Comparison of Clinical Outcomes of Acute Myocardial Infarction
Between Prasugrel and Clopidogrel
Kaho Shibata,
1MD, Kenichi Sakakura,
1MD, Yousuke Taniguchi,
1MD, Kei Yamamoto,
1MD,
Takunori Tsukui,
1MD, Masaru Seguchi,
1MD, Hiroyuki Jinnouchi,
1MD,
Hiroshi Wada,
1MD and Hideo Fujita,
1MD
SummaryThe rapid introduction of dual antiplatelet therapy (DAPT) is important for patients with acute myocardial infarction (AMI). The risks and benefits of reduced-dose prasugrel (20 mg loading and 3.75 mg maintenance) over clopidogrel have not been fully discussed. The purpose of this study was to compare the 90-days clinical outcomes of AMI between prasugrel-based DAPT and clopidogrel-based DAPT. We included 534 AMI patients and divided them into the clopidogrel group (n = 330) and the prasugrel group (n = 204). The primary endpoint was the total ischemic events and total bleeding events. In all, 52 ischemic events and 35 bleeding events were observed during the study period. The total ischemic events were similar between the clopidogrel and the pra-sugrel groups (P = 0.385). The total bleeding events were similar between the clopidogrel and the prapra-sugrel groups (P = 0.125). The multivariate Cox hazard analysis showed that prasugrel was not associated with the to-tal ischemic events (hazard ratio (HR) 0.955, 95% confidence interval (CI) 0.499-1.829, P = 0.890) and was not associated with the total bleeding events after controlling confounding factors (HR 0.972, 95% CI 0.528-1.790,
P = 0.927). In conclusion, as compared to clopidogrel, the reduced dose of prasugrel was not associated with
the excess risk of bleeding or the excess risk of ischemic events. Our real-world data support the current regi-men of prasugrel for AMI patients who underwent primary percutaneous coronary intervention.
(Int Heart J 2021; 62: 479-486)
Key words: Dual antiplatelet therapy, Ischemic event, Bleeding
T
he clinical outcomes of acute myocardial infarc-tion (AMI) have been greatly improved by pri-mary percutaneous coronary intervention (PCI).1)Dual antiplatelet therapy (DAPT), which is typically com-posed of aspirin and P2Y12 inhibitors such as clopidogrel or prasugrel, has been important for successful primary PCI, especially since the beginning of clopidogrel load-ing.2)
As compared to clopidogrel (loading 300 mg and maintenance 75 mg), prasugrel (loading 60 mg and main-tenance 10 mg) had a more potent antiplatelet effect, which was confirmed by randomized control trials in Western countries.3) However, the bleeding risk was
greater in prasugrel than in clopidogrel in those trials.3)
The dose of prasugrel was adjusted (loading 20 mg and maintenance 3.75 mg) for East Asian individuals in Japan, because the bleeding risk was considered to be greater in East Asian individuals than in White individu-als.4) A randomized trial showed that prasugrel (20 mg/
3.75 mg) was associated with a low incidence of ischemic events and a low risk of clinically serious bleeding up to 24 weeks in Japanese patients.5) However, the risks and
benefits of prasugrel over clopidogrel have not been fully discussed in real clinical practices. The purpose of this
study was to compare the 90-days clinical outcomes of AMI between prasugrel-based DAPT and clopidogrel-based DAPT.
Methods
Study design: We reviewed consecutive AMI patients
who underwent primary PCI at our medical center from January 2015 to December 2017. The exclusion criteria were the following: 1) DAPT was not continued for some reasons such as coronary artery bypass surgery, vasospas-tic angina, or no stent implantation, 2) DAPT was com-posed of aspirin and ticlopidine, 3) warfarin or direct oral anticoagulant (DOAC) was prescribed together with DAPT, and 4) final PCI procedure without drug-eluting stent implantation. The study patients were divided into the clopidogrel group, in which DAPT was composed of aspirin and clopidogrel, and the prasugrel group, in which DAPT was composed of aspirin and prasugrel. Clinical characteristics and outcomes were compared between the two groups. The primary endpoint for this study was the total ischemic events and total bleeding events. The total ischemic events were defined as the composite of cardiac
From the1
Division of Cardiovascular Medicine, Saitama Medical Center, Jichi Medical University, Saitama, Japan.
Address for correspondence: Kenichi Sakakura, MD, Division of Cardiovascular Medicine, Saitama Medical Center, Jichi Medical University, 1-847 Amanuma, Omiya, Saitama 330-8503, Japan. E-mail: [email protected]
Received for publication June 1, 2020. Revised and accepted November 25, 2020. Released in advance online on J-STAGE May 15, 2021.
doi: 10.1536/ihj.20-357
All rights reserved by the International Heart Journal Association.
death, nonfatal AMI, cerebral infarction, and ischemia-driven target vessel revascularization. The total bleeding events were defined as global utilization of streptokinase and tissue plasminogen activator for occluded coronary ar-teries (GUSTO) moderate/severe bleeding.6)
The day of admission was defined as the index day, and the patients were followed up until the primary endpoint or 90 days. This study was approved by the institutional review board, and written informed consent was waived because of the retrospective study design.
Definitions: The diagnosis of AMI required the following
criteria: symptoms consistent with AMI: elevated cardiac enzymes including troponin T, troponin I, and/or cre-atinine kinase (at least a twofold increase from the normal upper limit), and ST-segment elevation or depression in electrocardiograms compatible with AMI.7) Diagnostic ST
elevation was defined as new ST elevation at the J point in at least two contiguous leads of 2 mm (0.2 mV), and the AMI patients with ST elevation were diagnosed as ST elevation myocardial infarction (STEMI).8)
Hypertension was defined as a medical treatment for hypertension and/or a history of hypertension before ad-mission.7,9)
Dyslipidemia was defined as total cholesterol levels > 220 mg/dL or low-density lipoprotein cholesterol levels > 140 mg/dL or medical treatment for dyslipidemia or a history of dyslipidemia.10) Diabetes mellitus was
de-fined as a hemoglobin A1c level (as NGSP value) > 6.5% or a medical treatment for diabetes mellitus or a history of diabetes mellitus.11) Significant coronary artery stenosis
was defined as at least a 75% reduction in the internal di-ameter. Initial and final thrombosis in myocardial infarc-tion (TIMI) flow grades were recorded.12) The Predicting
Bleeding Complication in Patients Undergoing Stent Im-plantation and Subsequent Dual Antiplatelet Therapy (PRECISE-DAPT) score was also calculated to evaluate the bleeding risk according to the literature.13)All strokes
including cerebral infarction and hemorrhage were defined according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification.14)
Statistical analysis: Data were expressed as mean ±
stan-dard deviation (SD) for continuous variables and percent-age for categorical variables. Normally distributed con-tinuous variables were compared using the unpaired Stu-dent’s t-test. Other continuous variables were compared using the Mann-Whitney U-test. Categorical variables were presented as numbers and compared with Fisher’s exact test. Kaplan-Meier survival curves were constructed to investigate the total ischemic events-free survival and the bleeding events-free survival. We also performed mul-tivariate Cox hazard analysis to investigate the association between prasugrel and the total ischemic/bleeding events after controlling confounding factors. In this model, the total ischemic events or total bleeding events were used as a dependent variable, and prasugrel was used as an inde-pendent variable. Confounding factors were selected from variables that had a significant difference (P < 0.05) be-tween the clopidogrel and prasugrel groups in univariate comparisons. However, we did not include variables with substantial missing values, and the maximum number of independent variables was set as (number of total ischemic events)/10 or (number of total bleeding events)/
10.15) Hazard ratios (HRs) and 95% confidence intervals
(95% CIs) were also calculated. A P value < 0.05 was considered to be statistically significant. Propensity score matching was applied to compare the incidence of clinical outcome between the matched clopidogrel group and the matched prasugrel group. First, a logistic regression analy-sis was performed to calculate the propensity score using the full database. In this model, the prasugrel group was set as a dependent variable, whereas parameters that had a significant difference between the clopidogrel group and the prasugrel group in univariate analysis were set as in-dependent variables. Parameters with missing values were not included as independent variables. For matching, the match tolerance was set as a width of 0.25 multiplied by the SD of the propensity score distribution.16,17)All
analy-ses were performed with IBM SPSS statistics version 25 (Chicago, IL, USA).
Results
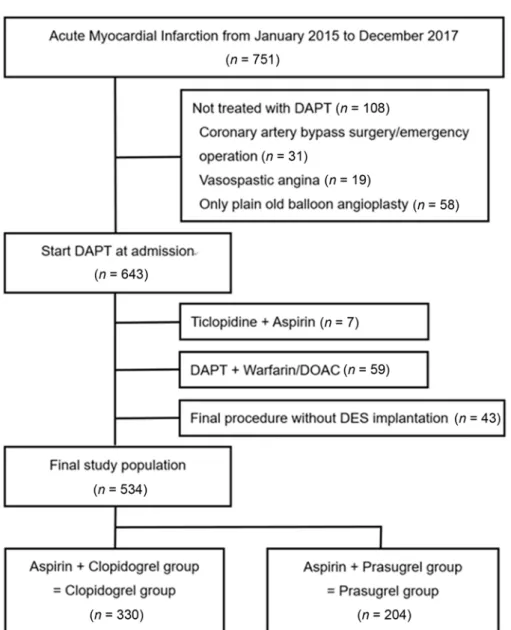
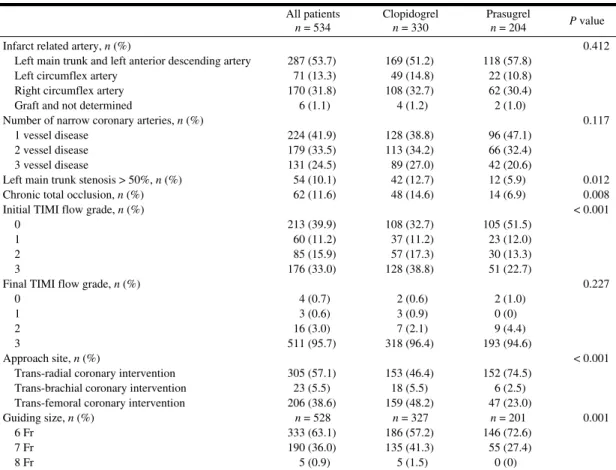
In all, 751 AMI patients were admitted to our hospi-tal during the study period. Among them, 217 patients were excluded from the analysis. The final study popula-tion consisted of 534 AMI patients, and they were divided into the clopidogrel group (n = 330) and the prasugrel group (n = 204) (Figure 1). Table I shows the comparison of the clinical characteristics between the two groups. The mean age was significantly older in the clopidogrel group (72.8 ± 11.9 years) than in the prasugrel group (63.9 ± 13.6 years) (P < 0.001). The prevalence of female sex was significantly greater in the clopidogrel group (30.0%) than in the prasugrel group (18.1%) (P = 0.002). Body mass index was significantly lower in the clopidogrel group (23.5 ± 3.5) than in the prasugrel group (24.7 ± 3.9) (P < 0.001). The prevalence of hemodialysis was significantly higher in the clopidogrel group (11.5%) than in the pra-sugrel group (2.9%) (P < 0.001). The PRECISE-DAPT score was significantly higher in the clopidogrel group (30 ± 14) than in the prasugrel group (21 ± 12) (P < 0.001). Table II shows the comparison of lesion and procedural characteristics between the two groups. Infarct-related ar-tery and number of narrowed coronary arteries were not different between the two groups. The prevalence of trans-femoral PCI was significantly greater in the clopidogrel group (48.2%) than in the prasugrel group (23.0%) (P < 0.001).
Table III shows the comparison of clinical outcomes between the two groups, and Kaplan-Meier curves were constructed to compare the clinical outcomes between the two groups (Figure 2). The total ischemic events-free sur-vival was similar between the clopidogrel group and the prasugrel group (P = 0.385). The total bleeding events-free survival was not different between the clopidogrel group and the prasugrel group (P = 0.125).
Table IV shows the results of multivariate Cox haz-ard analysis. The prasugrel group was not associated with the total ischemic events after controlling confounding factors (HR 0.955, 95% CI 0.499-1.829, P = 0.890). The prasugrel group was not associated with the total bleeding events after controlling confounding factors (HR 0.972, 95% CI 0.528-1.790, P = 0.927).
Figure 1. Study flow chart. DAPT indicates dual antiplatelet therapy.
To calculate the propensity score, we selected the fol-lowing parameters as independent variables: age, sex, height, STEMI (or NSTEMI), hypertension, malignancy, prior AMI, prior PCI, prior stroke, serum creatinine, cre-atine kinase, left main trunk stenosis, chronic total occlu-sion, and trans-femoral coronary intervention. After apply-ing the propensity score matchapply-ing, a matched clopidogrel group (n = 140) and a matched prasugrel group (n = 140) were generated for further analysis. The comparison of clinical characteristics between the two matched groups is shown in Supplemental Table I. Clinical characteristics were comparable between the two groups except for calcium-channel blocker before admission, β-blocker and diuretics at discharge, and brain natriuretic peptide on ad-mission. The comparison of lesion and procedural charac-teristics between the two matched groups is shown in Supplemental Table II. Lesion and procedural characteris-tics were comparable between the two groups except for approach site. The comparison of clinical outcomes
be-tween the two matched groups is shown in Supplemental Table III, and Kaplan-Meier curves were constructed to compare the clinical outcomes between the two matched groups (Supplemental Figure). The total ischemic events-free survival was similar between the two matched groups (P = 0.421), and the total bleeding events-free survival was significantly better in the prasugrel group than in the clopidogrel group (P = 0.007).
Discussion
In this retrospective study, we included 534 AMI pa-tients who underwent PCI and divided them into the clopidogrel group (n = 330) and the prasugrel group (n = 204). Regarding the efficacy of antiplatelet therapy, the to-tal ischemic events were not different between the clopi-dogrel group and the prasugrel group. Regarding the safety of antiplatelet therapy, the total bleeding events were not different between the clopidogrel group and the
Table I. Comparison of Clinical Characteristics between the Clopidogrel Group and the Prasugrel Group All patients n = 534 Clopidogrel n = 330 Prasugrel n = 204 P value Age (years) 69.4 ± 13.3 72.8 ± 11.9 63.9 ± 13.6 < 0.001 Female, n (%) 136 (25.5) 99 (30.0) 37 (18.1) 0.002 Height (cm) 162 ± 9.1 (n = 527) 160 ± 9.1 (n = 325) 164 ± 8.6 (n = 202) < 0.001 Body weight (kg) 63.2 ± 13.3 (n = 530) 61 ± 12.6 (n = 328) 67 ± 13.5 (n = 202) < 0.001 BMI 24.0 ± 3.7 (n = 527) 23.5 ± 3.5 (n = 325) 24.7 ± 3.9 (n = 202) < 0.001 STEMI, n (%) 331 (62.0) 189 (57.3) 142 (69.6) 0.004 Hypertension, n (%) 415 (77.7) 272 (82.4) 143 (70.1) 0.001 Diabetes mellitus, n (%) 228 (42.8) (n = 533) 141 (42.7) 87 (42.9) (n = 203) 1.000 Dyslipidemia, n (%) 323 (61.2) (n = 528) 184 (55.8) 139 (70.2) (n = 198) 0.001 Malignancy, n (%) 67 (12.5) 53 (16.1) 14 (6.9) 0.002 Current smoker, n (%) 187 (35.4) (n = 528) 93 (28.4) (n = 328) 94 (47.0) (n = 200) < 0.001 Hemodialysis, n (%) 44 (8.2) 38 (11.5) 6 (2.9) < 0.001 Prior AMI, n (%) 53 (9.9) 42 (12.7) 11 (5.4) 0.007 Prior PCI, n (%) 72 (13.5) 60 (18.2) 12 (5.9) < 0.001 Prior CABG, n (%) 17 (3.2) 14 (4.2) 3 (1.5) 0.125 Prior stroke, n (%) 66 (12.4) 61 (18.5) 5 (2.5) < 0.001 Medication before admission, n (%)
Statin 156 (31.1) (n = 501) 115 (36.6) (n = 314) 41 (21.9) (n = 187) 0.001 ACEI/ARB 181 (36.2) (n = 500) 130 (41.4) (n = 314) 51 (28.2) (n = 186) 0.002 β-Blocker 97 (19.4) (n = 500) 72 (22.9) (n = 314) 25 (13.4) (n = 186) 0.01 Calcium-channel blocker 189 (37.8) (n = 500) 139 (44.3) (n = 314) 50 (26.9) (n = 186) < 0.001 Diuretics 46 (9.2) (n = 501) 39 (12.4) (n = 314) 7 (3.7) (n = 187) 0.001 Oral hypoglycemia agent 120 (24.0) (n = 501) 72 (22.9) (n = 314) 48 (25.7) (n = 187) 0.517 Insulin 31 (6.2) (n = 503) 20 (6.3) (n = 315) 11 (5.9) (n = 188) 1.000 Medication at discharge, n (%) Statin 492 (96.3) (n = 511) 300 (95.2) (n = 315) 192 (98.0) (n = 196) 0.15 ACEI/ARB 449 (87.9) (n = 511) 267 (84.8) (n = 315) 182 (92.9) (n = 196) 0.008 β-Blocker 484 (94.7) (n = 511) 291 (92.4) (n = 315) 193 (98.5) (n = 196) 0.002 MRA 60 (11.7) (n = 511) 46 (14.6) (n = 315) 14 (7.1) (n = 196) 0.011 Diuretics 120 (23.5) (n = 511) 96 (30.5) (n = 315) 24 (12.2) (n = 196) < 0.001 Switch to clopidogrel or prasugrel during admission 11 (2.1) 4 (1.2) 7 (3.4) 0.114 Systolic blood pressure on admission (mmHg) 141 ± 32 (n = 530) 140 ± 32 (n = 327) 142 ± 32 (n = 203) 0.673 Diastolic blood pressure on admission (mmHg) 80 ± 20 (n = 524) 78 ± 20 (n = 321) 84 ± 20 (n = 203) 0.002 Heart rate on admission (/minute) 81 ± 22 (n = 531) 81 ± 24 (n = 328) 80 ± 19 (n = 203) 0.557 Killip, n (%) 0.001
1or 2 426 (79.8) 254 (77.0) 172 (84.3) 3 47 (8.8) 41 (12.4) 6 (2.9) 4 61 (11.4) 35 (10.6) 26 (12.7)
Cardiac arrest before admission, n (%) 33 (6.2) 16 (4.8) 17 (8.3) 0.138 Cardiac shock, n (%) 68 (12.7) 42 (12.7) 26 (12.7) 1.000 IABP, n (%) 35 (6.6) 23 (7.0) 12 (5.9) 0.720 ECMO, n (%) 23 (4.3) 15 (4.5) 8 (3.9) 0.828 Serum creatinine (mg/dL) 1.52 ± 2.12 1.84 ± 2.55 1.01 ± 0.92 < 0.001 Creatine kinase (IU/L) 1833 ± 2888 1529 ± 2225 2324 ± 3672 0.006 Creatine kinase myocardial band (IU/L) 165 ± 236 (n = 533) 138 ± 205 (n = 329) 209 ± 274 0.002 Brain natriuretic peptide on admission (pg/mL) 359 ± 633 (n = 502) 482 ± 748 (n = 310) 161 ± 285 (n = 192) < 0.001 PRECISE-DAPT score 27 ± 14 (n = 533) 30 ± 14 21 ± 12 (n = 192) < 0.001 LVEF in hospital (%) 54 ± 14 (n = 528) 52 ± 14 (n = 325) 56 ± 12 (n = 203) 0.002 Categorical variables were compared using Fisher’s exact test. Normally distributed continuous variables were compared using the unpaired Stu-dent’s t-test. Non-normally distributed continuous variables were compared using the Mann–Whitney U-test. BMI indicates body mass index; STEMI, ST-segment elevation myocardial infarction; AMI, acute myocardial infarction; PCI, percutaneous coronary intervention; CABG, coro-nary artery bypass graft surgery; ACEI, angiotensin converting enzyme inhibitor; ARB, angiotensin II receptor blocker; MRA, mineralocorticoid receptor antagonist; IABP, intra-aortic balloon pumping; ECMO, extracorporeal membrane oxygenation; PRECISE-DAPT, Predicting Bleeding Complication in Patients Undergoing Stent Implantation and Subsequent Dual Antiplatelet Therapy; and LVEF, left ventricular ejection fraction.
prasugrel group. The multivariate Cox hazard models showed that the total ischemic events and the total bleed-ing events were not different between the prasugrel group and the clopidogrel group after controlling confounding factors. However, in the propensity score matching
analy-sis, the total bleeding events were significantly less in the prasugrel group than in the clopidogrel group. Our results support the fact that the current regimen of prasugrel ad-justed for the Asian population would not increase the risk of bleeding as compared to clopidogrel.
Table II. Comparison of Lesion and Procedural Characteristics between the Clopidogrel Group and the Prasugrel Group All patients n = 534 Clopidogrel n = 330 Prasugrel n = 204 P value
Infarct related artery, n (%) 0.412 Left main trunk and left anterior descending artery 287 (53.7) 169 (51.2) 118 (57.8)
Left circumflex artery 71 (13.3) 49 (14.8) 22 (10.8) Right circumflex artery 170 (31.8) 108 (32.7) 62 (30.4) Graft and not determined 6 (1.1) 4 (1.2) 2 (1.0)
Number of narrow coronary arteries, n (%) 0.117 1 vessel disease 224 (41.9) 128 (38.8) 96 (47.1)
2 vessel disease 179 (33.5) 113 (34.2) 66 (32.4) 3 vessel disease 131 (24.5) 89 (27.0) 42 (20.6)
Left main trunk stenosis > 50%, n (%) 54 (10.1) 42 (12.7) 12 (5.9) 0.012 Chronic total occlusion, n (%) 62 (11.6) 48 (14.6) 14 (6.9) 0.008 Initial TIMI flow grade, n (%) < 0.001
0 213 (39.9) 108 (32.7) 105 (51.5) 1 60 (11.2) 37 (11.2) 23 (12.0) 2 85 (15.9) 57 (17.3) 30 (13.3) 3 176 (33.0) 128 (38.8) 51 (22.7)
Final TIMI flow grade, n (%) 0.227 0 4 (0.7) 2 (0.6) 2 (1.0)
1 3 (0.6) 3 (0.9) 0 (0) 2 16 (3.0) 7 (2.1) 9 (4.4) 3 511 (95.7) 318 (96.4) 193 (94.6)
Approach site, n (%) < 0.001 Trans-radial coronary intervention 305 (57.1) 153 (46.4) 152 (74.5)
Trans-brachial coronary intervention 23 (5.5) 18 (5.5) 6 (2.5) Trans-femoral coronary intervention 206 (38.6) 159 (48.2) 47 (23.0)
Guiding size, n (%) n = 528 n = 327 n = 201 0.001 6 Fr 333 (63.1) 186 (57.2) 146 (72.6)
7 Fr 190 (36.0) 135 (41.3) 55 (27.4) 8 Fr 5 (0.9) 5 (1.5) 0 (0)
Categorical variables were compared using Fisher’s exact test. Normally distributed continuous variables were compared using the unpaired Student’s t-test. Non-normally distributed continuous variables were compared using the Mann–Whitney U-test. TIMI indi-cates thrombolysis in myocardial infarction.
We should discuss why the incidence of ischemic events was not different between the two groups. First, the possible explanation was that the current regimen of pra-sugrel (20 mg loading and 3.75 mg maintenance) was not sufficient to prove the superiority of efficacy over clopido-grel, because the current regimen of prasugrel was more conservative as compared to the regimen of the Western dose (60 mg loading and 10 mg maintenance). However, the overall incidences of ischemic events were relatively low in both the clopidogrel and prasugrel groups as com-pared to those in Western countries.18) Thus, the
clopido-grel group as well as the prasuclopido-grel group might suffi-ciently suppress the incidence of ischemic events, which supports the fact that the current reduced dose of pra-sugrel was appropriate for the Japanese population. Sec-ond, the nonsignificant difference between the two groups might be caused by beta error due to the small sample size.19) As our retrospective observation study could not
perform sample size calculation, our study population might be too small to find the difference of ischemic events between the two groups.
Moreover, we should discuss why the incidence of bleeding events was not different between the two groups in the unadjusted comparison and the multivariable Cox hazard model, but the incidence of bleeding was
signifi-cantly less in the prasugrel group than in the clopidogrel group after propensity score matching. A randomized trial in White individuals showed that prasugrel had higher bleeding risk than clopidogrel.20)
Although the dose of pra-sugrel was adjusted for East Asian individuals in Japan, the safety of prasugrel in the adjusted dose was not widely recognized in Japan. Akita et al. reported the greater risk of bleeding following reduced-dose prasugrel as compared to that following clopidogrel.21) Although
their results were drawn from the large multicenter regis-try in Japan (J-PCI regisregis-try), only in-hospital outcomes were investigated, whereas acute and mid-term outcomes were not available.21)Yasuda et al. reported the lower risk
of bleeding following reduced-dose prasugrel as compared to that following clopidogrel in the JAMIR study.22) The
JAMIR study is a multicenter, nationwide, prospective registry enrolling 3069 patients with 12-months follow-up.22)Our results of the propensity score matching
analy-sis were similar to those of the JAMIR study. However, the incidence of ischemic and bleeding events was greater in the present study than in the JAMIR study, partly be-cause our study included patients with no return of spon-taneous circulation on admission after out-of-hospital car-diopulmonary arrest.
Figure 2. Kaplan–Meier survival curves of clinical events between the clopidogrel group and the prasugrel group. A: Comparison of total ischemic events. B: Comparison of total bleeding events. Log-rank test. AMI indicates acute myocardial infarction; and TVR, target vessel revascularization.
Table III. Comparison of 90-Day Clinical Outcomes between the Clopidogrel Group and the Prasugrel Group All patients n = 534 Clopidogrel n = 330 Prasugrel n = 204 P value
Total ischemic event 52 (9.7) 35 (10.6) 17 (8.3) 0.454 Cardiac death 25 (4.7) 17 (5.2) 8 (3.9) 0.674 Nonfatal AMI 11 (2.1) 8 (2.4) 3 (1.5) 0.544 Cerebral infarction 13 (2.4) 11 (2.1) 2 (1.0) 0.145 Ischemia-driven TVR 16 (3.0) 8 (2.4) 8 (3.9) 0.434 Total bleeding event 64 (12.0) 45 (13.6) 19 (9.3) 0.093 Moderate GUSTO bleeding classification 57 (10.7) 42 (12.7) 15 (7.4) 0.346
Bleeding site Neck 1 (0.2) 1 (0.3) 0 (0) Chest 1 (0.2) 0 (0) 1 (0.5) Upper extremity 3 (0.6) 3 (0.9) 0 (0) Pelvis 4 (0.7) 3 (0.9) 1 (0.5) Lower extremity 14 (2.6) 11 (3.3) 3 (1.5) Unspecified but required blood transfusion due to surgery 5 (0.9) 3 (0.9) 2 (1.0) Unspecified 29 (5.4) 21 (6.4) 8 (3.9)
Severe GUSTO bleeding classification 7 (1.4) 3 (0.9) 4 (2.0) 0.259 Bleeding site
Cerebral hemorrhage 1 (0.2) 1 (0.3) 0 (0) Abdominal pelvis 2 (0.4) 0 (0) 2 (1.0) Pericardial effusion 4 (0.8) 2 (0.6) 2 (1.0)
Categorical variables were compared using Fisher’s exact test. AMI indicates acute myocardial infarction; TVR, target vessel revas-cularization; GUSTO, global utilization of streptokinase and tissue plasminogen activator for occluded coronary arteries.
be noted. Recent clinical trials, including the STOPDAPT-2 trial, support the short duration of DAPT.23) The
Japa-nese Circulation Society conducted a focused update on antithrombotic therapy in patients with coronary artery disease, which recommends 1-3 months DAPT for pa-tients with high bleeding risk.24) If patients do not have
high bleeding risk, 3-12 months DAPT is recommended for patients with high thrombotic risk, and 1-3 months DAPT is recommended for patients with low thrombotic risk.24)
Therefore, 3 months DAPT is suitable for all types of patients unless patients have oral antithrombotic ther-apy. Because our study set the follow-up period as 90 days, our study results would be easily applicable to the contemporary clinical practice.
Study limitations: The present study has the following
limitations. Because this study was a single-center retro-spective observational study, there was a risk of selection bias. As the choice of drugs (prasugrel or clopidogrel) was not randomly assigned to patients, there should be a substantial selection bias regarding the selection of such drugs. It is well known that CYP2C19 polymorphisms are frequent in the Japanese.25) The antiplatelet effects of
clopidogrel might be affected by CYP2C19 polymor-phisms, which were not checked in our daily clinical practice. Although we performed multivariate Cox hazard analysis to control confounding factors, we could not ad-just potential confounding factors. Because we excluded patients who had warfarin or DOAC, we could not exam-ine the efficacy and safety regarding triple antithrombotic therapy. As our institution was a tertiary university
hospi-Table IV. Multivariate Cox Hazard Models to Predict Total Ischemic Events and Total Bleeding Events Hazard ratio 95% confidence interval P value
Model 1. Dependent variable: total ischemic events
Prasugrel (versus clopidogrel) 0.955 0.499–1.829 0.890 Age (1 year incremental) 1.010 0.985–1.036 0.437 Current smoker 1.081 0.557–2.096 0.819 Serum creatinine 1.105 1.004–1.217 0.041 Prior PCI 1.112 0.512–2.412 0.789 Model 2. Dependent variable: total bleeding events
Prasugrel (versus clopidogrel) 0.972 0.528–1.790 0.927 Age (1 year incremental) 1.047 1.020–1.074 0.001 Current smoker 1.548 0.858–2.794 0.147 Serum creatinine 1.093 0.998–1.197 0.055 Prior PCI 0.806 0.379–1.714 0.575 Trans-femoral coronary intervention 1.480 0.864–2.535 0.153 All variables are adjusted in one step. PCI indicates percutaneous coronary intervention.
tal, patients were referred to their primary care physicians at discharge. We wrote a letter for primary care physicians including the recommended duration of DAPT, which was at least 90 days (3 months) during the study period. Al-though we expected that all patients had DAPT until 90 days, we could not confirm whether DAPT was continued in each patient as recommended. Moreover, there is a pos-sibility that the regimen of DAPT was changed after the hospital discharge.
Conclusion
As compared to clopidogrel, the reduced dose of pra-sugrel was not associated with the excess risk of bleeding or the excess risk of ischemic events. Our real-world data support the current regimen of prasugrel for patients with AMI.
Acknowledgments
The authors acknowledge all staff in the catheter laboratory and cardiology units in Jichi Medical Univer-sity, Saitama Medical Center for their technical support in this study.
Disclosure
Conflicts of interest: Dr. Sakakura has received speaking
honoraria from Abbott Vascular, Boston Scientific, Med-tronic Cardiovascular, Terumo, OrbusNeich, Japan Life-line, Kaneka, Daiichi-Sankyo, Sanofi, and NIPRO; he has served as a proctor for Rotablator for Boston Scientific and as a consultant for Abbott Vascular and Boston Scien-tific. Dr. Taniguchi has received speaking honoraria from Daiichi-Sankyo and Sanofi. Dr. Yamamoto has received speaking honoraria from Daiichi-Sankyo and Sanofi. Dr. Wada has received speaking honoraria from Daiichi-Sankyo. Prof. Fujita has served as a consultant for Meher-gen Group Holdings, Inc. and has received speaking honoraria from Daiichi-Sankyo and Sanofi. The other authors declare no conflict of interest.
References
1. Dégano IR, Salomaa V, Veronesi G, et al. Twenty-five-year trends in myocardial infarction attack and mortality rates, and case-fatality, in six European populations. Heart 2015; 101: 1413-21.
2. Sabatine MS, Cannon CP, Gibson CM, et al. Effect of clopido-grel pretreatment before percutaneous coronary intervention in patients with ST-elevation myocardial infarction treated with fi-brinolytics: the PCI-CLARITY study. JAMA 2005; 294: 1224-32.
3. Wiviott SD, Braunwald E, McCabe CH, et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med 2007; 357: 2001-15.
4. Levine GN, Jeong YH, Goto S, et al. Expert consensus docu-ment: World Heart Federation expert consensus statement on antiplatelet therapy in East Asian patients with ACS or undergo-ing PCI. Nat Rev Cardiol 2014; 11: 597-606.
5. Saito S, Isshiki T, Kimura T, et al. Efficacy and safety of adjusted-dose prasugrel compared with clopidogrel in Japanese patients with acute coronary syndrome: the PRASFIT-ACS study. Circ J 2014; 78: 1684-92.
6. Mehran R, Rao SV, Bhatt DL, et al. Standardized bleeding defi-nitions for cardiovascular clinical trials: a consensus report from the Bleeding Academic Research Consortium. Circulation 2011; 123: 2736-47.
7. Watanabe Y, Sakakura K, Taniguchi Y, et al. Determinants of slow flow in percutaneous coronary intervention to the culprit lesion of non-ST elevation myocardial infarction. Int Heart J 2018; 59: 1237-45.
8. Tsukui T, Sakakura K, Taniguchi Y, et al. Determinants of short and long door-to-balloon time in current primary percutaneous coronary interventions. Heart Vessels 2018; 33: 498-506. 9. Noguchi M, Sakakura K, Akashi N, et al. The comparison of
clinical outcomes between inferior ST-elevation myocardial in-farction with right ventricular inin-farction versus without right ventricular infarction. Int Heart J 2019; 60: 560-8.
10. Sawano S, Sakakura K, Yamamoto K, et al. Further validation of a novel acute myocardial infarction risk stratification (nARS) system for patients with acute myocardial infarction. Int Heart J 2020; 61: 463-9.
11. Yamamoto K, Sakakura K, Akashi N, et al. Clinical outcomes after acute myocardial infarction according to a novel stratifica-tion system linked to a rehabilitastratifica-tion program. J Cardiol 2018; 72: 227-33.
12. Helal AM, Shaheen SM, Elhammady WA, Ahmed MI, Abdel-Hakim AS, Allam LE. Primary PCI versus pharmacoinvasive strategy for ST elevation myocardial infarction. Int J Cardiol Heart Vasc 2018; 21: 87-93.
13. Costa F, van Klaveren D, James S, et al. Derivation and valida-tion of the predicting bleeding complicavalida-tions in patients under-going stent implantation and subsequent dual antiplatelet ther-apy (PRECISE-DAPT) score: a pooled analysis of individual-patient datasets from clinical trials. Lancet 2017; 389: 1025-34. 14. Adams HP Jr, Bendixen BH, Kappelle LJ, et al. Classification
of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in acute stroke treatment. Stroke 1993; 24: 35-41.
15. Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol 1996; 49: 1373-9. 16. Cavender MA, Norhammar A, Birkeland KI, et al. SGLT-2
in-hibitors and cardiovascular risk: an analysis of CVD-REAL. J Am Coll Cardiol 2018; 71: 2497-506.
17. Stuart EA. Matching methods for causal inference: a review and a look forward. Stat Sci 2010; 25: 1-21.
18. Kang J, Park KW, Palmerini T, et al. Racial differences in is-chaemia/bleeding risk trade-off during anti-platelet therapy: in-dividual patient level landmark meta-analysis from seven RCTs. Thromb Haemost 2019; 119: 149-62.
19. Jenny JY. [Beta risk: an unrecognized risk of statistical error]. Rev Chir Orthop Réparatrice Appar Mot 2001; 87: 170-2. 20. Montalescot G, Wiviott SD, Braunwald E, et al. Prasugrel
com-pared with clopidogrel in patients undergoing percutaneous coronary intervention for ST-elevation myocardial infarction (Triton-TIMI 38): double-blind, randomised controlled trial. Lancet 2009; 373: 723-31.
21. Akita K, Inohara T, Yamaji K, et al. Impact of reduced-dose
prasugrel vs. standard-dose clopidogrel on in-hospital outcomes of percutaneous coronary intervention in 62,737 patients with acute coronary syndromes: a nationwide registry study in Japan. Eur Heart J Cardiovasc Pharmacother 2020; 6: 231-8.
22. Yasuda S, Honda S, Takegami M, et al. Contemporary antiplate-let therapy and clinical outcomes of Japanese patients with acute myocardial infarction-Results from the prospective Japan acute myocardial infarction Registry (JAMIR). Circ J 2019; 83: 1633-43.
23. Watanabe H, Domei T, Morimoto T, et al. Effect of 1-month dual antiplatelet therapy followed by clopidogrel vs 12-month dual antiplatelet therapy on cardiovascular and bleeding events in patients receiving PCI: the STOPDAPT-2 randomized clinical trial. JAMA 2019; 321: 2414-27.
24. Nakamura M, Kimura K, Kimura T, et al. JCS 2020 guideline focused update on antithrombotic therapy in patients with coro-nary artery disease. Circ J 2020; 84: 831-65.
25. Jinnai T, Horiuchi H, Makiyama T, et al. Impact of CYP2C19 polymorphisms on the antiplatelet effect of clopidogrel in an ac-tual clinical setting in Japan. Circ J 2009; 73: 1498-503.
Supplemental Files Supplemental Tables I-III
Supplemental Figure