* 奈良県立医科大学住居医学講座 Department of Indoor Environmental Medicine, Nara Medical University School of Medicine, Nara, Japan. ** 奈良県立医科大学地域健康医学講座 Department of Community Health and Epidemiology, Nara Medical University School of Medicine, Nara, Japan.
温熱・光住環境と血圧モーニングサージおよび
夜間血圧変動に関する横断研究
大 林 賢 史
*佐 伯 圭 吾
**A CROSS-SECTIONAL STUDY FOR THE ASSOCIATION BETWEEN
THERMAL/LIGHTING ENVIRONMENTS AND BLOOD
PRESSURE VARIABILITY
Kenji Obayashi and Keigo Saeki
SUMMARY
Objective: The purpose of this observational study was to evaluate the association between the thermal environ-ment after wake-up and morning blood pressure surge, and the association among the lighting environenviron-ment during daytime and nighttime, endogenous melatonin levels and nocturnal blood pressure decline.
Methods: We measured the following variables, twice in different seasons, among elderly individuals living in Nara prefecture in Japan: exposed temperature, exposed light levels, ambulatory blood pressure, overnight urine melatonin levels and physical activity evaluated by actigraphy. We defined morning blood pressure surge as aver-age systolic blood pressure in 2 hours after wake-up time minus averaver-age of three systolic blood pressure readings centered on the lowest sleeping reading (sleep trough blood pressure surge). Nocturnal blood pressure decline was defined as percentage nighttime systolic blood pressure decline compared with daytime systolic blood pressure. We also defined a blunted nocturnal blood pressure decline as a less than 10% of nocturnal blood pressure decline. Results: Univariate linear regression analysis showed significant association between sleep trough blood pres-sure surge and exposed temperature after wake-up. In addition, multivariate-multilevel linear regression model indicated significant and inverse association between sleep trough blood pressure surge and exposed temperature after wake-up independent of repeated rank of ambulatory blood pressure monitoring, age, body mass index, smoking status (current or non-current) and physical activity after wake-up. Next, participants were divided into two groups (high and low daytime light exposure groups) by the cutoff value for identifying the top quintile. Crude logistic regression analyses showed marginal to significant association of the high melatonin levels (top quintile) with habitual drinker (everyday vs. non-everyday), higher daytime light exposure (high vs. low) and total sleep time (≥ 6 vs. < 6 hr). In multivariate analysis adjusted for age (≥ 70 vs. < 70 years), habitual drinker, higher daytime light exposure and total sleep time, the odds ratio for the high melatonin levels in the high daytime light exposure group was significantly higher than that in the low daytime light exposure group. Finally, partici-pants were divided into two groups (high and low melatonin groups) by the cutoff value for identifying the top 平成 22 年度 pp.11∼22(2012.3)
緒 言 疫学研究では、冬季に心疾患や脳卒中による死 亡が増加し、他の季節に比べて総死亡の相対危 険が 20%上昇する冬季過剰死亡が認められてい る。これは外気温の低さではなく、住居の断熱設 備や暖房設備の整備状況に依存するとされること から、冬季の室温低下が死亡率上昇に寄与してい ることが考えられる1,5,6)。小サンプルによる生理 学実験では皮膚温を低下させた場合の血圧上昇 が確認されており16)、観察研究では室温が低い 場合の随時血圧の上昇や15)、自由行動下血圧計
(ambulatory blood pressure monitoring; ABPM)に よる調査では、外気温が低い場合の早朝および日 中の血圧上昇が報告されている12)が離床後室温 の低いことが血圧モーニングサージを増加させる という報告はない。 サーカディアン血圧変動により血圧は夜間に最 も低下し、日中に対する夜間の血圧降下率が小さ い群は大きい群と比較して脳卒中・心血管疾患発 症のリスクが高い10,13)。夜間に分泌されるメラト ニンは生体内でさまざまな働きをしており、よく 知られている催眠効果やサーカディアンリズム調 整だけでなく、一酸化窒素(NO)合成を促進し 血圧降下作用を発揮する3)と考えられる。実験 的研究において、日中の光曝露が多いほどメラト ニン分泌が増加し11)、夜間の光曝露が多いほど メラトニン分泌が減少する17)。現代人は日中の 屋内生活時間増加により光曝露量は減少し、夜間 の住居内で使用する人工照明により光曝露量は増 加すると考えられる。したがって、日中光曝露が 少なく夜間光曝露が多い生活をすることは、内因 性メラトニン分泌量を減少させ夜間血圧降下率を 減少させると考えられるが、これまでに住民を対 象にした研究はない。 本研究の目的は①離床後曝露温度と血圧モーニ ングサージの関連、②光曝露量とメラトニン分泌 量の関連、③メラトニン分泌量と夜間血圧降下率 の関連を明らかにすることである。 研 究 方 法 A.対象者 奈良県(生駒市,曽爾村,宇陀市,桜井市)在 住の 60 歳以上の男女 220 名。 B.必要対象者数の算出 横断研究においてα=0.05、1 β=0.8 として、 夜間の光曝露量によって対象者を四分位で 4 群に 分けて、最も夜間光曝露の多い群(Q1)とその他 の群(Q2-4)で比較する場合、Q2-4での夜間血圧 低下率が 10%未満の群(夜間血圧低下不良群) の割合は、我が国の先行研究などから約 40%と 予想された。この場合、検出したい相対危険を 2.5 とすると、Kelsey の方法8)で 208 名、Fleiss の方 法4)で 204 名となり、脱落者の発生や先行研究 における夜間血圧低下不良割合の過大評価の可能 性などを考慮し 220 名の対象者が必要と考えた。 C.調査方法 2010 年 9 月から 2011 年 7 月までの期間に 220 名の対象者宅を訪問し、自由行動下血圧測定・温 度測定・光曝露量測定・血液検査・夜間蓄尿・病 歴聴取・アンケート調査を実施した。すべての対 象者から調査参加の同意書を得て、奈良県立医科 大学医の倫理委員会の承認を得たプロトコールで 実施した (承認番号:301)。
quintile. Crude logistic regression analyses showed marginal to significant association of the blunted nocturnal blood pressure decline with diabetes (yes vs. no), higher melatonin (high vs. low) and frequent nocturia (≥ 1 vs. < 1 times/night). In multivariate analysis adjusted for age (≥ 70 vs. < 70 years), diabetes, higher melatonin and frequent nocturia, the odds ratio for the blunted nocturnal blood pressure decline in the high melatonin group was significantly higher than that in the low melatonin group.
Conclusion: Among elderly individuals, lower exposed temperature after wake-up is associated with higher morning blood pressure surge, and higher daytime light exposure is associated with higher nocturnal melatonin levels. Moreover, higher nocturnal melatonin levels are associated with lower prevalence of blunted nocturnal blood pressure decline.
D.測定項目と測定方法 220 名 の 対 象 者 に つ い て 12:00 か ら 翌 々 日 12:00 までの 3 日間連続で測定を行った。220 名 のうち本解析対象者は季節を変えた 2 回の調査 (冬と秋または春)を完了した 192 名とした。測 定項目と測定方法について以下に示す。 1 .自由行動下血圧 自由行動下血圧計(TM-2431, A&D, Japan)に て 30 分間隔で測定した。 1 )血圧モーニングサージは離床後 2 時間の平 均収縮期血圧睡眠中最低血圧前後 90 分の 平均収縮期血圧から算出し、睡眠トラフ血圧 モーニングサージとした。 2 )夜間血圧降下率は(日中平均収縮期血圧 夜間平均収縮期血圧)/日中平均収縮期血圧 × 100 から算出し、夜間血圧降下率が 10% 未満の者を夜間血圧降下不良と定義した。 2 .曝露温度 時刻と温度を記録する温度ロガー(Thermo-chron, Maxim Integrated Products, USA) を対象者宅 の居間および寝室に設置(床からの高さ 60cm) し 10 分間隔で測定した。外気温は気象庁データ から求め、生活記録の居室・外出記録から曝露温 度を算出した。 3 .光曝露 時刻と照度を記録する照度ロガー(LX-28SD, 佐藤商事 , Japan)を対象者宅の寝室に設置(床か らの高さ 60cm)し 1 分間隔で測定し夜間平均光 曝露量を算出した。照度センサーを搭載したアク チグラフ(Actiwatch 2, Respironics, USA)を対象 者の非利き腕手首に装着して 1 分間隔で日中平均 光曝露量を測定した。 4 .メラトニン分泌量 測定 2 日目の夜間蓄尿(就寝後∼起床直後)か ら尿量および尿中メラトニン代謝産物(6-sulpha-toxymelatonin)濃度を ELISA 法により測定(SRL, Japan)した。メラトニン分泌量は、尿中 6-sul-phatoxymelatonin 濃度(ng/ml)×夜間蓄尿量(ml) から算出した。 5 .睡眠の質・身体活動量
アクチグラフ(Actiwatch 2, Respironics, USA) を対象者の非利き腕手首に装着して 1 分間隔で測 定し総睡眠時間、睡眠効率および身体活動量とし
て日中の 1 分間当たりの平均カウント数を算出し た。
6 .その他
身長および体重から BMI(body mass index)を 算出した。アンケート調査により飲酒・喫煙状況 を聴取し、血液検査で空腹時血糖、HbA1c および クレアチニンを測定した。以前糖尿病と診断され 現在糖尿病治療薬を内服している者あるいは血液 検査で空腹時血糖≥ 126mg/dl かつ HbA1c ≥ 6.1% (JDS 値)の者を糖尿病罹患と定義した。推定糸 球体濾過量(eGFR)は「日本腎臓学会 CKD 診 療ガイド 2009」で推奨されている式9)から算出 した。以前高血圧と診断され現在降圧薬を内服し ている者あるいは 1 回目調査時の自由行動下血圧 測定の結果、日中平均血圧≥ 135/85mmHg あるい は夜間平均血圧≥ 120/70mmHg の者を高血圧罹患 と定義した。また対象者に生活記録を記入しても らい、就寝時間・離床時間・外出時間・夜間排尿 回数を把握した。アンケート調査により geriatric depression scale(GDS-15)日本語版14)のスコア を算出し、軽度うつ状態は GDS スコア≥ 6 と定 義した。住居周辺環境因子の調査には Interna-tional Physical Activity Questionnaire Environmental
Module(IPAQ-E)日本語版7)を用い、基本項目 7 問を解析対象とした。 E.解析方法 正規分布するデータは平均(標準偏差)、正規 分布しないデータは中央値(四分位範囲)を示し た。2 回の調査でそれぞれ測定している曝露温度 および血圧モーニングサージ以外の項目(夜間血 圧降下率,夜間排尿回数,メラトニン分泌量,光 曝露量,総睡眠時間,睡眠効率,日中身体活動量) は各調査回 2 日目のデータを平均して代表値とし た。 血圧モーニングサージ(睡眠トラフ血圧モーニ ングサージ)および夜間血圧降下率の日差変動(連 続する 2 日間の再現性)および季節変動(冬 [11 ∼ 3 月] と春 / 秋 [4 ∼ 7 月 / 9 ∼ 10 月] の平均 4 か月間の再現性)について Pearson 相関係数(rp) を用いて算出した。 曝露温度は生活記録による外出時間および寝室 滞在時間と、居間・寝室の室温または外気温から 求めた。曝露温度が血圧モーニングサージに及ぼ
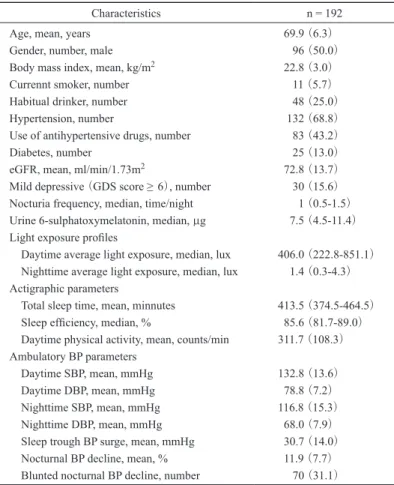
す影響について、睡眠トラフ血圧モーニングサー ジを従属変数、起床後 2 時間の曝露温度(各血圧 測定時の気温の平均)に加えて ABPM の繰り返 し測定順序、年齢、BMI、現在の喫煙習慣の有無、 アクチグラフを用いた身体活動量(起床後 2 時間 の平均値)を説明変数とする多変量マルチレベル 線形回帰分析を用いて解析した。 日中平均光曝露量および夜間平均光曝露量と以 下の項目について 2 群間比較を Mann-Whitney 検 定で行った。年齢(70 歳以上,70 歳未満)、性別 (男性,女性)、BMI(25kg/m2以上,25kg/m2未 満)、喫煙(現在喫煙している,現在喫煙してい ない)、飲酒(毎日飲酒している,毎日飲酒して いない)、年収(400 万円以上,400 万円未満)、 学歴(10 年以上,10 年未満)、高血圧罹患(あり, なし)、糖尿病罹患(あり,なし)、eGFR(60ml/ min/1.73m2以上,60ml/min/1.73m2未満)、夜間排 尿回数(1 回以上,1 回未満)、メラトニン分泌量 (高値 [上位 20%],低値 [下位 80%])、軽度うつ 状態(あり,なし)、総睡眠時間(6 時間以上,6 時間未満)、睡眠効率(80%以上,80%未満)、日 中身体活動量(300 カウント/分以上,300 カウン ト/分未満)、在住エリア(都市部 [生駒市],農 村部 [曽爾村,宇陀市,桜井市])、住宅密度(高い, 低い)、商店へのアクセス(良い,悪い)、公共交 通機関へのアクセス(良い,悪い)、歩道の設置(あ り,なし)、自転車レーンの設置(あり,なし)、 犯罪の安全性(安全,安全でない)。 日中平均光曝露量とメラトニン分泌量の関連 について、後に示す多変量ロジスティック回帰 分析における、日中平均光曝露量を高値(上位 20%)と低値(下位 80%)の 2 群に分ける際 の妥当性を示すため、日中平均光曝露量を五 分位に分けメラトニン分泌量のトレンド検定を Jonckheere-Terpstra 検定2)を用いて行った。同様 に後に示す多変量ロジスティック回帰分析におけ る、メラトニン分泌量を高値(上位 20%)と低 値(下位 80%)の 2 群に分ける際の妥当性を示 すため、メラトニン分泌量を五分位に分け夜間血 圧降下率のトレンド検定を行った。更にメラトニ ン分泌量の第 5 五分位群と第 1 ∼ 4 五分位群の 2 群間で夜間血圧降下率を t 検定で比較した。ロ ジスティック回帰モデルでメラトニン分泌量高値 (上位 20%)の粗オッズ比を推定した。説明変数 は年齢、性別、BMI、喫煙、飲酒、収入、学歴、 高血圧罹患、糖尿病罹患、eGFR、夜間排尿回数、 軽度うつ状態、総睡眠時間、睡眠効率、日中身体 活動量をそれぞれ前述の 2 群カテゴリーにして投 入し、日中平均光曝露量は(高値 [上位 20%], 低値 [下位 80%])の 2 群カテゴリーで投入した。 そのうち、年齢に加えてメラトニン分泌量高値と 関連を認めた(P<0.10)項目をロジスティック回 帰モデルに同時投入し調整オッズ比を推定した。 同様に夜間血圧降下不良の粗オッズ比は、説明変 数に前述の年齢、性別、BMI、喫煙、飲酒、収入、 学歴、高血圧罹患、糖尿病罹患、eGFR、夜間排 尿回数、軽度うつ状態、総睡眠時間、睡眠効率、 日中身体活動量に加えて、降圧薬内服(あり,なし) およびメラトニン分泌量(高値 [上位 20%],低 値 [下位 80%])を 2 群カテゴリーにして投入し た。年齢に加えて夜間血圧低下不良と関連を認め た(P<0.10)項目をロジスティック回帰モデルに 同時投入し調整オッズ比を推定した。 温度および血圧モーニングサージの解析には SPSS for windows ver17 を用い、その他の解析に は SPSS for windows ver19 を用いた。統計学的有 意水準は 5 %未満(P<0.05)とした。 結 果 A.対象者の特性、光曝露量、アクチグラフお よび血圧データ 対象者の特性、光曝露量、アクチグラフおよ び血圧データを表 1 に示す。平均年齢は 69.9 歳 で男女は同数であった。平均 BMI は 22.8kg/m2、 4.9%が現在も喫煙をしており、21.3%が毎日飲 酒をしていた。58.7%が高血圧で 36.9%が降圧薬 を内服していた。11.1%が糖尿病を罹患し、平均 eGFR は 72.8ml/min/1.73m2、13.3%が軽度うつ状 態であり、夜間排尿回数の中央値は 1 回であっ た。メラトニン分泌量は中央値が 7.5µg であり、 日中平均光曝露量の中央値は 406.0 lux、夜間平均 光曝露量の中央値は 1.4 lux であった。平均総睡 眠時間は 413.5 分、睡眠効率の中央値は 85.6%で あり、日中の身体活動量は 1 分間当たり 311.7 カ ウント、日中収縮期血圧は 132.8mmHg、日中拡 張期血圧は 78.8mmHg であった。夜間収縮期血
圧は 116.8mmHg、夜間拡張期血圧は 68.0mmHg であり、睡眠トラフ血圧モーニングサージが 30.7mmHg であった。夜間血圧降下率は 11.9%で あり、夜間血圧降下率が 10%に満たない夜間血 圧降下不良の割合は 31.1%であった。 B.血圧変動の日差変動および季節変動 血圧変動の日差変動および季節変動を表 2 に 示す。冬における睡眠トラフ血圧モーニング サ ー ジ は 測 定 1 日 目 が 34.6mmHg、2 日 目 が 32.7mmHg、覚醒前モーニングサージは測定 1 日 目が 20.8mmHg、2 日目が 17.5mmHg、夜間収縮 期血圧降下率は測定 1 日目が 15.0%、2 日目が 13.0%であった。冬の連続する 2 日間の再現性 は睡眠トラフ血圧モーニングサージで rp=0.36、 夜間血圧降下率で rp=0.62 であった。同様に春 / 秋の連続する 2 日間の再現性は睡眠トラフ血圧 モーニングサージで rp=0.37、夜間血圧降下率で rp=0.58 であった。各季節の測定 1 日目と 2 日目 の平均値を比較した季節間の再現性は、睡眠トラ フモーニングサージで rp=0.40、夜間血圧降下率 で rp=0.52 であった。 C.離床後居室温度と血圧モーニングサージの 関連 単変量線形回帰モデルにおいて、睡眠トラフ血 圧モーニングサージと曝露温度は有意な関連を認 めた。多変量マルチレベル線形回帰モデルにおい て、曝露温度は ABPM の繰り返し測定順序、年齢、 BMI、喫煙状況、身体活動量に独立して、睡眠ト Characteristics n = 192
Age, mean, years 69.9 (6.3)
Gender, number, male 96 (50.0)
Body mass index, mean, kg/m2 22.8 (3.0)
Currennt smoker, number 11 (5.7)
Habitual drinker, number 48 (25.0)
Hypertension, number 132 (68.8)
Use of antihypertensive drugs, number 83 (43.2)
Diabetes, number 25 (13.0)
eGFR, mean, ml/min/1.73m2 72.8 (13.7)
Mild depressive (GDS score ≥ 6), number 30 (15.6)
Nocturia frequency, median, time/night 1 (0.5-1.5)
Urine 6-sulphatoxymelatonin, median, µg 7.5 (4.5-11.4)
Light exposure profiles
Daytime average light exposure, median, lux 406.0 (222.8-851.1)
Nighttime average light exposure, median, lux 1.4 (0.3-4.3)
Actigraphic parameters
Total sleep time, mean, minnutes 413.5 (374.5-464.5)
Sleep efficiency, median, % 85.6 (81.7-89.0)
Daytime physical activity, mean, counts/min 311.7 (108.3)
Ambulatory BP parameters
Daytime SBP, mean, mmHg 132.8 (13.6)
Daytime DBP, mean, mmHg 78.8 (7.2)
Nighttime SBP, mean, mmHg 116.8 (15.3)
Nighttime DBP, mean, mmHg 68.0 (7.9)
Sleep trough BP surge, mean, mmHg 30.7 (14.0)
Nocturnal BP decline, mean, % 11.9 (7.7)
Blunted nocturnal BP decline, number 70 (31.1)
Data are means (SD), medians (inter quartile range) or number (%). Habitual drinker is one who drinks any alcohol every day. eGFR; estimated glomerular filtra-tion rate, BP; blood pressure, SBP; systolic blood pressure, DBP; diastolic blood pressure.
表 1 .対象者特性、光曝露量、アクチグラフおよび血圧データ Table 1.Basic, clinical, light exposure, actigraphic and BP characteristics.
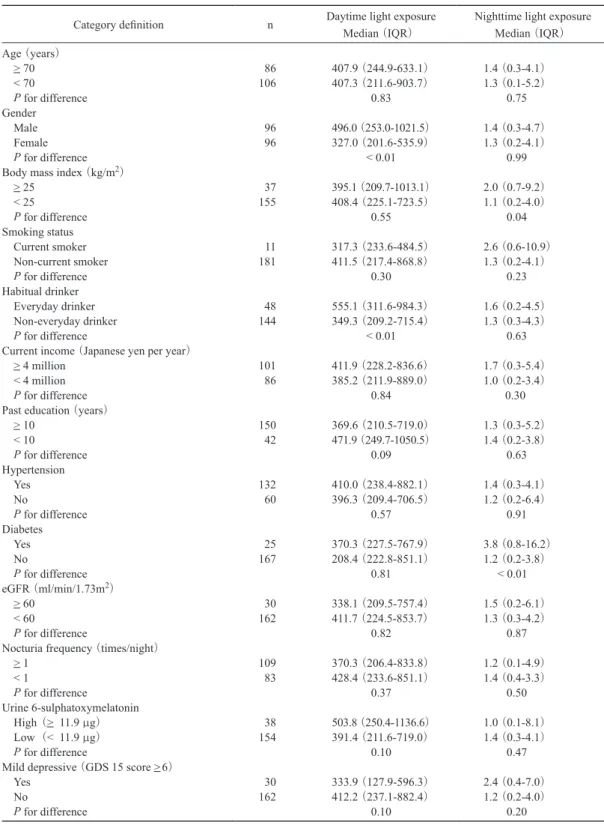
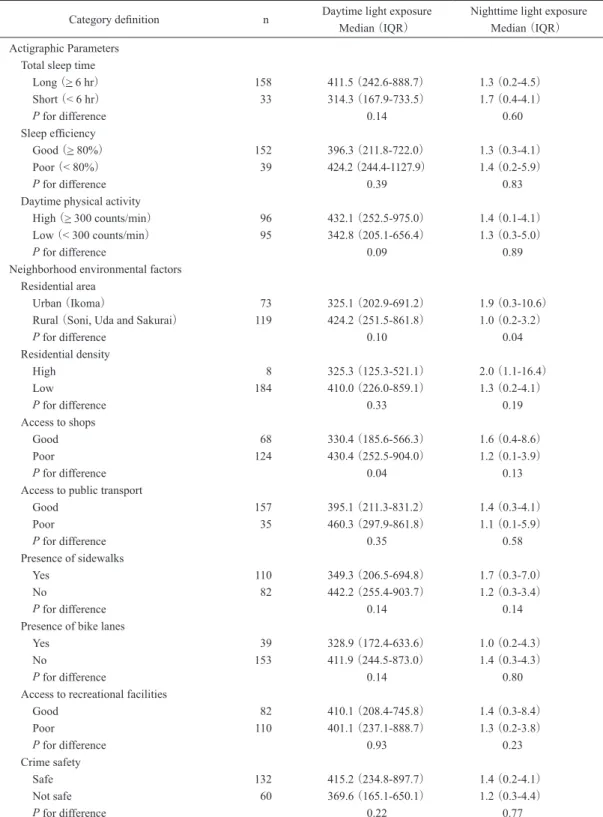
ラフ血圧モーニングサージと有意な負の相関を認 めた(表 3)。 D.光曝露量と対象者特性、睡眠の質、身体活 動量および近隣環境因子の関連 次に日中平均光曝露量および夜間平均光曝露量 と対象者特性項目での 2 群比較を表 4 に示す。日 中平均光曝露量は女性より男性に多く、日常的に 飲酒している群に多かった。学歴が高く、軽度う つ状態の群で日中平均光曝露量は少ない傾向を認 め、メラトニン分泌量高値を呈する群で多い傾向 を認めた。夜間平均光曝露量は BMI が 25kg/m2 以上の肥満群、糖尿病罹患群で多かったが、メラ トニン分泌量の間に明らかな関連は認めなかっ た。同様に睡眠、身体活動量および近隣環境因子 項目での 2 群比較を表 5 に示す。日中平均光曝露 量は商店へのアクセスが悪い群で多く、日中身体 活動量の多い群および農村部在住の群で多い傾向 を認めた。夜間平均光曝露量は都市部在住の群で 多かった。 E.日中平均光曝露量とメラトニン分泌量の関 連 対象者を日中光曝露量で五分位に層別化しメラ トニン分泌量の分布を示した。日中平均光曝露量 が多くなるほどメラトニン分泌量が増加してお り、有意な量反応関係を認めた(P trend=0.026, 図 1)。単変量ロジスティック回帰分析によりメ ラトニン分泌量高値(上位 20%)と関連を認め た項目は、日常飲酒者、日中平均光曝露量高値、 総睡眠時間であった。年齢、日常飲酒者、日中平 均光曝露量高値、総睡眠時間を同時投入した多変 量ロジスティック回帰モデルにおいて、メラトニ ン分泌量高値のオッズは日中平均光曝露量下位 80%より上位 20%で有意に他の因子に独立して 高かった(表 6)。 F.メラトニン分泌量と夜間血圧降下率の関連 対象者をメラトニン分泌量で五分位に層別化し 夜間血圧降下率の分布を示した。単調増加を示す トレンド検定では統計学的には有意ではないもの の(P trend= 0.073,図 2)、メラトニン分泌量の 第 4 五分位を閾値として第 5 五分位群(n=38) は他の第 1 ∼ 4 五分位群(n=154)より夜間収縮 期血圧降下率が有意に増加していた(14.8 6.3% vs. 11.2 7.8% , P<0.01)。単変量ロジスティック 回帰分析により夜間血圧降下不良と関連を認めた 項目は、糖尿病罹患、メラトニン分泌量高値、夜 間頻尿であった。年齢、糖尿病罹患、メラトニン 表 3 .睡眠トラフ血圧モーニングサージと各項目との多変量マルチレベル線形回帰分析結果
Table 3.Results of a multivariate multilevel linear analysis of the relationship between sleep trough blood pressure surge and variables.
β 95%CI P
Repeated rank of monitoring (1st-4th) 1.5 2.4 0.5 <0.01
Age (1 year) 0.5 0.2 0.8 <0.01
Body mass index (per 1 kg/m2) 0.4 0.2 0.9 0.24
Current smoker (yes) 2.1 5.5 9.7 0.59
Physical activity after wake-up (per 100 count/min) 1.5 0.5 2.4 <0.01
Exposed temperature (per 1℃) 0.4 0.6 0.2 <0.01
表 2 .血圧変動の日差変動および季節変動
Table 2.Diurnal and seasonal reproducibility of blood pressure variability.
Winter Spring/Fall Correlation
①day1 ②day2 ③mean ④day1 ⑤day2 ⑥mean ①vs.② ④vs.⑤ ③vs.⑥
Sleep trough BP surge mean (mmHg) 34.6 32.7 33.7 29.0 28.0 28.6 rp 0.36 0.37 0.40
SD 18.9 18.4 15.3 16.0 16.8 13.4 P <0.01 <0.01 <0.01
Nocturnal BP decline (%) mean (%) 15.0 13.0 14.0 12.5 10.5 11.5 rp 0.62 0.58 0.52
SD 10.3 9.4 8.8 10.3 9.5 8.8 P <0.01 <0.01 <0.01
Category definition n Daytime light exposure Median (IQR)
Nighttime light exposure Median (IQR) Age (years) > 70 86 407.9 (244.9-633.1) 1.4 (0.3-4.1) < 70 106 407.3 (211.6-903.7) 1.3 (0.1-5.2) P for difference 0.83 0.75 Gender Male 96 496.0 (253.0-1021.5) 1.4 (0.3-4.7) Female 96 327.0 (201.6-535.9) 1.3 (0.2-4.1) P for difference < 0.01 0.99
Body mass index (kg/m2)
> 25 37 395.1 (209.7-1013.1) 2.0 (0.7-9.2) < 25 155 408.4 (225.1-723.5) 1.1 (0.2-4.0) P for difference 0.55 0.04 Smoking status Current smoker 11 317.3 (233.6-484.5) 2.6 (0.6-10.9) Non-current smoker 181 411.5 (217.4-868.8) 1.3 (0.2-4.1) P for difference 0.30 0.23 Habitual drinker Everyday drinker 48 555.1 (311.6-984.3) 1.6 (0.2-4.5) Non-everyday drinker 144 349.3 (209.2-715.4) 1.3 (0.3-4.3) P for difference < 0.01 0.63
Current income (Japanese yen per year)
> 4 million 101 411.9 (228.2-836.6) 1.7 (0.3-5.4)
< 4 million 86 385.2 (211.9-889.0) 1.0 (0.2-3.4)
P for difference 0.84 0.30
Past education (years)
> 10 150 369.6 (210.5-719.0) 1.3 (0.3-5.2) < 10 42 471.9 (249.7-1050.5) 1.4 (0.2-3.8) P for difference 0.09 0.63 Hypertension Yes 132 410.0 (238.4-882.1) 1.4 (0.3-4.1) No 60 396.3 (209.4-706.5) 1.2 (0.2-6.4) P for difference 0.57 0.91 Diabetes Yes 25 370.3 (227.5-767.9) 3.8 (0.8-16.2) No 167 208.4 (222.8-851.1) 1.2 (0.2-3.8) P for difference 0.81 < 0.01 eGFR (ml/min/1.73m2) > 60 30 338.1 (209.5-757.4) 1.5 (0.2-6.1) < 60 162 411.7 (224.5-853.7) 1.3 (0.3-4.2) P for difference 0.82 0.87
Nocturia frequency (times/night)
> 1 109 370.3 (206.4-833.8) 1.2 (0.1-4.9) < 1 83 428.4 (233.6-851.1) 1.4 (0.4-3.3) P for difference 0.37 0.50 Urine 6-sulphatoxymelatonin High (> 11.9 µg) 38 503.8 (250.4-1136.6) 1.0 (0.1-8.1) Low (< 11.9 µg) 154 391.4 (211.6-719.0) 1.4 (0.3-4.1) P for difference 0.10 0.47
Mild depressive (GDS 15 score >6)
Yes 30 333.9 (127.9-596.3) 2.4 (0.4-7.0)
No 162 412.2 (237.1-882.4) 1.2 (0.2-4.0)
P for difference 0.10 0.20
表 4 .対象者特性による光曝露量の比較
Table 4.Comparisons of light exposure profiles by basic and clinical characteristics.
IQR; interquartile range, eGFR; estimated glomerular filtration rate. Comparisons between the two groups were performed using the Mann-Whitney test.
Category definition n Daytime light exposure Median (IQR)
Nighttime light exposure Median (IQR) Actigraphic Parameters
Total sleep time
Long (> 6 hr) 158 411.5 (242.6-888.7) 1.3 (0.2-4.5) Short (< 6 hr) 33 314.3 (167.9-733.5) 1.7 (0.4-4.1) P for difference 0.14 0.60 Sleep efficiency Good (> 80%) 152 396.3 (211.8-722.0) 1.3 (0.3-4.1) Poor (< 80%) 39 424.2 (244.4-1127.9) 1.4 (0.2-5.9) P for difference 0.39 0.83
Daytime physical activity
High (> 300 counts/min) 96 432.1 (252.5-975.0) 1.4 (0.1-4.1)
Low (< 300 counts/min) 95 342.8 (205.1-656.4) 1.3 (0.3-5.0)
P for difference 0.09 0.89
Neighborhood environmental factors Residential area
Urban (Ikoma) 73 325.1 (202.9-691.2) 1.9 (0.3-10.6)
Rural (Soni, Uda and Sakurai) 119 424.2 (251.5-861.8) 1.0 (0.2-3.2)
P for difference 0.10 0.04 Residential density High 8 325.3 (125.3-521.1) 2.0 (1.1-16.4) Low 184 410.0 (226.0-859.1) 1.3 (0.2-4.1) P for difference 0.33 0.19 Access to shops Good 68 330.4 (185.6-566.3) 1.6 (0.4-8.6) Poor 124 430.4 (252.5-904.0) 1.2 (0.1-3.9) P for difference 0.04 0.13
Access to public transport
Good 157 395.1 (211.3-831.2) 1.4 (0.3-4.1) Poor 35 460.3 (297.9-861.8) 1.1 (0.1-5.9) P for difference 0.35 0.58 Presence of sidewalks Yes 110 349.3 (206.5-694.8) 1.7 (0.3-7.0) No 82 442.2 (255.4-903.7) 1.2 (0.3-3.4) P for difference 0.14 0.14
Presence of bike lanes
Yes 39 328.9 (172.4-633.6) 1.0 (0.2-4.3)
No 153 411.9 (244.5-873.0) 1.4 (0.3-4.3)
P for difference 0.14 0.80
Access to recreational facilities
Good 82 410.1 (208.4-745.8) 1.4 (0.3-8.4) Poor 110 401.1 (237.1-888.7) 1.3 (0.2-3.8) P for difference 0.93 0.23 Crime safety Safe 132 415.2 (234.8-897.7) 1.4 (0.2-4.1) Not safe 60 369.6 (165.1-650.1) 1.2 (0.3-4.4) P for difference 0.22 0.77
IQR; interquartile range. Comparisons between the two groups were performed using the Mann-Whitney test. 表 5 .アクチグラフデータおよび住居周辺環境因子による光曝露量の比較
分泌量高値、夜間頻尿を同時投入した多変量ロジ スティック回帰モデルにおいて、夜間血圧降下不 良のオッズはメラトニン分泌量下位 80%より上 位 20%で有意に他の因子に独立して高かった(表 7)。 考 察 本研究の結果、離床後曝露温度と血圧モーニン グサージの間に有意な負の関連を認め、日中平均 光曝露量とメラトニン分泌量の間に正の関連を認
Covariates Crude OR (95% CI) P Adjusted OR§ (95% CI) P
Age (>70 vs. < 70 years) 0.76 (0.37-1.57) 0.46 0.72 (0.34-1.53) 0.40
Habitual drinker (everyday vs. non-everyday) 2.06 (0.96-4.41) 0.06 1.90 (0.86-4.18) 0.11
Daytime average light exposure (high vs. low) 2.68 (1.21-5.94) 0.02 2.32 (1.02-5.26) 0.04
Total sleep time (long vs. short) 4.57 (1.04-20.0) 0.04 4.27 (0.95-19.1) 0.06
表 6 .メラトニン分泌量高値の粗オッズ比および調整オッズ比 Table 6.Crude and adjusted odds ratios for high urine 6-sulphatoxymelatonin.
§Adjusted for all covariates shown. OR; odds ratio, CI; confidence interval. High urine 6-sulphatoxymelatonin is difined as top quintile of urine 6-sulphatoxymelatonin. High daytime average light exposure is defined as top quintile of daytime average light exposure.
Covariates Crude OR (95% CI) P Adjusted OR¶ (95% CI) P
Age (>70 vs. < 70 years) 1.42 (0.79-2.67) 0.25 1.12 (0.60-2.10) 0.73
Diabetes (yes vs. no) 2.07 (0.89-4.84) 0.09 1.68 (0.69-4.06) 0.25
Urine 6-sulphatoxymelatonin (high vs. low) 0.39 (0.17-0.91) 0.03 0.36 (0.15-0.86) 0.02
Nocturia frequency (>1 vs. < 1 times/night) 2.22 (1.20-4.11) 0.01 2.28 (1.19-4.37) 0.01
表 7 .夜間血圧降下不良の粗オッズ比および調整オッズ比 Table 7.Crude and adjusted odds ratios for blunted nocturnal blood pressure decline.
¶Adjusted for all covariates shown. OR; odds ratio, CI; confidence interval. Blunted nocturnal blood pressure decline is defined as less than 10% decline in nighttime systolic blood pressure compared with daytime systolic blood pressure. High urine 6-sul-phatoxymelatonin is difined as top quintile of urine 6-sul6-sul-phatoxymelatonin.
図 1 .日中平均光曝露量ごとのメラトニン分泌量の分布 Fig.1.Distribution of urine 6-sulphatoxymelatonin by daytime
average light exposure levels.
The P value is shown for the trend identified by the Jonckheere-Terpstra test2). Solid bars indicate the median urinary melatonin
excretion, and error bars indicate the upper half of the inter-quartile (75th percentile). Q1 (n=38) [51.0− 205.1] Q2 (n=38) [206.0− 317.3] Q3 (n=39) [319.9− 462.4] Q4 (n=39) [483.5− 975.6] Q5 (n=38) [981.0− 4802.2] (range, lux)
Daytime average light exposure levels
Urine 6-sulphatoxymelatonin levels
(μg, median, 75 percentile) P for trend=0.026 12.5 10 7.5 5 2.5 0 図 2 .メラトニン分泌量ごとの夜間血圧降下率の分布 Fig.2.Distribution of percentage nocturnal blood pressure
decline by urine 6-sulphatoxymelatonin levels.
The P value is shown for the trend identified by the Jonckheere-Terpstra test2). Solid bars indicate the mean percentage nocturnal
blood pressure decline, and error bars indicate the upper half of the 95% confidence intervals.
Percentage nocturnal blood pressure decline
(%, mean, 95% CI) 図 1 図 2 図 3 図 4 図 5 0 5 15 20 10 P for trend=0.073 Q1 (n=38) [1.4− 4.1] Q2 (n=39) [4.2− 6.5] Q3 (n=39) [6.5− 9.2] Q4 (n=38) [9.2− 11.8] Q5 (n=38) [11.9− 43.9]
Urine 6-sulphatoxymelatonin levels
め、更にメラトニン分泌量と夜間血圧降下率の間 に正の関連を認めた。 血圧モーニングサージと曝露温度の関連は、睡 眠トラフ血圧モーニングサージに関して曝露温度 が ABPM の繰り返し測定順序、年齢、BMI、喫 煙状況、身体活動量に独立して有意な負の相関を 認めたことにより示された(表 3)。血圧モーニ ングサージの季節変動の報告はあるが、居室温度 と血圧モーニングサージの関連を調査した報告は ない。室温による変動は、同指標の再現性がやや 低い一因と考えられる。更に今回の結果は、脳卒 中のリスクファクターである血圧モーニングサー ジを室温のコントロールによって抑制できる可能 性を示唆する結果であり、今後の臨床研究が待た れる。 日中平均光曝露量とメラトニン分泌量の関連 は、メラトニン分泌量高値(上位 20%)のオッ ズが日中平均光曝露量上位 20%で下位 80%より、 年齢、日常飲酒者、総睡眠時間に独立して有意に 高かったことにより示された(表 6)。その関連 は日中平均光曝露量とメラトニン分泌量の間の量 反応関係により強く裏付けられている。国内外の 先行研究において、住民を対象に客観的光曝露量 の測定とメラトニン分泌量の測定を同時測定した 研究はほとんどなく、小サンプル(n=20)の高 齢者に日中の高照度光曝露によりメラトニン分泌 量が増加したという先行研究11)と同様の結果を 192 名のサンプルサイズで得た意義は大きいと考 えられる。メラトニンは生体内でさまざまな働き をしており、よく知られている催眠効果やサーカ ディアンリズム調整だけでなく、抗癌作用や免疫 賦活化作用などにも関与していると考えられてい る3)。本研究の結果から屋外および住居内におい て日中平均光曝露量を調整することでメラトニン 分泌量を増加させることができる可能性があり、 睡眠障害や概日リズム障害のみならず発癌予防な どもできる可能性が示唆された。 本解析からは夜間平均光曝露量とメラトニン分 泌量の間に明らかな関連は認めなかった。その理 由の 1 つに全体の約 60%の対象者が平均 3 lux 未 満の dim light 下で睡眠しており、100 lux 以上曝 露されている対象者は全体の 1%に留まっていた ことがあげられる。先行実験研究17)において 3 lux の夜間光曝露でも 11%のメラトニン分泌抑制 作用があり、106 lux では 88%のメラトニン分泌 抑制作用があるとされている。条件を揃えた実験 研究では弱い光曝露でも十分にメラトニン分泌を 抑制されるが、本研究は観察研究であり条件は揃 えておらず、このサンプルサイズでは差を見いだ すための統計学的検出力が弱かったと考えられた。 次にメラトニン分泌量と夜間血圧降下率の関連 は、夜間血圧降下不良のオッズがメラトニン分泌 量上位 20%で下位 80%より、年齢、糖尿病罹患、 夜間頻尿に独立して有意に高かったことにより 示された(表 7)。メラトニン分泌量の第 4 五分 位を閾値として第 5 五分位群(n=38)は他の第 1 ∼ 4 五分位群(n=154)より夜間収縮期血圧降下 率が有意に増加していたが、単調増加を示すトレ ンド検定では統計学的に有意な関連は認めなかっ た(P=0.073)。サンプル数不足のために有意な関 連を検出できなかった可能性があると考えられ今 後の課題である。国内外の先行研究において、内 因性メラトニン分泌量と夜間血圧降下率の関連を 調査した研究はほとんどなく、192 名のサンプル サイズで夜間血圧降下不良の潜在的交絡因子であ る糖尿病罹患や夜間頻尿回数を同時調整し、関連 を認めた点で本研究の意義は大きい。先に示した ように、メラトニン分泌量は日中平均光曝露量増 加により増加する可能性があり、日中平均光曝露 量を増やすという生活習慣改善により脳卒中や心 疾患のリスクになる夜間血圧降下不良を減少させ られる可能性が示唆された。 光曝露量と対象者特性の関連の解析から、肥満 例や糖尿病例で夜間平均光曝露量が多かったこと は興味深い。本研究は農村部と都市部の対象者が 混在しており生活パターンの違いが交絡となって いる可能性があり、実際に農村部在住者では日中 平均光曝露量が多い傾向を認め、夜間平均光曝露 量は少なかった。しかし、農村部で糖尿病罹患が 少ないということはなかった(データは示してい ない)。農村部在住者は日中にしっかり光を浴び て、夜間は光を浴びない、光曝露量振幅の大きい 生活パターンであり、サーカディアンリズムを規 則正しく形成する理想的なものであると考えられ る。都市部在住者のなかでもこのパターンをとっ ている対象者も多い。今後コホート調査として脳
卒中・心疾患・癌の発症や死亡率をフォローする ことで、光曝露や温度曝露と健康の関連をより強 く説明できると考えている。 総 括 本研究は奈良県在住の高齢者を対象に温熱環境 と血圧モーニングサージの関連および光環境、メ ラトニン分泌量と夜間血圧降下率の関連を検討し た。本研究の結果、離床後曝露温度と血圧モーニ ングサージの間に負の関連を認め、日中平均光曝 露量とメラトニン分泌量の間に正の関連を認め、 更にメラトニン分泌量と夜間血圧降下率の間に正 の関連を認めた。 本研究の結果は脳卒中や心疾患のリスク因子で あるサーカディアン血圧変動を温熱環境および光 環境という普遍性の高い要因を調整することで改 善できることを示唆したものであり、社会的意義 は大きい。更に睡眠障害や癌発症などにかかわる 内因性メラトニン分泌と光環境の関連を示したこ とは、疾病予防の観点からやはり重要性は高いと いえる。今後、更に大規模なサンプルサイズで疾 病発症や死亡について追跡調査を行うことで温熱 光環境と健康問題についてより多くのことが説明 できると確信している。 謝 辞 本研究実施にあたり調査補助業務を献身的に行ってくれ た研究補助員の上村幸子さん、竹中直美さんに感謝いたし ます。また生駒市自治会、曽爾村役場、宇陀市保健センター、 桜井市老人会の皆様に多大なるご協力をいただきました。 本研究は財団法人明治安田厚生事業団第 27 回健康医科学 研究助成の支援を賜りました。ここに記して深謝いたしま す。 参 考 文 献
1)Aylin P, Morris S, Wakefield J, Grossinho A, Jarup L, Elliott P (2001): Temperature, housing, deprivation and their rela-tionship to excess winter mortality in Great Britain, 1986-1996. Int J Epidemiol, 30, 1100-1108.
2)Bewick V, Cheek L, Ball J (2004): Statistics review 10: further nonparametric methods. Crit Care, 8, 196-199. 3)Brzezinski A (1997): Melatonin in humans. N Engl J Med,
336, 186-195.
4)Fleiss JL (1981): Statistical methods for rates and propor-tions. John Wiley & Sons, New York.
5)Healy JD (2003): Excess winter mortality in Europe: a cross country analysis identifying keyrisk factors. J Epide-miol Community Health, 57, 784-789.
6)池田若菜,稲葉 裕 (2007): 季節と高齢者死亡.臨床 と研究,84,1609-1612.
7)Inoue S, Murase N, Shimomitsu T, Ohya Y, Odagiri Y, Takamiya T, Ishii K, Katsumura T, Sallis JF (2009): Asso-ciation of physical activity and neighborhood environment among Japanese adults. Prev Med, 48, 321-325.
8)Kelsey JL (1996): Methods in observational epidemiology. Oxford University Press, New York.
9)Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, Yamagata K, Tomino Y, Yokoyama H, Hishida A (2009): Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis, 53, 982-992.
10)Metoki H, Ohkubo T, Kikuya M, Asayama K, Obara T, Hashimoto J, Totsune K, Hoshi H, Satoh H, Imai Y (2006): Prognostic significance for stroke of a morning pressor surge and a nocturnal blood pressure decline: the Ohasama study. Hypertension, 47, 149-154.
11)Mishima K, Okawa M, Shimizu T, Hishikawa Y (2001): Diminished melatonin secretion in the elderly caused by insufficient environmental illumination. J Clin Endocrinol Metab, 86, 129-134.
12)Modesti PA, Morabito M, Bertolozzi I, Massetti L, Panci G, Lumachi C, Giglio A, Bilo G, Caldara G, Lonati L, Orlandini S, Maracchi G, Mancia G, Gensini GF, Parati G (2006): Weather-related changes in 24-hour blood
pres-sure profile effects of age and implications for hypertension management. Hypertension, 47, 155-161.
13)Ohkubo T, Hozawa A, Yamaguchi J, Kikuya M, Ohmori K, Michimata M, Matsubara M, Hashimoto J, Hoshi H, Araki T, Tsuji I, Satoh H, Hisamichi S, Imai Y (2002): Prognostic significance of the nocturnal decline in blood pressure in individuals with and without high 24-h blood pressure: the Ohasama study. J Hypertens, 20, 2183-2189.
14)Wada T, Ishine M, Sakagami T, Okumiya K, Fujisawa M, Murakami S, Otsuka K, Yano S, Kita T, Matsubayashi K (2004): Depression in Japanese community-dwelling elderly - prevalence and association with ADL and QOL. Arch Gerontol Geriatr, 39, 15-23.
15)Woodhouse PR, Khaw KT, Plummer M (1993): Seasonal variation of blood pressure and its relationship to ambient temperature in an elderly population. J Hypertens, 11, 1267-1274.
16)Yamazaki F, Sone R (2000): Modulation of arterial barore-flex control of heart rate by skin cooling and heating in humans. J Appl Physiol, 88, 393-400.
17)Zeitzer JM, Dijk DJ, Kronauer R, Brown E, Czeisler C
(2000): Sensitivity of the human circadian pacemaker to nocturnal light: melatonin phase resetting and suppression. J Physiol, 526, 695-702.

![図 1 図 2 図 3 図 4 図 50 5 15 2010 P for trend=0.073(n=38)Q1[1.4− 4.1] (n=39)Q2[4.2− 6.5] (n=39)Q3[6.5− 9.2] (n=38)Q4[9.2− 11.8] (n=38)Q5[11.9− 43.9]](https://thumb-ap.123doks.com/thumbv2/123deta/6697302.704468/9.773.83.694.714.815/図-図-図-図-図-for-trend-q.webp)
