RESURFACING EFFECTS OF SHORT
-PULSED CARBON DIOXIDE LASER FOR CUTANEOUS SQUAMOUS
CELL CARCINOMA IN SITU
Naoko Hasunuma1, Natsuko Noguchi2, Hajime Nagato2, Masaaki Tsuda2, Maki Kato2, Aya Yokoi2, Katsuhiro Yamada2, Takehiro Yamakawa2, Tomonori Akama2, Yoshihiro Umebayashi2 and Motomu Manabe2
(received 8 June 2009, Accepted 23 June 2009)
1Department of Community Medicine and Primary Care Development, Akita University Faculty of Medicine
2Department of Dermatology and Plastic Surgery, Akita University Graduate School of Medicine
Abstract
The carbon dioxide (CO2) laser in a short-pulsed mode is currently one of the most useful devices in dermatologic practice in the fields of oncology. To evaluate the safety and efficacy of the short-pulsed CO2 laser in the treatment of cutaneous squamous cell carcinoma (SCC) in situ, the clinical improvement of 40 cases SCC in situ treated with the laser was assessed by a retrospec- tive study. Consequently, it was shown that (1) no clinical evidence of recurrences during the follow-up time (3 to 63 months) in 27 cases, (2) lesion recurrence occurred and additional treat- ments were required in 13 cases, and (3) hypertrophic scarring was complicated in 1 case. Our findings suggested that the short-pulsed CO2 laser can be considered a safe and effective treat- ment for patients with SCC in situ, offering excellent cosmetic results.
Key words: short-pulsed carbon dioxide laser, actinic keratosis, actinic cheilitis, Bowen’s disease
Introduction
Squamous cell carcinoma (SCC) in situ is an early form of SCC defined by the absence of invasion of the dermis.
In other words, it is intra-epidermal proliferative disorder that may be precursors of SCC. SCC in situ includes ac- tinic keratosis, actinic cheilitis and Bowen’s disease.
Actinic keratosis is an erythematous, scaling lesion oc- curring on heavily sunlight exposed areas. Actinic chei- litis is a form of actinic keratosis developing on the lip.
Bowen’s disease is a full thickness SCC in situ affecting
both exposed and non-exposed skin sites1).
Many therapies have been attempted for the treatment of SCC in situ, including topical 5-fluorouracil (5-FU), cryotherapy, and excisional surgery2–4). However, these treatment options tend to either fall short of complete eradication of the lesion or result in an unacceptable scar that can be as disfiguring as the SCC in situ itself. Fur- thermore, although the carbon dioxide (CO2) laser has been proven effective for a wide range of dermatologic conditions including SCC in situ3,4), potential disadvan- tages of the traditional CO2 laser include the creation of a thermal injury zone deep to the ablation zone with suc- cessive pass. Excessive thermal injury has been impli- cated as a possible etiology for scar formation after the laser treatment.
Recent advance in laser technology has made it possi- ble to develop the modern pulsed and scanned CO2 laser Correspondence : Naoko Hasunuma
Department of Community Medicine and Primary Care Development, Akita University Faculty of Medicine, Hondo 1-1-1, Akita, Japan 010-8543
Tel : 018-884-6153 Fax : 018-836-2618
E-mail : [email protected]-u.ac.jp
as an excellent treatment choice for patients with SCC in situ5). By selection of the proper pulse parameters, the newer CO2 laser systems offer the ability to control va- porization depth with minimal damage to surrounding tis- sues, which reduced risk of postoperative scar formation.
We herein outline a retrospective study to evaluate the efficiency of short-pulsed CO2 laser for the treatment of patients with SCC in situ. The present study sheds light on the short-pulsed CO2 laser as a safe and effective option for the treatment of SCC in situ.
Cases and Methods Laser Resurfacing Procedures :
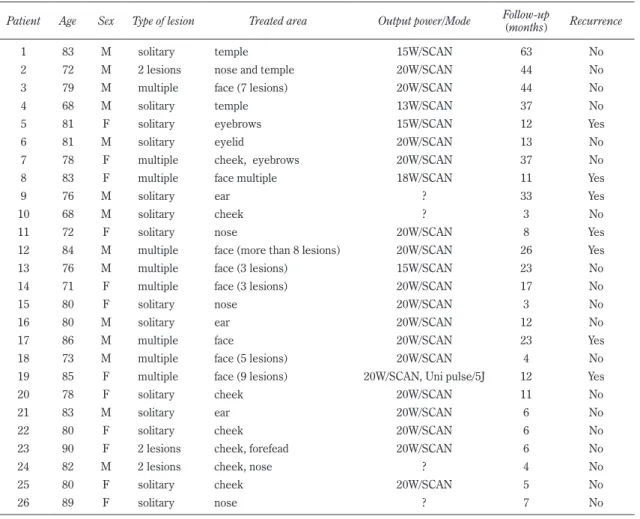
We treated 40 patients (24 men, 16 women; age ranged from 64 to 90 years) with SCC in situ (summa- rized in Table 1), under local anesthetics with 1% lido- caine, using a short-pulsed CO2 laser (UniPulseTM COL- 1040, NIDEK CO., Ltd) at the following conditions : 13 to 20 Watts, 300 Hertz (Hz), and 6.1×6.1 mm spot size.
These parameters were selected to provide identical ef- fects of the laser systems in this study. The diagnoses of SCC in situ were based on routine histopathological examination of biopsy specimen.
Several laser passes were performed, and each desic- cated lesion was completely removed with saline-soaked gauze between each pass. The wound was cleansed with saline and an antibiotics ointment applied once a day until re-epithelization was complete.
Evaluation of Laser Resurfacing using Normal Skin :
Skin specimens obtained from healthy volunteers were irradiated with a short-pulsed CO2 laser from one to 10 passes at 15 (6.36 J/cm2) or 20 Watts (8.48 J/cm2), and desiccated lesion was removed with saline-soaked gauze as described above. For histological analysis, specimens were fixed in 10% formaline, embedded in paraffin, and sectioned at 5 μm. Hematoxylin and eosin staining was performed using standard procedures.
Results Clinical Findings :
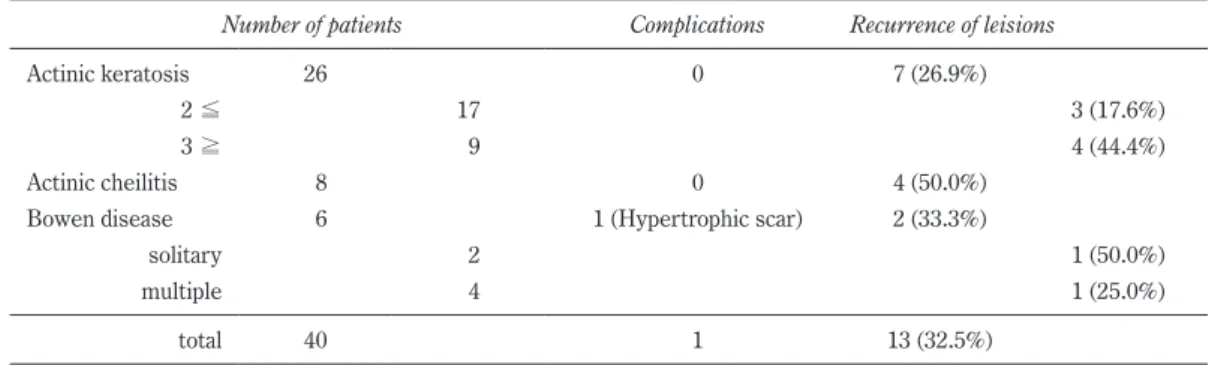
All 40 cases completed the study and were available for the required follow-up visits. Of those, 26 cases were actinic keratosis, 8 cases were actinic cheilitis, and 6 cases were Bowen’s disease. (Table 1-4) All cases completed the study with no serious complication. (Fig.
1, 2, 3, 4)
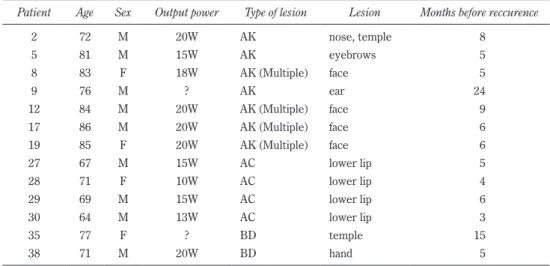
Of the 40 patients treated, lesion recurrence was ob- served in 13 cases (32.5%) : 7 cases with actinic kerato- sis (26.9%), 4 cases with actinic cheilitis (50%), 2 cases with Bowen’s disease (33.3%). Higher recurrence rate was observed in the case of actinic keratosis with 3 or more cancerous lesions (44.4%) rather than with solitary or two lesions (17.6%). (Table 1) The recurrence oc- curred within 12 months in 10 of 13 recurrence cases.
(Table 5) Especially in actinic cheilitis, all of the four recurrence cases were relapsed within six months.
Treatment with power setting of 13-18 W causes recur-
Table 1. Summary of the treated patients
Number of patients Complications Recurrence of leisions
Actinic keratosis 26 0 7 (26.9%)
2≦ 17 3 (17.6%)
3≧ 9 4 (44.4%)
Actinic cheilitis 8 0 4 (50.0%)
Bowen disease 6 1 (Hypertrophic scar) 2 (33.3%)
solitary 2 1 (50.0%)
multiple 4 1 (25.0%)
total 40 1 13 (32.5%)
Table 2. Patients with actinic keratosis
Patient Age Sex Type of lesion Treated area Output power/Mode Follow-up
(months) Recurrence
1 83 M solitary temple 15W/SCAN 63 No
2 72 M 2 lesions nose and temple 20W/SCAN 44 No
3 79 M multiple face (7 lesions) 20W/SCAN 44 No
4 68 M solitary temple 13W/SCAN 37 No
5 81 F solitary eyebrows 15W/SCAN 12 Yes
6 81 M solitary eyelid 20W/SCAN 13 No
7 78 F multiple cheek, eyebrows 20W/SCAN 37 No
8 83 F multiple face multiple 18W/SCAN 11 Yes
9 76 M solitary ear ? 33 Yes
10 68 M solitary cheek ? 3 No
11 72 F solitary nose 20W/SCAN 8 Yes
12 84 M multiple face (more than 8 lesions) 20W/SCAN 26 Yes
13 76 M multiple face (3 lesions) 15W/SCAN 23 No
14 71 F multiple face (3 lesions) 20W/SCAN 17 No
15 80 F solitary nose 20W/SCAN 3 No
16 80 M solitary ear 20W/SCAN 12 No
17 86 M multiple face 20W/SCAN 23 Yes
18 73 M multiple face (5 lesions) 20W/SCAN 4 No
19 85 F multiple face (9 lesions) 20W/SCAN, Uni pulse/5J 12 Yes
20 78 F solitary cheek 20W/SCAN 11 No
21 83 M solitary ear 20W/SCAN 6 No
22 80 F solitary cheek 20W/SCAN 6 No
23 90 F 2 lesions cheek, forefead 20W/SCAN 6 No
24 82 M 2 lesions cheek, nose ? 4 No
25 80 F solitary cheek 20W/SCAN 5 No
26 89 F solitary nose ? 7 No
Table 3. Patients with actinic cheilitis
Patient Age Sex Type of lesion Treated area Output power/Mode Follow-up (months) Recurrence
27 67 M solitary lower lip 15W / SCAN 23 Yes
28 71 F solitary lower lip 10W / SCAN 13 Yes
29 69 M solitary lower lip 15W / SCAN 9 Yes
30 64 M solitary lower lip 13W / SCAN 28 Yes
31 71 F solitary lower lip 20W / SCAN 9 No
32 68 M solitary lower lip 20W / SCAN 34 No
33 60 M solitary lower lip 20W / SCAN 41 No
34 80 F solitary lower lip 20W / SCAN 3.5 No
rence at a significantly higher rate than with 20W (P<0.05, Fisher’s exact test). (Table 6) Adverse effects included mild hypertrophic scarring in only one patient with Bowen’s disease.
Histologic Findings
At 20W irradiation, after one pass, tissue injury ex- tended to the depth of 80-100 μm, and the entire epider- mal layer was removed. (Fig. 5a) After three passes,
tissue injury extended to the papillary dermis, and thin layers of desiccated dermal collagen at 120-130 μm thick were observed. After five passes, the structure of papil- lary dermis became unclear, thin layers of desiccated dermal collagen at 180-200 μm thick including homoge- nized layers at 80-100 μm thick were observed, and cap- illaries in the papillary dermis were denatured. After ten passes, tissue injury extended to the depth of 200 μm, the structure of the papillary dermis and the upper Table 4. Patients with Bowen’s disease
Patient Age Sex Type of lesion Treated area Output power/Mode Follow-up (months) Recurrence
35 77 F multiple temple ? 15 Yes
36 72 M multiple fingers (3 lesions) ? 21 No
37 79 M multiple fingers (2 lesions) 20W / SCAN 5 No
38 71 M solitary hand 20W / SCAN 8 Yes
39 79 M multiple chest, both hands (4 lesions) ? 3 No
40 76 M solitary foot ? 4 No
Table 5. Patients with recurrence following CO2 laser ablating
Patient Age Sex Output power Type of lesion Lesion Months before reccurence
2 72 M 20W AK nose, temple 8
5 81 M 15W AK eyebrows 5
8 83 F 18W AK (Multiple) face 5
9 76 M ? AK ear 24
12 84 M 20W AK (Multiple) face 9
17 86 M 20W AK (Multiple) face 6
19 85 F 20W AK (Multiple) face 6
27 67 M 15W AC lower lip 5
28 71 F 10W AC lower lip 4
29 69 M 15W AC lower lip 6
30 64 M 13W AC lower lip 3
35 77 F ? BD temple 15
38 71 M 20W BD hand 5
AK ; Actinikc keratosis AC ; Actinik cheilitis BD ; Bowen disease
Table 6. Patients with recurrence categorized according to power setting Number of Treated Patient Number of Reccurent Patient
13-18W SCAN 9 6 (66.6%)
20W SCAN 23 5 (21.7%)
P<0.05 (Fisher’s exact test)
Fig. 1. Patient 21 : Actinic keratosis of the auricle.
a, b : before CO2 laser irradiation; keratotic lesions are in the erythematous plaque (outlined).
c, d : 3 months after irradiation; no erythema or recurrence is observed.
Fig. 2. Patient 26 : Actinic keratosis of the nose.
a : Before CO2 laser irradiation; infiltrative erythema with scaling (outlined).
b : 6 weeks after irradiation; One observes slight erythema and pigmentation, but no infiltration nor hyperkeratosis to suggest a recurrence.
layer of reticular dermis including capillary were dena- tured.
In contrast, at 15 W irradiation, after one pass, several cells remained intact at the base of the rete ridges. (Fig.
5b) Even after five passes, the structure of papillary dermis was preserved steadily in comparison with that
irradiated at 20W.
Discussion
The short-pulsed CO2 laser allows high peak power in order to maximize tissue vaporization as well as short Fig. 3. Patient 32 : Actinic cheilitis of the lower lip.
a : Before CO2 laser irradiation; erosion and a hyperkeratotic lesion are visible (outlined).
b : 15 weeks after irradiation; no erosion is visible.
Fig. 4. Patient 34 : Actinic cheilitis of the lower lip.
a : Before CO2 laser irradiation; an irregular shaped erosion is observed (outlined).
b : 15 weeks after irradiation; no erosion remains.
Fig. 5. Histopathological features of the skin after short-pulsed CO2 laser treatment.
a : 20 W SCAN (HE, ×100) b : 15 W SCAN (HE, ×100)
pulse duration in order to minimize thermal injury to the cutting area5–8). The laser offers unique advantages for the treatment of SCC in situ. First, the short-pulsed nature enables the operator to recognize whether the la- ser vaporizes exclusively the epidermis, the papillary or reticular dermis. Thus the operator can directly esti- mate the level removed by vaporization and stop the va- porization as soon as affected lesion has been removed.
Second, the laser also produces excellent visualization of the operative border. This discriminator permits tissue sparing in the process of excision. The hazard of injury to surrounding tissue, a serious cosmetic complication, is correspondingly reduced.
Based on the above-mentioned advantages, we chose the laser treatment for the patients with SCC in situ at specific location such as oral mucosa, and for the patients who require palliative treatment. In comparison to oth- er treatments, the cure rate after the CO2 laser treatment showed about the same or higher rate after cryosurgery or topical 5-FU4,9) and offered the advantage of highly confined tissue damage and less scaring in comparison with surgical excision. Considering the excellent re- sults obtained in our patients, the short-pulsed CO2 laser is considered as a therapeutic option in the treatment of SCC in situ with fewer adverse effects and better cos- metic results.
A major criticism regarding laser treatment for SCC in situ is that this technique does not allow the operator to perform any intraoperatory histological examination, thus limiting the certainty of complete removal of the lesions.
The results obtained in our patients are an example of the limitation of laser treatment, which showed that SCC in situ might not always respond so favorably. For ex- ample, invasive SCC developed in one case after incom- plete laser ablating, although this case might already progressed to invasive SCC before the treatment.
Never theless, the risk of recurrence may be minimized by selection of the proper pulse parameters, while there is great variability in the depths of lesion involvement.
In this regards, our clinical experience reflects the spe- cific histological findings of normal skin vaporized by dif- ferent conditions, which offers interesting perspectives for optimal cure of SCC in situ with laser surgery.
Namely, the laser treatment at 13 to 15 W, in which con-
dition the vaporization extended to more superficial depth, showed higher recurrence rate. On the contrary, the laser treatment at 20W, in which condition the vapor- ization extended to deeper depth, showed lower recur- rence rate. These findings have encouraged us to treat patients with the laser at the condition of 20W in order to obtain the maximum effects; this is the endpoint of suc- cessful laser treatment regardless of the technique employed. We will continue to treat patients in this manner and initiate a long term follow-up study evalu- ating the effects of this condition.
The case series study presented here has several limi- tations, as it is retrospective, relatively small and has only a short term follow-up. Furthermore, a direct comparison of recurrence rate or other complications cannot be made between our study and the studies re- ported previously using the short-pulsed laser, since the different efficiency of laser at various conditions were used in these reports3,4,7,10). Despite of these unclear points, we expect that future larger studies will establish the short-pulsed CO2 laser as a promising tool for SCC in situ in the coming aging society.
References
1) Kao, G.F., Cerio, R., Salom, R. et al. (2006) Patholo- gy And Genetics of Skin Tumours(World Health Or- ganization Classification of Tumours). IARC Press, Lyon, pp. 26.
2) Shwartz, R.A. and H.L. Stoll, Jr. (1999) Fitzpatrick’s Dermatology in General Medicine. Fifth Edition.
McGraw-Hill, USA, pp. 824-826.
3) Mackie, R.M. (1998) Rook/Wilkinson/Ebling Text- book of Dermatology. Sixth Edition. Blackwell Sci- ence, USA, pp. 1670-1672.
4) Dufresne, Jr. R.G. and Curlin, M.U. (1997) Actinic Chilitis A Treatment Review. Dermatol. Surg., 23, 15-21.
5) Fitzpatrick, R.E., Goldman, M.P. and Ruiz-Esparza, J.
(1994) Clinical advantage of the CO2 laser super- pulsed mode. Treatment of verruca vulgaris, sebor- rheic keratosis, lentigines, and actinic keratosis. J.
Dermatol. Surg. Oncol., 20, 449-456.
6) McKenzie A.L. (1983) How far thermal damage extends beneath the surface of the CO2 incisions ?
Phys. Med. Biol., 28, 905-912.
7) Hobbs, E.R., Bailin, P.C., Wheeland, R.G. and Ratz, J.L. (1987) Superpulsed lasers : minimizing ther- mal damage with short duration, high irradiance pulses. J. Dermatol. Surg. Oncol., 13, 955-964.
8) Nakaoka, H., Hashimoto, K. and Ootsuka, H. (1999) Histological findings in normal skin after short- pulsed CO2 laser irradiation. Nishinihon J. Derma- tol., 61, 221-223.
9) Williams, H., Bigby, M., Diepgen, T. et al. (2008) Evidence-based Dermatology. Second Edition.
Blackwell Publishing, Malden, pp. 295-314.
10) Martinez-Gonzalez, M.C., Pozo, J.D., Paradela, S., Fernandes-Jorge, B., Fernandes-Torres, R., and Fon- seca, E. (2007) Bowen’s disease treated by carbon dioxide laser. A series of 44 patients. J. Dermatol.
Treat., 19, 293-299.