初診時単純 X 線で異常なく,急速進行した
頚椎多発性骨髄腫の 1 例
Rapidly Progressive Multiple Myeloma of the Cervical Vertebra in a Patient with Cervical Pain but Without Any Abnormal Findings on Plain Radiography in the Early Stages of Diagnosis ―A Case Report―
景 山 寛 志
*1尾 原 裕 康
*2菊地 奈穂子
*2松 岡 秀 典
*2富 田 禎 之
*2水 野 順 一
*2Hiroshi Kageyama, M.D.*1, Yukoh Ohara, M.D.*2, Nahoko Kikuchi, M.D.*2, Hidenori Matsuoka, M.D.*2,
Yoshiyuki Tomita, M.D.*2, Junichi Mizuno, M.D.*2 Abstract
Metastases of malignant cervical spine tumors often cause posterior cervical pain. We report a case of rapidly progressive multiple myeloma of the third cervical vertebra in a patient who presented with cervical pain but without any abnormal findings on plain radiography in the early stages of diag-nosis.
A 72 year old man with a 1 month history of posterior cervical pain visited our outpatient clinic. We did not identify any abnormal findings on plain radiography except for a degenerative change in the C5 C6 disk space. The patient was treated using conservative measures. Six weeks later, the patient returned with gradual development of the cervical and mandibular pains during swallowing. Plain radiography revealed destruction of the C3 vertebral body. Computed tomography revealed osteolytic changes and a C3 compression fracture. The magnetic resonance imaging scan demon-strated a tumor extending from the C3 vertebral body to the retropharyngeal space. Fludeoxyglu-cose positron emission tomography revealed abnormal accumulation only in C3. Moreover, Bence Jones protein expression was detected in the patient s urine. We performed laminectomy of C3, biopsy of the tumor, and posterior fixation.
The tumor was diagnosed as a myeloma. Stereotactic radiotherapy(Cyberknife 25 Gy/5 frac-tions)and chemotherapy(lenalidomide, bortezomib, and dexamethasone)were administered and resulted in the regression of the C3 tumor.
In cases of cervical pain without any abnormal findings on plain radiography, magnetic reso-nance imaging or computed tomography should not be performed on the basis of suspicion of a malignant spinal tumor. However, in cases of malignancy, rapid destruction of bone may occur. Therefore, in patients with chronic cervical pain and worsening of this pain while resting or at night, complete examination should be repeatedly performed.
(Received:October 31, 2016;accepted:March 14, 2017)
Key words
cervical spine, multiple myeloma, compression fracture, pain
*1 新久喜総合病院脳神経外科/Department of Neurosurgery, Shin Kuki General Hospital
連絡先:〒346 8530 久喜市上早見 418 1 新久喜総合病院脳神経外科 景山寛志〔Address reprint requests to:Hiroshi Kageyama, M.D., Department of Neurosurgery, Shin Kuki General Hospital, 418 1 Kamihayami, Kuki shi, Saitama 346 8530, Japan〕
*2 新百合ヶ丘総合病院脊椎脊髄末 神経外科/Center for Minimally Invasive Spinal Surgery, Shin Yurigaoka General Hospital
Case Report
症 例 報 告
頚部痛は頚椎疾患において,比較的多く遭遇する症候 である.大部分は変性疾患を含む良性疾患が原因である が,原発性,転移性を含めて頚椎悪性腫瘍の初発症状が 頚部痛である場合もあり,少ない頻度ながら見落としな く精査を進めなくてはならない.今回われわれは頚部痛 のみで発症し,初診時頚椎単純 X 線では病変が明らかで なかった頚椎多発性骨髄腫の 1 例を経験したため,提示 する. 患 者:72 歳,男性 主 訴:後頚部痛 既往歴:特記すべきことなし 現病歴ならびに初回外来:1 カ月間続く後頚部痛を主 訴として来院された.来院時,疼痛以外の神経学的異常 所見を認めなかった.来院時単純 X 線(Fig. 1)では C5/ 6の椎間板腔と左 C5/6 椎間孔狭窄を認めるのみで,それ 以外の明らかな異常を指摘できず鎮痛剤処方し保存的に 経過観察することとした. 外来再受診時:6 週間後,頚部痛の増悪と嚥下時下顎 部痛の出現を認めたため再診し,単純 X 線を施行した. 単純 X 線で C3 椎体の透亮像があり(Fig. 2 a),頚椎 com-puted tomography(CT)では C3 椎体の骨融解像を認め た(Fig. 2 b,c).頚椎 magnetic resonance imaging(MRI) では,C3 椎体右側に浸潤しつつ,後咽頭への進展と軽度 の硬膜管圧迫を示す長径 30 mm 大の腫瘍性病変が確認
された(Fig. 2 d∼f).18F fluorodeoxyglucose positron
emission tomography(FDG PET)では頚椎病変以外に 異常集積像はなかった.
血液生化学所見では,軽度の腎機能異常を認めるのみ だった(TP 6.2 g/dl,Alb 4.4 g/dl,AST 26 U/l,ALT 26 U/l,ALP 218 U/l,LDH 213 U/l,γ GTP 15 U/l,Bun
27.3 mg/dl,Cre 0.91,CRP 0.02).著明な貧血や,その 他の血球減少はなかった(WBC 3,600/μl,Hb 13.9 g/dl, Plt 16.8×104/μl).白血球分画は単球の割合がやや多い ものの,明らかな異常所見ではなかった(好塩基球 0.3%,好酸球 3.7%,単球 7.3%,リンパ球 43.9%,好中 球 44.8%).転移性脊椎腫瘍の可能性を考えて,一般的な 腫瘍マーカー(CEA,CA19 9,PSA,AFP)を検索した が,すべて陰性であった.尿中 Bence Jones タンパクが 陽性(k type)であり,多発性骨髄腫の可能性が示唆さ れた.その他の全身検索では,特に異常は指摘されな かった. 以上の検査所見より,C3 椎体原発の多発性骨髄腫を 第一の鑑別診断とした.比較的早い経過で進行する頚椎 椎体腫瘍であり,病理組織診断,病的骨折の進行による 不安定性増悪の可能性,硬膜管・脊髄圧迫による脊髄症 状出現の可能性を考え,外固定のみでは安定性の獲得が 困難と判断し,腫瘍生検ならびに頚椎後方除圧固定術を 計画した. 術中所見:全身麻酔下に患者を腹臥位とし,頭部を正 中位でメイフィールドに固定した.頚部正中で皮膚切開 を行い,筋肉を正中で左右に外側まで十分に展開し C2
C6を露出した.O arm ナビゲーションおよび C arm を
用いて,まず C2 より pedicle screw を挿入した.C3 骨破 壊による不安定性が強く,スクリュー挿入時に前方への 椎弓の動きを認めたため,まず左側のみスクリューを挿 入しロッド締結を行うこととした.C4 はスクリュー挿 入不可能であったため C5,6 に lateral mass screw を挿 入し,左側をロッドで締結した.続いて右側 C4,5,6
lateral mass screwを挿入し,こちらもロッドで締結し
た.その後顕微鏡を導入し,まず右側 C3 lateral mass の 骨削除を行った.少し深部に進むと灰褐色の柔らかい易 出血性腫瘍を認め,病理診断のため一部摘出した.続い て C3 椎弓切除を行い,黄色靭帯も除去し減圧した. CROSSLINKを置き,ロッド間を固定した.さらに腸骨 より骨片を採取して,二等分割し,それぞれをロッドの 両外側に挟んだ.残りの骨片も周囲に移植した.止血洗 浄を十分に行い,ドレーンを挿入し,層々に縫合して手 術を終了した(Fig. 3). その後の経過:術後は硬性カラーを継続した.ごく軽
はじめに
症例提示
Fig. 1Lateral plain radiograph at the first visit to the clinic, showing no abnormal findings except for a degener-ative change in the C5 C6 disk space.
度の右 C5 麻痺を認めたが次第に改善した.病理診断は myeloma〔κ(++),λ(+),CD79(++)〕だった. 病理診断確定ののち血液内科に転科し,化学療法が開始 された.まず BD 療法(Bortezomib 1.9 mg 皮下注射: day 1,4,8,11,Dexamethasone 20 mg:day 1,2,8,
9)を 4 クール施行した.しかし,自覚症状として頚部痛
が増悪し,MRI でも腫瘍増大,C2 椎体への浸潤も疑わ れたため,cyberknife(25 Gy/5 fr)照射した(Fig. 4 a,b). また,初回手術後 3 カ月の単純 X 線で C2 スクリューの looseningが認められ,MRI 所見と合わせて,不安定性 の増悪が懸念された.初回手術のロッドに追加するかた ちで OC C2 固定を行い,後頭骨と C2 棘突起間に骨移植 をした(Fig. 4 c).その後,化学療法プロトコルを RVD 療法(Lenalidomide 15 mg 経口:14 days,Bortezomib 1.9 mg皮下注射:day 1,4,8,11,Dexamethasone 20 mg: day 1,2,8,9)に変更し,計 9 クール施行した.フォ ローアップの PET CT では頚椎病変の集積を認めず,初 回手術から 12 カ月後の頚椎 MRI(Fig. 5 a∼c)でも腫 瘍増大を認めていない.また,頚椎 CT では融解してい た C3 椎体の再骨化が確認された(Fig. 5 d).なお,初 回手術後から再骨化が確認されるまで,硬性カラー装着 を継続した.頚部痛は改善し,現在外来経過観察中である. Fig. 2
Plain radiograph, computed tomography(CT)scan, and magnetic resonance image(MRI)obtained at the patient s second visit to the outpatient clinic, during which time cervical pain was reported.
a :Lateral plain radiograph showing the radiolucency of the C3 vertebral body. b :Reconstructed sagittal CT scan showing osteolysis of the C3 vertebral body. c :Axial CT scan showing osteolysis of the right aspect of the C3 vertebral body.
d , e :Preoperative MRI in the sagittal view showing compression and retropulsion of the C3 vertebral body (d:T1 weighted image and e:T2 weighted image).
f : Axial T1 weighted preoperative MRI scan showing that the tumor invaded the right aspect of the C3 vertebral body. The tumor extended into the retropharyngeal space with retropulsion into the canal.
aa
bb
cc
dd
ee
ff
Fig. 3
a : Lateral plain radiograph after a surgery, tumor biopsy, C3 lami-nectomy, and posterior fixation.
b :Anteroposterior plain radiograph.
脊椎は癌の骨転移先として最も頻度が高い.高齢化や 医療の発達により,癌患者数ならびに生存期間が延長し てきているため,悪性腫瘍の脊椎転移の患者数も増えて きている.原発巣としては乳癌,肺癌,腎癌,前立腺癌, 甲状腺癌,悪性黒色腫,多発性骨髄腫,悪性リンパ腫, 大腸癌などが多い.70%程度の担癌患者は脊椎転移を発 症するといわれている.疼痛や神経脱落症状,脊椎不安 定性などが現れ,放射線療法,化学療法,あるいは手術 が必要となることもある1).脊椎転移で最も多いのは, 胸椎・胸腰椎である(70%).これに腰仙椎が続く(20%). 頚椎転移は比較的少なく,全脊椎転移性腫瘍の 8∼20% 程度とされる2,3).なお,転移性頚椎腫瘍連続 51 症例を 集めた Jonsson らの報告では乳癌(37%)に続いて骨髄 腫が多かったとされている(18%)4).脊椎転移では,麻 痺を発症する前に疼痛を訴えている時点で放射線治療を 行った場合,一時的な疼痛緩和だけではなく,生存期間 中の麻痺を回避できる可能性が高くなる.乳癌などの放 射線感受性の高い腫瘍であれば,早期発見により局所コ ントロールが可能である.逆に軽微でも症状が出現して いる場合,放射線感受性の悪い腫瘍であれば,麻痺が進
考 察
Fig. 4Magnetic resonance image(MRI)3 months after the first MRI(Fig. 2d∼f).
a:T2 weighted MRI in the sagittal view showing tumor invasion to the C2 vertebral body. b :Contrast enhanced T1 weighted MRI in the axial view showing tumor enlargement. c :Lateral plain radiograph after an additional surgery with OC C2 fixation.
aa
bb
cc
Fig. 5
Magnetic resonance image and computed tomography(CT)scan obtained 12 months after surgery(tumor biopsy, C3 laminectomy, and posterior fusion), chemotherapy, and radiotherapy.
a :Sagittal T1 weighted image. b :Sagittal T2 weighted image.
c : Axial T1 weighted image. The tumor marginally decreased in size. The spinal cord was released from compression.
d : Reconstructed sagittal CT scan showing remineralization of the C3 verte-bral body.
aa
bb
cc
行し生活レベル(activities of daily living:ADL)が低下 する可能性が高い.したがって,早期診断し治療を開始 することが,転移性脊椎腫瘍患者にとって生存期間中の ADL維持のために重要である5). 今回われわれは,頚椎発症の骨髄腫を経験した.多発 性骨髄腫(multiple myeloma)は,形質細胞由来の悪性 腫瘍である.脊椎に発症することがしばしばあり,腫瘍 細胞が骨髄腔に浸潤すると,interleukin を含めた
osteo-clast activating factorsが分泌される.この interleukin に
より tumor necrosis factor(TNF)が誘導され,さらなる 骨吸収が進む.そのため骨髄腫では骨溶解により痛みを 発症することが多い.椎体骨折も主要な症候である.椎 体変形と腫瘍の硬膜外進展に伴い,脊髄圧迫をきたすこ ともある.骨髄腫は放射線感受性が強く,放射線治療の よい適応だが,骨折後の不安定性や脊髄症状をきたして いるような圧迫病変の場合は内固定も含めた外科的治療 が考慮される4).本症例と同様に,頚部痛を主訴として 単純 X 線で頚椎椎体骨折が指摘され,最終的に多発性骨 髄腫と診断された症例報告は過去に 4 報ある(Table 1)4,6∼8).いずれの症例でも,初回の検査で椎体の異常が 指摘されている.頚部痛の性状については詳細な記載は 少なかったが,Chiropractic doctor の報告した症例では, 咳嗽により増悪する頚部痛と記載されていた5).また, 診断にいたるまでの期間は頚部痛発症から数週∼1 年と 長期にわたっており,比較的希少な疾患で,さらに頚部 痛という一般的な症状しか示さないことが診断の遅れに つながっていると考えられた.治療は,4 例中 2 例は手 術(生検と内固定)ならびに放射線化学療法が行われ, 1例は生検と外固定ならびに放射線治療が行われてい た.残り 1 例は,全身状態不良で根治的治療が不可能で あった.本症例のように,初回単純 X 線で異常を認め ず,後日の再検査で異常が指摘された多発性骨髄腫の報 告は渉猟し得るかぎり確認できなかった. 脊椎腫瘍の初発症状で最も多いのは疼痛である2).緩 徐に発症・増悪し,夜間増悪や安静時にまで持続する痛 みは,脊椎腫瘍の典型的症状である3,9).荷重や咳嗽によ り増悪する疼痛も,脊椎腫瘍を疑う10).体重減少や食思 不振を伴っていても,悪性腫瘍を疑う9,10).また,外傷機 転のない急な痛みは,病的骨折の症状と考えられる.6 週間以上続く疼痛,治療抵抗性の疼痛なども,転移を中 心とする脊椎腫瘍を考慮すべき症状である10,11).脊椎腫 瘍の疼痛はさまざまな理由で起こるが,発症初期は皮質 骨の圧排拡大に伴う骨膜の伸張刺激であり,骨折したの ちは骨折痛,脊髄症状,神経根症状,kyphosis など脊椎 変形による3).頚椎に絞って検討してみると,転移性頚 椎腫瘍では 89∼93%に頚部痛を認める3).したがって, 頚椎腫瘍の早期診断は頚部痛の段階で腫瘍の存在を疑 い,必要な検査を行うことで得られる.既往に悪性腫瘍 があれば,頚部痛に関して初診時に脊椎転移を疑うこと も可能である.しかし,本症例のように骨転移の 10∼ 30%が初診時原発不明である.その中で,最終診断は肺 癌が最多である.次いで多発性骨髄腫,悪性リンパ腫な どの造血器腫瘍と前立腺癌が多い12).本症例では初発症 状は頚部痛のみで,最終病理診断は多発性骨髄腫であっ た.Rao ら4)の報告によると,頚椎の多発性骨髄腫の治療 例 35 例において,89%に頚部痛を認めたとされている. 11%は頚部痛がなかったが,スクリーニングの画像検査 で指摘されている.なお,同シリーズにおいて急性発症 の神経根症状・脊髄症状は認められなかった4). 頚椎のレベルによって検討してみると,まず C1,C2 椎体の転移性腫瘍に限定した検討でもすべての患者が頚 部痛を訴えており,91%は頚部の回旋時痛を認めた. 33%で後頭部痛を呈した.初診時に myelopathy を呈し た患者はいなかった13).C3 以下の subaxial lesion におけ る報告でも,頚部痛が主症状であった9).なお,いずれ の報告でも初期から脊髄症状を呈していることは少な かったが,その中でも初期症状ではないが,cranioverte-bral junctionのほうが脊柱管が広く,複雑な多数の靭帯 により保護されているため,後縦靭帯のみがある sub-axial lesionと比較してC1/C2転移性腫瘍の後方進展によ
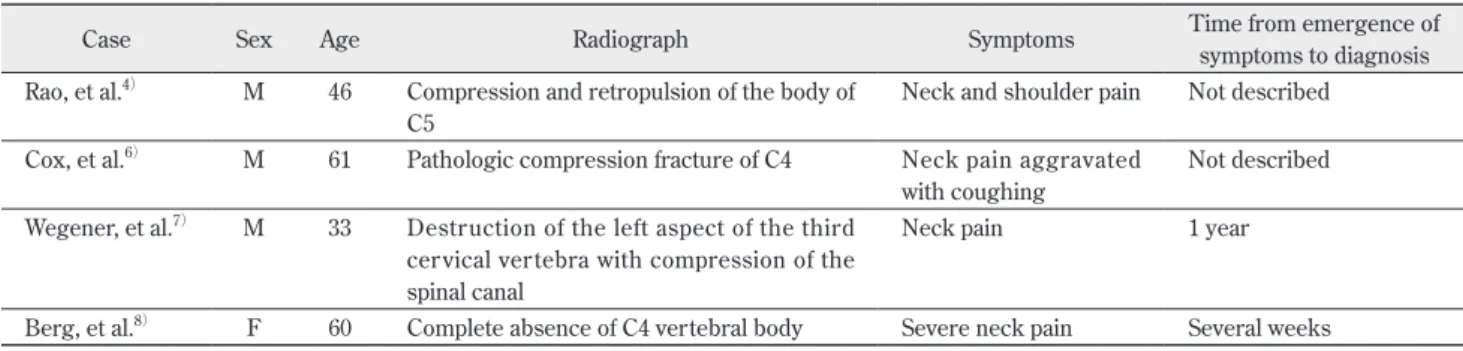
Table 1 Four case reports of cervical myeloma diagnosed on the basis of neck pain and the initial plain radiograph
Case Sex Age Radiograph Symptoms Time from emergence ofsymptoms to diagnosis Rao, et al.4) M 46 Compression and retropulsion of the body of
C5
Neck and shoulder pain Not described Cox, et al.6) M 61 Pathologic compression fracture of C4 Neck pain aggravated
with coughing
Not described Wegener, et al.7) M 33 Destruction of the left aspect of the third
cervical vertebra with compression of the spinal canal
Neck pain 1 year
る脊髄圧迫の頻度は少ないと報告されている3).今回わ れわれが経験した症例は,C3 原発の多発性骨髄腫で あった.初診時の単純 X 線では異常が見当たらず,その 時点で悪性疾患を疑うとしたら,1 カ月間継続する頚部 痛であったことが早期発見の鍵になった可能性がある. これに加えて,夜間・安静時や咳嗽による疼痛の増悪な どもチェックしておくべきだったと考える. 以上のように,頚部痛を主体として臨床症状を詳細に 検討したのち,外来でまず行われる検査は単純 X 線検査 である.脊椎転移の単純 X 線の特徴は,正面像での椎弓 根の消失である.特異性の高い所見だが,脊椎では骨破 壊が 50%以上にならないと明らかにならないため,感度 は低い.また,最も麻痺を発症しやすい上位胸椎では, 胸椎の後弯や胸骨の重なりのために正確な評価は困難で ある5).造血器腫瘍は当初骨髄を置換するかたちで増殖 するため,進行期でないと単純 X 線で検出しづらい.前 立腺癌や乳癌は造骨像を呈し,肺癌や甲状腺癌,腎細胞 癌は溶骨することが多い2).単純 X 線で早期に骨転移を 疑う点として,まず挙げられるのは骨折のレベルであ る.頚椎から中上位胸椎では,大きな外傷機転なく圧迫 骨折することはまれであり,このレベルでの圧迫骨折は 病的骨折の可能性が高くなる.胸腰椎移行部では骨粗鬆 症性圧迫骨折が多い.ただし,L4 以下や T10 では少ない ため,病的骨折の可能性がある5).また片桐ら5)は,骨折 の形態として椎体の片側圧潰が病的骨折と相関すること を挙げている.自験例をもとに脊椎 X 線正面像で左右の 椎弓根に垂直二等分線を引き,その線と上下の終板の交 点を左右に延長した交線の角(おおむね上下終板の角) が 5 度以上の場合は病的骨折の可能性が高くなると提唱 している.本症例のような多発性骨髄腫の場合,過去の 報告では 55∼70%に椎体圧迫骨折がある14).ほかの悪性 腫瘍は骨髄腔を置換するように増殖するが,多発性骨髄 腫は骨吸収を活発に行う.その結果,骨髄腫の脊椎転移 は,ほかの癌種より骨破壊が進行しやすいとされてい る4).Rao ら4)の報告では頚椎多発性骨髄腫の罹患レベル としては C2,C3 レベルが多い(C2 27%,C3 20%).本 症例も単純 X 線で異常所見が出たのは C3 レベルだった. 以上のように,持続する頚部痛があり,単純 X 線で異 常所見がある場合,CT,MRI,骨シンチグラフィー,各 種腫瘍マーカー,全身画像検索などが行われれば,脊椎 腫瘍の早期診断は可能と思われる.しかし,単純 X 線で の異常所見がない初期段階で,頚部痛のみを根拠とし て,それ以外の精査を行うか否かについては判断が分か れるであろう.ただし,単純 X 線の感度を考えると,そ れで異常所見がなかったとしても,前述のような転移性 頚椎腫瘍を疑う頚部痛の特徴がある場合は,CT,MRI の 追加を検討してもよい.また,本症例のように頚部痛の 持続・増悪のみで急速に椎体破壊が進行していることも ある.したがって,持続する頚部痛の訴えがある場合に は,再検査が必要な症例が含まれている.初回検査から 再検査までの間隔は個々の症例によって検討すべきであ るが,特に 6 週間以上続き,夜間の増悪や,安静時の持 続する頚部痛の場合に関しては,初診時の単純 X 線で異 常がなかったとしても,再検査に消極的になるべきでは ないと考えられた. 頚部痛のみで発症し,初診時の単純 X 線では異常が認 められなかった頚椎発症の多発性骨髄腫の 1 例を経験し た.悪性腫瘍では本症例のように短期間で急速に骨破壊 が進行する可能性があり,改善せず 6 週間以上安静時に も持続する痛み,夜間に増悪する痛みに関しては画像検 査を含めた積極的なフォローアップが必要である. 利益相反開示 筆頭著者は開示すべき利益相反を有していない. 文 献
1) Choi D, Crockard A, Bunger C, et al:Review of metastatic spine tumour classification and indications for surgery:the consensus statement of the Global Spine Tumour Study Group.
Eur Spine J 19:215 222, 2010
2) Ciftdemir M, Kaya M, Selcuk E, et al:Tumors of the spine.
World J Orthop 7:109 116, 2016
3) Molina CA, Gokaslan ZL, Sciubba DM:Diagnosis and manage-ment of metastatic cervical spine tumors. Orthop Clin North
Am 43:75 87, 2012
4) Rao G, Ha CS, Chakrabarti I, et al:Multiple myeloma of the cervical spine:treatment strategies for pain and spinal instabil-ity. J Neurosurg Spine 5:140 145, 2006
5) 片桐浩久,鈴木辰隆,和佐潤志,他:転移性骨腫瘍の早期診 断と早期治療.関節外科 35:360 367,2016
6) Cox J, DeGraauw C, Klein E:Pathological burst fracture in the cervical spine with negative red flags:a case report. J Can
Chiropr Assoc 60:81 87, 2016
7) Wegener B, Muller PE, Jansson V, et al:Cervical spine metas-tasis of multiple myeloma:a case report with 16 years of fol-low up. Spine 29:E368 372, 2004
8) Berg AJ, Hernandez M, Bhatia C:Complete C4 vertebral body destruction:a dramatic finding in a patient with a new diagno-sis of myeloma. BMJ Case Rep, 2014, doi:10.1136/bcr 2013 203108
9) Abdu WA, Provencher M:Primary bone and metastatic tumors of the cervical spine. Spine 23:2767 2777, 1998
10) 柴田浩行:緊急に対応が必要な骨転移の症状は何か? 日本 臨床腫瘍学会:骨転移診療ガイドライン.東京,南江堂, 2015,p13
11) 小林英介,川井 章:骨転移診療ガイドラインに基づいた転 移性脊椎腫瘍の診断と治療.関節外科 35:342 346,2016 12) 穂積高弘,五嶋孝博,山川聖史,他:初診時原発不明であっ
た転移性脊椎腫瘍の原発巣の診断と治療.関節外科 35:12 17,2016
13) Bilsky MH, Shannon FJ, Sheppard S, et al:Diagnosis and
man-agement of a metastatic tumor in the atlantoaxial spine. Spine 27:1062 1069, 2002
14) Lecouvet FE, Vande Berg BC, Maldague BE, et al:Vertebral compression fractures in multiple myeloma. PartⅠ. Distribu-tion and appearance at MR imaging. Radiology 204:195 199, 1997