Fukushima Medical University
This document is downloaded at: 2021-11-08T00:38:33Z
Title
Tumor mutation burden and immunological, genomic, and clinicopathological factors as biomarkers for checkpoint inhibitor treatment of patients with non-small-cell lung cancer(
本文 ) Author(s) 尾崎, 有紀
Citation
Issue Date 2020-09-30
URL http://ir.fmu.ac.jp/dspace/handle/123456789/1334
Rights
Fulltext: © 2019, Springer-Verlag GmbH Germany. This is a post-peer-review, pre-copyedit version of an article published in [Cancer Immunology, Immunotherapy]. The final
authenticated version is available online at:
https://doi.org/10.1007/s00262-019-02446-1 DOI
Text Version ETD
Tumor mutation burden and immunological, genomic, and clinicopathological factors as biomarkers for checkpoint inhibitor treatment of patients with non-small-cell lung cancer
Yuki Ozaki
Department of Chest Surgery, Fukushima Medical University, Fukushima, Japan
Abstract
Cancer treatment using immune checkpoint inhibitors is widely used, although biomarkers predictive of response
are not well-established. However, both the expression of programmed cell death ligand 1 (PD-L1) and the tumor
mutation burden (TMB) hold promise as such biomarkers for immune checkpoint inhibitors; however, its
characteristics and clinical and immunological impacts have not been fully analyzed. We therefore evaluated the
clinical and immunological parameters related to TMB to identify potential new biomarkers. We enrolled 92 patients
with non-small-cell lung cancer who underwent surgery at Fukushima Medical University Hospital from 2013 to
2016. TMB of individual tumors was calculated by whole-exome sequencing analysis. Major cancer-related gene
mutations were evaluated using panel sequencing. Expression of PD-L1 and abundance of tumor-infiltrating
lymphocytes were evaluated by immunohistochemistry using surgical samples. The median TMB value was 60.
TMB was significantly higher in men, current or former smokers, and in patients with squamous cell carcinoma,
tumor size ≥2.8 cm, wild-type EGFR, TP53 gene mutation-positive status, and cyclin-dependent kinase-inhibitor
gene 2A mutation-positive status. According to multivariate analysis, TMB was significantly associated with EGFR
gene mutation-negative status (p=0.0111) and TP53 gene mutation-positive status (p=0.0425). If TMB is identified
as a robust biomarker for immune checkpoint inhibitor administration, analysis of TP53 and EGFR mutations may
provide a relatively rapid and easy proxy for predicting TMB.
Abbreviations
MSI microsatellite instability
NGS next-generation sequencing
NSCLC non-small-cell lung cancer
PD-1 programmed cell death 1
PD-L1 programmed death ligand 1
TIL tumor-infiltrating lymphocyte
TMB tumor mutation burden
TP53 tumor protein 53
Introduction
Developments in immune checkpoint inhibitors have progressed rapidly, and they are now major pillars of cancer
treatment, along with cytotoxic anticancer drugs and molecular-targeted therapeutic agents. Several immune
checkpoint inhibitors, including programmed cell death 1 (PD-1) inhibitors and programmed-death ligand 1 (PD-
L1) inhibitors, were recently approved by the US Food and Drug Administration for the treatment of advanced non-
small-cell lung cancer (NSCLC). PD-L1 is the primary PD-1 ligand and is upregulated in many solid tumors. PD-
L1 is believed to inhibit cytokine production and the cytolytic activity of PD-1-positive tumor-infiltrating
lymphocytes (TILs). Most prospective trials found that the treatment was more effective in PD-L1-positive
compared with PD-L1-negative patients. However, the PD-L1-negative group still demonstrated response rates of
around 10%, indicating that PD-L1 was not a perfect predictive biomarker for response (1-8). More definite
biomarkers are therefore needed, and many studies are currently addressing this issue.
Several parameters other than PD-L1 expression (TILs, microsatellite instability (MSI), and tumor mutation burden
(TMB)) have been considered as potential predictive biomarkers of immune checkpoint inhibitor response. Pre-
existing CD8+TILs located in the tumor and invasive margin might predict response to therapy in patients with
melanoma (9). Although MSI is often used as a biomarker in colorectal cancer and Lynch syndrome, high MSI was
only detected in 0.8% of 480 patients with pulmonary adenocarcinoma using a sensitive mononucleotide marker
panel (10). MSI is currently used as a companion diagnostic technique in various tumors; however the rate of MSI
in NSCLC is thought to be very low, indicating the need for more accurate and clinically useful biomarkers. Several
solid tumors, including NSCLC, have TMB levels >10 somatic mutations per megabase of coding DNA, which is
sufficient to produce neoantigens that can be recognized by effector-T cells (11). Among these potential parameters
(PD-L1, CD8+TILs, MSI, and TMB), the current study focused on the use of TMB to predict the efficacy of immune
checkpoint inhibitors. A higher nonsynonymous TMB was correlated with the clinical efficacy of pembrolizumab
in one study (12), and although several other reports have been published, detailed information on TMB remains
limited. In a biomarker analysis of TMB conducted as a subgroup analysis of the Check-mate 026 trial, which
compared first-line nivolumab with chemotherapy in patients with PD-L1-positive NSCLC, the response rate
among patients with high TMB was higher in the nivolumab group than in the chemotherapy group (13).
Furthermore, patients with both high TMB and ≥50% PD-L1 expression had higher response rates than those with
only one or neither of these factors. Most TMB studies have evaluated the association between TMB and response
to immune checkpoint inhibitors, while the associated clinical features have not been well-documented. In this study,
we therefore evaluated the correlations between TMB and clinical and immunological parameters in patients with
NSCLC, with the aim of identifying more convenient factors to use as surrogate markers for TMB.
Materials and Methods Patients and characteristics
We enrolled a total of 92 patients who underwent surgery at the Hospital of Fukushima Medical University from
2013–2016. No patients received chemotherapy or immunotherapy before surgery. Disease staging was evaluated
according to the current International Union Against Cancer TNM classification, 7
thedition. Paired tumor and
normal tissues dissected from surgical specimens were collected from all 92 patients for whole-exome sequencing
and immunohistochemistry.
Whole-exome sequencing
The 92 pairs of matched tumor and non-tumor samples (184 samples in total) were subjected to whole-exome next-
generation sequencing (NGS) using an Ion AmpliSeq™ Exome technology and Ion Proton™ platform (Thermo
Fisher Scientific, Waltham, MA, USA), according to the manufacturer’s instructions. Briefly, exome libraries were
prepared using an Ion AmpliSeq Exome RDY Kit (Thermo Fisher Scientific) with 100 ng of genomic DNA
extracted from the paired tumor and adjacent non-tumor tissue (or corresponding peripheral blood sample) for target
amplification by PCR, as described in the manufacturer’s protocol. The obtained libraries were optimized using an
Ion Library Equalizer kit (Thermo Fisher Scientific) and then sequenced using an Ion Proton or Ion S5XL platform
(Thermo Fisher Scientific). The sequenced reads were aligned to the reference genome build hg19 and GRCh37,
and converted into binary alignment map files using Ion Torrent Suite software (Thermo Fisher Scientific). The
average of Q20 bases and mean coverage depth of the 184 samples were 6.44 Gbp and 123×, respectively, and
90.4% of target bases had a coverage of 20×. Sequence variants found only in tumors were called using Ion
Reporter™ 5.0 (Thermo Fisher Scientific) and CLC Genomics Workbench 8.0 software (Qiagen, Hilden, Germany),
and the number of nonsynonymous coding variants was counted. The resulting value was designated as the TMB.
Tumor variants within the hotspot regions for the following genes were detected using the Ion Ampliseq™ Colon
and Lung Cancer Panel v2 (Thermo Fisher Scientific) and Ion Personal Genome Machine™ (PGM™ platform
(Thermo Fisher Scientific): EGFR, TP53, KRAS, ERBB2, BRAF, CTNNB1, PTEN, cyclin-dependent kinase-
inhibitor 2A (CDKN2A), and PIK3CA. Briefly, 10 ng of genomic DNA extracted from the 92 pairs of matched
tumor and non-tumor samples was used to prepare a DNA library, as described in the manufacturer’s instructions.
Mutation hotspots in CDKN2A were also sequenced using the Ion Ampliseq™ Cancer Hotspot Panel v2 (Thermo
Fisher Scientific) using Ion PGM™, according to the manufacturer’s instructions.
Immunohistochemistry
Fresh-frozen paraffin-embedded tissue sections of 4-µm thickness were stained for PD-L1 as described previously
(14). Sections were also stained for CD8 to evaluate CD8+TILs, and p53 to evaluate p53 protein expression. The
sections were dewaxed in xylene and dehydrated through an alcohol gradient. Endogenous peroxidase activity was
quenched by 20-min incubation with a 0.3% (v/v) solution of hydrogen peroxidase (Wako Pure Chemical Industries
Ltd., Osaka, Japan) in 100% methanol. The sections were then incubated in 5% dried skimmed milk in phosphate-
buffered saline for 30 min at room temperature, and incubated overnight at 4°C with primary monoclonal antibodies
to PD-L1 (1:100; clone SP142; Ventana, Tucson, AZ, USA), CD8 (1:50; clone C8/144B; DAKO, Santa Clara, CA,
USA), or p53 (1:500; Bp53-12, anti-human p53 protein monoclonal antibody, Santa Cruz Biotechnology, TX, USA)
using the avidin-biotin complex method. The sections were washed several times in phosphate-buffered saline after
each step and counterstained with Mayer’s hematoxylin (Muto Pure Chemicals, Co., Ltd., Tokyo, Japan),
dehydrated through an alcohol gradient, and mounted on glass slides.
PD-L1-positivity was determined as >1% tumor area infiltrated by PD-L1-positive immune cells (tumor cell: TC1
or immune cell: IC1) for the SP142 (15). CD8+TILs were classified as low (<30%), intermediate (30%–60%), or
high (>60%) according to the positive rate of CD8 staining (16). p53-positivity was defined by nuclear staining as
0 (absence of p53- positive cells), 1 (low p53, <5%), 2 (intermediate p53, 5%–50%), and 3 (high p53, >5%) (17).
Statistical analyses
The associations between TMB and clinical/immunological parameters were evaluated by univariate analysis using
the Mann–Whitney test. Multivariate analysis was performed by multiple linear regression analysis. We estimated
the correlation between TP53 mutation and p53 protein expression using Pearson’s correlation coefficient.
Multivariate analysis was conducted using SPSS version 23 (IBM, Armonk, NY, USA) and Graph Pad Prism
version 7 (GraphPad Software, CA, USA) was used for all other statistical analyses.
Results
Patients and characteristics
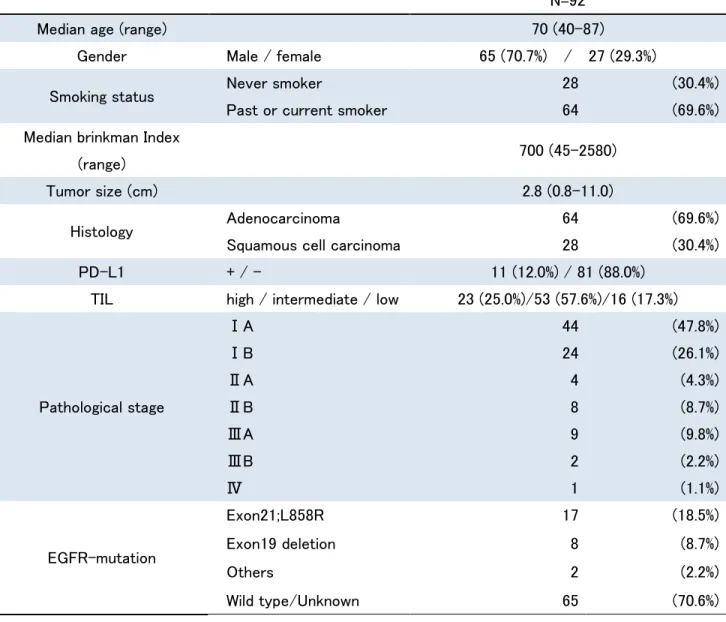
A total of 92 patients were enrolled and their characteristics are summarized in Supplementary Table 1. The median
age was 70 years, 70.7% of patients were male, and 69.6% of all patients were current or former smokers (median
Brinkman Index 700, range 45–2580). Sixty-four patients (69.6%) were diagnosed with adenocarcinoma based on
surgical specimens. In terms of pathological staging, 73.9% of all patients were stage I. Lung cancer recurrence was
seen in 22 patients (24.2%) except one patient with stage IV adenocarcinoma diagnosed at surgery. Overall 14.1%
of patients died.
TMB analysis using NGS
We evaluated the TMB in surgical samples from the 92 patients by NGS. The median TMB was 60 somatic
mutations per megabase of coding DNA (range 10–502) (Fig. 1). The most common type of mutation was missense
mutations. The clinical/immunological parameters and mutations in cancer-associated genes obtained by panel
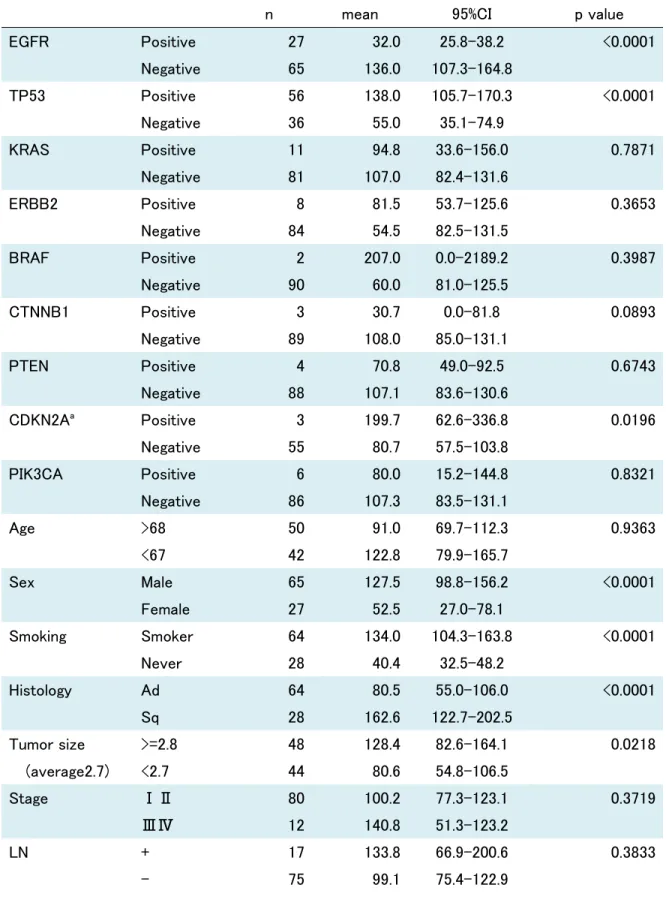
sequencing are shown in Fig. 1, and correlations between these parameters and TMB obtained by univariate analysis
are shown in Table 1. Regarding the clinical parameters, male sex (p<0.0001), current or former smoking status
(p<0.0001), squamous cell carcinoma (p<0.0001), and tumor size ≥2.8 cm (p=0.0218) were significantly correlated
with higher TMB. In terms of cancer-associated mutations, wild-type EGFR (p<0.0001), TP53 mutation positive
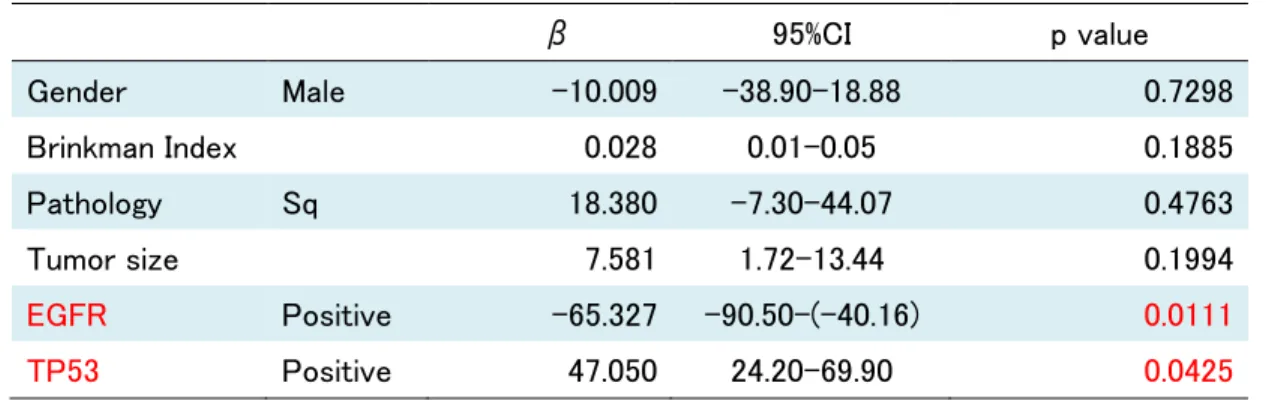
(p<0.0001), and CDKN2A mutation positive (p=0.0196) were significantly related to TMB. EGFR mutation-
negative and TP53 mutation-positive status significantly contributed to TMB based on multivariate analysis
(p=0.0111 and p=0.0425, respectively) (Supplementary Table 2). We derived the following equation to predict TMB
level: TMB = 55.461 − 10.009 × (male: 1, female: 0) + 0.028 × Brinkman Index + 18.380 × (squamous cell
carcinoma: 1, adenocarcinoma: 0) + 7.581 × tumor size (cm) − 65.327 × (EGFR+: 1, EGFR−: 0) + 47.050 − (TP53+:
1, TP53−: 0). The coefficient of determination (R
2) was 0.260, indicating a weak correlation.
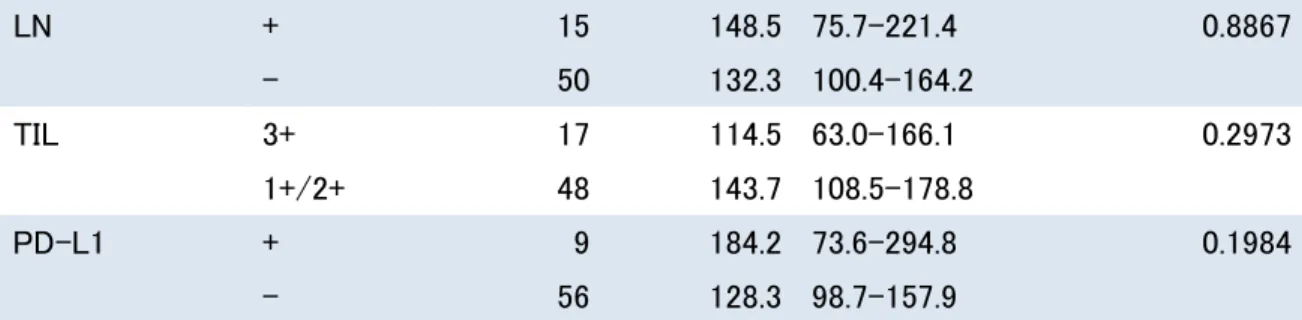
Among the 65 EGFR-mutation-negative patients (Supplementary Table 3), male sex (p=0.0296), current or former
smoker (p=0.0022), squamous cell carcinoma (p=0.0034), and TP53 alteration (p=0.0006) were correlated with
TMB according to univariate analysis, and a significant association between TMB and TP53 was identified by
multivariate analysis (Supplementary Tables 4 and 5). There was no association between TMB and CD8+TILs
(p=0.2973) or TMB and PD-L1 (p=0.1984) (Supplementary Fig. 1).
Immunohistochemistry
Immunohistochemistry revealed that 12.7% of the tumors expressed PD-L1, but there was no correlation between
PD-L1 and TMB. High CD8+TILs were detected in 23 (25.0%), intermediate in 53 (57.6%), and low in 16 (17.4%),
with no correlation between CD8+TILs and TMB. There was also no significant correlation between PD-L1 and
CD8+TILs. p53 protein expression in tumors was strongly related to TP53 mutation status measured by
immunochemical staining and whole-exome sequencing, respectively (r=0.6599, p<0.0001) (Supplementary Fig.
2).
Discussion
The results of the current study indicated that higher TMB was strongly associated with both TP53 mutation-
positive and EGFR mutation-negative status, while TMB was also significantly correlated with TP53 mutation-
positive status among EGFR mutation-negative patients. Notably, we found a lack of correlation between TMB and
CD8+TILs, and between TMB and PD-L1 expression. All these parameters have been reported to play essential
roles in immuno-oncology (18-20), and might also be predictive biomarkers for the efficacy of immune checkpoint
inhibitors. The current results suggest that TMB, CD8+TILs, and PD-L1 are independent factors.
PD-L1 is currently the only clinical biomarker predicting a reliable effect of the anti-PD-1 antibody
pembrolizumab for first-line therapy; however, even PD-L1-negative patients showed better survival outcomes
with pembrolizumab compared with chemotherapy (12.6 versus 8.9 months, respectively) (21). Anti-PD-L1
inhibitors are also effective in approximately 10% of PD-L1-negative patients. To explain why PD-L1-negative
patients benefit from immune checkpoint inhibitors, it is necessary to evaluate complex immunological
microenvironments (20) and comprehensively consider the clinical events related to TMB and TILs.
The current study found that TMB was not correlated with either PD-L1 or CD8+TILs. Several previous studies
also found no association between TMB and PD-L1 expression (13, 18). Although several previous studies have
analyzed the relationship between TMB and TILs (22, 23), to the best of our knowledge, none have reported on the
relationship between TMB and CD8+TILs. We also showed that PD-L1 expression in tumors was not correlated
with the amount of CD8+TILs, indicating that TMB, PD-L1, and CD8+TILs may independently influence the effect
of immune checkpoint inhibitors. However, immune-cell PD-L1 expression and infiltration into tumors might
correlate with nonsynonymous mutations and tumor number in patients with large-cell neuroendocrine carcinoma
(24). Multiple factors must thus be considered in relation to biomarkers of immune checkpoint inhibitors. Blank et
al. and Karasaki et al. previously suggested the concept of ‘cancer immunograms’ representing several
immunological factors as a spider plot, which might be helpful for guiding personalized immunotherapy (25, 26).
Human cancers with higher TMB have been considered suitable for immunotherapy, because a higher TMB may
be associated with more neoantigens (11, 27). Patients with higher TMB levels are more likely to benefit from
immunotherapy using immune checkpoint inhibitors (12, 14, 28). It should be noted that the TMB in the current
study was lower than in previous studies. This may be because we only counted nonsynonymous variants in tumor
tissues compared with normal lung tissue, and there were therefore fewer nonsynonymous variants because adjacent
lung tissue, rather than peripheral blood, was used for germline comparison. A high TMB can enrich neoantigen-
specific T cells, which attack tumors and subsequently lead to successful treatment outcomes (11). However, there
is currently no evidence to support the ability of TMB alone to predict the efficacy of immune checkpoint inhibitors,
and although both high TMB and high PD-L1 expression are known to predict the effectiveness of anti-PD-1/PD-
L1 inhibitors (13, 18), neither marker alone is sufficiently accurate. Both TMB and PD-L1 are tumor characteristics,
thus highlighting the importance of patient immunological status. It might thus be necessary to analyze both tumor-
specific parameters and the general conditions of patients to predict the benefits of immune checkpoint inhibitors.
Neoantigen-specific T cells mobilized by various gene mutations play a major role in tumor immunity, indicating
the importance of the presence of TILs and T-cell activation. Regarding the classification of the tumor
microenvironment, Teng et al. proposed four categories based on PD-L1 status and the amount of TILs (16).
Furthermore, although the correlation between PD-L1 expression and TILs has been investigated in NSCLC, the
results were controversial (24, 29, 30). Immune-cell infiltration appears to be related to nonsynonymous mutations
in the tumor (30), but studies showing a correlation between TMB and TILs are lacking. Unlike melanoma, it is
difficult to investigate TILs in patients with advanced or recurrent NSCLC because of difficulties in obtaining
sufficient tissue samples. Although we analyzed TILs in surgical specimens in the current study, it was difficult to
predict how many lymphocytes infiltrated the tumor before administering immune checkpoint inhibitors based on
smaller sample volumes such as bronchoscopic biopsies.
The following results were also derived from the current whole-exome sequencing. Genes related to the mismatch
repair system were examined to identify candidate genes determining TMB. However, we detected no somatically-
altered variants in the MLH1, MSH2, MSH6, and PMS2 genes in any of the 92 cases. Regarding other mismatch
repair system gene groups, somatically altered variants were only detected in one or two cases per gene (data not
shown). The rare detection of MSI in lung cancer was similar to previous reports (10, 31). In addition, among the
genes with many detected variants, such as those for squamous cell carcinoma, it was difficult to relate these results
to the TMB (data not shown).
Whole-exome sequencing is becoming widely used in major research institutions, and genetic analysis is thus
becoming more common (32). Targeted panel sequences focusing on cancer-related genes are also now available.
Targeted panel sequencing analysis could provide a surrogate marker for TMB (33, 34), and may be easier to
introduce for clinical use. Furthermore, the cost of using whole-exome sequencing to determine TMB is about five-
to ten-fold that of using Cancer Hotspot Panel sequencing to determine TP53 and EGFR. However, it may be
difficult to introduce panel sequencing for large numbers of patients worldwide (35). Predicting TMB by analyzing
specific gene alterations such as TP53 may represent a useful alternative approach. TP53 is a well-known major
regulator and repairer of genomic damage, and may thus also affect the TMB. However, our results suggested that
EGFR mutation, unlike TP53 mutation, was not associated with a high mutation load. Fast growth and division do
not necessarily produce many genetic mutations. Driver mutations, such as EGFR gene mutations, are known to be
a strong oncogenic phenomenon, while situations without driver mutations may require more gene alterations to be
oncogenic. The rates of cancer cell proliferation and division do not seem to depend on the presence of driver
mutations or the diversity of other gene mutations. However, further studies are needed to clarify this essential
oncologic issue.
The p53 protein is encoded by the TP53 gene, and TP53 gene mutation increases the expression of p53.
Overexpression of p53 protein in tumors without lymph node metastasis is an independent adverse prognostic factor
in patients with NSCLC, with 5-year survival rates of 74.1% and 37.5% in p53-negative and p53-positive node-
negative patients, respectively (p=0.022) (36). p53 protein expression is thought to increase in line with cancer
growth and progression (17). Both TP53 mutations and TMB tend to increase with tumor growth, as supported by
the current correlation between TP53 mutation and TMB. Although this correlation was revealed by univariate
analysis in our study, TMB was significantly higher in larger tumors (diameter ≥2.8 cm), indicating that TMB and
TP53 reflected tumor growth. We have used the term ‘growth’ rather than ‘progression’, because there is no
correlation between stage and TMB, and TMB and TP53 are thought to be affected by local tumor growth rather
than progression.
In conclusion, TMB may be associated with aberrations in the tumor suppressor gene TP53. Given that TMB is
considered as a powerful potential biomarker for immune checkpoint inhibitors, it is possible that TP53 may
contribute to predicting the benefit of immune checkpoint inhibitors. However, the current study did not demonstrate
an association between TP53 and clinical outcome in patients using immune checkpoint inhibitors. Nevertheless, if
TMB is recognized as a robust biomarker of response to immune checkpoint inhibitors, it is possible that analyzing
TP53 and EGFR mutations may provide a rapid and easy proxy for predicting TMB. Although TMB was poorly
correlated with TILs and PD-L1, future biomarkers involving combinations of several factors are likely to become
more important in the future. Further studies are necessary to confirm our results and to assess the value of TP53 as
a predictive biomarker of response to immune checkpoint inhibitors in patients with NSCLC.
Author contributions
Yuki Ozaki and Hiroyuki Suzuki designed the study. Yuki Ozaki wrote the initial draft of the manuscript. Satoshi
Muto, Daisuke Tanaka, Hideaki Nanamiya, Jun-ichi Imai, Takao Isogai, and Shinya Watanabe contributed to
analysis and interpretation of data, and assisted in the preparation of the manuscript. Satoshi Muto, Hironori Takagi,
Masayuki Watanabe, Takuya Inoue, Mitsuro Fukuhara, Takumi Yamaura, Naoyuki Okabe, Yuki Matsumura, Takeo
Hasegawa, Jun Ohsugi, Mika Hoshino, and Yutaka Shio contributed to data collection and interpretation, and
critically reviewed the manuscript. All authors approved the final version of the manuscript, and agree to be
accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of
the work are appropriately investigated and resolved.
Acknowledgements
We thank Ms. Kikuta, Ms. Otomo, and Ms. Otsuki for excellent technical support for this study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit
sectors.
Compliance with ethical standards Conflicts of interest
The authors declare that they have no conflict of interest.
Ethical approval and ethical standards
This study was approved by the Institutional Ethics Committee at Fukushima Medical University (No. 2538).
Whole-exome sequencing by next-generation sequencing was performed in accordance with the Ethical Guidelines
for Human Genome and Genetic Analysis Research.
Informed consent
Patients with lung cancer provided written informed consent for the use (including the use for NGS) of tissue
specimens and clinical data for research prior to undergoing pulmonary resection at the Department of Chest
Surgery of Fukushima Medical University.
Figure legends
Fig. 1 TMB and clinical/immunological parameters. Bar chart showing TMB for each patient, with bars in descending order of TMB. The most common mutation type was missense mutations. The patients’ clinical features
are described immediately underneath the bar, and gene variants according to panel sequence analysis are described
in the bottom panel. Colored cells on the left indicate the state or positive mutation, and tumor diameter ≥2.8 cm
TMB: tumor mutation burden, Sq: squamous cell carcinoma, LN: lymph node, TIL: tumor-infiltrating lymphocyte,
PD-L1: programmed cell-death ligand 1, IHC: immunohistochemical staining, TP53; tumor protein 53, KRAS; v-
Ki-ras2 Kirsten rat sarcoma viral oncogene homolog, ERBB2; human epidermal growth factor receptor 2, BRAF;
v-raf murine sarcoma viral oncogene homolog B1, CTNNB1; catenin beta-1, PTEN; phosphatase and tensin
homolog deleted from chromosome 10, CDKN2A: cyclin-dependent kinase-inhibitor gene 2A, PIK3CA;
phosphoinositide-3-kinase, catalytic alpha polypeptide
References
1. Carbognin L, Pilotto S, Milella M et al. (2015) Differential Activity of Nivolumab, Pembrolizumab and
MPDL3280A according to the Tumor Expression of Programmed Death-Ligand-1 (PD-L1): Sensitivity Analysis of
Trials in Melanoma, Lung and Genitourinary Cancers. PloS one. 10: e0130142. doi: 10.1371/journal.pone.0130142
2. Herbst RS, Soria JC, Kowanetz M et al. (2014) Predictive correlates of response to the anti-PD-L1
antibody MPDL3280A in cancer patients. Nature. 515: 563-7. doi: 10.1038/nature14011
3. Gettinger SN, Horn L, Gandhi L et al. (2015) Overall Survival and Long-Term Safety of Nivolumab (Anti-
Programmed Death 1 Antibody, BMS-936558, ONO-4538) in Patients With Previously Treated Advanced Non-
Small-Cell Lung Cancer. Journal of clinical oncology : official journal of the American Society of Clinical Oncology.
33: 2004-12. doi: 10.1200/JCO.2014.58.3708
4. Rizvi NA, Garon EB, Patnaik A et al. (2014) Safety and clinical activity of MK-3475 as initial therapy in
patients with advanced non-small cell lung cancer (NSCLC). J. Clin. Oncol. 32: 8007-. doi:
10.1200/jco.2014.32.15_suppl.8007
5. Rizvi NA, Shepherd FA, Antonia SJ et al. (2014) First-Line Monotherapy With Nivolumab (Anti-PD-1;
BMS-936558, ONO-4538) in Advanced Non-Small Cell Lung Cancer (NSCLC): Safety, Efficacy, and Correlation
of Outcomes With PD-L1 Status: Metastatic Non-Small Cell Lung Cancer. International Journal of Radiation
Oncology • Biology • Physics. 90: S31. doi: 10.1016/j.ijrobp.2014.08.204
6. Antonia SJ, Gettinger S, Goldman J et al. (2014) Safety and Efficacy of First-Line Nivolumab (Anti-PD-
1; BMS-936558, ONO-4538) and Ipilimumab in Non-Small Cell Lung Cancer (NSCLC): Metastatic Non-Small
Cell Lung Cancer. International Journal of Radiation Oncology • Biology • Physics. 90: S32-S3. doi:
10.1016/j.ijrobp.2014.08.207
7. Garon EB, Rizvi NA, Hui R et al. (2015) Pembrolizumab for the treatment of non-small-cell lung cancer.
The New England journal of medicine. 372: 2018-28. doi: 10.1056/NEJMoa1501824
8. Rizvi NA, Mazieres J, Planchard D et al. (2015) Activity and safety of nivolumab, an anti-PD-1 immune
checkpoint inhibitor, for patients with advanced, refractory squamous non-small-cell lung cancer (CheckMate 063):
a phase 2, single-arm trial. The Lancet. Oncology. 16: 257-65. doi: 10.1016/s1470-2045(15)70054-9
9. Tumeh PC, Harview CL, Yearley JH et al. (2014) PD-1 blockade induces responses by inhibiting adaptive
immune resistance. Nature. 515: 568-71. doi: 10.1038/nature13954
10. Warth A, Korner S, Penzel R, Muley T, Dienemann H, Schirmacher P, von Knebel-Doeberitz M, Weichert
W, Kloor M (2016) Microsatellite instability in pulmonary adenocarcinomas: a comprehensive study of 480 cases.
Virchows Archiv : an international journal of pathology. 468: 313-9. doi: 10.1007/s00428-015-1892-7
11. Schumacher TN, Schreiber RD (2015) Neoantigens in cancer immunotherapy. Science. 348: 69-74. doi:
10.1126/science.aaa4971
12. Rizvi NA, Hellmann MD, Snyder A et al. (2015) Cancer immunology. Mutational landscape determines
sensitivity to PD-1 blockade in non-small cell lung cancer. Science. 348: 124-8. doi: 10.1126/science.aaa1348
13. Carbone DP, Reck M, Paz-Ares L et al. (2017) First-Line Nivolumab in Stage IV or Recurrent Non-Small-
Cell Lung Cancer. The New England journal of medicine. 376: 2415-26. doi: 10.1056/NEJMoa1613493
14. Owada-Ozaki Y, Muto S, Takagi H et al. (2018) Prognostic Impact of Tumor Mutation Burden in Patients
With Completely Resected Non-Small Cell Lung Cancer: Brief Report. Journal of thoracic oncology : official
publication of the International Association for the Study of Lung Cancer. doi: 10.1016/j.jtho.2018.04.003
15. Hirsch FR, McElhinny A, Stanforth D et al. (2016) PD-L1 Immunohistochemistry Assays for Lung
Cancer: Results from Phase 1 of the "Blueprint PD-L1 IHC Assay Comparison Project". Journal of thoracic
oncology : official publication of the International Association for the Study of Lung Cancer. doi:
10.1016/j.jtho.2016.11.2228
16. Teng MW, Ngiow SF, Ribas A, Smyth MJ (2015) Classifying Cancers Based on T-cell Infiltration and
PD-L1. Cancer research. 75: 2139-45. doi: 10.1158/0008-5472.can-15-0255
17. Rashed HE, Abdelrahman AE, Abdelgawad M, Balata S, Shabrawy ME (2017) Prognostic Significance
of Programmed Cell Death Ligand 1 (PD-L1), CD8+ Tumor-Infiltrating Lymphocytes and p53 in Non-Small Cell
Lung Cancer: An Immunohistochemical Study. Turk Patoloji Derg. 1: 211-22. doi: 10.5146/tjpath.2017.01398
18. Rizvi H, Sanchez-Vega F, La K et al. (2018) Molecular Determinants of Response to Anti-Programmed
Cell Death (PD)-1 and Anti-Programmed Death-Ligand 1 (PD-L1) Blockade in Patients With Non-Small-Cell Lung
Cancer Profiled With Targeted Next-Generation Sequencing. Journal of clinical oncology : official journal of the
American Society of Clinical Oncology. 36: 633-41. doi: 10.1200/JCO.2017.75.3384
19. Reck M, Rodriguez-Abreu D, Robinson AG et al. (2016) Pembrolizumab versus Chemotherapy for PD-
L1-Positive Non-Small-Cell Lung Cancer. The New England journal of medicine. doi: 10.1056/NEJMoa1606774
20. Chen DS, Mellman I (2017) Elements of cancer immunity and the cancer–immune set point. Nature. 541:
321. doi: 10.1038/nature21349
https://www.nature.com/articles/nature21349#supplementary-information
21. Seetharamu N, Preeshagul IR, Sullivan KM (2017) New PD-L1 inhibitors in non-small cell lung cancer -
impact of atezolizumab. Lung Cancer (Auckland, N.Z.). 8: 67-78. doi: 10.2147/lctt.s113177
22. Rooney MS, Shukla SA, Wu CJ, Getz G, Hacohen N (2015) Molecular and genetic properties of tumors
associated with local immune cytolytic activity. Cell. 160: 48-61. doi: 10.1016/j.cell.2014.12.033
23. Spranger S, Luke JJ, Bao R, Zha Y, Hernandez KM, Li Y, Gajewski AP, Andrade J, Gajewski TF (2016)
Density of immunogenic antigens does not explain the presence or absence of the T-cell-inflamed tumor
microenvironment in melanoma. Proc Natl Acad Sci U S A. 113: E7759-e68. doi: 10.1073/pnas.1609376113
24. Kim HS, Lee JH, Nam SJ, Ock CY, Moon JW, Yoo CW, Lee GK, Han JY (2018) Association of PD-L1
Expression with Tumor-Infiltrating Immune Cells and Mutation Burden in High-Grade Neuroendocrine Carcinoma
of the Lung. Journal of thoracic oncology : official publication of the International Association for the Study of
Lung Cancer. 13: 636-48. doi: 10.1016/j.jtho.2018.01.008
25. Blank CU, Haanen JB, Ribas A, Schumacher TN (2016) CANCER IMMUNOLOGY. The "cancer
immunogram". Science. 352: 658-60. doi: 10.1126/science.aaf2834
26. Karasaki T, Nagayama K, Kuwano H et al. (2017) An Immunogram for the Cancer-Immunity Cycle:
Towards Personalized Immunotherapy of Lung Cancer. Journal of thoracic oncology : official publication of the
International Association for the Study of Lung Cancer. 12: 791-803. doi: 10.1016/j.jtho.2017.01.005
27. Alexandrov LB, Nik-Zainal S, Wedge DC et al. (2013) Signatures of mutational processes in human cancer.
Nature. 500: 415-21. doi: 10.1038/nature12477
28. Van Allen EM, Miao D, Schilling B et al. (2015) Genomic correlates of response to CTLA-4 blockade in
metastatic melanoma. Science. 350: 207-11. doi: 10.1126/science.aad0095
29. Konishi J, Yamazaki K, Azuma M, Kinoshita I, Dosaka-Akita H, Nishimura M (2004) B7-H1 expression
on non-small cell lung cancer cells and its relationship with tumor-infiltrating lymphocytes and their PD-1
expression. Clinical cancer research : an official journal of the American Association for Cancer Research. 10:
5094-100. doi: 10.1158/1078-0432.CCR-04-0428
30. He Y, Rozeboom L, Rivard CJ, Ellison K, Dziadziuszko R, Yu H, Zhou C, Hirsch FR (2017) PD-1, PD-
L1 Protein Expression in Non-Small Cell Lung Cancer and Their Relationship with Tumor-Infiltrating
Lymphocytes. Medical Science Monitor. 23: 1208-16. doi: 10.12659/msm.899909
31. Takamochi K, Takahashi F, Suehara Y et al. (2017) DNA mismatch repair deficiency in surgically resected
lung adenocarcinoma: Microsatellite instability analysis using the Promega panel. Lung cancer (Amsterdam,
Netherlands). 110: 26-31. doi: 10.1016/j.lungcan.2017.05.016
32. Steuer CE, Ramalingam SS (2018) Tumor Mutation Burden: Leading Immunotherapy to the Era of
Precision Medicine? Journal of clinical oncology : official journal of the American Society of Clinical Oncology.
36: 631-2. doi: 10.1200/JCO.2017.76.8770
33. Garofalo A, Sholl L, Reardon B et al. (2016) The impact of tumor profiling approaches and genomic data
strategies for cancer precision medicine. Genome Med. 8: 79. doi: 10.1186/s13073-016-0333-9
34. Campesato LF, Barroso-Sousa R, Jimenez L, Correa BR, Sabbaga J, Hoff PM, Reis LF, Galante PA,
Camargo AA (2015) Comprehensive cancer-gene panels can be used to estimate mutational load and predict clinical
benefit to PD-1 blockade in clinical practice. Oncotarget. 6: 34221-7. doi: 10.18632/oncotarget.5950
35. Global Burden of Disease Cancer C, Fitzmaurice C, Allen C et al. (2017) Global, Regional, and National
Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-years
for 32 Cancer Groups, 1990 to 2015: A Systematic Analysis for the Global Burden of Disease Study. JAMA
oncology. 3: 524-48. doi: 10.1001/jamaoncol.2016.5688
36. Suzuki H, Kawaguchi T, Hasegawa T et al. (2006) Prognostic impact of p53 protein overexpression in
patients with node-negative lung adenocarcinoma. Cancer Lett. 237: 242-7. doi: 10.1016/j.canlet.2005.06.014
Table 1. Univariate analysis for predicting TMB.
n mean 95%CI p value
EGFR Positive 27 32.0 25.8-38.2 <0.0001
Negative 65 136.0 107.3-164.8
TP53 Positive 56 138.0 105.7-170.3 <0.0001
Negative 36 55.0 35.1-74.9
KRAS Positive 11 94.8 33.6-156.0 0.7871
Negative 81 107.0 82.4-131.6
ERBB2 Positive 8 81.5 53.7-125.6 0.3653
Negative 84 54.5 82.5-131.5
BRAF Positive 2 207.0 0.0-2189.2 0.3987
Negative 90 60.0 81.0-125.5
CTNNB1 Positive 3 30.7 0.0-81.8 0.0893
Negative 89 108.0 85.0-131.1
PTEN Positive 4 70.8 49.0-92.5 0.6743
Negative 88 107.1 83.6-130.6
CDKN2A
aPositive 3 199.7 62.6-336.8 0.0196
Negative 55 80.7 57.5-103.8
PIK3CA Positive 6 80.0 15.2-144.8 0.8321
Negative 86 107.3 83.5-131.1
Age >68 50 91.0 69.7-112.3 0.9363
<67 42 122.8 79.9-165.7
Sex Male 65 127.5 98.8-156.2 <0.0001
Female 27 52.5 27.0-78.1
Smoking Smoker 64 134.0 104.3-163.8 <0.0001
Never 28 40.4 32.5-48.2
Histology Ad 64 80.5 55.0-106.0 <0.0001
Sq 28 162.6 122.7-202.5
Tumor size >=2.8 48 128.4 82.6-164.1 0.0218
(average2.7) <2.7 44 80.6 54.8-106.5
Stage ⅠⅡ 80 100.2 77.3-123.1 0.3719
ⅢⅣ 12 140.8 51.3-123.2
LN + 17 133.8 66.9-200.6 0.3833
- 75 99.1 75.4-122.9
p53 IHC 1-3+ 47 122.1 89.3-155.0 0.0249
- 45 88.2 57.1-119.2
ALK IHC Positive 2 38.0 0.0-228.6 0.3586
Negative 90 107.0 84.1-129.9
CD8+TIL 3+ 23 93.5 53.1-133.9 0.6688
1+/2+ 69 109.5 82.2-136.8
PD-L1 + 11 156.3 60.2-252.3 0.1479
- 81 98.6 76-121.3
a
CDKN2A mutation was identified using a CHP panel only, while other mutations were identified
using CLP panel sequences. Therefore, the total number of CDKN2A analyses was 58, which differed
from other CLP panel sequence analyses.
TMB: tumor-mutation burden, TP53; tumor protein 53, KRAS; v-Ki-ras2 Kirsten rat sarcoma viral
oncogene homolog, ERBB2; human epidermal growth factor receptor 2, BRAF; v-raf murine sarcoma
viral oncogene homolog B1, CTNNB1; catenin, beta-1, PTEN; phosphatase and tensin homolog
deleted from chromosome 10, CDKN2A: cyclin-dependent kinase-inhibitor gene 2A, PIK3CA;
phosphoinositide-3-kinase, catalytic, alpha polypeptide, CHP: cancer hotspot panel, CLP: colon and
lung cancer research panel, Ad: adenocarcinoma, Sq: squamous cell carcinoma, LN: lymph node,
IHC: immunohistochemical staining, ALK; anaplastic lymphoma kinase, CD8; cluster of
differentiation 8 , TIL; tumor infiltrating lymphocyte, PD-L1; programmed cell death ligand 1
Supplementary Tables
Table S1. Patients’ characteristics.
N=92
Median age (range) 70 (40-87)
Gender Male / female 65 (70.7%) / 27 (29.3%)
Smoking status Never smoker 28 (30.4%)
Past or current smoker 64 (69.6%)
Median brinkman Index
(range) 700 (45-2580)
Tumor size (cm) 2.8 (0.8-11.0)
Histology Adenocarcinoma 64 (69.6%)
Squamous cell carcinoma 28 (30.4%)
PD-L1 + / - 11 (12.0%) / 81 (88.0%)
TIL high / intermediate / low 23 (25.0%)/53 (57.6%)/16 (17.3%)
Pathological stage
ⅠA 44 (47.8%)
ⅠB 24 (26.1%)
ⅡA 4 (4.3%)
ⅡB 8 (8.7%)
ⅢA 9 (9.8%)
ⅢB 2 (2.2%)
Ⅳ 1 (1.1%)
EGFR-mutation
Exon21;L858R 17 (18.5%)
Exon19 deletion 8 (8.7%)
Others 2 (2.2%)
Wild type/Unknown 65 (70.6%)
PD-L1: programmed cell-death ligand 1, TIL: tumor-infiltrating lymphocytes
Table S2. Multivariate analysis for predicting TMB.
β 95%CI p value
Gender Male -10.009 -38.90-18.88 0.7298
Brinkman Index 0.028 0.01-0.05 0.1885
Pathology Sq 18.380 -7.30-44.07 0.4763
Tumor size 7.581 1.72-13.44 0.1994
EGFR Positive -65.327 -90.50-(-40.16) 0.0111
TP53 Positive 47.050 24.20-69.90 0.0425
CorrectedR
2=0.260 TMB, tumor-mutation burden, Sq: squamous cell carcinoma
Table S3. Characteristics of patients without the EGFR mutation.
N=65
Median age (range) 70 (40-87)
Gender Male / female 54 (83.1%) / 11 (16.9%)
Smoking status Past or current smoker 54 (83.1%)
Never smoker 11 (16.9%)
Median brinkman Index (range) 840 (120-2580)
Tumor size (cm) 2.9 (0.8-11.0)
Histology Adenocarcinoma 37 (56.9%)
Squamous cell carcinoma 28 (43.1%)
PD-L1 + / - 9 (13.8%) / 56 (86.2%)
TIL high / intermediate / low 17 (26.1%)/37 (56.9%)/11 (16.9%)
Pathological stage
ⅠA 29 (44.6%)
ⅠB 16 (24.6%)
ⅡA 4 (6.2%)
ⅡB 5 (7.7%)
ⅢA 9 (13.8%)
ⅢB 1 (1.5%)
Ⅳ 1 (1.5%)
EGFR: EGFR gene
Table S4. Univariate analysis for predicting TMB in EGFR-mutation-negative patients.
n mean 95%CI p value
TP53 Positive 45 162.2 125.3-199.1 0.0006
Negative 20 77.2 43.8-110.6
KRAS Positive 11 94.8 33.6-156.0 0.1015
Negative 54 144.4 111.8-177.0
ERBB2 Positive 8 89.6 53.7-125.6 0.6204
Negative 57 142.6 110.3-174.8
BRAF Positive 2 207.0 0.0-2189 0.7221
Negative 63 133.8 105.1-162.4
CTNNB1 Positive 1 - - -
Negative 64 - -
PTEN Positive 4 70.8 49.0-92.3 0.4713
Negative 61 140.3 110.0-170.7
CDKN2A
bPositive 3 199.7 62.6-336.8 0.1435
Negative 39 133.0 103.1-162.8
PIK3CA Positive 5 86.0 2.78-169.2 0.3263
Negative 60 140.2 109.6-170.9
ALK IHC Positive 2 38.0 0-228.6 0.0976
Negative 63 139.2 109.8-168.5
p53 IHC 1-3+ 36 148.0 108.8-187.2 0.1429
- 29 121.2 76.9-165.5
Age >68 36 112.1 85.7-138.5 0.3361
<67 29 165.8 110.0-221.6
Gender Male 54 146.7 114.4-178.9 0.0296
Female 11 83.9 21.4-146.5
Smoking Smoker 54 153.0 120.3-185.8 0.0022
Never 11 52.6 38.3-67.0
Pathology Ad 37 115.9 75.1-156.8 0.0034
Sq 28 162.6 122.7-202.5
Tumor size >=2.8 37 156.8 114.6-199.0 0.0610
<2.7 28 108.6 71.4-145.7
Stage ⅠⅡ 54 132.9 102.6-163.3 0.9484
ⅢⅣ 11 151.4 55.6-247.1
LN + 15 148.5 75.7-221.4 0.8867
- 50 132.3 100.4-164.2
TIL 3+ 17 114.5 63.0-166.1 0.2973
1+/2+ 48 143.7 108.5-178.8
PD-L1 + 9 184.2 73.6-294.8 0.1984
- 56 128.3 98.7-157.9
b