Synergistic effect of the combination of corticosteroids and long acting-/32 agonists on inhibiting the in vitro proliferation of T cells isolated from asthmatic patients
Ryuta Hiroyuki
Haraguchi,' Hitomi Zushi,2 Katsuyuki Tomita,2 Hiroyuki Sano,2 Miyajima,2 Keizoh Tsukamoto,2 Hiroshi Santoh,2 Takayuki Miyara,2
Yuji Higashimoto2 and Yuji Tohda2 'Department of Respiratory
2Department of Respiratory
Medicine, Higashiosaka City General Hospital, 3-4-5 Nishi-Iwata,
Higashiosaka, Japan
Medicine and Allergology, Kinki University Faculty of Medicine, Osakasayama, Osaka 589-8511, Japan
Abstract
The clinical efficacy of inhaled corticoster- oids (ICS) combined with long-acting ,32-
agonists (LABA) has been widely demonstrated in asthma. In order to validate the benefits of
the combination of these agents in vitro, we studied the inhibitory effect of fluticasone propionate (FP) or salmeterol either alone or in-
combination on the proliferation of T cells. In the present study, peripheral blood mononuclear cells (PBMCs) from asthmatic patients were stimulated with phytohemagglutinin (PHA) for four days in the presence of FP and/or salmeter- ol. We assessed cell proliferation by quantifying
the fluorescence of carboxyfluorescein diacetate succinimidyl ester (CFSE) in CD3+ cells using flow cytometry. A high concentration (10-8 M), but not a low concentration (10-12 M) of FP
alone inhibited PHA-induced T cell prolifera- tion, while salmeterol alone did not have any effect. The combination of FP (10-12 M) and salmeterol inhibited PHA-induced T cell prolif- eration, however, the combination of FP (10-12 M) and salbutamol, which is another short- acting g2-agonist, did not inhibit PHA-induced T cell proliferation. This study shows that the combination of a low concentration of FP and salmeterol synergistically inhibits lymphocyte proliferation in vitro. This novel synergistic interaction of ICS and LABA may partly explain the benefits that result when these agents are given in combination to treat asthma.
Key words : asthma, inhaled corticosteroids, synergic effect
Introduction
The addition of an inhaled long-acting /32- adrenoceptor agonist (LABA) to an inhaled corticosteroid (ICS) is more effective for improv- ing asthma control, reducing exacerbations re- quiring oral steroids, and reducing the use of rescue /3-agonists better than increasing the dose of ICS.1-6 This is further illustrated by the recent demonstration that the combination of formoterol/beclomethasone in a single inhaler is
equivalent to formoterol/budesonide and sal- meterol/fluticasone with respect to asthma con- trol, rate of asthma exacerbation, and the fre- quency of adverse events.7-9 With regard to the combination of these agents, a meta-analysis comparing four studies in which the same doses of salmeterol and fluticasone were administered either separately or in the same canisters suggest- ed that there was a synergy between LABA and ICS." The effects of combination treatment with ICS and LABA have been attributed to their
Received January 20, 2011 ; Accepted March 16, 2011
23
anti-inflammatory and bronchodilator effects.
Some papers have reported that in vitro inter- actions between glucocorticoids and fl2- adrenoceptors underlie their additive anti- inflammatory effects on mast cells," airway smooth muscle cells" and lymphocytes."'" In contrast to this additive effect, a synergic effect is characterized by a result obtained from a combi- nation of two drugs at low concentrations, at which neither of the drugs alone are effective. A study reported by Aziz and colleagues" demon- strated that the combination of a low concentra- tion of fluticasone propionate (FP) and salmeter- ol induced apoptosis in peripheral blood T cells to an extent that was equivalent to a higher concentration of FP alone," however, another study indicated that the FP-salmeterol combina- tion acts synergistically only in healthy controls but not in asthmatic patients.16
Until recently, cell proliferation was only amenable to study by standardized thymidine incorporation methods,' which measure bulk cell division over a narrow window of time, or BrdU incorporation" to identify cells which have recently divided. However, these methods cannot determine which cell subpopulations have proliferated or how many cycles of divi- sions have taken place. Carboxyfluorescein diacetate succinimidyl ester (CFSE), a fluores- cent dye staining living cells in vitro, provides a powerful tool to monitor cell migration, and to quantify cell division in separated cell subpopulations, because of the sequential decrease in fluorescent labeling in daughter
In order to investigate the possible synergistic effect of the combination of FP and salmeterol on inhibiting cell proliferation, we analyzed CFSE dye fluorescence using flow cytometry in phytohemagglutinin (PHA)-stimulated PBMCs isolated from patients with asthma.
Methods
Study Population
We recruited seven volunteers with ICS-naive asthma for this study. All of the subjects met the following criteria : (1) meeting the definition of asthma proposed by the American Thoracic Society (ATS)" ; (2) confirmation of a >20%
improvement in force expiratory volume in 1 s (FEY,) or peak expiratory flow (PEF) values after the inhalation of A-agonists (salbutamol
200 ,u g) ; (3) no smoking history ; and (4) no exacerbation over the preceding 4 weeks.
Separation of peripheral blood mononuclear cells
Peripheral blood mononuclear cells (PBMCs) were isolated from heparinized blood samples by means of density gradient centrifugation over Histopaque ® -1077 (Sigma, St. Louis, MO, USA), washed twice in PBS (MP Biomedicals, LLC, OH, USA), and were cultured for 4 days in 24-well round-bottomed culture plates (Becton Dickinson, Labware, NJ, USA) at 1 X 106 cells per well in RPMI with 10% FCS media in the absence or presence of 5 ,ug/mL PHA. FP, 10-12 to 10-7 M, was used to assess the response of cells to steroids. A concentration of 10-12 to 10-11 M FP was found to be the suboptimal concentra- tion that did not inhibit T cell proliferation when cells were treated with PHA. These con- centrations were used in combination with differ- ent concentrations of salmeterol (10-12 to 10-7 M) and a concentration of salbutamol (10-7 M) to determine the potential anti-proliferative effects of such drug combinations.
CFSE staining
CFSE in the form of a 5 mM stock solution in DMSO was added to give a final concentration of 5 ,u M. The procedure was performed under the CFSE labeling protocol described by Quah and colleagues,2° which allows the detection of up to eight cell divisions before CFSE fluores- cence is decreased to the background level of fluorescence in unlabeled cells.
Flow cytometry analysis
In the present study, PBMCs from asthmatic patients were cultured for four days in the pres- ence of FP and/or salmeterol, labeled with CFSE for 1 h, and assayed for PHA-induced proliferation. On day 4, cells were stained with a fluorescently conjugated monoclonal antibody (mAb), anti-CD3-PE (BD Biosciences, NJ, USA), or an isotype- matched control. Cells were analyzed by flow cytometry with logarith- mic detection of green (CFSE) and red fluores- cence (PE). The inhibition of T cell prolifera- tion was measured using the division index=
(100-Y)/Y, where Y(%)= Do/ 2°±D1/ 21+ D2/
22+1)3/23+ D4/24 + D5/26, and Do represents the percentage of T cell blasts that have not divided, and D1_, represents those within progressive CFSE division gates. A division index of 1 therefore represents one mitosis for every T cell added to the culture, with higher or lower values
24
representing greater or lesser mitotic activity.
Data Analysis
One-way analysis of variance (ANOVA) (Kruskal-Wallis) and Duncan's multiple range tests were conducted to statistically analyze the division index. A p value of less than 0.05 was considered to be statistically significant. A sta- tistical analysis was performed using the SPSS statistical software program (SPSS v. 16.0, SPSS Inc., Chicago, IL, USA).
Results
A major advantage of the CFSE technique is the ability to quantitatively analyze T cell responses in mixed populations, allowing re- sponder frequencies to be calculated. When PBMCs were cultured in the absence of PHA, the cells did not divide into daughter cells (Do) (Figure 1A). Figure 1B demonstrates that CFSE labeling prior to culture allows the identification of at least six discrete division cycles (D6) in PBMCs cultured with PHA for 4 days. A high concentration of FP (10-8 M) alone (Figure 1C), but not a low concentration of FP (10-" M) alone (Figure 1D), inhibited PHA-induced T- cell proliferation, while salmeterol alone (Figure 1E) had no effect. The combination of FP (10-12 M) and salmeterol inhibited PHA-induced T cell proliferation (Figure 1F), however, a combina- tion of FP (10-12 M) and salbutamol did not
inhibit PHA-induced T cell proliferation (Fig- ure 1G).
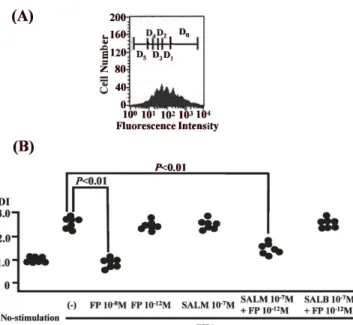
When T cell proliferation was measured using the division index, 62% of T-cells stimulated with PHA showed proliferation (Figure 2). The Kruskal-Wallis test indicated significant differ- ences between the groups (p < 0.01). The Dun- can's multiple range tests revealed that a high concentration of FP (10-8 M) alone or the com- bination of FP (10-12 M) and salmeterol signifi- cantly inhibited PHA-induced T cell prolifera- tion compared to the control (P < 0.01) (Figure 2)
Discussion
In the present study, the proliferation of PBMCs, which was stimulated by PHA, was assessed by quantifying the fluorescence of CFSE in CD3+ cells by flow cytometric analysis.
We found that the combination of a low concen- tration of FP and salmeterol is able to inhibit the proliferation of lymphocytes by a synergistic interaction.
To our knowledge, this is the first study to report that the FP-salmeterol interaction has synergic effects against the proliferation of PHA- stimulated lymphocytes. Our result was concor- dant with another paper by Pace and col- leagues15 which demonstrated that the combina- tion of FP and salmeterol is able to control
Fig. 1
(A)
200- 6160 .tt'. s 120-,
4 801
40c,.) 0
10° 101 102 103 104 Fluorescence Intensity
(B) (C) (D)
200 200 .— 200.!
6 160 y 160,,
4=.1.1604
E E120:, ZE120,,E120=
4801 4 801 4801
c..) 40 .1,40640.340-340-44600004'
0
0 ' ' ' (1'
10° 10' 102 103 1 4 10° 101 102 103 104 10. 101 102 103 104 Fluorescence Intensity Fluorescence Intensity Fluorescence Intensity
(E) (F) (G)
200 - ' 200 200
,.161x 1,160; 1,160 Z
Z 1 .
4= E121E1204 51211
4 81 Z 80 Z=i 80 1
c'T') 41 , '.'''4o],c.,,401
A 3/4,0;'''C) 0. 1' ' ' ' 01 '
10° 101 102 103 104 10° 10' 102 103 104 10° 10' 102 103 104 Fluorescence Intensity Fluorescence Intensity Fluorescence Intensity
profile of PHA-induced T cell proliferation. Peripheral blood mononu- ncubated for 4 days in the absence (A) or presence (B : filled histogram) entration of FP alone (FP 10-6 M) (C : grey line), a low concentration ) (D : grey line), salmeterol alone, and with a combination of a low
10-12 M) (E : grey line) and salmeterol (10-6 M) (F : grey line) or grey line). We assessed cell proliferation by quantifying the fluorescence by flow cytometric analysis. The figure denotes histograms of CFSE Representative inhibition profile of PHA-induced T cell proliferation. Periphe
clear cells (PBMCs) were incubated for 4 days in the absence (A) or presence (B of PHA, with a high concentration of FP alone (FP 10-8 M) (C : grey line), a of FP alone (FP 10-" M) (D : grey line), salmeterol alone, and with a con concentration of FP (FP 10-12 M) (E : grey line) and salmeterol (10-6 M) salbutamol (10-6 M) (G : grey line). We assessed cell proliferation by quantifyi of CFSE in CD3 T cells by flow cytometric analysis. The figure denotes hi fluorescence in gated CD3 T cells.
25
(A)
(B)
200
b,160IDo
I
E1z0 D5 D, Di Z 80
40 AAA
0 Y11.4:00:11.
100 101 102 103 104 Fluorescence Intensity
P<0.01
Fig. 2 The numbers of cells in each division cycle allows a graphical representation of division kinetics to be made (A) and analyzed using the division index (DI) of the synergic effect on inhibiting proliferation in PHA-stimulat- ed PBMCs from asthmatic patients (B) (n=
7). The division index (DI) was calculated as : Division index (DI)=(100-Y)/Y, where Y(%)=130/2°-FD1/21-FD2/22+1)3/23+ D,/
24+1)5/25. Dn indicates the number of divi- sions.
peripheral blood T cell activation in asthmatic patients more efficiently than FP alone, and with a lower concentration of steroids and using thymidine incorporation.
Given that salmeterol monotherapy does not produce anti-inflammatory effects, other path- ways may exist by which salmeterol enhances the activity of FP. According to a traditional knowledge, agonism of g2-adrenoceptors by sal- meterol augments the activity of adenylyl cyclase, leading to cAMP accumulation, activa- tion of cAMP-dependent protein kinase (PKA), and the induction of functional responses such as airway smooth muscle relaxation .2' It was re- ported that the synergy between FP and salmeter- ol was related to increased nuclear translocation of the GR.16.22-23 Consistent with the clinical situation, in the human bronchial epithelial cell line BEAS-2B, the addition of a /32-adrenoceptor agonist to a glucocorticoid was steroid-sparing, in that the maximal glucocorticoid response element (GRE)-dependent responses evoked by glucocorticoid were achieved at approximately
10-fold lower concentrations in the presence of the /32-adrenoceptor agonist, and this effect oc- curred via the classical cAMP-PKA pathway.24
Our study indicated that inhibition of cell proliferation by the combination of FP-salmeter- ol occurred during the early phase of prolifera- tion. In our study, we showed that 4-day culture of PBMCs with PHA induced six division cycles, and the high concentration of FP and the combi- nation of FP-salmeterol inhibited the division of cells during the early stage, because our data demonstrated inhibition of cell division at the
4th 4 (D4) and 5th divisions (D5).
There are some limitations to this study, in- cluding the number of subjects. Only seven subjects were recruited, therefore, the risk of a type-2 error was possible, however, some features were significantly different during the time course. Another consideration is that this study did not assess other subpopulations of T cells, such as suppressor T cells (CD8) and regulatory T cells. Interleukin-10-secreting "regulatory" T cells are induced by glucocorticoids and P2- agonists.13 Future studies will be required to investigate cell proliferation among subpopula- tions of T cells. Third, in our study, as we added a concentration of salbutamol as short-acting /32- agonist, it is difficult to conclude no effect of short-acting /32-agonist on T cell proliferation.
In the present study, there is synergism between FP and salmeterol with regard to the inhibition of T cell proliferation in vitro.
Conflict of Interest Statement
None of the authors has a financial relation- ship with a commercial entity that has an interest in the subject of this manuscript.
References
1. Greening AP, Ind PW, Northfield M, Shaw G (1994) Added salmeterol versus higher-dose corticosteroid in asthma patients with symptoms on existing inhaled corticosteroid. Allen & Hanburys Limited UK Study Group. Lancet 344: 219-224
2. Woolcock A, Lundback B, Ringdal N, Jacques LA (1996) Comparison of addition of salmeterol to in-
26
haled steroids with doubling of the dose of inhaled steroids. Am J Respir Crit Care Med 153 : 1481-1488 3. Pauwels RA, Lofdahl CG, Postma DS, Tattersfield
AE, O'Byrne P, Barnes PJ, Ullman A (1997) Effect of inhaled formoterol and budesonide on exacerbations of asthma. Formoterol and Corticosteroids Establishing Therapy (FACET) International Study Group. N Engl J Med 337: 1405-1411
4. Shrewsbury S, Pyke S, Britton M (2000) Meta-analy- sis of increased dose of inhaled steroid or addition of salmeterol in symptomatic asthma (MIASMA). BMJ 320: 1368-1373
5. O'Byrne PM, Bisgaard H, Godard PP, Pistolesi M, Palmqvist M, Zhu Y, Ekstrom T, Bateman ED (2005) Budesonide/formoterol combination therapy as both maintenance and reliever medication in asthma. Am J Respir Crit Care Med 171 : 129-136
6. Ducharme FM, Ni Chroinin M, Greenstone I, Las- serson TJ (2010) Addition of long-acting beta2- agonists to inhaled corticosteroids versus same dose inhaled corticosteroids for chronic asthma in adults and children. Cochrane Database Syst Rev (5) : CD005535
7. Papi A, Paggiaro PL, Nicolini G, Vignola AM, Fabbri LM (2007) Beclomethasone/formoterol versus budesonide/formoterol combination therapy in asthma. Eur Respir J 29 : 682-689
8. Bousquet J, Boulet LP, Peters MJ, Magnussen H, Quiralte J, Martinez-Aguilar NE, Carlsheimer A (2007) Budesonide/formoterol for maintenance and relief in uncontrolled asthma vs. highdose salmeterol/
fluticasone. Respir Med 101 : 2437-2446
9. Huchon G, Magnussen H, Chuchalin A, Dymek L, Gonod FB, Bousquet J (2009) Lung function and asthma control with beclomethasone and formoterol in a single inhaler. Respir Med 103 : 41-49
10. Nelson HS, Chapman KR, Pyke SD, Johnson M, Pritchard JN (2003) Enhanced synergy between fluticasone propionate and salmeterol inhaled from a single inhaler versus separate inhalers. J Allergy Clin Immunol 112: 29-36
11. Akabane H, Murata M, Kubota M, Takashima E, Tanaka H, Inagaki N, Horiba M, Nagai H (2006) Effects of salmeterol xinafoate and fluticasone propionate on immunological activation of human cultured mast cells. Allergol Int 55 : 387-393 12. Pang L, Knox AJ (2000) Synergistic inhibition by
beta(2)-agonists and corticosteroids on tumor necrosis factor-alpha-induced interleukin-8 release from cul- tured human airway smooth-muscle cells. Am J Respir
Cell Mol Biol 23 : 79-85
13. Peek EJ, Richards DF, Faith A, Lavender P, Lee TH, Corrigan CJ, Hawrylowicz CM (2005) Interleu- kin-10-secreting "regulatory" T cells induced by
glucocorticoids and beta2-agonists. Am J Respir Cell Mol Biol 33: 105-111
14. Aziz I, Hall IP, McFarlane LC, Lipworth BJ (1998) Beta2-adrenoceptor regulation and bronchodilator sen- sitivity after regular treatment with formoterol in sub- jects with stable asthma. J Allergy Clin Immunol 101 : 337-341
15. Pace E, Gagliardo R, Melis M, La Grutta S, Ferraro M, Siena L, Bonsignore G, Gjomarkaj M, Bousquet J, Vignola AM (2004) Synergistic effects of fluticasone propionate and salmeterol on in vitro T-cell activation and apoptosis in asthma. J Allergy Clin Immunol 114 :
1216-1223
16. Goleva E, Dunlap A, Leung DY (2004) Differential control of TH1 versus TH2 cell responses by the combi- nation of low-dose steroids with beta2-adrenergic agonists. J Allergy Clin Immunol 114: 183-191 17. Angulo R, Fulcher DA (1998) Measurement of
Candida-specific blastogenesis : comparison of carbox- yfluorescein succinimidyl ester labelling of T cells, thymidine incorporation, and CD69 expression.
Cytometry 34 : 143-151
18. Hasbold J, Lyons AB, Kehry MR, Hodgkin PD (1998) Cell division number regulates IgG1 and IgE switching of B cells following CD4OL and IL-4 stimula- tion. Eur J Immunol 28 : 1040-1051
19. Eliasson 0, Degraff ACJr (1985) The use of criteria for reversibility and obstruction to define patient groups for bronchodilator trials. Influence of clinical diagnosis, spirometric, and anthropometric variables.
Am Rev Respir Dis 132 : 858-864
20. Quah BJ, Warren HS, Parish CR (2007) Monitoring lymphocyte proliferation in vitro and in vivo with the intracellular fluorescent dye carboxyfluorescein diacetate succinimidyl ester. Nat Protoc 2 : 2049-2056 21. Giembycz MA, Newton R (2006) Beyond the dogma : novel { beta}2-adrenoceptor signalling in the airways. Eur Respir J 27 : 1286-1306
22. Usmani OS, Ito K, Maneechotesuwan K, Ito M, Johnson M, Barnes PJ, Adcock IM (2005) Glucocor- ticoid receptor nuclear translocation in airway cells after inhaled combination therapy. Am J Respir Crit Care Med 172: 704-712
23. Roth M, Johnson PR, Rudiger JJ, King GG, Ge Q, Burgess JK, Anderson G, Tamm M, Black JL (2002) Interaction between glucocorticoids and beta2 agonists on bronchial airway smooth muscle cells through synchronised cellular signalling. Lancet 360: 1293-
1299
24. Kaur M, Chivers JE, Giembycz MA, Newton R (2008) Long-acting beta2-adrenoceptor agonists syner- gistically enhance glucocorticoid-dependent transcrip- tion in human airway epithelial and smooth muscle cells. Mol Pharmacol 73 : 203-214
27