INTRODUCTION
Child deaths worldwide have decreased in num-ber from 13!5 (13!4-13!6) million in 1980 to an
estimated 9!7 (9!5-10!0) million in 2005 ; how-ever, the decline is less than the target set by Mil-lennium Development Goal 4 (MDG4) (1). Most of the child deaths were caused by preventable and treatable illness despite effective health interven-tions. At least half of the deaths are caused by un-dernutrition (2). UNICEF has developed a frame-work for the basic underlying causes of undernu-trition and has demonstrated that a combination of insufficient nutrient intake and infection are the
ORIGINAL
Nutritional status, feeding practice and incidence of
infectious diseases among children aged 6 to 18
months in northern mountainous Vietnam
Masayo Nakamori
1, Nguyen Xuan Ninh
2, Nguyen Cong Khan
2, Cao Thu Huong
2,
Nguyen Anh Tuan
2, Le Bach Mai
2, Vu Thi Thu Hien
2, Bui Thi Nhung
2,
Takashi Nakano
3, Nobuo Yoshiike
4, Kaoru Kusama
5, and Shigeru Yamamoto
1 1Department of Nutrition and Food Science, Ochanomizu University, Tokyo, Japan ;2
National Institute of Nutrition, Hanoi, Vietnam ;3
Department of Pediatrics, National Mie Hospital, Mie, Japan ;4
Faculty of Health Science, Aomori University of Health and Welfare, Aomori, Japan ; and 5
Department of Human Resources Development, National Institute of Public Health, Saitama, Japan
Abstract : Objective : To assess the prevalence of undernutrition, incidence of infectious diseases and the situation of feeding practices to determine the risk factors for undernutri-tion among children aged 6 to 18 months in rural Vietnam. Design : A cross-secundernutri-tional study was conducted among one hundred eighty-eight mother-child pairs in Bac Giang, Viet-nam. Weight and height of the children were measured and referred to data from the WHO/CDC/NCHS. Incidence of infectious diseases was diagnosed based on the WHO Rec-ommended Surveillance Standards. Data on socio-demographic variables and feeding practices were obtained through a structured questionnaire. Result : The prevalence of underweight, stunting and wasting was 19.7%%, 23.4%% and 5.3%%, respectively. The incidence of diarrhea and acute respiratory infections (ARIs) during the last 14 days of the inter-view was 12.2%% and 20.2%%, respectively. Although 99%% of the children were breastfed, the prevalence of exclusive breastfeeding in the first 4 mo was 21.3%%. Non-exclusive breast-feeding in the first 4 month (OR 3.95, p=0.025) and low birth weight (OR 4.38, p=0.009) were associated with underweight in the children, while incidence of infectious disease was not (OR 1.16, p=0.734). Conclusion : Undernutrition is highly prevalent in the study site and non-exclusive breast feeding is one of the risk factors. J. Med. Invest. 57 : 45-53, February, 2010
Keywords : undernutrition, exclusive breastfeeding, infectious disease, Vietnam, infant and child
Received for publication August 5, 2009 ; accepted September 28, 2009.
Address correspondence and reprint requests to Shigeru Yamamoto, Department of Nutrition and Food Science, Ochano-mizu University, 2 - 1 - 1 Otsuka, Bunkyo - ku, Tokyo 112 - 8610, Japan and Fax : +81 - 3 - 5978 - 5448.
primary factors (3). When children consume insuf-ficient nutrients, their immune systems deteriorate, resulting in greater incidence, severity and duration of disease. Disease in turn affects their nutrient in-take and also interferes with nutrient absorption, fur-ther aggravating the undernutrition. As to the un-derlying causes of undernutrition, poverty plays a central role with environmental, economic, and so-ciopolitical factors.
In Vietnam, child undernutrition is one of the ma-jor national health problems. It has been reported that the nationwide prevalence of child undernutri-tion has been remarkably reduced during the last 2 decades : the prevalence of underweight among chil-dren aged under 5 y was 51.5% in 1985, but it was reduced to 25.2% in 2005 (4). However, the preva-lence of undernutrition varied among ecological re-gions in Vietnam. A greater proportion of the popu-lation in mountanious and remote areas were under-nourished than in urban areas. The child undernu-trition problem was reported to occur from an early stage of their life in Vietnam. The prevalence of un-dernutrition increased remarkably during 6 to 18 mo and was sustained over the next 3 y (4). Previous studies indicated that premature complementary feeding (5, 6) and frequent infectious disease (7) were the primary causes. It has also been recog-nized that stunting occurred even before 6 mo of age : 6.3% of children aged under 6 mo were stunted (4). Poor health care and insufficient food intake during pregnancy were also suggested as high risk factors for childhood undernutrition.
Although approach for general deprivation and inequality would result in substantial reduction in undernutrition and should be global priority, major reduction in undernutrition can also be achieved through programmatic health and nutrition interven-tion (8-11). The present study was aimed at provid-ing baseline information, includprovid-ing the prevalence of undernutrition, incidence of infectious disease and the situation in feeding practice among children aged 6 to 18 mo for future programs with which to combat child undernutrition in northern mountain-ous Vietnam.
METHODS
During May and June 2005, in the middle of the dry season, a cross-sectional survey was conducted in 4 communes in Yen The, Bac Giang, Vietnam. Bac Giang province is a rural mountainous region
in Vietnam, located in the North-East region and 51 km from Hanoi. The province had a relatively high prevalence of childhood undernutrition among the 8 regions in Vietnam (4). Yen The district is one of the nine districts in the province. The district has a population of approximately 91,000 with 7,500 chil-dren under 5 y of age and 2,900 chilchil-dren under 2 y (Dec, 2004). There are 19 communes in the district, out of which four communes were selected. Ex-tremely poor villages which belong to the govern-ment’s “Phase One 10,000 Poorest Communities” Program and the villages that were already targeted in special intervention programs by the government were not included among the selected communes. All children aged 6 to 18 mo were recruited for the survey. A census was carried out to identify all chil-dren aged 6 to 18 mo and 191 eligible chilchil-dren were identified.
Anthropometric measurements comprising height and weight were performed among the children and mothers by four trained field workers using standard procedures (12). Briefly, children were weighed in light cloths on an infant scale. Recumbent length was measured to the nearest 0.1 cm with a portable infant measuring board. The anthropometric indica-tors for children, Z-scores of weight-for-age (WAZ), height-for-age (HAZ) and weight-for-height (WHZ), were calculated on the basis of growth references de-veloped by the World Health Organization (WHO), the Center Disease for Control (CDC), and the Na-tional Center for Health Statistics (NCHS) (13) and were calculated also by using growth references re-cently developed by WHO (14). Most of the avail-able data on the growth of children in Vietnam were calculated based on WHO/CDC/NCHS growth ref-erences at the time that the present study was con-ducted. Undernutrition was classified according to the cut-off indicated by WHO (15) : underweight was defined as WAZ!-2, stunting as HAZ!-2, wast-ing as WHZ!-2. Mothers were weighed in light clothes (to the nearest 100 g) on a scale. Height was measured to the nearest 0.1 cm. Chronic Energy Deficiency (CED) among mothers was classified as Body Mass Index (BMI) under 18.5 kg/m2.
Morbidity data were collected from the mother’s description of the infant’s symptoms of diarrhea, acute respiratory infections (ARIs), measles and per-tussis during the previous two weeks. The descrip-tions of the infectious diseases were based on the WHO recommended Surveillance Standards (16). Children who had a passage of 3 or more loose or watery stools in the past 24 hours were classified
as suffering from diarrhea. If the diarrhea lasted more than 2 weeks, these children were classified as suffering from chronic diarrhea. If the stool con-tained blood, these children were classified as suf-fering from dysentery. Children who had a cough or difficulty breathing were classified as suffering from ARIs. If the cough or difficult breathing was accom-panied by frequent breathing ("50 breath/min. for age 2 mo to!1 y,"40 breath/min. for age 1 to!5 y), these children were classified as suffering from pneumonia. Measles was determined if a child had all of the following three symptoms : fever, maculo-papular rash, and cough or coryza or conjunctivitis. Pertussis was determined if a child showed both of the following symptoms : cough for at least 2 wks with at least one of the following : paroxysms of coughing, inspiratory “whooping”, post-tussive vomiting without other apparent cause.
In this survey, a face-to-face interview was con-ducted with mothers and children to collect infor-mation on socio-demographic status, feeding prac-tices and coverage of local immunization and Vita-min A supplementation. Data collection concerning breast feeding practice was based on WHO guide-lines (17) and on a previous study in Vietnam (5). The mothers were asked about their breastfeeding practices during the children’s first 6 mo and also about the current breastfeeding status. The follow-ing operational definitions were used in the survey : breastfeeding referred to children who were receiv-ing at the time of interview or had ever received breast milk. Breastfeeding status at 4 and 6 mo of age were classified as exclusive breastfeeding (only breast milk plus medical drops and syrups), almost exclusive breastfeeding (only breast milk and water plus medical drops and syrups), predominant breast-feeding (water, herbal teas or fruit juice in addition to breast milk), partial breastfeeding (breast milk plus other types of milk or foods) and weaned (no longer breastfed). All the questions were pre-tested at a study site and revised before initiating the sur-vey. The interviewers, physicians from the NIN and local community health centers, were trained in standardized questionnaire administration and an-thropometric measurements through lectures and practice in the field. Four investigation teams were established for the four communities, each one in-cluding at least eight members and a supervisor. During the survey, a check system was applied in-cluding checking in the field by interviewers, inter-viewer’s checking each other, and checking by su-pervisors. Personnel in the local community centers
and collaborators assisted in the organization of data collection and in the explanation of procedures to the study participants. The study participants were re-interviewed whenever transcription or logical questions arose or missing values were found. The apparatus and method for measurement were checked and/or adjusted for accuracy by the super-visors before each day’s work. The precise age of each child was obtained from the Permanent Resi-dence Registration where birth data are recorded.
Before the survey, all eligible mothers in the com-munities were informed of the procedures and pur-pose of the study, then informed consent was ob-tained. The protocol of this study was approved by the Scientific Board of the National Institute of Nu-trition of Vietnam and the Ethical Committee of Tokushima University.
A database was established using Epi info version 6 (CDC, Atlanta, GA, USA). All data were checked for missing data and outliers, and cleaned before data analysis. Statistical analysis was performed us-ing SPSS version 11.5J (Statistical Package for Social Science, Inc.). A one-sample Kolmogorov-Smirnov test was used to assess whether the data were nor-mally distributed. Results were presented as mean and standard deviation (SD) or as median and 25th, 75thpercentile. Z-scores between children aged 6 to 11.9 mo and those aged 12 to 17.9 mo were com-pared by unpaired t-test. Z-scores calculated by WHO/CDC/NCHS and WHO growth reference were compared by paired t-test. The proportion of children classified as underweight, stunted and wasted were compared by chi-square test. Logistic regression analysis was used to analyze the effects of infectious disease and exclusive breastfeeding status, as well as those of socioeconomic and demo-graphic factors, on the nutritional status of children. We selected children’s underweight for the analysis since acute malnutrition among children is a key in-dicator routinely used for describing the presence and magnitude of humanitarian emergencies (18).
RESULTS
Socio-demographic characteristics and coverage of some of local health services
A pair of twins and a child whose mother was suf-fering from tuberculosis were excluded and the data of 188 children were used for the analysis in the pre-sent study. Socio-demographic characteristics of the children are shown in Table 1. Ninety one percent
of children belonged to the “Kinh” ethnic group. As to the main family occupation, 55.3% were farmers or agricultural workers. Water from wells was used by 98.4% of the participant households and 99% of mothers answered that they boiled the water for drinking. The latrine types were mainly traditional pit latrine (76.1%) and ventilated improved pit latrine (13.3%). The family income per capita was!17,800 VND, 17,800-35,600 VND and "35,600 VND for 67.0%, 20.7% and 12.2% of the study participants, re-spectively. Coverage of immunization in the study site was 99.5% for BCG, 97.4% for DPT 3rd, 97.9% for OPV 3rd, 97.3% for Measles and 63.7% for Hepatitis B 3rd. The coverage of Vitamin A distribution among the children aged 6 to 36 mo was 96.7%.
Z-scores and the prevalence of undernutrition calculated by WHO/CDC/NCHS reference (13) among the children are shown in Table 2. The prevalence of underweight, stunting and wasting
was 19.7%, 23.4% and 5.3%, respectively. The WAZ, HAZ and WHZ among the children aged 12 to 18.9 mo were significantly lower than those among the children aged 6 to 11.9 mo (P!0.05). When the Z-score was calculated by the recent WHO growth ref-erence (14) for all the children (n=188), the mean WAZ, HAZ and WHZ were -0.91!1.08, -1.21!1.19 and -0.37!1.09, respectively ; and the prevalence of underweight, stunting and wasting was 25.5% (n= 48), 14.9% (n=28), 6.9% (n=13), respectively. Com-paring these scores with the NCHS growth refer-ence, the mean WAZ and WAZ were significantly lower (P!0.001), the mean HAZ was similar (P = 0.772), and a higher proportion of children was clas-sified as stunted (P!0.001) and fewer children were classified as underweight (P!0.001).
Table 3 shows the incidence of diarrhea and ARIs Table 1 Socio - demographic characteristics
Variable All (n=188) Gender Boys 111 (53.7%)1 Girls 87 (46.3%) Age 6 - 8.9 mo 64 (34.0%) 9 - 11.9 mo 34 (18.1%) 12 - 14.9 mo 30 (16.0%) 15 - 18.9 mo 60 (31.9%) Birth weight, g 3000 (2700, 3375)2 Low Birth Weight 20 (10.6%) Number of children aged under 5 y
1 child 149 (79.3%)
"2 children 39 (20.7%) Family income, 1000VND/capita/d3 11.1 (6, 22.2) Mother’s age, y 25.0 (22, 28) Mother’s education level
Primary school (1 - 5 y) 26 (13.8%) Secondary school (6 - 9 y) 130 (69.1%) More ("10 y) 32 (17.0%) Mother’s BMI4 6 - 11.9 mo postpartum, kg/m2 19.7 (18.4, 20.8) 12 - 18.9 mo postpartum, kg/m2 19.0 (17.8, 20.1) Abbreviation : BMI, Body Mass Index
1Number, % in parentheses (all such values).
2Median, 25th and 75th percentile in parentheses (all such val-ues).
3Exchange rate as of May - June 2007 : US1$ = VND17,803. 4n = 98 for 6 - 11.9 mo postpartum and n = 90 for 12 - 18.9 mo post-partum
Table 2 Z- scores and prevalence of undernutrition All 6 - 11.9 mo 12 - 18.9 mo n 188 98 90 WAZ - 1.21!1.011 - 0.89!1.01 - 1.57!0.90 ** HAZ - 1.20!1.06 - 0.94!1.04 - 1.50!1.01 ** WHZ - 0.52!0.88 - 0.21!0.86 - 0.99!0.77 ** Underweight 37 (19.7%)2 14 (14.3%) 23 (25.6%) * Stunting 44 (23.4%) 18 (18.4%) 26 (28.9%) Wasting 10 (5.3%) 3 (3.1%) 7 (7.8%) Abbreviation : WAZ, Weight- for - Age ; HAZ, Height- for - Age ; WHZ, Weight- for - Height
1Mean!SD (all such values).
2Number, % in parentheses (all such values).
*P!0.05 ; ** P!0.01. vs. children aged 6-11.9 month (unpaired
t - test)
Table 3 Incidence of infectious disease during the last 14 days of the survey
Total age group 6 - 11.9 mo 12 - 18.9 mo n 188 98 90 Diarrhea acute diarrhea 23 (12.2%)1 10 (10.2%) 13 (14.4%) dysentery 5 (2.7%) 2 (2.0%) 3 (3.3%) chronic diarrhea 1 (0.5%) 1 (1.0%) 0 (0.0%) Acute Respiratory Infectious
disease
cough and difficult
breath-ing 38 (20.2%) 21 (21.4%) 17 (18.9%) bronchial infection 5 (2.7%) 2 (2.0%) 3 (3.3%) pneumonia 11 (5.9%) 8 (8.2%) 3 (3.3%) throat infection 15 (8.0%) 8 (8.2%) 7 (7.8%) nose infection 3 (1.6%) 4 (2.0%) 2 (1.1%) 1Number, % in parentheses (all such values).
during the last 14 days of the interview. The inci-dence of diarrhea and ARI was 12.2% and 20.2%, re-spectively. The incidence of diarrhea and ARIs did not differ for older children and younger children. There was no child with measles or pertussis during the time of the survey.
Ninety nine percent of the children had been breastfed or were being breastfed at the time of in-terview. The percentage of currently breastfed chil-dren was 99.0% among those aged 6 to 11.9 mo, while that was 73.3% among those aged 12 to 18.9 mo. Breastfeeding status in the first 4 and 6 mo is shown in Table 4. In the first 4 mo, 21.3% of the
children were exclusively breastfed and 18.6% were almost exclusively breastfed. The prevalence of ex-clusively and almost exex-clusively breastfed children declined rapidly as at 6 mo, there was no child who had been exclusively breastfed and only 3.2% who were almost exclusively breastfed, while the per-centage of partially breastfed children increased to 95.2%.
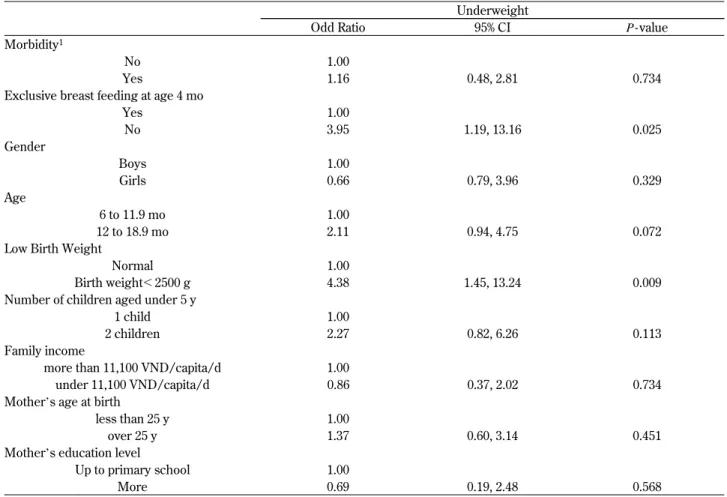
A logistic regression model was used to identify the risk factors related to a child’s underweight (Table 5). As independent variables, incidence of in-fectious disease, exclusive breastfeeding in the first 4 mo, gender, age of children, low birth weight, number of children age under 5 y, family income, mother’s age and mother’s education level were ap-plied. For the analysis, incidence of infectious dis-ease was defined if the child had diarrhea or ARIs. Exclusive breastfeeding was defined if the child had exclusive breastfeeding or almost exclusive breast-feeding in the first 4 mo. Non-exclusive breastfeed-ing in the first 4 mo (OR 3.95, p=0.025) and low birth weight (OR 4.38, p=0.009) were associated with underweight in the children, while incidence of infectious disease was not (OR 1.16, p=0.734). Table 4 Breastfeeding status (Total n = 188)
Breastfeeding Breastfeeding at age 4 mo at age 6 mo Exclusive 40 (21.3%)1 0 (0%) Almost exclusive 35 (18.6%) 6 (3.2%) Predominant 4 (2.1%) 2 (1.1%) Partial 108 (57.4%) 179 (95.2%) Artificial 1 (0.5%) 1 (0.5%) 1Number, % in parentheses (all such values).
Table 5 Odds ratio of the risk factors for underweight (Total n = 188)
Underweight
Odd Ratio 95% CI P - value
Morbidity1
No 1.00
Yes 1.16 0.48, 2.81 0.734
Exclusive breast feeding at age 4 mo
Yes 1.00 No 3.95 1.19, 13.16 0.025 Gender Boys 1.00 Girls 0.66 0.79, 3.96 0.329 Age 6 to 11.9 mo 1.00 12 to 18.9 mo 2.11 0.94, 4.75 0.072
Low Birth Weight
Normal 1.00
Birth weight!2500 g 4.38 1.45, 13.24 0.009
Number of children aged under 5 y
1 child 1.00
2 children 2.27 0.82, 6.26 0.113
Family income
more than 11,100 VND/capita/d 1.00
under 11,100 VND/capita/d 0.86 0.37, 2.02 0.734
Mother’s age at birth
less than 25 y 1.00
over 25 y 1.37 0.60, 3.14 0.451
Mother’s education level
Up to primary school 1.00
More 0.69 0.19, 2.48 0.568
DISCUSSION
To our knowledge, this is the first study to assess the nutritional status, feeding practice and incidence of infectious diseases simultaneously in order to de-termine the risk of undernutrition among children aged 6 to 18 mo in northern mountainous Vietnam. In mountainous areas, the prevalence of undernu-trition among children is remarkably higher com-pared to other regions (19). Growth faltering in Vi-etnam occurs early in their life and the prevalence of undernutrition accumulates with age; it starts from 3 to 4 mo of age and increases quickly from 6 to 12 mo of age, then obtains the highest level at age 24 mo (20); therefore, early prevention and control of undernutrition are expected. The present study in-dicated that high prevalence of undernutrition in terms of underweight, stunting and wasting among children aged 6 to 18 mo in northern mountainous Vietnam. Non-exclusive breastfeeding status in the first 4 mo and low birth weight were predictors for the child undernutrition, while incidence of infec-tious disease was not.
The prevalence of underweight and stunting in the study site were relatively lower compared to those nationwide as well as a previous report in Bac Giang province on children under 5 y (4). This was due to the fact that the prevalence of malnutrition was relatively higher among children older than 12 mo compared to younger children, which is consis-tent with a previous report of Vietnam (21), and that our study participants were relatively younger than those in the previous reports. Another report on Vi-etnamese children of the same age in a mountainous region demonstrated a similar prevalence of under-nutrition (22). Additionally, using the recent WHO growth reference resulted both in a difference in mean Z scores for WAZ and WHZ and in changes in the prevalence of stunting and underweight. The dif-ferences in results between the WHO/CDC/NCHS growth reference and the recent WHO growth ref-erence were similar to those in a previous report in Vietnam (23).
Since suitable and low-cost alternatives to breast-feeding are not available and non-breast milk food such as unhygienic water and low nutrient-density food has several problems in most of developing countries, WHO (24) has recommended giving only breast milk during the first 4 to 6 mo. The benefits of exclusive breastfeeding in the first 6 mo for the child’s nutritional status were also reported both in industrialized countries and developing countries
(25). In this study, non-exclusive breastfed children in the first 4 mo had 3.95 times higher incidence of underweight (P=0.025). The result supports the previous findings that Vietnamese children who were not exclusively breastfed or predominantly breastfed in the first 4 mo showed significantly lower anthropometric measurements at the age of 6 to 12 mo than the children who were exclusively or pre-dominantly breastfed (5). It has been reported that an ideal method of identifying exclusive breastfeed-ing is a descriptive longitudinal and prospective study design with an indicator of “exclusively breast-feeding since birth” (26). In this study, we devel-oped a standardized definition of exclusive breast feeding status following the definition that WHO has proposed (17), while we determined the status by retrospectively asking the time of introduction of non-breast milk food. Since this study has a cross-sectional design, the assessments might have retro-spective bias. Although we could not draw a direct epidemiological inference for causality between ex-clusive breastfeeding and underweight, our findings indicate that advantages of the practice of exclusively breastfeeding would include amelioration of under-nutrition among the children. Exclusive breastfeed-ing has been recommended through a childhood undrernutrition control program provided by the government of Vietnam since 2000 to the present and covering all communes in the country (27) ; however, the percentage of mothers giving exclu-sive breastfeeding in the first 4 mo is still low in Vietnam and even lower than the global rate : 51% (28). In the present study, chronic energy malnu-trition among mothers was also highly prevalent and mothers complained that “the child appeared hun-gry just after breastfeeding” and gave this as the reason for non-exclusive breastfeeding (data not shown). Further efforts to scale-up exclusive breast-feeding, such as monitoring and evaluation with a feedback system that allow for periodic program corrections and continued innovation (29), are ex-pected.
As to the other risk factors of underweight in this study, low birth weight was the strong predictor of underweight. This observation is consistent with the findings of other studies in Vietnam (21) and other Asian countries (30, 31). In Vietnam, thanks to the economic improvement during the last two decades, the prevalence of low birth weight has been decreas-ing, especially in urban areas ; however, the preva-lence of low birth weight remains high in rural areas (32). It has been demonstrated that the identification
in an early stage and immediate direct interven-tion such as extra macro- and micro-nutriinterven-tion can help infants of low birth weight catch up with their heavier contemporaries (33). It has been also shown that appropriate breastfeeding and the quality of breast milk are also important to catch up to the nor-mal nutritional status (34).
Although a marked negative relationship between diarrhea and the physical growth of children has been demonstrated in clinical and epidemiological studies (35-38) and the relative risk of diarrhea mor-tality is significantly increased for malnourished chil-dren especially among chilchil-dren aged 6 to 11 mo (39), this relationship was not observed in the pre-sent study. Since the incidence of diarrhea has sea-sonal variation and the survey was conducted in May, colder and drier season with a lower incidence of diarrhea, a further prospective longitudinal sur-vey is needed.
In addition, socioeconomic factors such as older age, male gender, higher number of children aged under 5 yrs, lower family income, young mothers’ age at giving birth and mothers’ poor education those observed association with childhood undernu-trition in previous studies in Vietnam (19, 21) and also in other Asian countries (27, 28, 40-42) were assumed to be predictors of childhood underweight in the present study. However, we did not observe any association between these socioeconomic factors and children’s underweight in the logistic regres-sion model. For economic status, inequality of in-come was reported in Vietnam and it was the low-est in the northern mountainous area compared to other regions (43). The mean family income in the present study was similar to the reported income in northern mountainous areas : 10.9000 VND (40). Significant association between economic status and childhood undernutrition has been observed when across different economic areas are plotted (19) ; however, the present study was conducted in a par-ticular rural mountainous area, and the difference of family income might be too small to show the significant association to childhood underweight. Mother’s young age at birth was assumed to be a risk factor for underweight because of lack of ex-perience in child care ; however, younger mothers in the study area usually lived with their parents and could have support from them. Therefore the mother’s younger age at birth may not be a risk fac-tor for the childhood underweight. Lower educa-tion is considered to create difficulties in accessing skills, information and health care services (44), and
several previous studies have reported a relationship between the mother’s education level and the child-hood underweight ; however, the small sample size may limit the opportunity to observe such a statis-tical association in the present study.
Other factors such as vitamin A deficiency, zinc deficiency and anemia continue to be serious prob-lem in the public health of preschool children, par-ticularly in children aged under 2 y in mountainous areas, and contribute to underweight in this popu-lation (22, 45). A further research is needed to as-sess their micronutrient status and efficacy of nu-tritive intervention for children aged under 2 y to be considered in the health system in northern moun-tainous Vietnam.
ACKNOWLEDGEMENT
We would like to thank the study participants for their cooperation, and the staff in the district health center in Yen The and the community health centers in Bo Ha commune, Bo Ha town, An Thuang and Tien Thuang, and the staff of the National Institute of Nutrition for their cooperation and organization of the field data collection. We also would like to thank Andrew R. Durkin, Indiana University, Bloomington (USA), for his assistance in reviewing the manuscript.
REFERENCES
1. Murray CJL, Laakso T, Shibuya K, Hill K, Lopez AD : Can we achieve Millennium Devel-opment Goal 4? New analysis of country trends and forecasts of under - 5 mortality to 2015. Lancet 370 : 1040-54, 2007
2. Caulfield LE, de Onis M, Blössner M, Black RE : Undernutrition as an underlying cause of child deaths associated with diarrhea, pneumo-nia, malaria, and measles. Am J Clin Nutr 80 : 193-8, 2004
3. United Nation Child’s Fund (UNICEF). The State of the World’s Children. Oxford Univer-sity Press, New York, 1988
4. National Institute of Nutrition-General Statis-tical Office. Nutritional status of children and their mothers in 2005. Medical publishing house, Hanoi, 2006
5. Hop LT, Gross R, Giay T, Sastroamidjojo S, Schultink W, Lang NT : Premature complemen-tary feeding is associated with poorer growth of
Vietnamese children. J Nutr 130 : 2683-2690, 2000
6. Helena P, Dirk GS, David RM, Kirk AD, Tran TH, Tran TL : Effect of an integrated child nu-trition intervention on the complementary food intake of young children in rural north Viet Nam. Food Nutr Bull 23(4) : 62-69, 2002 7. Sripaipan T, Schroeder DG, Marsh DR, Pachon
H, Dearden KA, Ha TT, Lang TT : Effect of an integrated nutrition program on child morbid-ity due to respiratory infection and diarrhea in northern Viet Nam. Food Nutr Bull 23(4) : 70-7, 2002
8. Black RE, Allen LH, Bhutta ZA, Caulfield LE, de Onis M, Ezzati M, Mathers C, Rivera J, for the Maternal and Child Undernutrition Study Group : Maternal and child undernutrition : global and regional exposures and health con-sequences. Lancet 371 : 243-60, 2008
9. Bhutta ZA, Ahmed T, Black RE, Cousens S, Dewey K, Giugliani E, Haider BA, Kirkwood B, Morris SS, Sachdev HPS, Shekar M, for the Maternal and Child Undernutrition Study Group : What works? Interventions for maternal and child undernutrition and survival. Lancet 371 : 417-40, 2008
10. Bryce J, Coitinho D, Darnton-Hill I, Pelletier D, Pinstrup-Andersen P, for the Maternal and Child Undernutrition Study Group : Maternal and child undernutrition : effective action at na-tional level. Lancet 371 : 510-26, 2008
11. Morris SS, Cogill B, Uauy R, for the Maternal and Child Undernutrition Study Group : Effec-tive international action against undernutrition : why has it proven so difficult and what can be done to accelerate progress? Lancet 371 : 608-21, 2008
12. Gibson RS : Principles of nutrition assessment. Oxford University Press, New York, 1990 13. Dibley MJ, Staehling N, Neiburg P, Towbridge
FL : Interpretation of Z-score anthropometric indicators derived from the international growth reference. Am J Clin Nutr 46 : 749-762, 1987 14. World Health Organization (WHO). WHO
child growth standards : length/height for -age, for--age, for-length, weight-for-height and body mass-index-for-age. Meth-ods and development. WHO Press, Geneva, 2006
15. WHO. Physical status : the use and interpreta-tion of anthropometry. WHO Technical Report Ser 854. WHO Press, Geneva, 1995
16. WHO. WHO recommended surveillance stan-dards, Second edition. WHO Press, Geneva, 1999
17. WHO. Indicators for assessing breast-feeding practices. WHO/CDC/SER 91 14. WHO Press, Geneva, 1991
18. Center for Disease Control (CDC). Impact of New WHO Growth Standards on the Preva-lence of Acute Malnutrition and Operations of Feeding Programs---Darfur, Sudan, 2005-2007. Morbidity and Mortality Weekly Report. Cen-ters for Disease Control and Prevention, 2009. http : / / www . cdc . gov / mmwr / preview / mmwrhtml/mm5821a4.htm
19. Khan NC, Tuyen LDT, Ngoc TX, Duong PH, Khoi HH : Reduction in childhood malnutrition in Vietnam from 1999 to 2004. Asia Pac Clin Nutr 16(2) : 274-278, 2007
20. National Institute of Nutrition-General Statis-tical Office. 2000-Vietnam Child and Mother Nutrition Situation. Medical publishing house, Hanoi, 2001
21. Hien NN, Kam S : Nutritional status and char-acteristics related to malnutrition in chidren un-der five years of age in Nghean, Vietnam. J Prev Med Public Health 41(4) : 232-240, 2008 22. Ninh NX : High prevalence of anemia, zinc and
sub-clinical vitamin A deficiency in Infants from 5 to 8 mo of age in a district in the Northern mountainous area in Vietnam”. Medical Prac-tic Journal 456 : 9-12, 2003 (in Vietnamese) 23. Fenn B, Penny ME : Using the new world
health organisation growth standards : differ-ences from 3 countries. J Pediatr Gastroenterol Nutr 46 : 316-321, 2008
24. WHO. Complementary feeding of young chil-dren in developing countries : a review of cur-rent scientific knowledge. WHO Press, Geneva, 1998
25. WHO. Global data bank on breast-feeding : breast feeding-the best start in life. WHO Press, Geneva, 1996
26. Aarts C, Kylberg E, Hornell A, Hofvander Y, Medhin MG, Greiner T : How exclusive is ex-clusive breastfeeding? A comparison of data since birth with current status data. Int J Epi-demiol 29 : 1041-1046, 2000
27. National Institute of Nutrition Vietnam. Plan of implementation of child malnutrition programme in 2004. Hanoi, 2004
28. UNICEF : Infant and young child feeding (2000-2007).
http : //www.childinfo.org/breastfeeding_ countrydata.php (Access : 2009/09/01) 29. Bhandari N, Kabir AK, Salam MA :
Main-streaming nutrition into maternal and child health programmes : scaling up of exclusive breastfeeding. Matern Child Nutr 4(Suppl 1) : 5-23, 2008
30. Nojomi M, Tehrami A, Aradi SN : Risk analy-sis of growth failure in under-5-year children. Arch Iranian Med 7(3) : 195-200, 2004
31. Ricci JA, Becker S : Risk factors for wasting and stunting among children in Metro Cebu, Philippines. Am J Clin Nutr 63(6) : 966-975, 1996
32. Hop LT : Secular trend in size at birth of Viet-namese newborns during the last 2 decades (1989-2000). Asia Pac Clin Nutr 12 : 266-270, 2003
33. Diamond ID, Abd EL-Aleem AM, Ali MY, Mostafa SAM, EI-Nashar SMA, Guidotti RJ : The relationship between birth weight, and arm and chest circumference in Egypt (brief re-port). J Trop Pediatr 37 : 323-6, 1991
34. Li Y, Liu J, Liu F, Guo G, Anme T, Ushijima H : Maternal child-rearing behaviors and correlates in rural minority areas of Yunnan, China. J Dev Behav Pediatr 21 : 114-22, 2000
35. Scrimshaw NS, taylor CE, Goldon JE : Interac-tions of nutrition and infection. WHO mono-graph series no. 57. WHO Press, Geneva, 1968 36. Tomkins AM, Garlick PJ, Schofield NW, Waterlow JC : The combined effects of infection and malnutrition on protein metabolism in chil-dren. Clin Sci 65 : 313-324, 1983
37. Briend A, Bari A : Critical assessment of the use of growth monitoring for identifying high risk children in primary health care programs. BMJ 298 : 1607-1611, 1989
38. Keusch GT : Malnutrition, infection, and im-mune function. In : Suskind RM, ed. Lewinter-Suskind L. The malnourished child. Nestle Nu-trition Workshop Series, Vol 19. Raven Press, Vevey : Nestec, Newyork, 1990, pp. 37-55 39. Yoon PW, Black RE, Moultan LH, Becker S :
The effect of malnutrition on the risk of diar-rhoeal and respiratory mortality in children!2 years of aga in Cebu, Philippines. Am J Clin Nutr 65 : 1070-1077, 1997
40. Li Yan, Guo G, Shi A, Li Y, Anme T, Ushijima H : Prevalence and correlates of malnutrition among children in rural minority areas of China. Pediatr Int 41(5) : 549-556, 1999
41. Phengxay M, Ali M, Yagyu F, Soulivanh P, Kuroiwa C, Ushijhima H : Risk factors for pro-tein-energy malnutrition in children under 5 years : Study from Luangprabang province, Laos. Pediatr Int 49 : 260-265, 2007
42. Singh GCP, Nair M, Grubesic RB, Connell FA : Factors associated with underweight and stunt-ing among children in rural Terai of eastern Nepal. Asia Pac J Public Health 21 : 144-152, 2009
43. General Statistical office of Vietnam : Monthly average income per capita at current prices by residence and by region. http : //www.gso.gov. vn (Access : 2009/09/01)
44. Lisa CS, Haddad L : Overcoming child malnu-trition in developing countries : past achieve-ment and future choices. International Food Policy Institute, Washington, D.C, 2000 45. Khan NC, Ninh NX, Van Nhien N, Khoi HH,
West CE, Hautvast JG : Sub-clinical vitamin A deficiency and anemia among Vietnamese chil-dren less than five years of age. Asia Pac Clin Nutr 16(1) : 152-157, 2007