Fukushima Medical University
福島県立医科大学 学術機関リポジトリ
This document is downloaded at: 2021-11-07T23:36:23Z
Title Distant organ injury following unilateral renal ischemia- reperfusion in hypertensive Dahl salt-sensitive rats and the ameliorating effect of rosuvastatin pretreatment( 本文 ) Author(s) 菅野, 真理
Citation
Issue Date 2015-03-24
URL http://ir.fmu.ac.jp/dspace/handle/123456789/629
Rights
This is the pre-peer reviewed version of the following article:
[Nephrology (Carlton). 2018 Nov;23(11):1046-1054], which has been published in final form at
[https://doi.org/10.1111/nep.13169]. This article may be used for non-commercial purposes in accordance with Wiley Terms and Conditions for Use of Self-Archived Versions.
DOI
Text Version ETD
1 Title
Distant organ injury following unilateral renal ischemia-reperfusion in hypertensive Dahl salt-sensitive rats and the ameliorating effect of rosuvastatin pretreatment
高血圧性Dahl食塩感受性ラットにおける片側腎虚血再灌流による遠隔臓器障害およびロスバス タチンによるその保護効果についての検討
Author Makoto Kanno
Department of Nephrology, Hypertension, Diabetology, Endocrinology and Metabolism, Fukushima Medical University School of Medicine, Fukushima, Japan
菅野真理
福島県立医科大学 腎臓高血圧・糖尿病内分泌代謝内科学講座
2 Abstract
Background
Recent limited studies have shown that unilateral renal ischemia-reperfusion (I/R) induces distant organ injury (DOI) with inflammatory changes and oxidative stress. However, the pathological backgrounds of previous study subjects, especially in regards to blood pressure levels, have not been consistent. Statins have anti-inflammatory and antioxidant effects independent of their cholesterol-lowering properties and can protect against post-I/R kidney injury.
We investigated the hypotheses that blood pressure is associated with the pathogenesis of DOI, and that this injury can be ameliorated by rosuvastatin (RO) pretreatment using a rat model of I/R.
Methods
Our study consisted of two phases. In the Phase 1 study, 10-week-old Dahl salt-sensitive rats were fed a low-salt (0.3%) diet for six weeks. These rats were randomly divided into four groups: a sham group, a sham with RO group, an I/R group, and an I/R with RO group. RO (10 mg/kg/day) was administered orally by dissolving it in water starting two weeks before I/R. The rats then underwent unilateral renal I/R for 45 min and subsequent reperfusion for seven days. In the Phase 2 study, 6-week-old Dahl salt-sensitive rats were fed a high-salt (8%) diet for six weeks.
Administration of RO and I/R were performed in the same way as in the Phase 1 study, except that the reperfusion period was three days.
Results
In the Phase 1 study, hypertension was not induced in rats through the feeding period, and no visible histological changes were found in the contralateral kidney and the heart, which suggested the absence of DOI. In the Phase 2 study, all rats developed severe hypertension and showed histological injury in the contralateral kidney, but not in the heart. I/R worsened contralateral kidney
3
injury with histological changes including increases in the glomerular sclerosis index, tubular dilation area, and infiltration of ED-1 positive cells, as well as inducing serological changes including increases in serum creatinine and malondialdehyde levels and a decrease in creatinine clearance. I/R also reduced the protein expression of superoxide dismutase (SOD) in the contralateral kidney. RO pretreatment significantly ameliorated all these changes following I/R.
Conclusions
Unilateral renal I/R induced contralateral kidney injury in Dahl salt-sensitive rats with hypertension, but not in those with normotension. RO pretreatment significantly prevented the down-regulation of SOD in the contralateral kidney after I/R and ameliorated contralateral kidney injury with histological and serological improvements. These results indicated that basic conditions of oxidative stress in individual organs might be involved in the pathogenesis of DOI following I/R, and that the protective effect of RO on DOI might be associated with a decrease in oxidative stress in distant organs via up-regulation of SOD.
Keywords
Acute kidney injury, Distant organ injury, Oxidative stress, Renal ischemia reperfusion, Rosuvastatin, Superoxide dismutase
4 Abbreviations
8-OHdG, 8-hydroxy-2'-deoxyguanosine; AKI, acute kidney injury; BP, blood pressure; CCr, creatinine clearance; CK-MB, creatine kinase-myocardial band; CT-GF, connective tissue growth factor; DOI, distant organ injury; eNOS, endothelial nitric oxide synthase; GADPH, glyceraldehyde 3-phosphate dehydrogenase; HMG-CoA, 3-Hydroxy-3-methylglutaryl-coenzyme A; IL-1β, interleukin-1β; IL-6, interleukin-6; IL-12, interleukin-12; I/R, ischemia-reperfusion; MCP-1, monocyte chemotactic protein-1; MDA, malondialdehyde; NADPH, nicotine-adenine dinucleotide phosphate; NO, nitric oxide; NOS, nitric oxide synthase; PAI-1, plasminogen activator inhibitor-1;
RO, rosuvastatin; ROS, reactive oxygen species, RT-PCR, Real-Time Quantitative Polymerase Chain Reaction; SOD, superoxide dismutase; TGF-β, transforming growth factor-β; TNF-α; tumor necrosis factor-α
5 Introduction
Acute kidney injury (AKI) is a frequent complication in critically ill patients and is associated with increased morbidity and mortality despite the recent widespread availability of renal replacement therapy (1, 2). AKI is commonly triggered by acute renal ischemia-reperfusion (I/R), caused by reduced renal blood flow due to severe hypotension, serious infection, major cardiovascular surgery, and renal transplantation. Post-ischemic AKI seems to be a complication of hypoxia derived from impaired blood supply to local tissues and subsequent reperfusion leading to acute inflammatory changes (3). Reperfusion of ischemic tissue initiates complex cellular events that result in injury and renal cell apoptosis (4). Although it is necessary for the survival of ischemic tissue, reperfusion itself causes additional cellular injury and tissue damage (5). These harmful aspects of renal I/R are not limited to the ischemic kidney itself, but instead spread systemically and trigger inflammation and functional changes in distant organs, including heart, lung, liver, and brain (6-9). Using Dahl salt-sensitive rats, we previously confirmed that unilateral renal I/R also affects the contralateral kidney and the heart with histological changes accompanied by increased infiltration of ED-1 positive cells and overexpression of oxidative stressors (10). However, there have been some studies that have examined the effects of unilateral renal I/R on distant organs (11-14), including the contralateral kidney, but the pathological background of the study animals, especially in regards to blood pressure (BP), has not been consistent, even though high BP is a powerful risk factor for exacerbating organ injury.
Statins, 3-Hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase inhibitors, which are commonly used to lower serum cholesterol levels and are effective for primary and secondary prevention of cardiovascular diseases (15, 16), possess strong anti-inflammatory and anti-oxidative capabilities that are independent of their direct lipid-lowering properties (17, 18).
6
These capabilities can include improvements in endothelial function, decreases in smooth muscle proliferation, vascular inflammation, and antiplatelet actions, as well as effects on other lipids and lipoproteins (19). The pleiotropic effects of statins have been confirmed not only during chronic inflammation, but also during acute inflammation, including I/R injury. There have been several studies in experimental animal models showing that statin pretreatment ameliorates post-I/R kidney injury with serological and histological improvements (3, 20-22). However, it is uncertain whether statins can also protect against distant organ injury following renal I/R.
Based on this background, the present study was undertaken to clarify the following two hypotheses using a hypertensive rat model: First, whether BP is associated with the pathogenesis of distant organ injury following unilateral I/R. Second, whether distant organ injury can be ameliorated by rosuvastatin (RO) pretreatment. We also investigated the possible molecular mechanisms of distant organ injury and the ameliorating effect of RO pretreatment.
7 Material and methods
Animals and study protocols
The present study consisted of two phases. Experimental schema of studies was shown in Figure 1. The Phase 1 study was performed with 10-week-old male Dahl salt-sensitive rats (300-320 g) purchased from Japan SLC, Inc. (Shizuoka, Japan). These rats were randomly allocated to four groups: a sham group, a sham with RO group, an I/R group, and an I/R with RO group (n = 5, each group), and were fed a low-salt (0.3%) diet for six weeks. RO was purchased from LKT Laboratories, Inc. (St. Paul, MN) and was administered orally by dissolving it in tap water starting two weeks before renal I/R. The dosage of RO was adjusted to 10 mg/kg/day as previously reported (23). RO-dissolved water was changed every other day and was delivered by a metallic straw from a closed bottle. All rats were housed in a temperature- and humidity-controlled room with 12 h light/dark cycles. Five weeks later, rats were subjected to unilateral clamping of the left renal pedicle for 45 min using microvascular clips and, thereafter, reperfused. Rats in sham groups were given the same operation, including incisions in the skin and the abdominal wall and exteriorization of the left kidney, but not clamping of the left renal pedicle. During I/R or sham operations, rats were given general anesthesia with inhalation of isoflurane (Intervet, Tokyo, Japan). Seven days after I/R, rats were sacrificed for histology and blood analyses. The Phase 2 study was performed with 6-week-old male Dahl salt-sensitive rats (180-230 g). These rats were allocated to four groups as stated above (n = 11, each group) and fed a high-salt (8%) diet for six weeks. Otherwise, the study protocol was the same as for the Phase 1 study, except the reperfusion period following I/R was three days in the Phase 2 study. All experiments were performed according to the institutional guidelines for the care and use of laboratory animals, and all protocols were approved by the Animal Committee of Fukushima
8 Medical University School of Medicine.
Measurements
During the course of the study, body weight and blood pressure were regularly measured. Blood pressure in conscious rats was measured by the tail-cuff method using a BP-98A blood pressure monitor for mice and rats (Softron Co., Tokyo, Japan). For each time point, five measurements were obtained and averaged for each rat. The volume of drinking water, diet, and urine were measured by housing in individual metabolic cages for 24 h at the start and at the end of the study.
Organ weights of the right kidney (unaffected side) and heart were measured at the end of the study. Blood samples from the aortic artery were collected at the time of killing and immediately centrifuged, and the obtained serum was stored at -20ºC until analyzed. Serum total cholesterol (TC) and high-density lipoprotein cholesterol (HDL-C), serum and urinary creatinine, and urinary albumin were measured conventionally. Serum malondialdehyde (MDA) was measured by the lipid peroxidation assay method with an NWLSS kit (Northwest Life Science Specialties, Vancouver, Canada) following the company's protocol. Urinary 8-hydroxy-2'-deoxyguanosine (8-OHdG) was measured using enzyme-linked immunosorbent assays (JaICA, Shizuoka, Japan).
Urinary isoprostane was measured using enzyme-linked immunosorbent assays (Northwest Life Science Specialties). Serum tumor necrosis factor-α (TNF-α) was measured using enzyme-linked immunosorbent assays (Shibayagi, Gunma, Japan). Serum monocyte chemotactic protein-1 (MCP-1) was measured using enzyme-linked immunosorbent assays (IBL Co., Gunma, Japan).
Creatinine clearance (CCr) was calculated based on serum creatinine, urinary creatinine, urine volume, and body weight using the following formula: CCr = urinary creatinine (mg/dL) × urine volume (mL/kg/min) / serum creatinine (mg/dL) (24).
9 Histology and immunohistochemistry
Right kidneys and hearts for histological examinations were collected at the end of the study.
Kidney and heart sections were stained using the Masson-Trichrome stain for renal injury and Picrosirius-Red stain for renal and cardiac fibrosis. To semiquantify glomerular sclerosis, 50 cortical glomeruli were randomly selected. The severity of each glomerulus was estimated given a score (1, normal or minor mesangial proliferation; 2, moderate mesangial proliferation; 3, focal sclerosis; 4, global sclerosis). Glomerular sclerosis index scores were calculated from the following formula: [(1 × n1)+(2 × n2)+(3 × n3)+(4 × n4)] / 50 (25). To semiquantify tubulointerstitial fibrosis, five areas of renal outer medulla were randomly selected. The percentage of each area that showed sclerofibrotic changes (red area in Picrosirius-Red staining) was measured by Image J software (National Institutes of Health, Bethesda, MD). To semiquantify the tubular dilation area, five areas of renal outer medulla were randomly selected. The percentage of each area that showed dilated change (unstained area following Masson-Trichrome staining) was measured by Image J software. To semiquantify the area of cardiac fibrosis, five areas of heart tissue were randomly selected. The percentage of each area that showed fibrotic changes (red area in Picrosirius-Red staining) was measured by Image J software. For immunohistochemical analysis, kidney and heart tissues were immediately fixed with 12% neutral formalin fluid. Tissue was embedded in paraffin and 2.5-μm-thick sections were cut and mounted on slide glasses. Slides were deparaffinized with xylene and ethanol. Immunohistochemical staining was performed using a monoclonal antibody against ED-1 (LSBio, Seattle, WA). The slides were then incubated overnight at 4ºC. Five areas of renal cortex, renal outer medulla, and heart tissue were randomly selected, and results were analyzed by counting the number of cells labeled positively for ED-1 in
10 each area.
Western blotting
The protein levels of superoxide dismutase 1 (SOD1) and superoxide dismutase 2 (SOD2) in the contralateral kidney and the heart and osteopontin in the contralateral kidney were determined by western blotting. In brief, tissue proteins were separated by sodium dodecylsulfate-polyacrylamide gel electrophoresis (SDS-PAGE) and transferred onto a polyvinylidene difluoride (PVDF) membrane (Immobilon-P, Millipore) using a semi-dry transblot apparatus (Bio-Rad Laboratories Inc., Hercules, CA). The membranes were blocked for 1 h with Tris-buffered saline (TBS) containing 5% non-fat dried milk (Bio-Rad Laboratories Inc.). After washing, the membranes were incubated overnight at 4ºC with the following primary antibodies:
rabbit polyclonal antibody to SOD1 (1:5,000, Abcam, Cambridge, UK), rabbit polyclonal antibody to SOD2 (1:50,000, Abcam), and mouse monoclonal antibody to osteopontin (1:1,000, Santa Cruz Biotechnology, Santa Cruz, CA). Subsequently, the membranes were washed three times with TBS, incubated for 2 h at room temperature with horseradish peroxidase-conjugated secondary antibody (1:10,000), and then washed three times with TBS containing 0.05% Tween 20. The blots were also probed with antibody against β-actin (1:5,000, Cell SignalingTechnology, Inc., Boston, MA) to ensure equal protein loading. The density of each protein band was quantified by densitometry using Image J software.
RNA extraction and real-time quantitative polymerase chain reaction (RT-PCR)
Total RNA samples were extracted from whole kidneys and hearts with TRIzol reagent, and total RNAs were further purified using an RNeasy kit with RNase-free DNase I treatment according to
11
the manufacturer's instructions. Total RNA (1 μg) was reverse-transcribed with an iScript cDNA Synthesis Kit according to the manufacturer’s instructions (Bio-Rad Laboratories, Inc.).
Quantitative real-time PCR was performed with a Bio-Rad system using iQ SYBR Green Supermix (Applied Biosystems, Foster City, CA). Primer sequences were as listed in Table 1. The relative mass of specific RNAs was calculated by the comparative cycle of threshold detection method according to the manufacturer's instructions. Glyceraldehyde 3-phosphate dehydrogenase (GADPH) was used as an internal control. The data were expressed as fold increase vs. sham group.
Statistical analysis
All values are expressed as means ± standard error of the mean (SEM). Statistical comparisons of the groups were performed followed by the independent t-test or one-way analysis of variance (ANOVA). P < 0.05 was considered significant. All analyses were performed using SPSS version 21 software (IBM, Chicago, IL).
12 Results
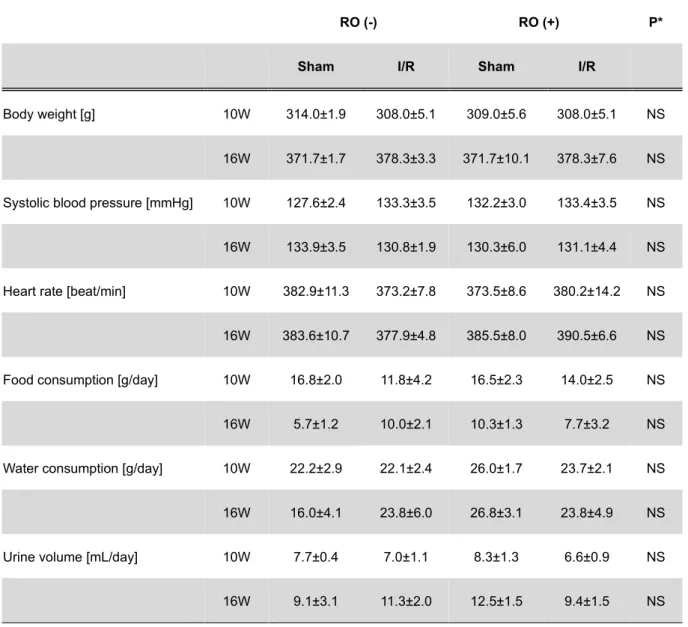
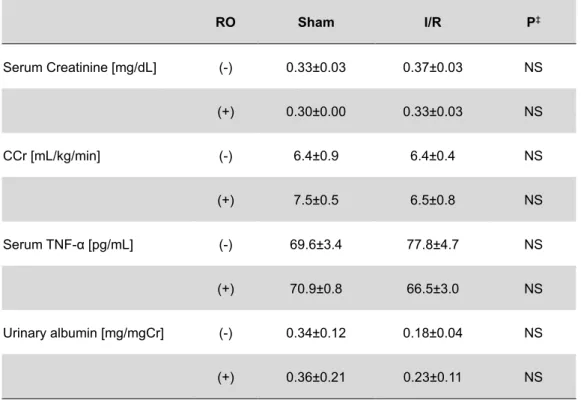
Blood pressure, histology, blood and urine tests, and organ weight in the Phase 1 study A comparison of parameters between groups in the Phase 1 study is shown in Table 2. Mean systolic blood pressure in each group was 125-135 mmHg at baseline and remained nearly unchanged until the end of the study. Unilateral renal I/R induced obvious histological damages including tubular dilation, interstitial edema, and infiltration of ED-1 positive cells in renal cortex and outer medulla of ipsilateral kidneys. However, there were no significant differences between the sham group and I/R group in histological findings in contralateral kidneys or heart (Figure 2a-d), as well as in serum creatinine, CCr, and urinary albumin excretion (Table 3). There were also no significant differences in the organ weights of the contralateral kidney and heart between the sham group and I/R group, or between sham with RO group and I/R with RO group (data not shown).
Blood pressure and organ weight in the Phase 2 study
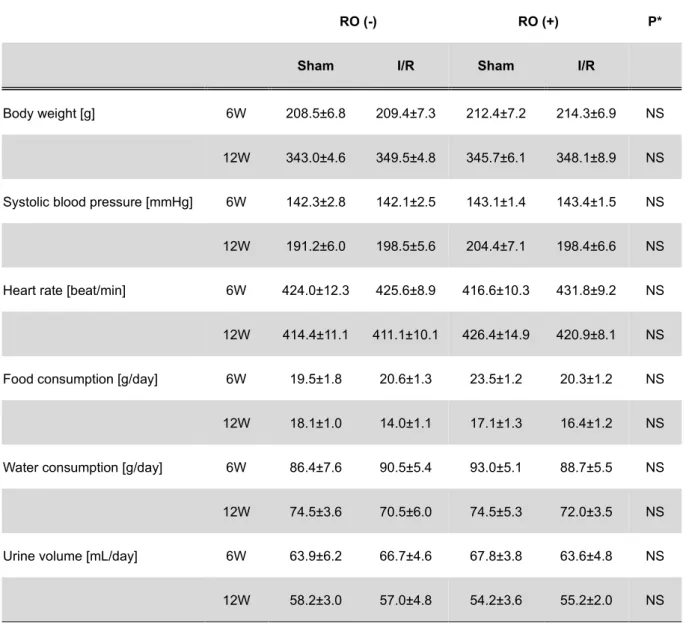
Changes in mean body weight, systolic blood pressure, heart rate, food consumption, water consumption, and urine volume in each group in the Phase 2 study are shown in Table 4. There were no significant differences in these parameters between groups neither at the start nor at the end of the study. Mean systolic blood pressure was elevated from 140-145 mmHg at baseline to 190-205 mmHg at the end of the study. All rats survived with no fatal accidents through the feeding period. The right kidney (contralateral side) / body weight ratio in sham group was 0.55 ± 0.01%/BW and significantly increased to 0.65 ± 0.02%/BW after I/R; this increase was not affected by RO pretreatment (0.63 ± 0.02%/BW). The heart / body weight ratio was not changed after I/R (sham vs. I/R: 0.51 ± 0.01%/BW vs. 0.52 ± 0.01%/BW). However, RO pretreatment significantly decrease the ratio after I/R (0.48 ± 0.01%/BW; P < 0.05) as compared to its counterpart.
13 Blood and urine tests in the Phase 2 study
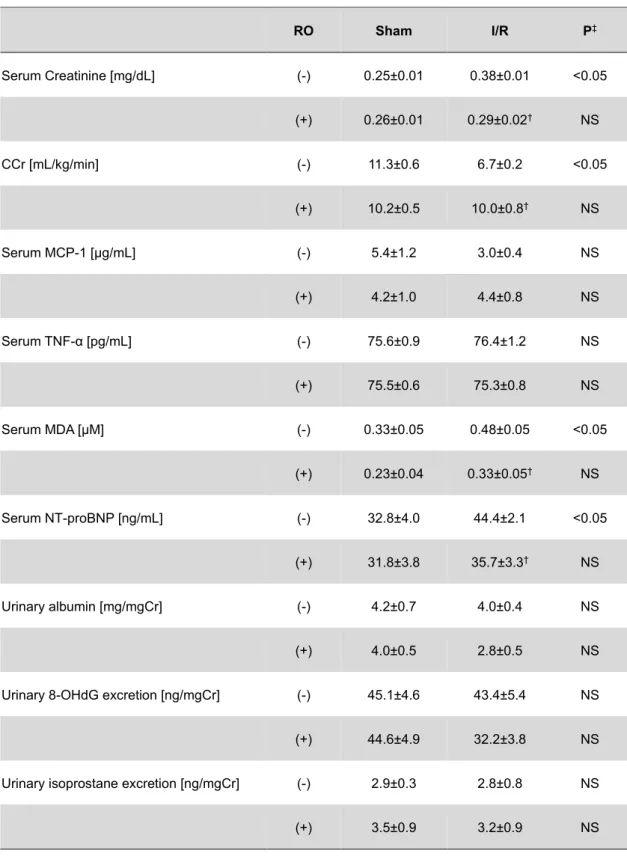
Serum and urinary parameters in each group at three days after I/R are shown in Table 5. There were no statistical differences in serum TC and HDL-C between the sham group and sham with RO group, or between the I/R group and I/R with RO group (data not shown). Serum creatinine levels were significantly increased in the I/R group compared with the sham group (0.38 ± 0.01 mg/dL vs. 0.25 ± 0.01 mg/dL; P < 0.05). RO pretreatment significantly ameliorated the increase in serum creatinine levels after I/R (0.29 ± 0.02 mg/dL; P < 0.05). To substantiate the effects of RO pretreatment on renal function after I/R, we calculated CCr in each rat. CCr in the sham group was 11.3 ± 0.6 mL/kg/min and was reduced to 6.7 ± 0.2 mL/kg/min after I/R; this reduction was suppressed by RO pretreatment (10.0 ± 0.8 mL/kg/min; P < 0.05). Serum MDA levels were significantly higher in the I/R group compared with the sham group (0.48 ± 0.05 μM vs. 0.33 ± 0.05 μM; P < 0.05). RO pretreatment significantly ameliorated the increase in serum MDA levels after I/R (0.33 ± 0.05 mg/dL; P < 0.05). No statistical differences were found in other oxidative stress markers or proinflammatory cytokines in blood or urine samples between the sham group and I/R group, or between the sham with RO group and I/R with RO group.
Histological findings of contralateral kidneys and hearts in the Phase 2 study
Representative histological findings in contralateral kidneys and hearts are presented in Figure 3. Histological comparisons of the contralateral kidneys between groups are shown in Figure 4. As compared to the Phase 1 study, the glomerular sclerosis index and number of ED-1 cells in the renal cortex and outer medulla were significantly higher in all groups. Among groups without RO pretreatment, there were significant increases in the glomerular sclerosis index (sham vs. I/R: 1.45
14
± 0.06 vs. 1.60 ± 0.03; P < 0.05, Figure 4a), tubular dilation area (24.2 ± 0.9% vs. 27.2 ± 0.9% per slice; P < 0.05, Figure 4b), and number of ED-1 cells in renal outer medulla (4.1 ± 0.9 vs. 8.1 ± 1.5 per slice; P < 0.05, Figure 4e), while no differences were found in interstitial fibrosis area (4.8 ± 0.4% vs. 4.2 ± 0.5% per slice, Figure 4c) or number of ED-1 cells in the renal cortex (8.5 ± 2.0 vs.
12.3 ± 2.1 per slice, Figure 4d). In the I/R with RO group, the levels were significantly less for the glomerular sclerosis index (1.44 ± 0.05; P < 0.05, Figure 4a), tubular dilation area (24.1 ± 1.0% per slice; P < 0.05, Figure 4b), and number of ED-1 cells in renal outer medulla (4.2 ± 0.8 per slice; P <
0.05, Figure 4e) as compared to the respective counterpart group. Regarding ipsilateral kidneys, renal I/R triggered significant histological damages including tubular dilation and infiltration of ED-1 cells in renal cortex and outer medulla, as well as in the Phase 1 study. RO pretreatment significantly ameliorated these damages similarly in ipsilateral kidneys (Supplementary Figure 1, 2), as previously reported (3, 22, 26).
Western blotting analysis of contralateral kidneys in the Phase 2 study
Figure 5 shows the protein expressions of SOD1, SOD2, and osteopontin in contralateral kidneys by western blotting. Among groups without RO pretreatment, renal I/R significantly reduced the expression of both SOD1 and SOD2 (39% and 47%, respectively) as compared to the sham group, while these reductions were completely abolished by RO pretreatment. The expression of osteopontin was increased by 18% after renal I/R as compared to the sham group, although this increase was not suppressed by RO pretreatment. Regarding the left kidney (I/R side), the protein expressions of SOD1 and SOD2 (80% and 43%, respectively) were also reduced as compared to the sham group, and the reduction of SOD1 was significantly improved by 16% with RO pretreatment (data not shown).
15
Quantitative RT-PCR analysis of contralateral kidneys in the Phase 2 study
Quantitative RT-PCR analyses of mRNA expression (per GAPDH ratio) in contralateral kidneys are shown in Figure 6. At three days after I/R, there were no significant differences in mRNA levels of SOD1, SOD2, MCP-1, TNF-α, interleukin-6 (IL-6), transforming growth factor-β (TGF-β), connective tissue growth factor (CT-GF), or type 1 collagen between the sham and I/R groups, or between the sham with RO and I/R with RO groups (Figure 6a-h).
Histological findings, western blotting analysis, and quantitative RT-PCR analysis of hearts in the Phase 2 study
Histological comparisons of hearts between groups are shown in Figure 7. Among groups without RO pretreatment, there were no significant differences in cardiac interstitial fibrosis areas (sham vs. I/R: 2.3 ± 0.3% vs. 2.2 ± 0.3% per slice, Figure 7a) or number of ED-1 cells (5.1 ± 1.4 vs.
6.6 ± 1.2 per slice, Figure 7b). Figure 8 shows protein expressions of SOD1 and SOD2 in hearts by western blotting. Among groups without RO pretreatment, renal I/R significantly reduced the expressions of SOD1 and SOD2 (50% and 41%, respectively) as compared to the sham group;
these reductions were not improved by RO pretreatment. Quantitative RT-PCR analyses of mRNA expression (per GAPDH ratio) in hearts are shown in Figure 9. At three days after I/R, there were significant increases in the mRNA levels of TGF-β (1.3-fold, Figure 9f) and type 1 collagen (2.1-fold, Figure 9h) as compared to the sham group. Additionally, RO pretreatment ameliorated the increases in TGF-β mRNA expression after I/R. There were no significant differences in the mRNA levels of SOD1, SOD2, MCP-1, TNF-α, IL-6, or CT-GF between the sham and I/R groups, or between the sham with RO and I/R with RO groups.
16 Discussion
Summary of the results
In the present study, we applied an animal model of DOI using hypertensive Dahl salt-sensitive rats with unilateral renal I/R and examined whether DOI could be ameliorated by RO pretreatment.
In the Phase 1 study, 10-week-old rats were fed a low-salt (0.3%) diet for six weeks and were administered RO-dissolved water from two weeks before I/R. Seven days after I/R, rats were sacrificed for histology and blood analyses. Systolic blood pressure of rats in the Phase 1 study was 125-135 mmHg at the start and remained unchanged until the end of the study. Unilateral renal I/R triggered obvious histological damages in ipsilateral kidneys, whereas no visible changes were found in contralateral kidneys or hearts, which indicated the absence of DOI. In the Phase 2 study, 6-week-old rats were fed a high-salt (8%) diet for six weeks and were sacrificed three days after I/R. Systolic blood pressure of rats in the Phase 2 study was elevated up to 190-205 mmHg at the time of I/R. Unilateral renal I/R induced serious histological changes in ipsilateral kidneys as well as in the Phase 1 study. Additionally, histological examination of contralateral kidneys showed significant increases in the glomerular sclerosis index, tubular dilation area, and infiltration of ED-1 labeled cells in the outer medulla in the I/R group as compared to the sham group; these increases were not detected in hearts. RO pretreatment suppressed these changes following I/R in contralateral kidneys. Blood and urine tests showed increases in serum creatinine levels and MDA levels and decreases in CCr in the I/R group, which were significantly ameliorated by RO pretreatment. Western blotting analysis demonstrated that the protein expressions of SOD1 and SOD2 in contralateral kidneys were decreased, and were also ameliorated by RO pretreatment.
Unilateral renal I/R and distant organ injury in contralateral kidneys
17
The protocol of the Phase 1 study was determined with reference to a previous study (10) in which the systolic blood pressure of rats was 160-165 mmHg at the time of I/R. However, no visible histological injury was triggered in contralateral kidneys in normotensive rats. In the Phase 2 study, hypertension was induced by a high-salt diet, and histological examinations showed significant increases in the glomerular sclerosis index, tubular dilation area, and ED-1 positive cells in the outer medulla in contralateral kidneys. Western blotting analysis demonstrated a decrease in the protein expressions of SOD1 and SOD2 in contralateral kidneys. RT-PCR analysis showed a decrease in the mRNA expressions of SOD1 and SOD2, but with no significance. Moreover, serum MDA levels were increased after I/R, which together with the above suggests enhanced oxidative stress with impaired anti-oxidative capacity in contralateral kidneys.
Furthermore, I/R increased the expression of osteopontin in contralateral kidneys. Osteopontin is a proinflammatory cytokine that promotes cell recruitment to inflammatory sites and mediates cell activation and cytokine production (27). The increase in osteopontin might reflect enhanced inflammation in contralateral kidneys. Meanwhile, there were no significant differences between the sham group and I/R group with respect to the mRNA expressions of proinflammatory cytokines such as MCP-1, IL-6, and TNF-α. Meldrum et al. performed unilateral renal ischemia in male Sprague-Dawley rats for 1 h and reported that the expression of TNF-α in contralateral kidneys continuously increased from the time of reperfusion to 4 h later and reached a peak 2 h later (11).
Sung et al. performed unilateral renal ischemia under similar operating conditions and reported that the mRNA expression of MCP-1 increased only in the ipsilateral kidney, but not in the contralateral kidney regardless of the time-course (28). Our RT-PCR results were from samples taken at three days after I/R. Taken together, we surmise that the mRNA expression of TNF-α was increased after I/R but was already decreased at the time of sacrifice. Regarding interstitial fibrosis,
18
no differences were found between the sham group and I/R group, which is consistent with the results of a previous report (10). There were also no differences in the mRNA expressions of TGF-β, CT-GF, and type 1 collagen in contralateral kidneys. Basile et al. performed unilateral renal I/R in male Sprague-Dawley rats for 35 min and confirmed that interstitial cells in contralateral kidneys were significantly increased at 33 days after I/R (12). These findings suggest that interstitial fibrosis is induced even in the contralateral kidney following unilateral renal I/R, though it takes seven days or more for the changes to become visible.
Since Meldrum et al. first reported on the subject in 2002, there have been few reports concerning distant effects on the contralateral kidney by unilateral renal I/R, because most studies have featured contralateral nephrectomy simultaneous with unilateral renal I/R. Kato et al.
performed unilateral renal I/R in male Sprague-Dawley rats for 45 min and reported that histological examination in contralateral kidneys showed no obvious changes in 7-week-old rats, but there were significant increases in 40-week-old rats in glomerular sclerosis, interstitial fibrosis, and infiltration of ED-1 positive cells (14). On the other hand, other studies have reported that no histological changes were found in contralateral kidneys in pigs subjected to unilateral renal I/R for 120 min (29) or in mice at one day, one week, or three weeks after unilateral renal I/R (30). These previous studies, though limited, suggest that age at the time of I/R and the species of experimental animal might be involved in the pathogenesis of contralateral kidney injury. Our results show for the first time that hypertension might be a possible factor in contralateral kidney injury. In comparison with the sham group in the Phase 1 study, the glomerular sclerosis index, ED-1 positive cells in the outer medulla, and urinary albumin excretion were increased in rats in the Phase 2 study. This finding suggests the existence of hypertensive renal damage at the time of I/R. Since DOI was not triggered in young rats or normotensive rats, existing inflammation,
19
including an increase in infiltration of ED-1 positive cells, might be involved in inducing DOI following unilateral renal I/R.
Unilateral renal I/R and distant organ injury in the heart
Regarding the heart, there were no significant differences between the sham group and I/R group in the number of ED-1 positive cells and interstitial fibrosis areas both in the Phase 1 study and the Phase 2 study. However, following I/R, the mRNA expressions of TGF-β and type 1 collagen were significantly increased and CT-GF also showed increased expression, although not to a significant extent. Overexpression of TGF-β leads to abnormal accumulation of extracellular matrix proteins and promotes tissue fibrosis (31). CT-GF is a downstream peptide of TGF-β and is highly involved in the production of extracellular matrix proteins by TGF-β (32). There have been two reports in which histological examination at seven days after renal I/R showed an increase in infiltration of ED-1 positive cells and interstitial fibrosis, even in the heart (10, 14). Our RT-PCR results suggest that cardiac fibrosis was already promoted at three days after I/R. Taken together, histological changes might become apparent over time. Western blotting analysis demonstrated a decrease in the expression of SOD1 and SOD2 in the heart, which suggested enhanced oxidative stress with impaired antioxidative capacity in the heart as well as in the contralateral kidney, but these decreases were not correlated with histological changes.
Distant effects of renal I/R on the heart were first reported by Kelly et al. in 2003 (6). They performed bilateral renal ischemia in mice for 15-45 min and subsequent reperfusion for 48 h, and found an increase in the mRNA expression of proinflammatory cytokines including TNF-α, IL-1, and IL-6 in the heart. They also confirmed an increase in cardiomyocyte apoptosis, cardiac dysfunction by ultrasonography, and pulmonary congestion after renal I/R. In another study,
20
Sprague-Dawley rats subjected to bilateral renal ischemia for 45 min and subsequent reperfusion for 3 h showed cardiac dysfunction by ultrasonography and increased serum CK-MB and troponin T (33). Our results at three days after I/R showed no differences between the sham group and I/R group in the mRNA expressions of TNF-α and IL-6 in the heart. This might be due to the differences between in bilateral I/R and unilateral I/R, as well as the reperfusion period. The differences between bilateral renal I/R and unilateral renal I/R have been examined in a previous study using a mouse model (7). Bilateral renal I/R induces significant increases in serum IL-6, IL-1β, and IL-12 2-4 h after I/R coupled with abnormal histological changes, including alveolar septal edema and infiltration of neutrophils in the pulmonary interstitium, whereas none of these changes are triggered by unilateral renal I/R. These results indicate that unilateral renal I/R had less of an effect on serum cytokines and distant organs as compared to bilateral renal I/R.
Mechanisms of distant organ injury following I/R
Several previous studies have shown that renal I/R decreases the protein expression of SOD and increases the production of MDA in post-ischemic kidneys (34, 35). Our study demonstrated that unilateral renal I/R decreased the expression of both SOD1 and SOD2 even in the contralateral kidney and the heart. SOD1 is cytosolic, copper/zinc-containing SOD (Cu/Zn-SOD);
SOD2 is a mitochondrial manganese SOD (Mn-SOD). SODs are major antioxidant enzymes and catalytically enhance the normal dismutation of superoxide, which is one of major reactive oxygen species (ROS). By decreasing the intracellular steady state levels of superoxide, SODs can successfully inhibit the formation of a potent oxidant, peroxynitrite (36), which results in protecting cells from oxidative stress injury. MDA is one of several low-molecular weight end products as well as a reliable estimator of lipid peroxidation (37). In our study, the serum MDA level was
21
significantly increased after I/R. Taken together, these findings indicate that unilateral renal I/R induces the down-regulation of SODs in contralateral kidneys, which results in the overproduction of superoxide, leading to enhanced oxidative stress and increased production of MDA. In other words, down-regulation of SODs in individual distant organs might be involved in the pathogenesis of DOI. Jang et al. reported that unilateral renal I/R in mice for 30 min induces a significant increase in the formation of superoxide and the infiltration of inflammatory cells in contralateral kidneys, and that these changes are significantly suppressed by administration of a mimetic of SOD, Mn (III) Tetrakis (1-methyl-4-pyridyl) porphyrin (13). Our presumption is consistent with their results. However, the precise mechanisms by which renal I/R down-regulate SODs in post-ischemic kidneys or in distant organs remain unknown. During I/R injury, reperfused tissues generate a great deal of free radicals and ROS, which lead to cell apoptosis and tissue injury (38, 39). Impaired renal tubules generate various cytokines and chemokines and trigger the activation of inflammatory cells, including leukocytes and macrophages, which generate further proinflammatory cytokines (40, 41). Presumably, these various impairments in the post-ischemic kidneys spread to distant sites through the bloodstream. However, as our results in the Phase 1 and Phase 2 studies showed, DOI was not always induced by unilateral renal I/R. This difference indicates that some factors in distant organs may be involved in the pathogenesis of DOI. Our results demonstrated that hypertension at the time of I/R is a possible factor. There is a report showing that hypertensive Dahl-salt sensitive rats fed with a high-salt diet show decreased expressions of SOD1 and SOD2 in renal medulla and increased oxidative stress as compared to Dahl salt-resistant rats (42). According to our results, in all rats of the Phase 2 study, oxidative stress in contralateral kidneys was already increased at the time of I/R. In addition, aging is a well-known risk factor for oxidative stress and is a possible factor for the induction of DOI as
22
pointed out above. Taken together, the basic condition of oxidative stress in individual distant organs might be associated with the pathogenesis of DOI following I/R.
Pleiotropic effects of statins against DOI
As mentioned above, several previous studies have demonstrated that statin pretreatment ameliorates post-I/R kidney injury with serological and histological improvements. In our experiments, RO pretreatment attenuated an elevation in serum MDA levels and histological injury even in the contralateral kidney with an increase in the expression of SODs. Although the mechanisms by which statins up-regulate SODs are not understood, recent studies have revealed the mechanisms of the organ protective actions of statins. Statins reduce cholesterol synthesis by inhibiting HMG-CoA reductase, which results in inhibiting the synthesis of downstream products such as mevalonate, farnesyl-pyrophosphate, and geranylgeranyl-pyrophosphate (Figure 10). A decrease in mevalonate activates the PI3k-Akt pathway and promotes the synthesis of nitric oxide (NO) and angiogenesis through an increase in the expression and activation of endothelial nitric oxide synthase (eNOS) (43, 44). Farnesyl-pyrophosphate and geranylgeranyl-pyrophosphate are known to play an important role in the post-translational modification of G proteins such as the Ras and Rho families (45). Rho inactivation by statins prevents thrombus formation through an increase in eNOS function and a decrease in gene expression of plasminogen activator inhibitor-1 (PAI-1) (46). Inhibition of Rac activates eNOS function and decreases the formation of superoxide and oxidative stress through the inactivation of nicotine-adenine dinucleotide phosphate (NADPH) oxidase (47). Sharyo et al. reported that the renoprotective effect of pravastatin is diminished by the co-administration of mevalonate in a model of bilateral renal I/R in mice (48). They also reported that treatment with mevalonate alone worsens the degree of renal I/R injury, and that
23
treatment with L-744832, an isoprenylation inhibitor, significantly ameliorates renal dysfunction after I/R. These results indicate that the renoprotective effects of statins are mediated by the mevalonate-isoprenoid pathway. Based on our results and previous studies, we theorize some possible molecular mechanisms by which RO affects DOI (Figure 11). Namely, the formation of superoxide in the post-I/R kidney is suppressed via the mevalonate-isoprenoid pathway. We presume that up-regulation of SODs by RO is probably associated with this pathway and which leads to the decrease in oxidative stress including MDA. Additionally, RO activates NOS function and increases NO, which induces vasodilative changes and protects vascular endothelium. As a result, tissue injury in the post-I/R kidney is diminished, which also suppresses the spread of proinflammatory cytokines and inflammatory cells to distant organs, resulting in the indirect protection of distant organs. Moreover, RO acts in the same way even in distant organs and directly protects them through a decrease in oxidative stress and vasodilation by NO.
Clinical implications of this study
Unilateral renal I/R reflects clinical conditions such as renal transplantation, renal aneurysmectomy, or partial nephrectomy. Whether statin pretreatment for renal transplant recipients is effective has been discussed in many clinical studies and is still a controversial issue (49). Our results indicate that hypertension at the time of I/R might be involved in spreading post-I/R kidney impairments to the contralateral kidney. In addition, since contralateral kidney injury was ameliorated by RO pretreatment, this may indicate that RO pretreatment is especially effective for renal transplant recipients with hypertension. Needless to say, urine and blood tests are convenient and useful markers for estimating renal function. However, these markers are expressed as the total of right and left kidney function and are unsuitable for estimating split renal
24
function. In addition, since renal transplantation is sometimes accompanied by rejection, the function of kidneys is rarely separately assessed even when developing post-operative AKI.
Recent studies have demonstrated that AKI is not only a local metabolic disorder, but also a systemic inflammatory disease that causes various side effects. When treating AKI, we must pay attention to the possibility of DOI along with the injured kidney. Our results indicate that RO is a possible preventative drug for DOI.
25 Conclusions
In conclusion, we confirmed that unilateral renal I/R induced contralateral kidney injury in Dahl salt-sensitive rats with hypertension, but not in those with normotension. In impaired contralateral kidneys, the protein expressions of SOD1 and SOD2 were significantly down-regulated. RO pretreatment prevented this down-regulation and ameliorated contralateral kidney injury with histological and serological improvements. These results indicate that the basic condition of oxidative stress in individual organs might be involved in the pathogenesis of DOI following I/R. In addition, the protective effect of RO on DOI might be associated with a decrease in oxidative stress in individual distant organs via up-regulation of SODs. Several studies have shown that DOI is triggered even in lung, brain, liver, or intestine, in addition to the contralateral kidney and heart.
Further research is needed to determine whether statin pretreatment can ameliorate these multiple organ disruptions following AKI.
26 Acknowledgements
I express my sincere gratitude to my supervisors, Professor Masaaki Nakayama and Professor Tsuyoshi Watanabe, for providing me this precious study opportunity. I especially express my deepest appreciation to my supervisor, Dr. Yoshimitsu Hayashi, for his elaborate guidance, considerable encouragement, and invaluable discussions that made my research a great achievement and my post-graduate life unforgettable. I am very grateful to Dr. Hiroyuki Terawaki, Dr. Koichi Asahi, and Wan-Jun Zhu for their valuable cooperation in my experiments. Finally, I would like to express appreciation for Yuko Ohashi and Atsuko Hashimoto for their excellent technical assistance.
27 References
1. Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, et al. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA : the journal of the American Medical Association. 2005;294(7):813-8.
2. Ympa YP, Sakr Y, Reinhart K, Vincent JL. Has mortality from acute renal failure decreased? A systematic review of the literature. The American journal of medicine. 2005;118(8):827-32.
3. Gueler F, Rong S, Park JK, Fiebeler A, Menne J, Elger M, et al. Postischemic acute renal failure is reduced by short-term statin treatment in a rat model. Journal of the American Society of Nephrology : JASN. 2002;13(9):2288-98.
4. Lieberthal W, Levine JS. Mechanisms of apoptosis and its potential role in renal tubular epithelial cell injury. The American journal of physiology. 1996;271(3 Pt 2):F477-88.
5. Weight SC, Bell PR, Nicholson ML. Renal ischaemia--reperfusion injury. The British journal of surgery. 1996;83(2):162-70.
6. Kelly KJ. Distant effects of experimental renal ischemia/reperfusion injury. Journal of the American Society of Nephrology : JASN. 2003;14(6):1549-58.
7. Hoke TS, Douglas IS, Klein CL, He Z, Fang W, Thurman JM, et al. Acute renal failure after bilateral nephrectomy is associated with cytokine-mediated pulmonary injury. Journal of the American Society of Nephrology : JASN. 2007;18(1):155-64.
8. Golab F, Kadkhodaee M, Zahmatkesh M, Hedayati M, Arab H, Schuster R, et al. Ischemic and non-ischemic acute kidney injury cause hepatic damage. Kidney international. 2009;75(8):783-92.
9. Liu M, Liang Y, Chigurupati S, Lathia JD, Pletnikov M, Sun Z, et al. Acute kidney injury leads to inflammation and functional changes in the brain. Journal of the American Society of Nephrology : JASN. 2008;19(7):1360-70.
28
10. Zhu WJ, Nakayama M, Mori T, Nakayama K, Katoh J, Murata Y, et al. Intake of water with high levels of dissolved hydrogen (H2) suppresses ischemia-induced cardio-renal injury in Dahl salt-sensitive rats. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2011;26(7):2112-8.
11. Meldrum KK, Meldrum DR, Meng X, Ao L, Harken AH. TNF-alpha-dependent bilateral renal injury is induced by unilateral renal ischemia-reperfusion. American journal of physiology Heart and circulatory physiology. 2002;282(2):H540-6.
12. Basile DP, Leonard EC, Tonade D, Friedrich JL, Goenka S. Distinct effects on long-term function of injured and contralateral kidneys following unilateral renal ischemia-reperfusion. American journal of physiology Renal physiology. 2012;302(5):F625-35.
13. Jang HS, Kim JI, Kim J, Na YK, Park JW, Park KM. Bone marrow derived cells and reactive oxygen species in hypertrophy of contralateral kidney of transient unilateral renal ischemia-induced mouse. Free radical research. 2012;46(7):903-11.
14. Kato J, Nakayama M, Zhu WJ, Yokoo T, Ito S. Ischemia/reperfusion of unilateral kidney exaggerates aging-induced damage to the heart and contralateral kidney. Nephron Experimental nephrology. 2014;126(4):183-90.
15. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet. 1994;344(8934):1383-9.
16. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. The New England journal of medicine. 1998;339(19):1349-57.
17. Influence of pravastatin and plasma lipids on clinical events in the West of Scotland Coronary Prevention Study (WOSCOPS). Circulation. 1998;97(15):1440-5.
29
18. Kwak B, Mulhaupt F, Myit S, Mach F. Statins as a newly recognized type of immunomodulator.
Nature medicine. 2000;6(12):1399-402.
19. Davignon J. Pleiotropic effects of pitavastatin. British journal of clinical pharmacology.
2012;73(4):518-35.
20. Zarbock A, Schmolke M, Spieker T, Jurk K, Van Aken H, Singbartl K. Acute uremia but not renal inflammation attenuates aseptic acute lung injury: a critical role for uremic neutrophils. Journal of the American Society of Nephrology : JASN. 2006;17(11):3124-31.
21. Shepherd J, Kastelein JJ, Bittner V, Deedwania P, Breazna A, Dobson S, et al. Effect of intensive lipid lowering with atorvastatin on renal function in patients with coronary heart disease: the Treating to New Targets (TNT) study. Clinical journal of the American Society of Nephrology : CJASN.
2007;2(6):1131-9.
22. Haylor JL, Harris KP, Nicholson ML, Waller HL, Huang Q, Yang B. Atorvastatin improving renal ischemia reperfusion injury via direct inhibition of active caspase-3 in rats. Experimental biology and medicine. 2011;236(6):755-63.
23. Manucha W, Kurban F, Mazzei L, Benardon ME, Bocanegra V, Tosi MR, et al. eNOS/Hsp70 interaction on rosuvastatin cytoprotective effect in neonatal obstructive nephropathy. European journal of pharmacology. 2011;650(2-3):487-95.
24. Xue W, Lei J, Li X, Zhang R. Trigonella foenum graecum seed extract protects kidney function and morphology in diabetic rats via its antioxidant activity. Nutrition research. 2011;31(7):555-62.
25. Raij L, Azar S, Keane W. Mesangial immune injury, hypertension, and progressive glomerular damage in Dahl rats. Kidney international. 1984;26(2):137-43.
26. Wu K, Lei W, Tian J, Li H. Atorvastatin treatment attenuates renal injury in an experimental model of ischemia-reperfusion in rats. BMC nephrology. 2014;15:14.
30
27. Wang KX, Denhardt DT. Osteopontin: role in immune regulation and stress responses.
Cytokine & growth factor reviews. 2008;19(5-6):333-45.
28. Sung FL, Zhu TY, Au-Yeung KK, Siow YL, O K. Enhanced MCP-1 expression during ischemia/reperfusion injury is mediated by oxidative stress and NF-kappaB. Kidney international.
2002;62(4):1160-70.
29. Malagrino PA, Venturini G, Yogi PS, Dariolli R, Padilha K, Kiers B, et al. Catheter-based induction of renal ischemia/reperfusion in swine: description of an experimental model. Physiological reports. 2014;2(9).
30. Zager RA, Johnson AC, Becker K. Acute unilateral ischemic renal injury induces progressive renal inflammation, lipid accumulation, histone modification, and "end-stage" kidney disease. American journal of physiology Renal physiology. 2011;301(6):F1334-45.
31. Lijnen PJ, Petrov VV, Fagard RH. Induction of cardiac fibrosis by transforming growth factor-beta(1). Molecular genetics and metabolism. 2000;71(1-2):418-35.
32. Gore-Hyer E, Shegogue D, Markiewicz M, Lo S, Hazen-Martin D, Greene EL, et al. TGF-beta and CTGF have overlapping and distinct fibrogenic effects on human renal cells. American journal of physiology Renal physiology. 2002;283(4):F707-16.
33. Chen TH, Yang YC, Wang JC, Wang JJ. Curcumin treatment protects against renal ischemia and reperfusion injury-induced cardiac dysfunction and myocardial injury. Transplantation proceedings.
2013;45(10):3546-9.
34. Beytur A, Binbay M, Sarihan ME, Parlakpinar H, Polat A, Gunaydin MO, et al.
Dose-dependent protective effect of ivabradine against ischemia-reperfusion-induced renal injury in rats. Kidney & blood pressure research. 2012;35(2):114-9.
35. Tasdemir C, Tasdemir S, Vardi N, Ates B, Parlakpinar H, Kati B, et al. Protective effect of
31
infliximab on ischemia/reperfusion-induced damage in rat kidney. Renal failure. 2012;34(9):1144-9.
36. Kalyanaraman B. Teaching the basics of redox biology to medical and graduate students:
Oxidants, antioxidants and disease mechanisms. Redox biology. 2013;1(1):244-57.
37. Janero DR. Malondialdehyde and thiobarbituric acid-reactivity as diagnostic indices of lipid peroxidation and peroxidative tissue injury. Free radical biology & medicine. 1990;9(6):515-40.
38. Baud L, Ardaillou R. Involvement of reactive oxygen species in kidney damage. British medical bulletin. 1993;49(3):621-9.
39. Weinberg JM. The cell biology of ischemic renal injury. Kidney international.
1991;39(3):476-500.
40. Jang HR, Ko GJ, Wasowska BA, Rabb H. The interaction between ischemia-reperfusion and immune responses in the kidney. Journal of molecular medicine. 2009;87(9):859-64.
41. Jang HR, Rabb H. The innate immune response in ischemic acute kidney injury. Clinical immunology. 2009;130(1):41-50.
42. Meng S, Roberts LJ, 2nd, Cason GW, Curry TS, Manning RD, Jr. Superoxide dismutase and oxidative stress in Dahl salt-sensitive and -resistant rats. American journal of physiology Regulatory, integrative and comparative physiology. 2002;283(3):R732-8.
43. Fulton D, Gratton JP, McCabe TJ, Fontana J, Fujio Y, Walsh K, et al. Regulation of endothelium-derived nitric oxide production by the protein kinase Akt. Nature.
1999;399(6736):597-601.
44. Dimmeler S, Fleming I, Fisslthaler B, Hermann C, Busse R, Zeiher AM. Activation of nitric oxide synthase in endothelial cells by Akt-dependent phosphorylation. Nature. 1999;399(6736):601-5.
45. Palinski W, Tsimikas S. Immunomodulatory effects of statins: mechanisms and potential impact on arteriosclerosis. Journal of the American Society of Nephrology : JASN. 2002;13(6):1673-81.
32
46. Markle RA, Han J, Summers BD, Yokoyama T, Hajjar KA, Hajjar DP, et al. Pitavastatin alters the expression of thrombotic and fibrinolytic proteins in human vascular cells. Journal of cellular biochemistry. 2003;90(1):23-32.
47. Wagner AH, Kohler T, Ruckschloss U, Just I, Hecker M. Improvement of nitric oxide-dependent vasodilatation by HMG-CoA reductase inhibitors through attenuation of endothelial superoxide anion formation. Arteriosclerosis, thrombosis, and vascular biology. 2000;20(1):61-9.
48. Sharyo S, Yokota-Ikeda N, Mori M, Kumagai K, Uchida K, Ito K, et al. Pravastatin improves renal ischemia-reperfusion injury by inhibiting the mevalonate pathway. Kidney international.
2008;74(5):577-84.
49. Palmer SC, Navaneethan SD, Craig JC, Perkovic V, Johnson DW, Nigwekar SU, et al. HMG CoA reductase inhibitors (statins) for kidney transplant recipients. The Cochrane database of systematic reviews. 2014;1:CD005019.
33 Figure legends
Figure 1. Experimental schema of the Phase 1 and Phase 2 study.
The Phase 1 study was performed with 10-week-old male Dahl salt-sensitive rats fed a low-salt (0.3%) diet. RO (10 mg/kg/day) was administered orally by dissolving it in tap water starting two weeks before renal I/R. Five weeks later, rats in I/R groups were subjected to unilateral clamping of the left renal pedicle for 45 min and thereafter, reperfused. Seven days after I/R, all rats were sacrificed for histology and blood analyses. The Phase 2 study was performed with 6-week-old male Dahl salt-sensitive rats fed a high-salt (8%) diet for six weeks. Otherwise, the study protocol was the same as for the Phase 1 study, except the reperfusion period following I/R was three days in the Phase 2 study.
Figure 2. Semiquantitative measurements of histological findings in contralateral kidneys and hearts in the Phase 1 study.
(a) Glomerular sclerosis index for the contralateral kidneys of sham rats (□RO (-), ■RO (+); n=5, each group) and I/R rats (□RO (-), ■RO (+); n=5, each group). (b) Number of ED-1 positive cells per slice in renal cortexes of contralateral kidneys of sham rats and I/R rats. (c) Number of ED-1 positive cells per slice in renal outer medullae in contralateral kidneys of sham rats and I/R rats. (d) Number of ED-1 positive cells per slice in hearts of sham rats and I/R rats.
Figure 3. Representative histological findings of kidneys (contralateral side) and hearts three days after unilateral renal I/R in the Phase 2 study.
Glomerular sclerosis and mesangial proliferation in an I/R-affected rat without (a) or with (b) RO pretreatment. Tubular dilation and interstitial fibrosis in renal outer medulla of an I/R-affected rat
34
without (c) or with (d) RO pretreatment. ED-1 staining in renal cortex of an I/R-affected rat without (e) or with (f) RO pretreatment. ED-1 staining in renal outer medulla of an I/R-affected rat without (g) or with (h) RO pretreatment. Interstitial fibrosis in the heart of an I/R-affected rat without (i) or with (j) RO pretreatment. ED-1 staining in the heart of an I/R-affected rat without (k) or with (l) RO pretreatment.
Figure 4. Semiquantitative measurements of histological findings in contralateral kidneys in the Phase 2 study.
(a) Glomerular sclerosis indexes of contralateral kidneys of sham rats (□RO (-), ■RO (+); n=11, each group) and I/R rats (□RO (-), ■RO (+); n=11, each group). (b) Tubular dilation area per field (%) in contralateral kidneys of sham rats and I/R rats. (c) Tubulointerstitial fibrosis area per field (%) in contralateral kidneys of sham rats and I/R rats. (d) Number of ED-1 positive cells per slice in renal cortexes of contralateral kidneys in sham rats and I/R rats. (e) Number of ED-1 positive cells per slice in renal outer medullae in contralateral kidneys of sham rats and I/R rats.
Figure 5. Protein expressions of SOD1, SOD2, and osteopontin determined by western blotting in contralateral kidneys in the Phase 2 study.
The bar graph shows the densitometric analysis of western blotting normalized to the corresponding β-actin signal in sham rats (□RO (-), n=10; ■RO (+), n=8), and I/R rats (□RO (-), n=11; ■RO (+), n=10). *P < 0.05 vs. sham; †P < 0.05 vs. RO (-).
Figure 6. Quantitative RT-PCR analyses of mRNA gene expressions in contralateral kidneys in the Phase 2 study.
35
(a) SOD1 expression in contralateral kidneys of sham rats (□RO (-), n=10; ■RO (+), n=11) and I/R rats (□RO (-), n=10; ■RO (+), n=11). (b) SOD2 expression in contralateral kidneys of sham rats and I/R rats. (c) MCP-1 expression in contralateral kidneys of sham rats and I/R rats. (d) TNF-α expression in contralateral kidneys of sham rats and I/R rats. (e) IL-6 expression in contralateral kidneys of sham rats and I/R rats. (f) TGF-β expression in contralateral kidneys of sham rats and I/R rats. (g) CT-GF expression in contralateral kidneys of sham rats and I/R rats. (f) Type 1 collagen expression in contralateral kidneys of sham rats and I/R rats.*P < 0.05 vs. sham;
†P < 0.05 vs. RO (-).
Figure 7. Semiquantitative measurement of histological findings of hearts in the Phase 2 study.
(a) Interstitial fibrosis area per field (%) in hearts of sham rats (□RO (-), ■RO (+); n=11, each group) and I/R rats (□RO (-), ■RO (+); n=11, each group). (b) Number of ED-1-labeled cells per slice in hearts of sham rats and I/R rats.
Figure 8. Protein expressions of SOD1 and SOD2 determined by western blotting in hearts in the Phase 2 study.
The bar graph shows the densitometric analysis of the western blotting normalized to the corresponding β-actin signal in sham rats (□RO (-), n=11; ■RO (+), n=9), and I/R rats (□RO (-), n=11; ■RO (+), n=10). *P < 0.05 vs. sham.
Figure 9. Quantitative RT-PCR analyses of mRNA gene expressions in hearts in the Phase 2 study.
36
(a) SOD1 expression in hearts of sham rats (□RO (-), n=10; ■RO (+), n=11) and I/R rats (□RO (-), n=9; ■RO (+), n=9). (b) SOD2 expression in hearts of sham rats and I/R rats. (c) MCP-1 expression in hearts of sham rats and I/R rats. (d) TNF-α expression in hearts of sham rats and I/R rats. (e) IL-6 expression in hearts of sham rats and I/R rats. (f) TGF-β expression in hearts of sham rats and I/R rats. (g) CT-GF expression in hearts of sham rats and I/R rats. (f) Type 1 collagen expression in hearts of sham rats and I/R rats.*P < 0.05 vs. sham; †P < 0.05 vs. RO (-).
Figure 10. Previously-reported mechanisms of pleiotropic effects of statins.
Statin-induced decreases in HMG-CoA reductase activity reduce downstream protein prenylation and have the potential to reduce oxidative stress and to improve vascular function through multiple pathways.
Figure 11. Expected molecular mechanisms of RO pretreatment against distant organ injury.
RO pretreatment inactivates NADPH oxidase and increases SOD expression in the post-I/R kidney, which leads to decreasing the formation of superoxide and results in reducing oxidative stress including MDA. Additionally, RO activates NOS function and increases NO, which induces vasodilative changes and protects vascular endothelium. As a result, tissue injury in the post-I/R kidney is ameliorated by RO pretreatment. This amelioration also leads to suppressing the spread of proinflammatory cytokines and inflammatory cells to distant organs, resulting in the indirect protection of distant organs. Moreover, RO acts in the same way even in distant organs and directly protects them through a decrease in oxidative stress and vasodilation by NO.
37
Supplementary Figure 1. Representative histological findings of I/R kidneys (ipsilateral side) three days after unilateral renal I/R in the Phase 2 study.
Tubular dilation in renal outer medulla of an I/R-affected rat without (a) or with (b) RO pretreatment.
ED-1 staining in renal cortex of an I/R-affected rat without (c) or with (d) RO pretreatment. ED-1 staining in renal outer medulla of an I/R-affected rat without (e) or with (f) RO pretreatment.
Supplementary Figure 2. Semiquantitative measurements of histological findings in I/R kidneys (ipsilateral side) in the Phase 2 study.
(a) Glomerular sclerosis indexes of ipsilateral kidneys of sham rats (□RO (-), ■RO (+); n=11, each group) and I/R rats (□RO (-), ■RO (+); n=11, each group). (b) Tubular dilation area per field (%) in ipsilateral kidneys of sham rats and I/R rats. (c) Tubulointerstitial fibrosis area per field (%) in ipsilateral kidneys of sham rats and I/R rats. (d) Number of ED-1 positive cells per slice in renal cortexes of ipsilateral kidneys in sham rats and I/R rats. (e) Number of ED-1 positive cells per slice in renal outer medulla in ipsilateral kidneys of sham rats and I/R rats.
38
39
Table 2. Comparison of parameters between groups at the start or at the end of the Phase 1 study.
RO (-) RO (+) P*
Sham I/R Sham I/R
Body weight [g] 10W 314.0±1.9 308.0±5.1 309.0±5.6 308.0±5.1 NS
16W 371.7±1.7 378.3±3.3 371.7±10.1 378.3±7.6 NS Systolic blood pressure [mmHg] 10W 127.6±2.4 133.3±3.5 132.2±3.0 133.4±3.5 NS 16W 133.9±3.5 130.8±1.9 130.3±6.0 131.1±4.4 NS Heart rate [beat/min] 10W 382.9±11.3 373.2±7.8 373.5±8.6 380.2±14.2 NS 16W 383.6±10.7 377.9±4.8 385.5±8.0 390.5±6.6 NS Food consumption [g/day] 10W 16.8±2.0 11.8±4.2 16.5±2.3 14.0±2.5 NS
16W 5.7±1.2 10.0±2.1 10.3±1.3 7.7±3.2 NS
Water consumption [g/day] 10W 22.2±2.9 22.1±2.4 26.0±1.7 23.7±2.1 NS 16W 16.0±4.1 23.8±6.0 26.8±3.1 23.8±4.9 NS
Urine volume [mL/day] 10W 7.7±0.4 7.0±1.1 8.3±1.3 6.6±0.9 NS
16W 9.1±3.1 11.3±2.0 12.5±1.5 9.4±1.5 NS
Values are expressed as means ± SEM. n=5, each group. RO, rosuvastatin; NS, no significance.*One-way ANOVA.
40
Table 3. Comparison of parameters between rats with or without RO in the Phase 1 study.
RO Sham I/R P‡
Serum Creatinine [mg/dL] (-) 0.33±0.03 0.37±0.03 NS
(+) 0.30±0.00 0.33±0.03 NS
CCr [mL/kg/min] (-) 6.4±0.9 6.4±0.4 NS
(+) 7.5±0.5 6.5±0.8 NS
Serum TNF-α [pg/mL] (-) 69.6±3.4 77.8±4.7 NS
(+) 70.9±0.8 66.5±3.0 NS
Urinary albumin [mg/mgCr] (-) 0.34±0.12 0.18±0.04 NS
(+) 0.36±0.21 0.23±0.11 NS
Values are expressed as means ± SEM. n=3, each group. RO, rosuvastatin; NS, no significance.
‡Unpaired t test.
41
Table 4. Comparison of parameters between groups at the start or at the end of the Phase 2 study.
RO (-) RO (+) P*
Sham I/R Sham I/R
Body weight [g] 6W 208.5±6.8 209.4±7.3 212.4±7.2 214.3±6.9 NS
12W 343.0±4.6 349.5±4.8 345.7±6.1 348.1±8.9 NS Systolic blood pressure [mmHg] 6W 142.3±2.8 142.1±2.5 143.1±1.4 143.4±1.5 NS 12W 191.2±6.0 198.5±5.6 204.4±7.1 198.4±6.6 NS Heart rate [beat/min] 6W 424.0±12.3 425.6±8.9 416.6±10.3 431.8±9.2 NS 12W 414.4±11.1 411.1±10.1 426.4±14.9 420.9±8.1 NS Food consumption [g/day] 6W 19.5±1.8 20.6±1.3 23.5±1.2 20.3±1.2 NS 12W 18.1±1.0 14.0±1.1 17.1±1.3 16.4±1.2 NS Water consumption [g/day] 6W 86.4±7.6 90.5±5.4 93.0±5.1 88.7±5.5 NS 12W 74.5±3.6 70.5±6.0 74.5±5.3 72.0±3.5 NS Urine volume [mL/day] 6W 63.9±6.2 66.7±4.6 67.8±3.8 63.6±4.8 NS 12W 58.2±3.0 57.0±4.8 54.2±3.6 55.2±2.0 NS Values are expressed as means ± SEM. n=11, each group. RO, rosuvastatin; NS, no significance. *One-way ANOVA.