy for metastatic breast cancer. J Clin Oncol 27: 3611‑3619, 2009.
23. Untch M, Jackisch C, Schneeweiss A, Conrad B, Aktas B, Denkert C, Eidtmann H, Wiebringhaus H, Kümmel S, Hilfrich J, et al:
Nab‑paclitaxel versus solvent‑based paclitaxel in neoadjuvant chemotherapy for early breast cancer (GeparSepto‑GBG 69): A randomised, phase 3 trial. Lancet Oncol 17: 345‑356, 2016.
24. Obayashi S, Horiguchi J, Higuchi T, Katayama A, Handa T, Altan B, Bai T, Bao P, Bao H, Yokobori T, et al: Stathmin1 expression is associated with aggressive phenotypes and cancer stem cell marker expression in breast cancer patients. Int J Oncol 51: 781‑790, 2017.
25. Allred DC, Harvey JM, Berardo M and Clark GM: Prognostic and predictive factors in breast cancer by immunohistochemical analysis. Mod Pathol 11: 155‑168, 1998.
26. Ledda F, Bravo AI, Adris S, Bover L, Mordoh J and Podhajcer OL:
The expression of the secreted protein acidic and rich in cysteine (SPARC) is associated with the neoplastic progression of human melanoma. J Invest Dermatol 108: 210‑214, 1997.
27. Rempel SA, Golembieski WA, Fisher JL, Maile M and Nakeff A:
SPARC modulates cell growth, attachment and migration of U87 glioma cells on brain extracellular matrix proteins.
J Neurooncol 53: 149‑160, 2001.
28. Thomas R, True LD, Bassuk JA, Lange PH and Vessella RL:
Differential expression of osteonectin/SPARC during human prostate cancer progression. Clin Cancer Res 6: 1140‑1149, 2000.
29. Liu QZ, Gao XH, Chang WJ, Wang HT, Wang H, Cao GW and Fu CG: Secreted protein acidic and rich in cysteine expression in human colorectal cancer predicts postoperative prognosis. Eur Rev Med Pharmacol Sci 19: 1803‑1811, 2015.
30. Guweidhi A, Kleeff J, Adwan H, Giese NA, Wente MN, Giese T, Büchler MW, Berger MR and Friess H: Osteonectin influences growth and invasion of pancreatic cancer cells. Ann Surg 242:
224‑134, 2005.
31. Wang CS, Lin KH, Chen SL, Chan YF and Hsueh S:
Overexpression of SPARC gene in human gastric carcinoma and its clinic‑pathologic significance. Br J Cancer 91: 1924‑1930, 2004.
32. Yiu GK, Chan WY, Ng SW, Chan PS, Cheung KK, Berkowitz RS and Mok SC: SPARC (secreted protein acidic and rich in cysteine) induces apoptosis in ovarian cancer cells. Am J Pathol 159:
609‑622, 2001.
33. Iacobuzio‑Donahue CA, Argani P, Hempen PM, Jones J and Kern SE: The desmoplastic response to infiltrating breast carcinoma:
Gene expression at the site of primary invasion and implications for comparisons between tumor types. Cancer Res 62: 5351‑5357, 2002.
34. Nagai MA, Gerhard R, Fregnani JH, Nonogaki S, Rierger RB, Netto MM and Soares FA: Prognostic value of NDRG1 and SPARC protein expression in breast cancer patients. Breast Cancer Res Treat 126: 1‑14, 2011.
35. Schneeweiss A, Seitz J, Smetanay K, Schuetz F, Jaeger D, Bachinger A, Zorn M, Sinn HP and Marmé F: Efficacy of nab‑pacli‑
taxel does not seem to be associated with SPARC expression in metastatic breast cancer. Anticancer Res 34: 6609‑6615, 2014.
36. Lindner JL, Loibl S, Denkert C, Ataseven B, Fasching PA, Pfitzner BM, Gerber B, Gade S, Darb‑Esfahani S, Sinn BV, et al:
Expression of secreted protein acidic and rich in cysteine (SPARC) in breast cancer and response to neoadjuvant chemo‑
therapy. Ann Oncol 26: 95‑100, 2015.
37. Yardley DA: Nab‑Paclitaxel mechanisms of action and delivery.
J Control Release 170: 365‑372, 2013.
tumours is inversely correlated with oestrogen receptor content.
Eur J Cancer 33: 1654‑1660, 1997.
42. Kurozumi S, Matsumoto H, Hayashi Y, Tozuka K, Inoue K, Horiguchi J, Takeyoshi I, Oyama T and Kurosumi M: Power of PgR expression as a prognostic factor for ER‑positive/HER2‑negative breast cancer patients at intermediate risk classified by the Ki67 labeling index. BMC Cancer 17: 354, 2017.
43. Kurozumi S, Matsumoto H, Inoue K, Tozuka K, Hayashi Y, Kurosumi M, Oyama T, Fujii T, Horiguchi J and Kuwano H:
Impact of combining the progesterone receptor and preoperative endocrine prognostic index (PEPI) as a prognostic factor after neoadjuvant endocrine therapy using aromatase inhibitors in postmenopausal ER positive and HER2 negative breast cancer.
PLoS One 13: e0201846, 2018.
44. Kurozumi S, Inoue K, Takei H, Matsumoto H, Kurosumi M, Horiguchi J, Takeyoshi I and Oyama T: ER, PgR, Ki67, p27(Kip1), and histological grade as predictors of pathological complete response in patients with HER2‑positive breast cancer receiving neoadjuvant chemotherapy using taxanes followed by fluorouracil, epirubicin, and cyclophosphamide concomitant with trastuzumab. BMC Cancer 15: 622, 2015.
45. Bekki Y, Yoshizumi T, Shimoda S, Itoh S, Harimoto N, Ikegami T, Kuno A, Narimatsu H, Shirabe K and Maehara Y: Hepatic stellate cells secreting WFA+‑M2BP: Its role in biological interactions with kupffer cells. J Gastroenterol Hepatol 32: 1387‑1393, 2017.
2006.
49. von Minckwitz G: Neoadjuvant chemotherapy in breast cancer‑insights from the German experience. Breast Cancer 19:
282‑288, 2012.
50. Puolakkainen PA, Brekken RA, Muneer S and Sage EH:
Enhanced growth of pancreatic tumors in sparc‑null mice is associated with decreased deposition of extracellular matrix and reduced tumor cell apoptosis. Mol Cancer Res 2: 215‑224, 2004.
51. Said N and Motamed K: Absence of host‑secreted protein acidic and rich in cysteine (SPARC) augments peritoneal ovarian carci‑
nomatosis. Am J Pathol 167: 1739‑1752, 2005.
52. Kim H, Samuel S, Lopez‑Casas P, Grizzle W, Hidalgo M, Kovar J, Oelschlager D, Zinn K, Warram J and Buchsbaum D:
SPARC‑Independent delivery of nab‑paclitaxel without depleting tumor stroma in patient‑derived pancreatic cancer xenografts.
Mol Cancer Ther 15: 680‑688, 2016.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0) License.