トップページ - 横浜国立大学学術情報リポジトリ
20
0
0
全文
(2) 48. (328). Yokohama Journal of Social Sciences, Vol. 19, No. 4・5. symptoms of distress in almost everyoneʼ and was ʻoutside the range of normal human experienceʼ. In addition four symptoms had to be present reflecting re-experiencing of the traumatic event, numbing and detachment, and a more pervasive change in arousal or emotions. The definition was defined in the Diagnostic and Statistical manual of Mental Disorders: DSM-III-R published in 1987, which introduced more symptoms and required at least one re-experiencing symptom (e.g., intrusive memories or nightmares), three avoidance or numbing symptoms (e.g., avoidance of reminders of the traumatic events or loss of interest in activities), and two hyper-arousal symptoms (e.g., exaggerated startle or irritability). Diagnostic and Statistical manual of Mental Disorders: DSM-IV, introduced in 1994, retained a similar structure. This study was based on DSM-IVʼs symptoms. Posttraumatic stress disorder (PTSD) is a chronic and disabling disorder, characterized by specific symptoms that develop after exposure to trauma to which an individual responds with intense fear, helplessness, or horror (DSM-IV). On the basis of the diagnostic criteria of the DSM-IV, PTSD is an anxiety disorder that follows a traumatic event (Criterion A). It is characterized by recurrent re-experiencing of the traumatic event (Criterion B), constant avoidance of trauma-related stimuli and emotional numbing (Criterion C), and persistent symptoms of hyper-arousal (Criterion D). In addition, symptoms must be prevalent for at least 1 month (Criterion E) and lead to impaired functioning in at least one important life domain (Criterion F).The core symptoms of PTSD are re-experiencing the event (B), stimuli avoidance (C), and persistent symptoms of increasing arousal (D). In order to be diagnosed with PTSD according to DSM-IV, a person needs to meet Criteria A, required at least one re-experiencing symptom (B), three avoidance or numbing symptoms (C), and two hyper-arousal symptoms (D) and Criterion E and F. The fifth revision (DSM-V) was released in May 2013.This revision includes changes to the diagnosis criteria for PTSD. The three core clusters (Criterion B, C and D) of DSM-IV symptoms 17-items are divided into four clusters (Criterion B, C, D and E) in DSM-V symptoms 20-items; (1) intrusion-B, (2) avoidance-C, (3) negative alterations in cognitions and moods-D and (4) alterations in arousal and reactivity-E. In DSM-V, the avoidance symptoms of PTSD will be separated from negative changes in thoughts and mood (such as emotional numbing). In order to be diagnosed with PTSD according to DSM-V, a person needs to meet Criterion A, at least one symptom from Criterion B, at least one symptom from Criterion C, at least two symptoms from Criterion D, at least two symptoms from Criterion E, and Criterion F through H. Our survey was conducted before DSM-V was released, therefore all criteria were based on DSM-IV. Over the past 20 years, there has been growing interest in developing tools for the assessment of posttraumatic stress symptoms. One of the most widely used self-report instruments for the assessment of PTSD symptoms is the Impact of Event Scale (IES) and its revised version, the Impact of Event Scale-Revised (IES-R). In 1979, Horowitz, Wilner, & Alvarez developed the IES, a 15-item self-report measure used to assess the frequency of 2 symptoms (7 intrusion items and 8 avoidance items) associated with the experience of a traumatic event. The original IES did not contain symptoms of arousal. In 1997, Weiss and Marmar added 7 items for hyper-arousal symptoms, a revised version of the IES. Thus, it consists of 22 items. The original IES evaluates the frequency of symptoms within the previous week on a 4-point scale (0, 1, 3 and 5), whereas the IES-R evaluates the severity of symptoms experienced during the previous week on a 5-point scale ranging from 0 (not at all) to 4 (extremely). The IES-R yields totals scores that range from 0 to 88. The sum of all individual scores was taken to indicate the severity of the psychological reactions to the previous stress. The IES-R has been of sufficient interest to scholars worldwide to have been translated into many.
(3) Validation of a Myanmar Version of the Impact of Event Scale-Revised in Survivors after Disaster(Khin Myo Htut, San San Oo, Zaw Sein Lwin) (329). 49. languages. Published translations exist in Japanese (Asukari et al., 2002), Chinese versions (Wu & Chan, 2004), French (Brunet, St. Hilaire, Jehel, & King, 2003), Greek (Mystakidou & Galanos, 2007), Korean (Lim et al., 2009), Swedish (Sveen, Low & Dyster-Aas et al., 2010), Taiwanese (Chen et al., 2011), Italian (Craparo, Faraci & Rotondo et al., 2013) and Malay (Norhayati & Aniza, 2014). These translated IES-R have been shown to have good psychometric properties and have been used following several traumatic events including lifetime mixed traumatic events, an arsenic poisoning case, earthquakes, metro sarin attack, motor vehicle accidents, natural disaster, during or preceding pregnancy, cancer patients, burned patients, floods, typhoon and post caesarian patients. Structured diagnostic interviews play an increasingly role in contemporary mental health research and practice. A number of structured interviews are now available for diagnosing PTSD. These include stand-alone interviews such as Structured Interview for PTSD (SI-PTSD; Davidson, Kudler, & Smith 1990; Davidson, Smith, & Kudler, 1989), the PTSD Interview (PTSD-I; Watson, Juba, Manifold, Kucala, & Anderson, 1991), the Clinician-Administered PTSD Scale (Blake et al., 1990) ) and the PTSD Symptom Scale-Interview (PSS-I; Foa, Riggs. Dancu, & Rothbaum, 1993). The CAPS-1 is the gold standard in PTSD assessment of our survey and consists of 30 items. The CAPS is composed of CAPS-1 or CAPS-DX (i.e., CAPS- Diagnostic version) and CAPS-2 or CAPS-SX (i.e., CAPS-Symptom Status version), which were designed to assess the current or lifetime PTSD status and PTSD symptoms experienced during the previous week, respectively. We chose the past week time frame and used CAPS-1 or CAPS-DX to measure frequency over a week while we were interviewing rather than frequency of severity over a week. We were using total IES-R-M score and total CAPS-1 (17 items) score of total severity to get a cut-off point. A cut-off point is used to distinguish normal from abnormal tests results. The objectives of this study were (1) to get a validation of a Myanmar version of the Impact of Event Scale-Revised in survivors after disaster, (2) to get a clear cut-off point of PTSD (Post Traumatic Stress Disorder) by using IES-R-M and (3) to find prevalence and risk factors of PTSD for survivors who had experienced Cyclone, Nargis in Myanmar in 2008. 2.Methodology 2. 1 Survey Period This survey was performed from February 25, 2013 to March 25, 2013, 4 years and 9 months after Cyclone, Nargis in Myanmar. 2. 2 Survey Methods This study was a cross-sectional study. After getting permission from MRCS (Myanmar Red Cross Society), our group (2 Psychiatrists and I) joined with 4 members of Bogalay townshipʼs center of MRCS. One Psychiatrist and I carried out face to face interviews with survivors at the same time. The questionnaire has 3 parts as demographic data, IES-R-M and CAPS-1.We marked parallel for IES-R-M score to get interrater reliability of the scale. The rest of the questionnairesʼ parts were asked separately. It took approximately 45 minutes per person. Thus, we got a completed answer one set and extra one set of IES-R-M score for each participant. A total of 112 people in Bogale Township over the age of 20 were recruited into this study. All were direct victims of Cyclone Nargis. We excluded those diagnosed as psychotic and more than one person.
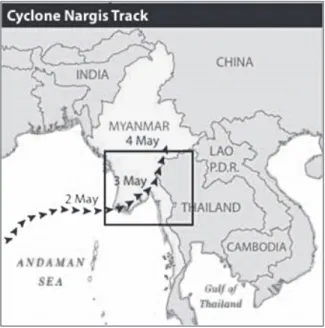
(4) 50. (330). Yokohama Journal of Social Sciences, Vol. 19, No. 4・5. from the same family. Participants are recruited randomly at Myanmar Red Cross Societyʼs sub-units by MRCS staff and local community leaders. In accordance with the ethical rules of MRCS, we did not mention names of participants. The investigator was strictly maintained the rules of confidentiality about the data and information obtained from the interviews as well as confidential medical records. We got completed answers from 100 participants out of 112: a survey response rate of 89.30%. 2. 3 Study Sites and Sample Myanmar is the largest country in main-land South-East Asia. The Cyclone Nargis, which struck Myanmar on May 2nd, 2008 left an estimated death toll of 84,537 and 53,836 people missing (Swiss Re(2009), 2-Sigma). There were 5 villages (1) Kyein Chaung Gyi (2) Bingalar (3) Western La Wine (4) Kan Kone and (5) Lake Gabar in Bogale Township, which was the most affected area, Bogale Township, Irrawady Division, Myanmar (see Figure 2). Cyclone Nargis struck Myanmar, making landfall in the Irrawaddy Division and Yangon Division. Thirty seven townships were significantly affected by the cyclone. Overall, an estimated 3.2 million people were affected by Cyclone-Nargis (www.jhsph.edu/research/centers-and-institutes). 2. 4 Instruments 2. 4. 1 Myanmar version of the Impact of event Scale-Revised (IES-R-M) After obtaining permission from the original author, Professor Daniel S. Weiss, of the translated version, we established the final IES-R-M on June 12, 2012. The comparability of IES-R-M and the original IES-R has been validated by stringent back-translation procedures. The IES-R was translated first in Myanmar by Dr. Zaw Sein Lwin, Senior Consultant/Psychiatrist. Then, the Myanmar IES-R was back translated by Daw Soe Moe Thu, Professor and Head of English Department, University of Medicine, Magway, Myanmar. The content of the final IES-R-M was further verified by back-translation procedure until the meaning of each item matched with the original item of IES-R. The process of translation has been carefully planned with the importance of ensuring the preservations of the meanings and followed by the content validity (content validity refers to adequacy of the content of an instrument in terms of the number and scope of the individual questions that it contains) and face validity (face validity refers to checking whether items in an instrument appear on the face of it to cover the intended topics clearly and unambiguously). Respondent testing was done among ten victims of Cyclone, Nargis in Yangon. They were required to review and comment on the whole questionnaire in terms of its presentation, arrangement, clarity and relatedness. The IES-R-M is composed of 22 items that measure symptoms of intrusion (dreams about the event), avoidance and numbing (effort to avoid reminders of the events), and hyper-arousal (feeling watchful and on guard). All items of IES-R-M were in Myanmar. Each item consists of a 5-point Likert scale from ʻnot at allʼ (0), ʻa little bitʼ (1), 'moderatelyʼ (2), ʻquite a bitʼ (3) to ʻextremelyʼ (4).The maximum score is 88, which would show the worst PTSD symptom state. Question numbers of 1, 2, 3, 6, 9, 14, 16 & 20 were regarding of Intrusion symptoms. Question numbers of 5, 7, 8, 11, 12, 13, 17 & 22 pertained to Avoidance symptoms and question numbers of 4, 10, 15, 18, 19 & 21 deal with Hyper-arousal (Weiss, D. S., Marmar, C. R., 1997). 2. 4. 2 Clinician-Administered PTSD Scale, version-1 (CAPS-1) CAPS is a widely used structured interview for assessing PTSD. According to a review of 10 years of research, CAPS has excellent reliability, giving consistent scores across items, raters, and testing occasions. It.
(5) Validation of a Myanmar Version of the Impact of Event Scale-Revised in Survivors after Disaster(Khin Myo Htut, San San Oo, Zaw Sein Lwin) (331). www.coolgeography.co.uk. Figure 1 Map of Myanmar.. www.jhsph.edu/research/centers-and-institutes. Figure 2 Cyclone Nargis affected areas in Myanmar. 51.
(6) 52. (332). Yokohama Journal of Social Sciences, Vol. 19, No. 4・5. has good convergent and discriminate validity and sensitivity to clinical change. In the present study, CAPS1 (Blake et al., 1990) which is a revised version of CAPS following the publication of DSM-III-R, was used. We choose CAPS-1 for this survey because it gives both continuous and dichotomous scores for current and lifetime PTSD symptoms. And then by using CAPS-1, we can measure frequency in the previous week. CAPS-1 consists of standardized prompt questions, supplementary follow up questions, and behaviorally anchored 5-point rating scales corresponding to the frequency and intensity of each symptoms assessment. It has 30 items. Eight items assessing associated features of guilt, hopelessness and memory impairment. Five items assessing response validity, global severity, global improvement and social-occupational impairment. For each of the 17 symptoms of PTSD in criteria B, C and D, CAPS-1 assesses both frequency of occurrence and the severity of symptoms at their worst during the previous month on a 5-point scale. We were not using the score 8 items assessing associated features of guilt, hopelessness, memory impairment and 5 items of associated features response validity, global severity, global improvement and social-occupational impairment left as a record. In 17 symptoms of PTSD, for frequency of occurrence, each item is rated from never (0), Once or twice (1), once or twice a week (2), several times a week (3) to nightly or almost every night (4) as well as for symptom intensity, each item is rated from none (0), mild, minimal distress did not awaken (1), moderate, awoke in distress but readily returned to sleep (2), severe, considerable distress, difficulty returning to sleep (3) to extreme, overwhelming or incapacitating distress, could not return to sleep (4). Thus, each item can have a score 0 to 8. Specific scores for criteria B, C and D can be found by adding the item scores belonging to the specific criteria together CAPS-1 (Clinician Administered PTSD Scale – Version1). We also choose the previous week time frame and we used CAPS-1 or CAPS-DX to measure how many times in a week. There are (9) rules of CAPS to determine PTSD and Non-PTSD which are: ◦Rationally derived rules 1. Frequency ≥ 1 or Intensity ≥ 2 2. Item Severity ≥ 4 3. Clinician – Rated 60 4. Clinician – Rated 75 ◦Empirically derived rules 1. SCID Diagnosis – Calibrated 2. SCID Symptom – Calibrated 3. Total severity ≥ 45 4. Total severity ≥ 65 (by Weathers et al., 1998) 5. Frequency ≥ 1 or Intensity ≥ 2 or Total severity ≥ 65 For this study, an empirically derived rule total severity (frequency+ intensity) ≥ 65 (by Weathers et al., 1998) for making a diagnosis of PTSD was adopted. 2. 5 Statistical Analysis Data analysis was performed using the SPSS version 20 for Windows. Descriptive statistics, including means, counts and percentages for the variables were calculated. Demographic data were compared in correlation and Chi squared tests to determine the impact of the theoretically possible independent variables in predicting PTSD. Fisherʼs exact test was used when the expected count of one or more cells was less than five..
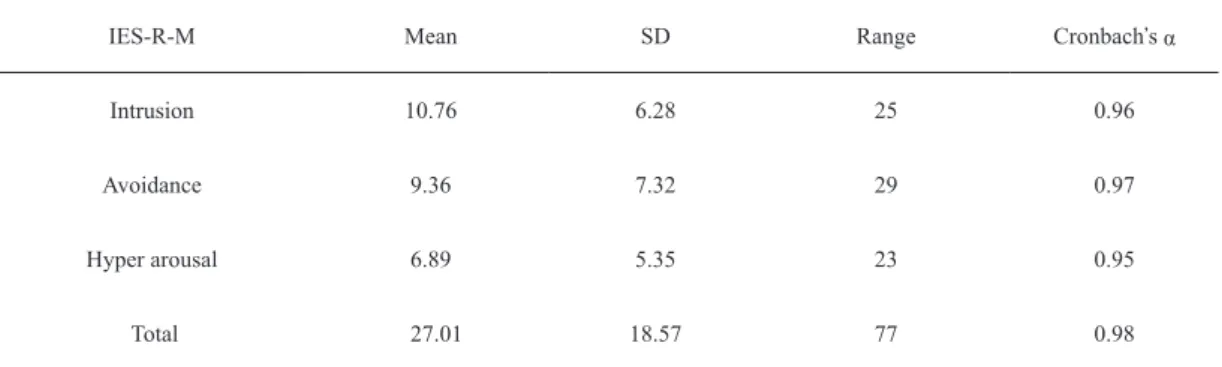
(7) Validation of a Myanmar Version of the Impact of Event Scale-Revised in Survivors after Disaster(Khin Myo Htut, San San Oo, Zaw Sein Lwin) (333). 53. The discriminative values Sensitivity, Specificity, Positive Predictive Accuracy, Negative Predictive Accuracy and Overall Accuracy were calculated according to the standard formulae. We calculated kappa coefficients that reflects the accuracy of the test. We analyzed a receiver operating characteristic (ROC) curve and Youden Index (J) to obtain the optimal cut-off score for detecting PTSD in all subjects. To assess the reliability of the questionnaire, internal consistency (Cronbachʼs alpha coefficients) and inter-raters were calculated for IESR-M. Significance level was interpreted at the p < .05 level for this study. 2. 6 Variables and demographic data characteristics In this survey, altogether 14 demographic questions including personal background, stress of job and recovery status to find out the prevalence of PTSD. The survey participants were composed of 47 male and 53 female. The completed age of respondent were collected and later categorized into 2 categories for analysis (from 20 to 60) as under 60 and (61 & above) as over 60. The average of age was 44.47 and SD was 14.21. Regarding the occupations of the participants, 37% were vendors, Government servants 0% (current Government staff were not victims of Nargis), 13% were sea-workers, 26 % were farmers, 17% were others and 7% were jobless. The current occupation of the respondent was collected by 6 categories. After initial analysis, the study of this data was too scattered to do further analysis. The data was re-grouped into 2 categories: having a job 76% (including vendors, Government servants, sea-workers and farmers) and jobless 24% (including others and jobless). Marital status of participants was 69% were married, 31% were others. Educationalstatus of participants was: 9% had never attended school, 72 % had only attended primary school, 16% had middle school level education, 2% were high school level and only 1% were University graduates. Similarly, educational status was later categorized into 2 categories as lower 81% (never, primary and middle) and Higher educational status 19% (high school and university graduate). As regards satisfaction of current job conditions 60% reported satisfaction and 40% were unsatisfied. Individual income amount of ≤ 50000 kyats were 91% and more than 50000 kyats were only 9%. Additionally, 97% were living with family and only 3% were not living with family. Sixteen percent of survivors were having trauma experiences before the disaster but 84% had never experienced trauma in their lives. While 94% reported severe damaged to their house, 6% did not have severe damage. Sixty percent of survivors were worried about the rebuilding of their houses and 40% were not worried about this. Only 3% of survivors were having worries about their relationship with their community, 97% were not having worries about their relationship. While 79% were receiving social support, 21% were not. All factors were taken into consideration using binary analysis. 2. 7 Response of mental health (PTSD) conditions 2. 7. 1 Reliability and Internal consistency The means and standard deviations of the IES-R subscale scores for the study group were examined. The internal consistency of IES-R was estimated using coefficient α for the intrusion (Cronbchʼs α = 0.96), avoidance (Cronbchʼs α = 0.97) and hyper-arousal (Cronbchʼs α = 0.95) while overall alpha was 0.98 (Table 2). The correlated item-total correlations for the 3 subscales produced the following ranges of coefficients, intrusion (r = 0.66 to 0.90), avoidance (r = 0.65 to 0.90) and hyper-arousal (r = 0.67 to 0.83). This data suggested that each of the individual items was consistent with the remaining items. The mean of total IES-R scores was 27.01 and (SD =18.5) with the range of 3 to 80..
(8) 54. Yokohama Journal of Social Sciences, Vol. 19, No. 4・5. (334). Table 1 Percentages and frequencies of demographic risk factors Sample (N = 100 ) %. N. 1. Gender Male Female. 47 53. 47 53. 2. Age Under 60 (20~60) Over 60 (61 and over). 87 13. 87 13. 3. Marital Status Married Others. 69 31. 69 31. 4. Educational Status Lower Higher. 81 19. 81 19. 5. Occupational Status Job Jobless. 76 24. 76 24. 6. Satisfaction of Current Job Conditions Good Bad. 60 40. 60 40. 7. Income (Individual) amount per Month in Kyats ≤ 50000 > 50000. 91 9. 91 9. 8. living with Family Yes No. 97 3. 97 3. 9. Having Loss Family in Disaster Yes No. 73 27. 73 27. 10. Having Trauma Experience before Disaster Yes No. 16 84. 16 84. 11. Having Severe Damaged of House Yes No. 94 6. 94 6. 12. Having Worried about Rebuild of House Yes No. 60 40. 60 40. 13. Having Worried about Relationship with Community Yes No. 3 97. 3 97. 14. Having Any Social Support Yes No. 79 21. 79 21.
(9) Validation of a Myanmar Version of the Impact of Event Scale-Revised in Survivors after Disaster(Khin Myo Htut, San San Oo, Zaw Sein Lwin) (335). 55. Table 2 Means, standard deviation and Cronbach s α of IES-R subscale scores IES-R-M. Mean. SD. Range. Cronbachʼs α. Intrusion. 10.76. 6.28. 25. 0.96. Avoidance. 9.36. 7.32. 29. 0.97. Hyper arousal. 6.89. 5.35. 23. 0.95. Total. 27.01. 18.57. 77. 0.98. Table 3 7 possible cut-off scores in distinguishing with and without PTSD assessed with CAPS-1. Data represents percentages Cut-off Point of IES-R. Sensitivity. Specificity. Positive Predictive Accuracy. Negative Predictive Accuracy. Overall Accuracy. Kappa. Optimal Cut-off point J. 30. 1. .78. .56. 1. .83. .61. .78. 31. .90. .87. .66. .97. .88. .69. .77. 32. .90. .93. .80. .97. .93. .80. .83. 33. .86. .98. .95. .96. .96. .88. .84. 34. .81. .98. .94. .95. .95. .84. .79. 35. .81. .98. .94. .95. .95. .84. .79. 36. .77. 1. 1. .93. .95. .84. .77. 2. 7. 2 Validity The interdependence of the three subscales was demonstrated when their relationship was examined by Pearsonʼs correlations. The subscale correlations were 0.93 for intrusion with avoidance, 0.93 for intrusion with hyper-arousal and 0.94 for avoidance with hyper-arousal (P<0.001). Pearsonʼs correlation between total IES-R-M and CAPS (17 items) was significant with r = 0.93, p <0.001. 2. 7. 3 Discriminative Ability 2. 7. 3 (a) Sensitivity, Specificity, PPV, NPV, OA and Kappa The value of 7 possible Kappa (Cohenʼs Kappa) were 0.61, 0.69, 0.80, 0.88, 0.84, 0.84 and 0.84 respectively by results of SPSS outputs. In accordance with the theory of Cohen Kappa, a value of 1 implies perfect agreement. The number of Kappa nearest 1 is the best result to determine the cut-off point,. So, Kappa = 0.88, cut-off point f 33 is the best result for our study (See Table 3)..
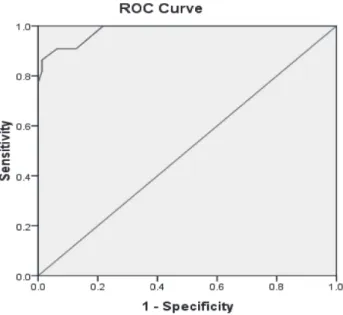
(10) 56. Yokohama Journal of Social Sciences, Vol. 19, No. 4・5. (336). Figure 3 The relative operating characteristics curve of the revised version of the IES-R-M at different cut-off points. 2. 7. 3 (b) Receiver Operative Characteristics Curve (ROC) To determine the criteria validity of the IES-R for PTSD we examined using ROC (Receiver Operative Characteristic) analysis. The area under this curve (AUC) is an overall index of the accuracy of the discrimination provided by IES-R-M. An AUC of 0.5 implies random performance, whereas an AUC of 1.0 represents perfect performance. Generally, an AUC above 0.85 is considered to be an indication of good diagnostic capability. The area under the ROC curve of IES-R-M was 0.98 (95% confidence interval = 0.95 to 1.00) with standard deviation 0.01 (Figure 3). 2. 7. 3 (c) Youden Index We calculated to get a clear cut-off point based on ROC analysis, by using the theory of Youden Index (Youden1950; Faraggi, 2000; Reiser, 2000; Miller 1981, Searle, 1971). Optimal cut-off point J = Maxt [Sensitivity + (Specificity – 1)] The results were 0.78, 0.77, 0.83, 0.84, 0.79, 0.79 and 0.77 of 7 possible cut-offs respectively. Among them we choose the biggest point of J, which was 0.84, optimal cut-off 33 where sensitivity was 0.86, specificity was 0.98, positive predictive accuracy was 0.95,negative predictive accuracy was 0.96 and overall accuracy was also 0.96. The kappa was 0.88 In accordance with the result of cut-off point of IES-R-M was 33,(20%) 20 people (15% male and 25% female) suffered from PTSD out of 100 participants (Figure 4 and 5)..
(11) Validation of a Myanmar Version of the Impact of Event Scale-Revised in Survivors after Disaster(Khin Myo Htut, San San Oo, Zaw Sein Lwin) (337). Figure 4 Gender distribution of PTSD group.. Figure 5 Score distribution on IES-R-M. 57.
(12) 58. (338). Yokohama Journal of Social Sciences, Vol. 19, No. 4・5. 3.Results of demographic risk factors 2 A X test was performed in order to study the characteristic factors that differentiate the PTSD group. from non-PTSD group. In this study, PTSD or Non-PTSD with a cut-off point of 33 or above on the IESR-M, is the dependent variable and the following (14) risk factors were; (1) gender, (2) age, (3) marital status, (4) educational status, (5) occupational status, (6) satisfaction of current job condition, (7) individual income amount per month in kyats, (8) living with family, (9) family loss, (10) having trauma experience before disaster, (11) severe damaged to house, (12) worry about rebuilding of house, (13) worry about relationship with community, and (14) having social support tested as independent variables. Lower education was significant (X2 = 7.16, df = 1, p < 0.05) as was satisfaction of current job condition (X2 = 9.38, df = 1, p < 0.01). Having family loss (X2 = 9.25, df = 1, P< 0.01) and worry about rebuilding of shelter/house (X2 = 4.17, df = 1, P < 0.05) were also significant with regards to having PTSD or not (See Table 4). 4.Discussions This is the first study that reports on the cut-off point and psychometric properties of the Myanmar version of IES-R among victims of disaster reported on convergent validity and reliability of IES-R using discriminative ability ROC curve analysis, interdependence of subscales correlations and internal consistency of subscales and total score. In this study, we found that the IES-R-M as an instrument for evaluation of mental disorder associated with exposure to natural disaster. Pearsonʼs correlations of subscales score are high and give good validity ranging from 0.93 to 0.94.The high Cronbachʼs alpha values for all subscales as well as the total scale indicate very good internal consistency ranging from 0.95 to 0.98 to compare with the findings of the original English version (Weiss and Marmar,1997) and Greek version (Mystakidou & Galanos, 2007). Although test-retest data were not available, inter-raters reliability of IES-R was r = 0.97, p < 0.001.The correlation between the IESR-M and CAPS-1 (gold standard) of 17 items (r = 0.93, P <0.001) was also high. The optimal cut-off point for IES-R-M in this study, when detecting PTSD, was determined to be 33, which give both good sensitivity 0.86 and specificity 0.98 with positive predictive accuracy 0.95, negative predictive accuracy 0.96, overall accuracy 0.96 and kappa 0.88 and optimal cut-off score of J was 0.84 (See Table 3). The cut-off score of the IES-R Korea version (Lim et al., 2009) was 22, with 0.95 in sensitivity and 0.80 in specificity while the Japanese version (Asukari et al., 2002) of IES-R, which has a reported cut-off score of 24/25 with sensitivity of 1.0 and specificity of 0.67 resulted in a lower score cut-off point than that of our study. Both of these studiesʼ gold standard of IES-R questionnaire was CAPS, which was the same as with our study, but the cut-off points are quite different. Possible reasons for this are, different sample sizes, different timing and different cultures. The area under the ROC curve of IES-R–M was 0.98 (95% CI, 0.95 to 1) with SD 0.01which was higher than that of IES-R-J, 0.85. Based on this cut-off point of 33, this research found 20% of participant survivors after Cyclone, Nargis to have a high risk of PTSD (see Figure 4). The frequency of participants with PTSD in this study was thus greater than that of a prior study (DSM-IV 1994), which found the lifelong prevalence of PTSD to be 1 to 14%. Studies that have documented the prevalence of PTSD in the general population after disaster have uniformly documented a lower prevalence of PTSD among direct victims and rescue workers (Havenaar JM,.
(13) Validation of a Myanmar Version of the Impact of Event Scale-Revised in Survivors after Disaster(Khin Myo Htut, San San Oo, Zaw Sein Lwin) (339). Table 4 Results of demographic risk factors data %. X2. df. P. Male Female. 47 53. 1.45. 1. 0.23 (ns). ≤ 60 > 60. 87 13. 0.20. 1. 1.00 (ns) Fisherʼs Exact Test. 3. Marital Status. Married Others. 69 31. 0.19. 1. 0.67 (ns). 4.Educational Status. Lower Higher. 81 19. 7.16. 1. 0.02* Fisherʼs Exact Test. 5. Occupational Status. Job Jobless. 76 24. 3.51. 1. 0.08 (ns) Fisherʼs Exact Test. Good Bad. 60 40. 9.38. 1. 0.002**. ≤ 50000k > 50000k. 91 9. 2.47. 1. 0.20 (ns) Fisherʼs Exact Test. 8. Living with Family. Yes No. 97 3. 0.34. 1. 0.49 (ns) Fisherʼs Exact Test. 9. Loss Family. Yes No. 73 27. 9.25. 1. 0.002**. 10. Trauma Experience. Yes No. 16 84. 0.02. 1. 1.0 (ns) Fisherʼs Exact Test. 11. Severely Damaged of House. Yes No. 94 6. 1.60. 1. 0.60 (ns) Fisherʼs Exact Test. 12. Rebuild of House. Yes No. 60 40. 4.17. 1. 0.04*. 13. Relationship with Community. Yes No. 3 97. 1. 0.49 (ns) Fisherʼs Exact Test. 14. Having Social Support. Yes No. 79 21. 1. 0.55 (ns). Item 1. Gender. 2. Age. 6. Satisfaction of Current Job Condition 7. Income Amount per Month. *P<.05, **P<.01. 0.34. 0.54. 59.
(14) 60. (340). Yokohama Journal of Social Sciences, Vol. 19, No. 4・5. Rumyantzeva GM & et al., 1997). Generally, studies of natural disasters report PTSD prevalence ranging from 3.7% (Canino et al., 1990) to 60% (Madakasira & OʼBrien, 1987) in the first 1‒2 years after the disaster, with most studies reporting prevalence estimates in the lower half of this range (Norris et al., 2004; Liu et al., 2006., Parslow et al., 2006). However, higher prevalence estimates of PTSD have been reported in specific groups such as clinical samples (Livanou et al., 2002; Soldatos et al., 2006) and populations in areas heavily affected by the disaster (Najarian et al., 2001; Finnsdottir & Elklit, 2002). For example 50% reported PTSD two years after 1988 Armenian earthquake (Armenian et al., 2000). Some longitudinal research of natural disasters documented a decline in PTSD prevalence over time (Carr et al., 1997a,b; Van Griensven et al., 2006); however some studies also showed an increase in PTSD prevalence over time. Research into residents in Florida exposed to Hurricane Andrew in 1992 found that the prevalence of PTSD increased from 26% to 29% between 6 and 30 months after the disaster. Similarly, an increase in prevalence of PTSD was observed between 3 and 9 months after the 1998 Zhangbei-Shangyi earthquake in China (Wang et al., 2000). Our findings show that the prevalence of PTSD was 20% over 4 years after the disaster can be seen as reasonable being that the most study took place in the most disaster affected areas and all participants were direct victims. Additionally, this was a cross sectional survey, rather than a comparison survey. In this survey altogether 14 demographic questions to find the prevalence of PTSD and Non-PTSD. Lower education was significant with PTSD (X2 = 7.16, df = 1, p <.05) and similar to a survey of traumatic stress response in earthquake survivors in turkey (Mertin Basoglu et al., 2002 and Armenian et al., 2000). Epidemiology studies have found higher rates of PTSD among women than men (Breslau et al., 1991; Kessler et al.,1995). Olff ʼs review of the literature on PTSD (2007) stated that women consistently have a higher risk of PTSD than men. Female gender as a predictor of PTSD symptoms is consistent with findings from some studies (Carr et al., 1995, 1997b, Durkin, 1993; Kananci et al., 1995). However, female gender was not always found to be a vulnerability factor in studies of other natural disaster survivors (Madakasira & Oʼbrien, 1987; Phifer, 1990). Our study also found that women reported a higher rate than men (25% Vs 15%) but the risk ratio for PTSD was not significant by gender. This may be due to the fact that all 7 men, out of 47 (20% of men), were direct victims and lost their nuclear family or parents in this Cyclone. Also, our sample size was small. Thus, the association between PTSD and Non-PTSD by gender was not significant (X2 = 1.45, df = 1, P = 0.23). Although PTSD can appear at any age, our study revealed that associated risk factor of age was not significant (X2 = 0.20, df = 1, P = 1.00) while other studies have found that older survivers (≥ 65 years old) have a higher risk of mental disorders than those of younger ones (< 65 years old) in Recurring Natural Disasters and PTSD. For example in a study of survivors of the eruption on Miyake Island by Fujimori Tatsuo and Omori Tetsushi (2012) found this to be the case. Also, senior middle school students had a higher risk than junior middle school students among Wenchuan earthquake survivors according to a study in 2008 by Zhou et al. 2 Other risk factors, such as marital status and having a job were also not significant in our study, (X = 0.19,. df = 1, P = 0.67 and X2 = 3.51, df = 1, P = 0.08) respectively. The impact of a disaster is felt more in developing countries due to the economic status, population density, and limited resources (Rubonis & Bickman, 1991). In our study only a few associated risk factors were significant for PTSD, including lower education, dissatisfaction with current job condition, family loss.
(15) Validation of a Myanmar Version of the Impact of Event Scale-Revised in Survivors after Disaster(Khin Myo Htut, San San Oo, Zaw Sein Lwin) (341). 61. and worry about rebuilding of houses. Other risk factors which were significant in other studies, such as a lack of, or lower social support were not found to be significant in our study. 2 Lack of satisfaction with current job status was significant with PTSD in our study (X = 9.38, df = 1, P. <.01), this matches a survey by Galea S. et al. (2005). Also loss of family was significant (X2 = 9.25, df = 1, P <.01) which can de seen in almost every disaster psychology study of PTSD including Metin Basoglu et al. (2002), Lai et al. (2004) and Armenian et al. (2000). In this study, the risk factor of having worried about rebuilding of house was also significant with PTSD/Non-PTSD (X2 = 4.17, df = 1, P <.05). While receiving social support after disaster was not significant in our study (X2 = 0.54, df = 1, P = 0.55), a study of Hanshin-Awaji earthquake victims (Kwon Y, Maruyama S. et al., 2001) and other studies (Galea S et al., 2005, Armenian et al., 2000, Bland et al., 1997, Metin Basoglu et al., 2004) showed that low or no social support was associated with a higher likelihood of PTSD. Some other associated risk factors of PTSD in our study which were also not significant were difficult to compare because of differences in sampling, assessment methods, time since the disaster, intensity of the disasters, and the scale of devastation. Several limitations have been encountered during the entire process of the study. Firstly, Myanmar version of IES-R was only administered on a single occasion in this study, so we were unable to examine other potentially important psychometric properties. The pre-disaster mental health situation of this area was not known. We were only able to obtain a follow up analysis between 2008 and 2013. 5.Conclusions Our data demonstrates that the IES-R-M was a reliable measure with good psychometric properties and can be used as a reliable, valid, and timesaving tool to assess PTSD. There are some strengths and limitations of IES-R-M like its original English version. The main strengths of this version are that is still short, easily administered and scored, correlates better with the DSM-IV, and can be used repeatedly to assess progress but it still is limited by remaining a screening tool rather than a comprehensive test. IES-R is not a diagnostic measure for PTSD because criteria A of the disorder are not assessed. Although the IES-R-M was not developed as a diagnostic tool, examination of its discriminative validity suggests that the measure can differentiate between individuals with and without PTSD. The data collected in the present study may serve as a baseline for comparison with clinical samples of future studies for Myanmar population. The findings of the present study will help other researchers to design prospective studies examining the long-term public health impact of disasters in these communities. This will help build a knowledge base of psychological consequences of disasters and to prepare for pre-disaster mental health planning. Acknowledgement. We would like to thank to Professor Fujimori Tatsuo, Dr. Thar Hla Shwe, President of MRCS, Dr. Hla Pe, Secretary of MRCS, Dr. Zaw Sein lwin, Senior Consultant/Psychiatrist, Dr. San San Oo, Junior Consultant/ Psychiatrist and Daw Soe Moe Thu, Head of English department, University of Medicine, Magway, Myanmar. This study was supported by Myanmar Red Cross Society (MRCS), permission letter No.483/sama-1/1 (2013). This study was also supported by grants from SLER (Sustainable Living with Environmental Risk) program,.
(16) 62. (342). Yokohama Journal of Social Sciences, Vol. 19, No. 4・5. Yokohama National University, Japan. References Acierno, R., K. J. Ruggiero, and D. G. Kilpatrick, (2006); Risk and Protective Factors for Psychopathology among Older versus Younger Adults after the 2004 Florida Hurricanes. American Journal of Geriatric Psychiatry 14, pp. 1051‒1059 Acierno, R., K. J. Ruggiero, S. Glea, H. S. Resnick, K. Koenen, J. Roitzsch, M. de Arellano, J. Boyle, and D. G. Kilpatrick (2007): Psychological Sequelae Resulting from the 2004 Florida Hurricanes: Implications for Post Disaster Intervention. American Journal of Public Health 97 (Suppl.1), pp. S 103‒S 108 Anthony N.Glser; High-Yield TM Biostatistics, pp. 78‒88. Asukai, N., Kato, H., Kawamura, N., Kim, Y., Yamamoto, K., Kishimoto, J., Miyake, Y., & Nishizono-Maher, A (2002). Reliability and validity of the Japanese-language version of the impact of event scale-revised (IES-R): four studies of different traumatic events. The Journal of Nervous and Mental Disease.190 (3), pp. 175‒82. American Psychiatric Association (1980). DSM-III Diagnostic and statistical manual of mental disorders.(3rd ed.) Washington. American Psychiatric Association (1987). DSM-III-R Diagnostic and statistical manual of mental disorders.(3rd ed.) Washington. American Psychiatric Association(1994). DSM-IV 309‒81 Posttraumatic Stress Disorder; Diagnostic and Statistical manual of Mental Disorders, (4th ed. ) American Psychiatric Association, Washington 424‒429, DCʼ Author. American Psychiatric Association(1994).DSM-IV-TR 309‒ 81 Posttraumatic Stress Disorder; Diagnostic and Statistical manual of Mental Disorders, (4th ed.-TR )American Psychiatric Association, Washington 424‒429, DCʼ Author. American Psychiatric Association (2013). DSM-V, Diagnostic and statistical manual of mental disorders. Washington DC. Armenian, H. K., M. Morikawa, A. K. Melkonian, A. P. Hovanesian, N. Haroutunian, P. A. Saigh, K. Akiskal, and H. Akiskal (2000): Loss as a Determinant of PTSD in a Cohort of Adult survivors of the 1988 Earthquake in Armenia: Implications for Policy, Acta Psychiatrica Scandinavica 102 pp. 58‒64. Blake D., Weathers F., Nagy L., Kaloupek D., Klauminzer G., Charney D., Keane T. (1990).Clinician –administered PTSD scale(CAPS) Boston, MA: National Center for Post-Traumatic Stress Disorder, Behavioral Science Division. Blake D., Weathers F., Nagy L., Kaloupek D., Klaumizer G., Charney D., and Keane T. (1995). The Development of a Clinician- Administered PTSD Scale; Journal of Traumatic Stress, Vol., 8, No. 1. Brunet A., St-Hilaire, A., jehel, L., & King, S. (2003): Validation of a French version of the Impact of Event ScaleRevised. Canadian Journal of Psychiatry, 48, pp. 56‒61. Canino G., Bravo M., Rubio-Stipec M., Woodbury M. (1990): The impact of disaster on mental health: prospective and retrospective analyses. International Journal of Mental Health, 19, pp. 51‒69. Carr, V. J., T. J. Lewin, R. A. Webster, J. A. Kenardy, P. L. Hazell , and G. L. Carter (1997a); Psychosocial Sequelae of the 1989 Newcastle Earthquake; II. Exposure and Morbidity profiles during the First 2 years Post-disaster, Psychological medicine 27 (1), pp. 167‒178. Carlson EB (1997): Trauma assessments: A clinicianʼs guide. New York: Guilford Press. Creamer M., Bell R., Failla S. (2003): Psychometric properties of the impact of event scale-revised. Behavior Research and Therapy, 41, pp. 1489‒1496. Cheng-Sheng Chen, Chung-Ping Cheng & et al. (2011): Validation of the Impact of Event Scale-Revised for adolescents experiencing the floods and mudslides in Taiwan. Kaohsing Journal of Medical Sciences 27, pp. 560‒565. Cronbach, L. J., & Meehl, P. E. (1955). Contruct validity in psychological tests. Psychological Bulletin, 52, pp. 281‒302. Dewitt, K. N., Kaltreider, N. B., Weiss, D. S. & Horowitz, M. J. (1983). Judging vchange in psychotherapy. Reliability of clinical for formulations. Archives of General Psychiatry. 40‒112‒118. Dr. Khin Maung Gyee and et al. (2008): Assessing Psychological Distress among Nargis Survivors..
(17) Validation of a Myanmar Version of the Impact of Event Scale-Revised in Survivors after Disaster(Khin Myo Htut, San San Oo, Zaw Sein Lwin) (343). 63. Davison J., Smith R., Kudler H. (1989): Validity and reliability of the DSM-III criteria for posttraumatic stress disorder: Experience with structured interview. J Nere Ment Dis 177, pp. 336‒341. Enrique F. Schisterman, David Faraggi and Jessica Hu (2008): Youden Index and the optimal threshold for markers with mass at zero; Sta Med. Jan 27(2), pp. 297‒315. Fatimah Lateef (2008): Cyclone Nargis and Myanmar; A wake up call: Journal of Emergencies, Trauma, and Shock 2009 May-Aug;2(2), pp. 106‒113. Frederick, C. J (ed) (1981); Emergency Mental Health Problems, DHHS Publication Number (ADM) 81‒956, Washington , D.C; US Government Printing Office. Frank W. Weathers, Terence M. Keane, and Jonathan R. T. Davidson (2001): Clinician- Administered PTSD Scaleʼ A Review of the First Ten Years of Research; Depression and Anxiety 13, pp. 132‒156. Frank W. Weathers, Terence M. Keane and Ayelet Meron Ruscio(1999): Psychometric Properties of Nine Scoring Rules for the Clinician-Administered Posttraumatic Stress Disorder Scale Vol. 11, No. 2, pp. 124‒133. Foa E. B., Riggs D. S., Dancu C. V., Rothbaum B. O. (1993). Reliability and validity of a brief instruction for assessing post-traumatic stress disorder. Jounnal of Traumatic Stress. 6, pp. 459‒473. Foa E. B., Riggs D. S., Dancu C. V., Rothbaum B. O. (1989): Behavioral/cognitive conceptualizations of posttraumatic stress disorder. Behavior Therapy; 20, pp. 155‒176. First M. B., Spitzer R. L., Gibbon M., Williams J. B. W. (1997): Structured Clinical interview for DSM-IV Axis I disorders: Clinician version. Washington, DC: American Psychiatric Press. Fukuda, S., K. Morimoto, K. Mure, and S. Maruyama (1999): Post-traumatic Stress and Change in Life Style among the Hanshin- Awaji Earthquake Victims, Preventive Medicine 29) 3), pp. 147‒151 Fujimori Tatsuo and Omori Tetsushi (2012): Recurring Natural Disaster and PTSD among survivors; Japanese Journal of Applied Psychology‒2012, Vol. 38 (special edition), pp. 68‒75. Galea, S., A. Nandimand, and D. Vlaohov (2005): the Epidemiology of Posttraumatic Stress Disorder after Disster, epidemiological Review 27, pp. 78‒91. Green B. L., J. D. Lindy, M. C. Grace, G. C. Gleser, A. C. Leonard, M. Karol, et al. (1990): Buffalo Creek survivors in the Second Decade : Stability of Stress Symptoms, American Journal of Orthopsychiatry 60, pp. 43‒54. Green BL(1993): Disaster and posttraumatic stress disorder. In JRT Davidson and EB Foa (Eds), Posttraumatic stress disorder. DSM-IV and beyond. (pp. 75‒97). Washington, DC: American Psychiatric Press. Guiseppe C., Palmira F., Giuseppe R., & Alessio G., (2013) the Impact of Event Scale-Revised: Psychometric properties of the Italian version in a sample of flood victims. Journal of Neuropsychiatric Disease and Treatment. 9, pp. 1427‒1432. Hyun K. L., Jong M. W., Tae-Suk K., Tae-Hyung K., Kyeong-Sook C., Sand-Keum C., Ik-Seoung C., Kyoung-Uk L., Ki C. P., Ho-Jun S., Won K., Bora J., Jeong-Ho C. (2009): Reliability and validity of the Korean version of the Impact of Event Scale-Revised, Comprehensive Psychiatry, pp. 385‒390. Horowitz, M. J. Stress response syndrome.1st ed.(1976): New York: Jason Aronson. Horowitz, M. J., Wilner, N., & Alvares, W. (1979): Impact of event scale; A measure of subjective stress. Psychosomatic Med, 41, pp. 209‒218. Hu Y., Stewart-Brown S., Twigg L., Weich S. (2007): Can the 12-item General Health Questionnaire be used to measure positive mental health? Psychological Medicine, pp. 37 (7), pp. 1005‒1013. Joseph S. Psychometric evaluation of Horowitzʼs Impact of Event Scale (2000): A review. Journal of Traumatic Stress.13, pp. 101‒113. Josefin S., Aili L., Johan D. A., Lisa Ekselius, Mimmie W., Bengt G. (2010): Validation of a Swedish version of the Impact of Event Scale-Revised (IES-R) in patients with burns; Journal of Anxiety Disorders 24‒618‒622 disaster Mental Health. A current Perspective. The Indian Journal of Social Work 61, pp. 664‒674. Juvva, S. and P. Rajenfran (2000); Disaster Mental Health: A current Perspective,. The Indian Journal of Social Work, 61 94), pp. 527‒541. Kyriaki Mystakidou, Antonis Galanos (2007): Psychometric Properties of the Impact of Event Scale in Greek Cancer Patients; 454 Journal of Pain and symptom management. Karanci, N. A. and A. Rustemli (1995): Psychological consequences of the 1992 Erzincan (turkey) Earthquake,.
(18) 64. (344). Yokohama Journal of Social Sciences, Vol. 19, No. 4・5. Disaster 19, pp. 8‒18. Kato, H., N. Asuki, Y. Miyake, Y. Minakawa, and K. Nishiyama (1996): Posttraumatic symptoms among Younger and Elder Evacuees in the Early Stages following the 1995 Hanshin-Awaji Earthquake in Japan. Acta Psychitrica Scaninavica 93, pp. 477‒481 Kato, H. & Iwai, K. (2000): Posttraumatic stress disorder after the Great Hanshin-Awaji Earthquake. Assessment by the structured interview to the survivors. Medical Journal of Kobe University, 60 (2), 147‒155. Kessler, R. C., Wittchen, H. U., Abelson, J., Zhao, S. (2000). Methodological issues in assessing psychiatric disorders with self-reports. In A.A. Stone, C. A. Kwon Y., Maruyam S., Morimoto K. (2001): Life events and posttraumatic stress in Hanshin-Awaji earthquake victims. Environmental Health Prevention Medicine 2001; 6, pp. 97‒103. Lai, T. J., C. M. Chang, K. M. Connor, L. C. Lee, and J. R. T. Davidson (2004): Full and Partial PTSD among Earthquake Survivors in Rural Taiwan, Journal of Psychiatric Research 38, pp. 313‒322. Last J. M., A dictionary of Epidemiology (1995): New York: Oxford University Press. Lopez-Castedo A., Fernandez L. (2005): Psychometric Properties of the Spanish Version of the 12-Item General Health Questionnaire in Adolescents. Percept Mot Skills. 100 (3 (Pt 1)), pp. 676‒680. Lima, B. R., S. Pai, H. Santacruz, J. Lozona, and J. Luna (1987); Screening for the Psychological Consequences of Major disaster in a Developing Country; Armero, Colombia, Acta Psychiatrica Scandinavica 76, pp. 561‒567. Lima, B. R., S. Pai, V. Taledo, L. Caris, J. M. haro, J. Lozona, and H. Sanacruz, (1993); Emotional Distress in disaster Victims; a Follow up Study, Journal of Nervous and mental disease, 181, pp. 388‒393. Mark Creamer, Richard Bell and Salvina Failla (2003): Psychometric properties of the Impact of Event ScaleRevised; Behaviour Research and Therapy 41‒1489‒1496. Mark Creamer, David Forbes and Dirk Biddle (2001): The validity of the PTSD checklist as a measure of symptomatic change in combat-related PTSD: Behavior Research and Therapy 39 (2001), pp. 977‒986. Maj, M., F. Statace, P. Crepet. S. Lobrace, F. Veltro, F. De marco, and D. Kemali (1989); Prevalence of Psychiatric Disorders among Subjects Exposed to a Natural Disaster. Acta Psychiatrica Scandinivica 79, pp. 544‒549. Madakasira, S. and F. OʼBrien (1987); Acute Posttraumatic Stress Disorder in Victims of a Natural Disaster, Journal of Merit. Dis.175, pp. 268‒290. Maercker A, Schuetzwohl M (1998): assessment of post-traumatic stress reactions: The impact of Event Scale-Revised (IES-R). Diagnostica; 44, pp. 130‒41. Metin Basoglu, Ebru Salcioglu and Maria Livanou (2002): Traumatic Stress Responses in Earthquake Survivors in Turkey. Journal of Traumatic Stress, Vol. 15, No. 4, August 2002, pp. 269‒276. Murphy S. A. (1984), Stress Levels and Health Status of Victims of a Natural Disaster, Res Nurs. Health 7, pp. 205‒215. Najarian L. M., Goenjian A. K., Pelcovitz D., mandel F., Najarian B. (2001): The effect of relocation after a natural disaster. Journal of Traumatic Stress 14, pp. 511‒526. Norris F. (1992): Epidemiology of trauma: Frequency and impact of different potentially traumatic events on different demographic groups. Journal of Consulting and Clinical Psychology. 60‒409‒418. Norris F., Perilla J. L., Ibanez G. E., Murphy A. D. (2001): Six differences in symptoms of posttraumatic stress: Does culture play a role? Journal of Traumatic Stress. 14, pp. 7‒28. Norris, F. H., A. D. Murphy, C. K. Baker, and J. L. Perilla (2004): Post Disaster PTSD over four Waves of a Panel Study of Mexicoʼs 1999 Flood, Journal of Traumatic Stress 17, pp. 283‒292. Norhayati MN & Aniza AA (2014): Psychometric properties of the Malay version of Impact of Event Scale-Revised (IES-R). International journal of collaborative Research on Internal medicine & Public Health.Vol. 6, No. 2. Nunnally JC, Bernstin IR (1994): Psychometric Theory.3rd ed. New York: Mc Graw-Hill. Olff, M., Langeland, W., Draijer, N., & Gersons, B. P. R. (2007) Gender Differences in Posttraumatic Stress Disorder. Psychological Bulletin, 133 (2), pp. 183‒204. Onder E., Tural U., Aker T., Kilic C., Erdogan S. (2006): Prevalence of psychiatric disorders three years after the 1999 earthquake in Turkey; Marmara Earthquake Survey (MES). Social psychiatry and Psychiatric Epidemiology 41, pp. 868‒874..
(19) Validation of a Myanmar Version of the Impact of Event Scale-Revised in Survivors after Disaster(Khin Myo Htut, San San Oo, Zaw Sein Lwin) (345). 65. Parslow R. A., Jorm A. F., Christensen H. (2006): Associations of pre-trauma attributes and trauma exposure with screening positive for PTSD: analysis of a community based study of 2085 young adults. Psychological Medicine 36, pp. 387‒395. Raphael, B. (1986): When disaster Strikes: How Individuals and Communities Cope with Catastrophe. New York: Basic Books. Shinfuku, N. (2002): disaster Mental Health; lessons Learned from the Hanshin Awaji Earthquake, World Psychiatry 1, pp. 158‒159. Sveen, J., Orwelius, L., Gerdin, B., Huss, F., Sjoberg. F., & willebrand, M. (2010): Psychometric properties of the Impact of Event Scale – Revised in patients one year after burn injury. Journal of Burn Care and Research, 31 (2), pp. 310‒318. Swiss Reinsurance Company Ltd. (2009): “Natural catastrophes and man-made disasters in 2008: North America and Asia suffer heavy losses”. 21 January 2009. p. 24. Retrieved 16 January 2010. Sudin E. C., Horowitz M. J. (2003): Horowitzʼs impact of event scale evaluation of 20 years of use. Psychosomatic Medicine, 65, pp. 870‒876. Udomratn, P. (2008): Mental Health and Psychosocial Consequences of Natural disaster in Asia, International Review of Psychiatry 20, pp. 441‒444. Wang, Li, Z. Yuqing, W. Wenzhong, S. Zhanbiao, S. Jianhua, L. Ming, and X. Yong (2009): Symptoms of Posttraumatic Stress Disorder Among Adult Survivors, Three Months After the Sichuan Earthquake in China, Journal of Traumatic Stress 22 (5), pp. 444‒450. Wang, X., Gao, N. Shinfuku, H. Zhang, C. Zhao, and Y. Shen (2000): Longitudinal Study of Earthquake – related PTSD in a Randomly Selected Community Sample in North China, American Journal of Psychiatry 157, pp. 1260‒1266. Weiss D. S. (2004a): The impact of event scale-revised. In: Wilson J. P., Keane T. M. (eds). Assessing psychological trauma and PTSD: A practitionerʼs hahdbook New York; Guilford Press. Weiss, D. S. (2004b): Structural clinical interviews for PTSD. In J. P. Wilson, & T. M. Keane (eds.), Assessing psychological trauma and PTSD: A practitionerʼs handbook (2nd ed., pp. 103‒121). New York: Guilford Press. Weiss, D. S, & Marmar, C. R. (1996). Psychometric review of the Impact of Event Scale-Revised. In: B. H. Stamm (eds). Measurment of stress, trauma, and adaptation (pp. 186‒188). Lutheville, MD: Sidran Press. Weiss, D. S, & Marmar, C. R. (1997). The Impact of Event Scale-Revised, Wilson, J. & Keane, T. (eds.), Assessing Psychological trauma and PTSD, The Guilford Press, New York, pp. 399‒411. Weiss, D. S., Zilberg, N. J., & Horowitz, M. J.(1982): Impact of Event Scale: A cross validation study and some empirical evidence supporting a conceptual model of stress response syndromes. Journal of Conculting and clinical Psychology, 50, pp. 407‒414. Weiss D. S (2003). Research methology and Statistics . In A. Tasman, J. A, Lieberman & J. Kay (eds). Psychiatry (2nd ed. Vol. 1) pp. 491‒506. Wu K. K., Chan KS(2004). The development of the Chinese version of the Impact of Event Scale-Revised (CIES-R) Social Psychiatry and psychiatric Epidemiology. 3, pp. 94‒98. World Health Organization (1978) Clinical modification of the World Health Organizationʼs Manual of the International Statistical Classification of Disease, Injuries & Causes of Death (9th eds ) Geneva. Xiaobo Zhou & et al. (2012); Prevalence and risk factors of post-traumatic stress disorder among adult survivors six months after the Wenchuan earthquake. Comprehensive Psychiatry 54 (2013), pp. 493‒499. [キン ミョ トウ 横浜国立大学大学院国際社会科学研究科博士課程後期] [サン サン オー 精神科医] [ザオ セイン ルィン 精神科医].
(20)
(21)
図

+3


関連したドキュメント
Keywords: continuous time random walk, Brownian motion, collision time, skew Young tableaux, tandem queue.. AMS 2000 Subject Classification: Primary:
It turns out that the symbol which is defined in a probabilistic way coincides with the analytic (in the sense of pseudo-differential operators) symbol for the class of Feller
We give a Dehn–Nielsen type theorem for the homology cobordism group of homol- ogy cylinders by considering its action on the acyclic closure, which was defined by Levine in [12]
Section 3 is first devoted to the study of a-priori bounds for positive solutions to problem (D) and then to prove our main theorem by using Leray Schauder degree arguments.. To show
This paper presents an investigation into the mechanics of this specific problem and develops an analytical approach that accounts for the effects of geometrical and material data on
Beyond proving existence, we can show that the solution given in Theorem 2.2 is of Laplace transform type, modulo an appropriate error, as shown in the next theorem..
While conducting an experiment regarding fetal move- ments as a result of Pulsed Wave Doppler (PWD) ultrasound, [8] we encountered the severe artifacts in the acquired image2.
The theory of log-links and log-shells, both of which are closely related to the lo- cal units of number fields under consideration (Section 5, Section 12), together with the
