はじめに 鏡視下手術手技・デバイスの発達により,巨大 単純性肝囊胞に対する治療は,腹腔鏡下手術が主 流となってきた.更に近年,single incision lapa roscopic surgery(SILS)やreduced port surgery (RPS)による開窓術や天蓋切除術の報告がみられ る.当科にて2例の巨大肝囊胞に対し,それぞれ 異なるデバイスを用いて手術を行い,良好な結果 を得たので報告する. 症 例 症例1:70代,女性. 主 訴:右上腹部の違和感,食欲不振. 既往歴:高血圧症,狭心症,帝王切開術. 現病歴:上記主訴に対して他院で腹部エコーを 施行.巨大肝囊胞と胆囊ポリープを指摘され,手 術目的に当科へ紹介となった. 初診時現症:全身状態良好,上腹部に境界明瞭 受付:2013年10月21日,採用:2013年11月14日 連絡先 江口 晋 〒852-8501 長崎県長崎市坂本1-7-1 長崎大学大学院移植・消化器外科 で圧痛を伴う弾性硬な腫瘤を触知,下腹部正中切 開痕あり,その他明らかな異常所見なし. 血液検査所見:血算,生化学,腫瘍マーカー全 て正常範囲内. 画像検査所見:腹部超音波検査;肝右葉に15.8 ×14.6cm大の囊胞を認めた.腹部造影CT;肝右葉 に最大径16cm大の肝囊胞を認めた.壁の一部に石 灰化が存在したが,明らかな結節は認めず.胆囊 内造影効果を伴う最大径1cmのポリープあり (Fig. 1 ).MRCP;肝囊胞により肝内胆管の強い 圧排を認めた.前区域枝は同定が困難であり,後 区域枝は尾側に圧排されていた.肝内胆管の拡張 なし(Fig. 2 ).胆道シンチ;薬剤投与後2時間後 でも囊胞内への流入はなく,胆管と囊胞の交通は 否定的であった. 手術所見:術式;単孔式腹腔鏡下肝囊胞天蓋切 除術,胆囊摘出術.手術時間;195分.出血量; 30g.囊胞内容液;4,000ml.手術要旨;臍部にSILS Port™を装着し,右季肋部よりMini Loop Retractor を挿入.SILSでの胆囊摘出術を施行した後に,肝 囊胞の天蓋切除術を施行した.デバイスは電気メ スとLigaSure Dolphin tip™を使用した.囊胞液を 内容要旨 〈症例1〉70代,女性.右上腹部の違和感と食欲不振を主訴に受診.精査にて肝右葉に最大径160mm 大の単純性囊胞を認めた.これに対し,SILS Port™,Mini Loop Retractorを用いたsingle incision laparoscopic surgery(SILS)を施行した.〈症例2〉70代,女性.上腹部痛,右肩痛を主訴に受診. 精査にて肝右葉に最大径190mm大の単純性肝囊胞を認めた.これに対し,GelPoint®,3mm鉗子を用 いたreduced port surgery(RPS)を施行した.異なる手術器具と手法を用いた2症例で良好な結果 を得ることができたため,腹腔鏡手術が主流となりつつある近年の巨大肝囊胞に対する外科的治療に 関して,その差異,文献的考察を含めて報告する. 索引用語:巨大肝囊胞,single incision laparoscopic surgery,reduced port surgery
症例報告
巨大肝囊胞に対するreduced port laparoscopic surgery
長崎大学大学院移植・消化器外科井上 悠介
曽山 明彦
日高 匡章
足立 智彦
北里 周
高槻 光寿
黒木 保
江口 晋
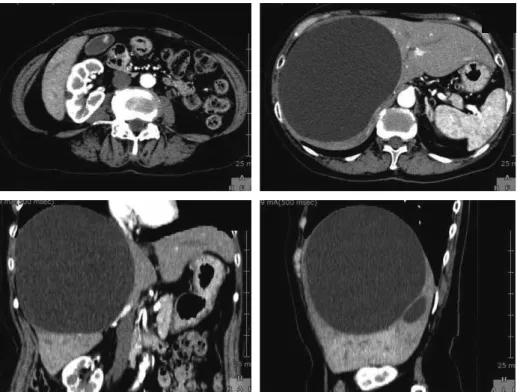
Fig. 2 MRCP showed that the intrahepatic bile duct was strongly compressed by the liver cyst. However, the diameter of the intrahepatic bile duct was normal.
Fig. 1 An enhanced abdominal CT scan showed a simple huge hepatic cyst with a maxi-mum diameter of 160mm in the right hepatic lobe, and an enhanced gallbladder polyp with
a maximum diameter of 10mm. a b c d 吸引嘴管で吸引し,天蓋の切除と電気メスによる 囊胞壁の焼灼を行った.肝円蓋部付近の処理に関 しては,鉗子を接線方向で操作する必要があり, 処理に難渋する場面もあった. 病理所見:Cholesterol polyps with mild chole cystitis(悪性所見なし). Hepatic solitary cyst(悪性所見なし). 術後経過:術後,症状は消失し,合併症なく退 院となった. 症例2:70代,女性. 主 訴:上腹部痛,右肩痛. 既往歴:十二指腸癌(EMR後),帝王切開術. 現病歴:10年程前より肝囊胞を指摘されていた が,症状はなく経過観察中であった.今回,上記 主訴にて手術目的に当科紹介となった. 初診時現症:全身状態良好,右季肋下に3cm程 度肝臓を触知する,その他明らかな異常所見なし. 血液検査所見:血算,生化学,腫瘍マーカー全 て正常範囲内. 画像検査所見:腹部造影CT;肝右葉に最大径 1 9 c m の 肝 囊 胞 あ り,結 節 や 石 灰 化 は 認 め ず (Fig. 3 ).MRCP;肝囊胞により肝内胆管の強い圧 排を認めた.肝内胆管の拡張なし.囊胞と胆管の
Fig. 3 An enhanced abdominal CT scan showed a simple huge hepatic cyst with a maximum diameter of 190mm in the right hepatic lobe with no nodules or calcifications.
Fig. 4 MRCP showed that the intrahepatic bile duct was strongly compressed by the liver cyst. However, the diameter of intrahepatic bile duct was normal. The cyst and bile duct were not connected. A non-uniform signal was present in the cyst. a b c 交通なし.内部に不均一な信号を認めた(Fig. 4 ). 手術所見:術式;腹腔鏡下肝囊胞天蓋切除術. 手術時間;249分.出血量;100g.手術要旨; (Fig. 5 ). 臍部にGelPoint®を装着.悪性が完全に否定で きていなかったため,サンドバルーンカテーテル にて内容液が漏出しないように吸引した.内容は 出血性の囊胞液であり,画像上不均一に見えた部 分はフィブリン塊であった.術中迅速細胞診でも 悪性所見は認めなかった.その後,電気メス, LigaSure Dolphin tip™を用いて囊胞壁を切除した. 後出血の予防目的に,囊胞壁をERBE VIO system のソフト凝固モードで焼灼した.囊胞壁にcounter tractionをかける際,右季肋部より3mmポートを 挿入した(reduced port surgery).これにより操 作性が格段に向上した. 病理所見:Hepatic solitary cyst(悪性所見な し). 術後経過:術後,症状は消失し,合併症なく退 院となった.
考 察 単純性肝囊胞は,通常,治療を要することは少 ないが,出血,破裂,感染,径の増大による疼痛 などが併発した場合は治療対象となる1)2).治療法 としては,エタノールや塩酸ミノサイクリンなど の囊胞内注入療法3)~6)と,肝切除,囊胞切除,開 窓術などの外科的治療に大別される.近年,腹腔 鏡手術の普及によって,腹腔鏡下肝囊胞開窓術, 天蓋切除術の報告がなされるようになり,最近で は,single incision laparoscopic surgery(SILS) やreduced port surgery(RPS)による手術の報 告もみられる7)~12).SILSやRPSは従来のマルチポ ートによる手術と比較して,整容性に優れており, 腹壁破壊などの侵襲も少ないと思われるが,その 反面,手術の難度が高く,習熟した技術を要する ため,未だ定型手術とまでは至っていないのが現 状である. 今回,われわれはSILS Port™とMini Loop Re tractorを利用したSILS,GelPoint®+3mm鉗子 を利用したRPSを各1例に行った.GelPoint®を 利用した手術は,SILS Port™と比較して,特殊な 鉗子が必要なく,また鉗子の自由度も大きいとい う特徴がある.いずれの症例においても術中,術 後に問題はなかった.症例2に関しては,肝囊胞 が巨大であり,囊胞壁が横隔膜下まで存在したた め,鉗子と囊胞壁が接線方向となり難度が高かっ た.横隔膜直下に存在する肝囊胞天蓋切除術を SILSの適応から除外しているという報告もみられ るが7),われわれは,3mmポートを右季肋下に挿 入することにより,格段に操作性を改善させ,安 全に手術を完遂することができた.症例1の様に, Mini Loop Retractor使用して囊胞壁を把持する方 法も報告されているが8),操作性,経済性の両面か ら,3mm鉗子の使用によるRPSは有用な方法と
a
b
c
d
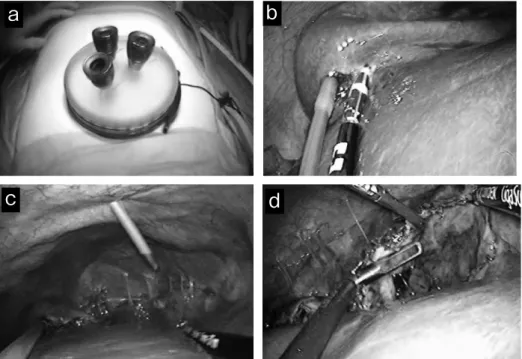
Fig. 5 The intraoperative findings. a: Installing the GelPoint®.
b: Starting the removal of the cyst wall with the LigaSure™ device after aspirating the contents with the sand balloon.
c: A 3mm port was added.
d: By using the two forceps, we could expand the field of view without inducing any ad-ditional stress.
思われる.また,胆管との交通を認める症例に関 しては,胆管の確実な結紮が必要になるため,ポ ートの追加を推奨している報告もみられる9). 術後の創に関しては,3mmポート部は,凝視 しないと認識が難しいほどの創となった(Fig. 6 ). Mini Loop Retractorの刺入痕と比較してもほとん ど変わらず,これより,術後の整容性にほとんど 影響しないということが示唆された.このように, 当科では,SILSに拘らず,ポート追加による利点 がより生かされる症例ではRPSを選択するという ように,両者を適切に使い分けることが重要と考 えている. 文 献 1)山田 護,武藤良弘:肝囊胞の取り扱い―症状と 治療適応・手技.綜合臨 43:2715-2716,1994 2)Litwin DE, Taylor BR, Langer B, et al : Nonpara sitic cysts of the liver. The case for conservative surgical management. Ann Surg 205 : 45-48, 1987 3)稲吉 厚,坂本快郎,徳永伸也,他:非寄生虫性 肝囊胞に対するエコーガイド下の塩酸ミノサイク リンと炭酸ガス1回注入療法.日臨外医会誌 61: 2276-2281,2000 4)志村純一,浮田雄生,井上博和,他:多発性肝囊 胞による胆管圧排狭窄を塩酸ミノサイクリン局注 により解除しえた1例.日消誌 97:1038-1042, 2000 5)高山哲夫,吉江研一,曽我洋一,他:肝囊胞の治 療としての囊胞内純エタノール注入療法の臨床的 意義.肝・胆・膵 10:969-973,1985
6)William JB, Bruce AR : Hepatic cysts : treatment with alcohol. AJR 144 : 237-241, 1985 7)鈴木文武,三澤健之,後町武志,他:単孔式腹腔 鏡下手術で肝囊胞開窓術と胆囊摘出術を同時施行 した1例.日外科系連会誌 6:987-991,2011 8)Sasaki K, Watanabe G, Matsuda M, et al : Original method of transumbilical singleincision laparo scopic deroofing for liver cyst. J Hepatobiliary Pancreat Sci 17 : 733-734, 2010 9)松本浩次,堀 義城,岩田英之,他:胆管と交通 を有した単純性肝囊胞に対し単孔式腹腔鏡下肝囊 胞天蓋切除術にて治癒し得た1例.日内視鏡外会 誌 16:575-579,2011 10)石川正志,古川尊子,松岡 裕,他:単孔式によ る吊り上げ式腹腔鏡手術を行った胆囊結石合併肝 囊胞の1例.臨と研 87:99-102,2010 11)Dapri G, Barabino M, Carnevali P,et al : Single access transumbilical laparoscopic unroofing of a giant hepatic cyst using reusable instruments. JSLS 16 : 296-300, 2012 12)Kashiwagi H, Kumagai K, Nozue M : Single incision laparoscopic surgery for a lifethreatening, cyst of liver. Tokai J Exp Clin Med 36 : 13-16, 2011 Fig. 6 A photograph of the