Efficacy of Mepolizumab for Long-term Treatment in Patients with Severe Asthma
Yoshito M IYATA
*, Shin O HTA , Akihiko T ANAKA , Kaho A KIMOTO , Hiroki S ATO , Tomoki U NO , Haruna S ATO , Yoshitaka U CHIDA , Megumi J INNO ,
Kuniaki H IRAI , Hideki I NOUE , Tetsuya H ONMA , Mayumi Y AMAMOTO , Shintaro S UZUKI and Hironori S AGARA
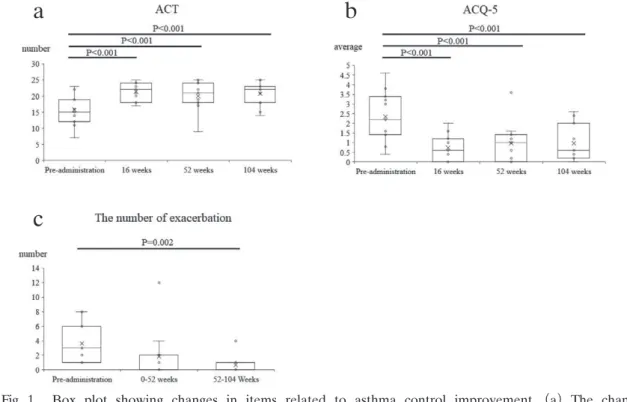
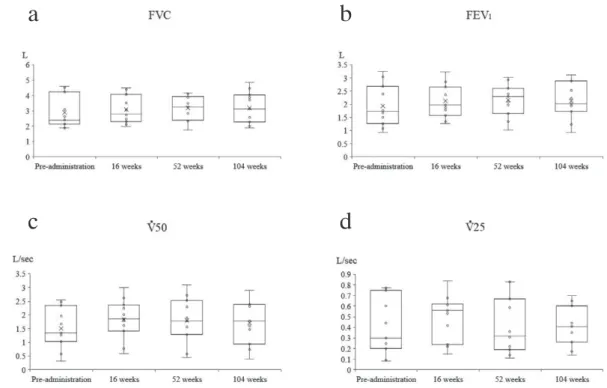
Abstract : Mepolizumab is a monoclonal antibody against interleukin-5 used for the treatment of severe asthma. The effect of long-term mepolizumab administration and its persistence in clinical practice is poorly understood. Thus, this study aimed to investigate the effect of long-term administration of mepolizumab in patients with severe asthma. Mepolizumab was administered to 20 patients with severe asthma. We then prospectively followed the patients for 104 weeks to investigate the efficacy of long-term mepolizumab administration in clinical practice. Eleven patients were evaluated for 104 weeks. Mepolizumab administration reduced asth- ma exacerbations in a year from 52 to 104 weeks and improved asthma control in every period as assessed by questionnaires. Also, blood eosinophil counts decreased at every point, and blood basophil counts decreased at 104 weeks. We compared various parameters among the 11 patients who continued administration for more than 104 weeks and 7 patients who discontinued treatment due to ineffectiveness.
Significant differences were observed in disease duration, maximum expiratory flow at 50%, and blood basophil count. Long-term mepolizumab administration improved asthma symptoms in patients with severe asthma and reduced the fre- quency of exacerbations.
Key words : mepolizumab, anti-IL-5 antibody, eosinophilic asthma, severe asthma, eosinophil count
Introduction
Bronchial asthma is a disease characterized by eosinophilic airway inflammation and remodel- ing, which limit airflow. These changes involve allergic inflammation that leads to the release of inflammatory cytokines and chemokines
1-3). The roles of several cytokines and chemokines in asthma have been elucidated
4-10). Interleukin (IL) -5 is involved in the proliferation and migra- tion of immature eosinophils in the bone marrow and in the activation of mature eosinophils, whereas IL-4 and IL-13 induce the production of immunoglobulin E (IgE) by B cells
4, 5).
Original
Department of Medicine, Division of Respiratory Medicine and Allergology, Showa University School of Medicine, 1-5-8 Hatanodai, Shinagawa-ku, Tokyo 142-8666, Japan.
*