Assessment of time - course changes in cerebral blood volume in preterm infants during the first 3 days of life using a portable near - infrared
time - resolved spectroscopy system
Tao FUJIOKA, Takeshi TAKAMI, Hiroki ISHII, Yuusuke SUGANAMI, Norio MIZUKAKI, Atsushi KONDO,
Daisuke SUNOHARA and Akinori HOSHIKA
Department of Pediatrics, Tokyo Medical University
Abstract
Objective
: The aim of this study was to evaluate, using a portable 3
-wavelength near
-infrared time
-resolved spectroscopy (NIR
-TRS) system, chronological changes in cerebral blood volume (CBV) and to clarify their asso- ciation with cerebral oxygen metabolism, PCO 2 , mean arterial blood pressure (MABP) and hematocrit (Ht) levels during the first 3 postnatal days of preterm infants.
Study Design
: CBV, cerebral oxygen saturation (cSO 2 ) and cerebral fractional tissue oxygen extraction (FTOE) among 31 preterm infants of 28
-35 weeks gestation were monitored using NIR
-TRS at 3
-6, 12, 24, 48 and 72 hours after birth with the optode placed on the front head. MABP, PCO 2 and Ht levels were measured simultaneously with the NIR
-TRS measurement.
Results
: CBV and cSO 2 transiently decreased 12 hours after birth and subsequently significantly increased (P<0.01) 72 hours after birth. Conversely, FTOE increased steadily until 12 hours after birth and then signifi- cantly decreased (P<0.01). CBV correlated with cSO 2 3
-6 hours (P<0.05, r=0.38), 12 hours (P<0.01, r=0.62) and 24 hours (P<0.05, r=0.36) after birth, with FTOE 12 hours (P<0.01, r=−0.58) after birth, and with Ht 3
-6 hours (P<0.01, r=−0.49), 48 hours (P<0.01, r=−0.51) and 72 hours (P<0.05, r=−0.38) after birth. There were no correlations among CBV, PCO 2 or MABP.
Conclusion
: This study indicates that changes in CBV may be related to those in the cerebral oxygen utili- zation and Ht level during the first 3 days of life in preterm infants.
Received November 4, 2011, Accepted December 19, 2011
Key words : Cerebral blood volume, Cerebral oxygen saturation, Cerebral fractional tissue oxygen extraction, Near
-infrared time
-re- solved spectroscopy, Preterm infant
Corresponding author : Tao Fujioka, MD., Department of Pediatrics, Tokyo Medical University, 6
-7
-1 Nishishinjuku, Shinjuku
-ku, Tokyo 160
-0023, Japan
TEL : +81
-(0)3
-3342
-6111 FAX : +81
-(0)3
-3344
-0643 E
-mail : [email protected] Introduction
Drastic hemodynamic changes in adaptation during the transition from fetal to extrauterine life lead to cardiac insufficiency and cerebral complications, including intra- ventricular hemorrhage (IVH) and hypoxic ischemic encephalopathy (HIE) in newborn infants during the postnatal period 1) . Furthermore, preterm infants are at
greater risk of these cerebral injuries due to their imma- turity. Cerebral complications are major problems that can cause long
-term neurological sequelae, and therefore it is essential to evaluate cerebral perfusion during the immediate postnatal period. To date, changes in cere- bral perfusion have not yet been fully elucidated.
Near
-infrared spectroscopy (NIRS) can noninvasively
investigate cerebral oxygenation and metabolism. Sev-
J. Tokyo Med. Univ., 70 (1) : 26
-33, 2012
eral kinds of NIRS instruments have been developed and widely applied to evaluate cerebral perfusion in different neonatal fields. Although there have been several reports on the quantification of cerebral blood flow (CBF) or cerebral blood volume (CBV) using NIRS in conjunc- tion with the intravenous 133 Xenon clearance technique 2) , rapid changes in arterial oxygen saturation 3
-7) and injec- tion of indocyanine green (ICG) 8) , these procedures may be harmful in immature neonates, and it is difficult to obtain measurements in sick infants.
By using a recently developed near
-infrared time
-resolved spectroscopy (NIR
-TRS) system, the distribu- tion of the optical path length is directly measured using a time
-correlated single photon counting (TCSPC) method 9)10) . Furthermore, by using a photon diffusion equation, we can measure absolute the light absorption coefficient (μ a ), light
-reduced scattering coefficient μ’ s , oxyHb and deoxyHb using a photon diffusion theory at the bedside, and also calculate CBV without performing any invasive procedures 11) .
In this study, we evaluated the time
-course changes in the CBV of preterm infants using a portable NIR
-TRS system and clarified their association with cerebral oxy- gen metabolism, PCO 2 , mean arterial blood pressure (MABP) and hematocrit (Ht) levels during the first 3 postnatal days.
Materials and Methods Study participants
We studied 31 preterm infants admitted to the neonatal intensive care unit of Tokyo medical university hospital from November 1, 2009 to February 28, 2011. The inclusion criteria of the study were as follows : 1) sub- jects without anomalies and who were not small for their gestational age ; 2) subjects who had not undergone a cranial ultrasound scan during the study ; 3) subjects who did not show severe electrolyte abnormalities or metabolic acidosis during the study ; 4) subjects who were maintained in a stable respiratory condition with or without mechanical ventilation (SpO 2 ≥ 90% and PCO 2
range=30
-60 mm Hg during the study period) ; 5) sub- jects with an Apgar score of greater than 7 at 5 min- utes. This study was approved by the Research Ethics Committee of Tokyo Medical University, and written informed consent was obtained from the parents of all infants.
NIR-TRS system and analysis
Measurements were obtained using a portable NIR
-TRS system (TRS
-20, Hamamatsu Photonics K.K., Shi- zuoka, Japan) employing the TCSPC method to obtain a temporal profile of the detected photons. This system features improved optical sensitivity compared with the TRS
-10 system 9)10) employing a GaAs photocathode pho- tomultiplier tube (H7422P
-50MOD, Hamamatsu Photon-
ics K.K.), with a quantum efficiency above 12% at approximately 800 nm. The TRS
-20 is computer
-con- trolled through a digital input/output (I/O) interface, con- sisting of a 3
-wavelength (761, 801 and 834 nm) pico- second light pulser (PLP, Hamamatsu Photonics K.K.) as the light source, a photon
-counting head (composed of a fast
-response, highly sensitive photomultiplier tube and high speed amplifier) with a 9
-step optical attenuator for single photon detection, and signal processing circuits (which consisted of a constant fraction discriminator, time
-to
-amplitude converter, analog/digital (A/D) con- verter and histogram memory) for time
-resolved mea- surement. The PLP generates a light pulse with a pulse width of 100 ps, a pulse rate of 5 MHz and an average power of approximately 80 µW. Three PLPs emit light pulses sequentially, and the 3
-wavelength light pulses are guided into 1 illuminating optical fiber by a fiber coupler (NTT Advanced Technology Corporation, Tokyo, Japan). A grated index (GI)
-type single optical fiber with a numerical aperture (NA) of 0.25 and a core diam- eter of 200 µm was used for tissue irradiation. An opti- cal bundle fiber (Moritex Corporation, Tokyo, Japan) with an NA of 0.26 and a bundle diameter of 3 mm was used to collect diffuse light from the tissue 12) for light detection.
To calculate the values of µ a , and μ’ s for the 3 wave- lengths, the re
-emission profiles observed at each mea- surement point were fitted into the photon diffusion equation proposed by Patterson et al 13) using the non
-lin- ear least squares fitting method. Then, oxyHb and deoxyHb levels were calculated from the µ a of the 3 wavelengths (761, 801 and 834 nm) using the following equations :
µ a 761 nm =ε oxyHb 761 nm C oxyHb +ε deoxyHb 761 nm C deoxyHb +ε H2O 761 nm C H2O
µ a 801 nm =ε oxyHb 801 nm C oxyHb +ε deoxyHb 801 nm C deoxyHb +ε H2O 801
nm C H2O
µ a 834 nm =ε oxyHb 834 nm C oxyHb +ε deoxyHb 834 nm C deoxyHb +ε H2O 834 nm C H2O
where ε m λ nm is the molar extinction coefficient of the sub- stance m at wavelength λ, and C m is the concentration of the substance m. On the assumption that in the living body, light absorption in this wavelength occurs in oxyHb, deoxyHb and water, and that there is no other background absorption in the living body, we determined the TRS values for TRS HbO 2 and TRS deoxyHb with a tissue water concentration of 85% 14)15) .
Cerebral total Hb (tHb) level, cerebral oxygen satura- tion (cSO 2 ), CBV and cerebral fractional tissue oxygen extraction (FTOE) were obtained using the following equations 11)16) .
[tHb] (μM)=[oxyHb]+[deoxyHb]
cSO 2 (%)=[oxyHb]/[tHb]×100
CBV (mL/100 g)=[tHb]×MW Hb ×10
-6 /(tHb×10
-2 ×Dt
×10) FTOE=(SpO 2 – cSO 2 )/SpO 2
where [ ] indicates the Hb level (µM), MW Hb is the molecular weight of Hb (64,500), tHb is the blood Hb level (g/dL), and Dt is the brain tissue density (1.05 g/
mL). The TRS
-20 was switched on for more than 20 min- utes before measurements were taken to stabilize the sys- tem. The optode with a distance of 30 mm between the irradiation fiber and the detection fiber was placed on the front head, and was covered with an opaque cloth to pre- vent stray light from reaching the detector. Measure- ments were taken in the reflectance mode 3
-6, 12, 24, 48 and 72 hours after birth. The conditions of infants were stable, and each measurement session lasted for more than 1 minute. If the measurement was affected by movement artifact or stray light, we took repeated mea- surements until we obtained reproducible data.
Measurements of other variables
Heart rate (HR), MABP and SpO 2 were monitored and recorded simultaneously with the NIRS measurement by a neonatal monitoring system (BSM
-2300 ; Nihon Kohden Corporation, Tokyo, Japan). MABP was mea- sured either directly with arterial lines or indirectly (oscillometric technique with an inflatable cuff : BSN
-2303 ; Nihon Kohden Corporation). HR and SpO 2
were continuously measured using a pulse oximeter (Nellcor Pulse Oximeter N
-200 ; Tyco Healthcare Japan, Tokyo, Japan). Blood gas (PCO 2 , blood Hb and Ht) levels were collected by a heel lance immediately after TRS
-20 measurements (ABL835 ; Radiometer K.K., Tokyo, Japan). The data were stored in a personal com- puter, and we calculated the median values over the mea- surement period.
Statistical analysis
Statistical analyses were performed using the computer package SPSS II for Windows (SPSS Japan, Tokyo, Japan). The gestational age (GA) and birth weight were expressed as means±standard deviation (SD). Serial data obtained using NIR
-TRS and physical examination at different time points were compared using repeated
-measures one
-way ANOVA, followed by Bonferroni multiple comparison tests. The Pearson correlation coefficient and simple linear regression analysis were used to determine the relationships among CBV, cSO 2 , MABP, PCO 2 and Ht level at each measurement point. A P value of less than 0.05 was considered to indicate a statistically significant difference.
Results
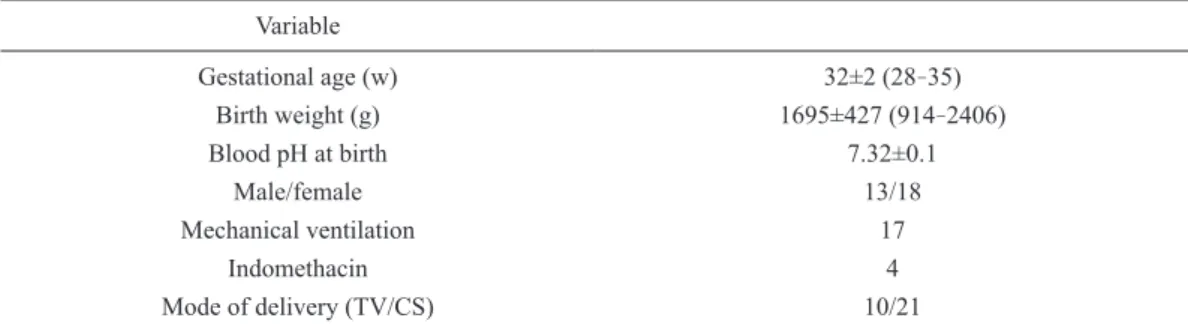
Cerebral complications were not diagnosed by cranial ultrasound examinations during the study period. Peri- ventricular leukomalacia diagnosed by magnetic reso- nance imaging developed in 1 infant before dis- charge. The clinical variables of the infants are shown in Table 1.
The mean CBV was 1.67±0.28 (standard deviation (SD)) mL/100 g during the study period. The mean cSO 2 was 71.1%±4.2% (SD) during the study period.
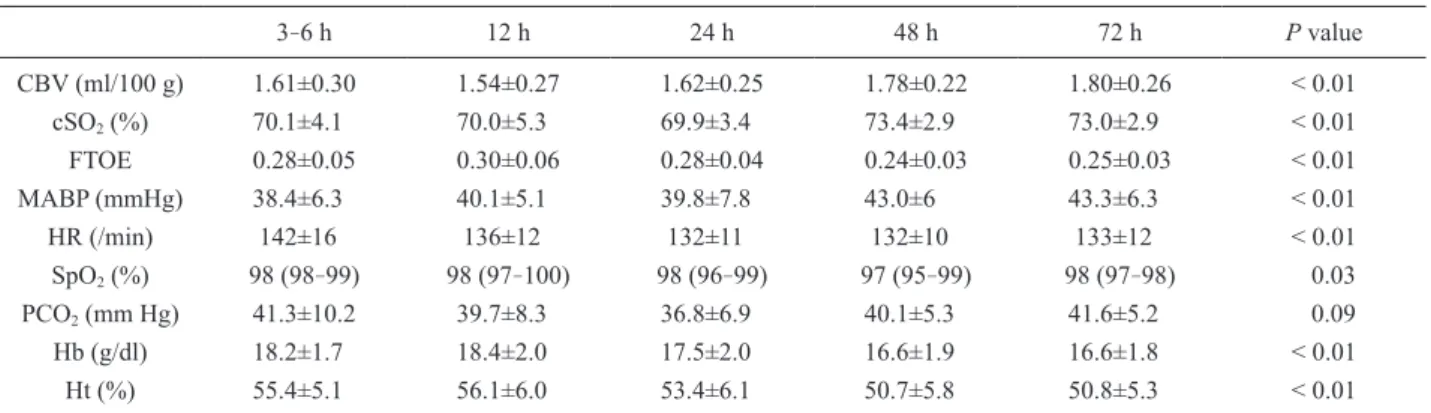
Changes in CBV, cSO 2 , FTOE, MABP, HR, SpO 2 , PCO 2 , and blood Hb and Ht levels are shown in Table 2. CBV steadily decreased until 12 hours after birth and then gradually increased. There was a marked increase in CBV between 12 hours and 48, and 72 hours after birth. Similarly, cSO 2 decreased steadily until 12 hours after birth, followed by a gradual increase. The cSO 2
increased significantly between 3 to 6 hours and 48, and 72 hours, between 12 hours and 48, and 72 hours, between 24 hours and 48, and 72 hours after birth.
Converse to CBV and cSO 2, FTOE increased steadily until 12 hours after birth, followed by a gradual decrease.
There was a marked decrease in FTOE between 3 to 6 hours and 48, and 72 hours, between 12 hours and 48, and 72 hours, and between 24 hours and 48 hours after birth. There were marked changes in MABP, HR, SpO 2 , and blood Hb and Ht levels.
The MABP increased significantly between 3 to 6 hours and 48, and 72 hours after birth. The HR decreased significantly between 3 to 6 hours and 24, 48, and 72 hours after birth. SpO 2 showed a marked decrease between 12 hours and 48 hours after birth.
There were marked decreases in blood Hb levels between
Table 1 Clinical data of 31 infant subjects Variable
Gestational age (w) 32±2 (28
-35)
Birth weight (g) 1695±427 (914
-2406)
Blood pH at birth 7.32±0.1
Male/female 13/18
Mechanical ventilation 17
Indomethacin 4
Mode of delivery (TV/CS) 10/21
Values are presented as means (standard deviation [SD]) of number of cases
VD, vaginal delivery ; CD, cesarean delivery
3 to 6 hours and 48, and 72 hours, and between 12 hours and 48, and 72 hours after birth. There were significant decreases in Ht level between 3 to 6 hours and 48, and 72 hours, between 12 hours and 48, and 72 hours after birth. There was no significant change in PCO 2 .
The correlations between CBV and other variables are shown in Table 3. There were significant correlations between CBV and cSO 2 3
-6 hours (P<0.05, r=0.38), 12 hours (P<0.01, r=0.62) and 24 hours (P<0.05, r=0.36) after birth. There was a significant inverse correlation between CBV and FTOE 12 hours (P<0.01, r=−0.58) after birth. Analysis of the correlation between cSO 2
and FTOE was not appropriate as FTOE was derived from cSO 2 . There was a significant inverse correlation between CBV and Ht 3
-6 hours (P<0.01, r=−0.49), 48 hours (P<0.01, r=−0.51) and 72 hours (P<0.05, r=
−0.38) after birth. Analysis of correlations among CBV and [tHb] and blood Hb levels was not appropriate as CBV was derived from [tHb] and blood Hb lev- els. There were no correlations between CBV and PCO 2 , or between CBV and MABP.
Discussion
We set out to evaluate the time course changes in CBV
of preterm infants by NIR
-TRS and clarified their associ- ation with cerebral oxygen metabolism, PCO 2 , MABP and Ht levels during the first 3 postnatal days. There have been several studies of CBV in neonates by NIRS using oxyHb 3)4) or ICG 8) as a tracer. The estimated CBVs were 2.22±0.4 and 3.7 mL/100 g using the modi- fied Beer
-Lambert law, with changes in arterial satura- tion 3) and PCO 2 4) , respectively. Leung et al 8) reported an estimated CBV of 1.72±0.76 mL/100 g as determined by NIR
-SRS with ICG. Ijichi et al 11) reported an absolute CBV of 2.31±0.56 mL/100 g as determined by NIR
-TRS in neonates (mean GA : 36.8±3.1 (SD) wks, mean BW : 2,365±791 g (SD)). These results were higher than those of the present study (1.67±0.28 (SD) mL/100 g). It has been reported that CBV increases with postcon- ceptional age, and that the relationship between these variables was based on the results of anatomic studies of the development of cerebral blood vessels 11)17) . Further- more, it has been reported that the CBV in human adults was 4.81±0.37 mL/100 g using single
-photon emission computed tomography 18) , and 4.7±1.1 mL/100 g using positron emission tomography 19) , which were higher than those in neonates. Wyatt et al 3) speculated that regional Table 2 Measurement results
3
-6 h 12 h 24 h 48 h 72 h P value
CBV (ml/100 g) 1.61±0.30 1.54±0.27 1.62±0.25 1.78±0.22 1.80±0.26 < 0.01
cSO
2(%) 70.1±4.1 70.0±5.3 69.9±3.4 73.4±2.9 73.0±2.9 < 0.01
FTOE 0.28±0.05 0.30±0.06 0.28±0.04 0.24±0.03 0.25±0.03 < 0.01
MABP (mmHg) 38.4±6.3 40.1±5.1 39.8±7.8 43.0±6 43.3±6.3 < 0.01
HR (/min) 142±16 136±12 132±11 132±10 133±12 < 0.01
SpO
2(%) 98 (98
-99) 98 (97
-100) 98 (96
-99) 97 (95
-99) 98 (97
-98) 0.03
PCO
2(mm Hg) 41.3±10.2 39.7±8.3 36.8±6.9 40.1±5.3 41.6±5.2 0.09
Hb (g/dl) 18.2±1.7 18.4±2.0 17.5±2.0 16.6±1.9 16.6±1.8 < 0.01
Ht (%) 55.4±5.1 56.1±6.0 53.4±6.1 50.7±5.8 50.8±5.3 < 0.01
Values are presented as means±standard deviation [SD]. Data for SpO
2are presented as medians (interquartile range [IQR]).
CBV : cerebral blood volume ; cSO
2: cerebral oxygen saturation ; FTOE : fractional regional cerebral oxygen extraction ; MABP : mean arterial blood pressure ; HR : heart rate ; Hb : blood hemoglobin ; Ht : hematocrit
Statistical values were generated by one
-factor repeated measures ANOVA. Details of analyses performed using the Bonferroni multiple comparison test are described in the text.
Table 3 Correlations between CBV and other variables
V ariable 3
-6 h 12 h 24 h 48 h 72 h
MABP P > 0.05 P > 0.05 P > 0.05 P > 0.05 P > 0.05 PCO
2P > 0.05 P > 0.05 P > 0.05 P > 0.05 P > 0.05
Ht P < 0.01
r = −0.49 P > 0.05 P > 0.05 P < 0.01
r = −0.51 P < 0.05 r = −0.38 FTOE P > 0.05 P < 0.01
r = −0.58 P > 0.05 P > 0.05 P > 0.05 cSO
2P < 0.05
r = 0.38 P < 0.01
r = 0.62 P < 0.05
r = 0.36 P > 0.05 P > 0.05
r = Pearson correlation coefficient
CBV was lower in the white matter than in the gray cere- bral matter, and the relatively low mean CBVs in infants may reflect a relative preponderance of the white matter compared with the adult brain. These hypotheses sup- port the current results, as the mean GA in this study (32 wks) was shorter than that of a study using NIR
-TRS (36.8 wks) 11) . The different time window of measure- ments may also have influenced these results, because CBV measurements by NIRS using oxyHb 3)4) and ICG 8) as a tracer were higher than the current results, despite the immaturities noted (mean GA : 29 wks 3)4) and 28 wks 8) ).
Changes in CBV mainly represent alterations in cere- bral Hb levels, which may be influenced by CBF. In this study, CBV gradually decreased until 12 hours from birth. We previously reported a relationship between systemic circulation and cerebral circulation by echocar- diography and NIR
-SRS in extremely low birth weight (ELBW) infants during the first 3 days after birth 20) which demonstrated that the tissue oxygenation index (TOI) values that represented CBF with stable blood Hb and SpO 2 levels 21)22) decreased until 12 hours and then increased gradually. The changing pattern of the CBV in the present study was similar to that of the TOI in our previous study. We also demonstrated in our previous report that the changing pattern of TOI was similar to that of systemic perfusion in terms of left ventricle car- diac output and superior vena cava flow. We proposed that the changes in cerebral oxygenation and blood flow immediately after birth were likely to reflect low cardiac output because of the limited capacity of the immature myocardium to adapt to perinatal circulatory change.
It has been said that PCO 2 is important factors that affect CBF. Cerebrovascular resistance decreases with an increase in PCO 2 23)
. CBF measurements using the Xenon clearance technique have indicated that an increase in postnatal age correlates with changes in PCO 2 2) . However, several other reports have failed to demonstrate a relation between CBF and PCO 2 5)7) . In the present study, there was no correlation between CBV and PCO 2 . While a report by Pryds and Greisen 2) showed a correlation between CBV and PCO 2 , the mean PCO 2 levels were (4.0 (30), 4.6 (34.5) and 4.4 (33) kPa (mm Hg) on days 1, 2 and 3, respectively), which were lower than the present results (mean : 39.9±7.5 (SD) mm Hg). This may explain why PCO 2 did not affect cerebrovascular resistance at approximately 40 mm Hg in the present study.
The Ht level increased until 12 hours after birth, and then gradually decreased. This changing pattern of Ht was inversely correlated to that of CBV, and we found significant inverse correlations between these vari- ables. The current results are supported by a study which demonstrated a significant inverse correlation
between CBF and arterial blood Hb concentration 2) , or Ht level 24) using the Xenon clearance technique. Although both arterial oxygen content and blood viscosity have been reportedly related to CBF 25) , it has been suggested that CBF increased mainly as a compensatory mecha- nism for the lower oxygen
-carrying capacity to maintain constant oxygen delivery 2)24)26) .
In the present study, we showed an inversely changing pattern in CBV and FTOE, and found a significant nega- tive correlation between these variables 12 hours after birth.
Cerebral fractional oxygen extraction (FOE) is a use- ful measurement variable which represents the ratio of cerebral oxygen consumption to cerebral oxygen deliv- ery 27) . Naulaes et al 16) showed a close correlation between the FTOE measured by NIRS and the actual FOE in piglets and concluded that FTOE is likely to pro- vide important information on the oxygenation status of the brain. An increase in FTOE reflects an increase in oxygen extraction by brain tissue, suggesting a higher consumption of oxygen than delivery and a decrease in FTOE indicates less utilization of oxygen by brain tissue compared with oxygen supply. There have been several reports of a relationship between blood Hb level and FTOE. Van Hoften et al 28) found that blood transfusion led to a decrease in FTOE, which indicated that if the blood Hb level decreased, FTOE would increase as a compensatory mechanism to maintain cerebral tissue oxygenation. However, in the present report, although the blood Hb level decreased, FTOE continued to decrease concurrently with an increase in CBV after birth. These results suggest that any increase in CBV which occurs as a result of an increase in CBF depends not only on a change in Ht level as described above, but also on other variable changes as adaptations from fetal to extrauterine life. Meek et al 5) and Kissack et al 6)7) showed an increase in CBF during the first 3 days of life of ELBW infants, and proposed that this change may be a normal adaptive response of the cerebral circulation to postnatal life. We speculate that an increase in oxygen delivery via increased CBF as an adaptive response exceeds a decrease in oxygen delivery via decreased blood Hb level. As a result of increased CBF, sufficient oxygen is delivered to the brain, possibly causing FTOE to decrease.
The relationship between cerebral perfusion and arte-
rial blood pressure is controversial. Tsuji et al 29)
reported that in preterm neonates, blood pressure and
cerebral oxygenation index (oxyHb level
-deoxyHb
level), which possibly reflects CBF, have a significant
association, which indicates an absence of cerebral auto-
regulation in some preterm infants. In this study, we
found no correlation between CBV and MABP. This
result suggests that the autoregulation of cerebral circula-
tion was intact in the subjects in our cohort. However, as the number of patients was small, the results should be interpreted cautiously, and further studies are required.
The change in cSO 2 is determined mainly by changes in blood Hb level, SpO 2, CBF, the cerebral metabolic rate of oxygen utilization and the arterial and venous anatom- ical ratio. For this reason, it has been considered that a change in cSO 2 may reflect a change in CBF among infants with stable blood Hb and SpO 2 levels 21)22) . How- ever, in the present study, although we demonstrated similar changing patterns in CBV and cSO 2, a significant correlation between these variables was not shown 48 hours after birth. This may be because the drastic changes in FTOE and blood Hb levels, which influence cerebral hemodynamics during the immediate postnatal period, affected these relationships.
There were some limitations in this study. The num- ber of patients of this cohort was small, and there were patients with various circulatory conditions. It has been considered that respiratory distress syndrome, surfactant therapy and mechanical ventilation influence cerebral hemodynamics 30)31) . However, these conditions were not investigated in the present study. Furthermore, although the sensitivity and the reliability of this NIR
-TRS system have previously been assessed using a piglet hypoxia model 32) , there have been few reports regarding the cerebral perfusion of human neonates, and further studies are required.
In conclusion, we evaluated changes in cerebral perfu- sion in preterm infants during the immediate postnatal period using a newly developed portable NIR
-TRS sys- tem without any invasive procedures. CBV showed a significant increase, and CBV changes may be related to changes in CBF, the cerebral metabolic rate of oxygen utilization, and Ht level. Serial measurements of these parameters at bedside using a portable NIR
-TRS system may be useful for evaluating postnatal changes in CBV and the cerebral metabolism of preterm infants in an intensive care unit.
Acknowledgments
We would like to thank Motoki Oda (Central Research Laboratory, Hamamatsu Photonics K.K.) for his techni- cal assistance, and the nursing staff in the NICU of Tokyo Medical University Hospital for their coopera- tion. We are also indebted to Mr. Roderick J. Turner, Assistant Professor Edward F. Barroga and Professor J.
Patrick Barron, Chairman of the Department of Interna- tional Medical Communications at Tokyo Medical Uni- versity, for their editorial review of the English manu- script.
Conflict of interest
All authors declare no conflicts of interest associated
with this study. There was no external financial support received for this study.
Reference
1) Phibbs RH : Delivery room management. In : Neonatology
-Pathophysiology Management of the Newborn (Avey GB, Flietcher MA and MacDonald MG, Lippincott Wiliams & Wilkins eds), 5 th edn, 279
-300, Philadelphia, 1999
2) Pryds O, Greisen G : Effect of PaCO 2 and haemoglo- bin concentration on day to day variation of cerebral blood flow in preterm neonates. Acta Paediatr Scand Suppl 360 : 33
-36, 1989
3) Wyatt JS, Cope M, Delpy DT, Wray S, Reynolds EO : Quantification of cerebral oxygenation and hae- modynamics in sick newborn infants by near infrared spectroscopy. Lancet 2 : 1063
-1066, 1986
4) Brun NC, Greisen G : Cerebrovascular responses to carbon dioxide as detected by near
-infrared spectroscopy : comparison of three measures. Pedi- atr Res 36 : 20
-24, 1994
5) M e e k J H , Ty s z c z u k L , E l w e l l C E , Wy a t t JS : Cerebral blood flow increases over first three days of life in extremely preterm neonates. Arch Dis Child Fetal Neonatal Ed 78 : F33–F37, 1998 6) Kissack CM, Garr R, Wardle SP and Weindling
AM : Cerebral fractional oxygen extraction in very low birth weight infants is high when there is low left ventricular output and hypocarbia but is unaffected by hypotension. Pediatr Res 55 : 400
-405, 2004 7) Kissack CM, Garr R, Wardle SP, Weindling
AM : Cerebral fractional oxygen extraction is inversely correlated with oxygen delivery in the sick, newborn, preterm infant. J Cereb Blood Flow Metab 25 : 545
-553, 2005
8) Leung TS, Aladangady N, Elwell CE, Delpy DT, Cos- teloe K : A new method for the measurement of cere- bral blood volume using near infrared spatially resolved spectroscopy and indocyanine green : application and validation in neonates. Pediatr Res 55 : 134
-141, 2004
9) Oda M, Yamashita Y, Nakano T, Suzuki A, Shimizu K, Hirano I, Shimomura F, Ohmae E, Suzuki T, Tsuchiya Y : Near
-infrared time
-resolved spectros- copy system for tissue oxygenation monitor. Proc SPIE 4160 : 204
-210, 2000
10) Ohmae E, Oda M, Suzuki T, Yamashita Y, Kakihana Y, Matsunaga A, Kanmura Y, Tamura M : Clinical evaluation of time
-resolved spectroscopy by measur- ing cerebral hemodynamics during cardiopulmonary bypass surgery. J Biomed Optics 12 : 062112, 2007 11) Ijichi S, Kusaka T, Isobe K, Okubo K, Kawada K,
Namba M, Okada H, Nishida T, Imai T, Itoh S :
Developmental changes of optical properties in neo-
nates determined by near
-infrared time
-resolved
spectroscopy. Pediatr Res 58 : 568
-573, 2005
12) Liebert A, Wabnitz H, Grosenick D and Macdonald R : Fiber dispersion in time domain measurements compromising the accuracy of determination of opti- cal properties of strongly scattering media. J Biomed Optics 8 : 512
-516, 2003
13) Patterson MS, Chance B, Wilson B : Time resolved reflectance and transmittance for the non
-invasive measurement of optical properties. Appl Opt 28 : 2331
-2336, 1989
14) Cooper CE, Elwell CE, Meek JH, Matcher SJ, Wyatt JS, Cope M, Delpy DT : The noninvasive measure- ment of absolute cerebral deoxyhemoglobin concen- tration and mean optical pathlength in the neonatal brain by second derivative near infrared spectros- copy. Pediatr Res 39 : 32
-38, 1996
15) Ohmae E, Ouchi Y, Oda M, Suzuki T, Nobesawa S, Kanno T, Yoshikawa E, Futatsubashi M, Ueda Y, Okada H, Yamashita Y : Cerebral hemodynamics evaluation by near
-infrared time
-resolved spectroscopy : Correlation with simultaneous posi- tron emission tomography measurements. Neuroim- age 29 : 697
-705, 2006
16) Naulaers G, Meyns B, Miserez M, Leunens V, Van Huffel S, Casaer P, Weindling M, Devlieger H : Use of tissue oxygenation index and fractional tissue oxy- gen extraction as non
-invasive parameters for cere- bral oxygenation. A validation study in pig- lets. Neonatology 92 : 120
-126, 2007
17) Ballabh P, Braun A, Nedergaard M : Anatomic analy- sis of blood vessels in germinal matrix, cerebral cor- tex, and white matter in developing infants. Pediatr Res 56 : 117
-124, 2004
18) Sakai F, Nakazawa K, Tazaki Y, Katsumi I, Hino H, Igarashi H, Kanda T : Regional cerebral blood vol- ume and hematocrit measured in normal human vol- unteers by single
-photon emission computed tomog- raphy. J Cereb Blood Flow Metab 5 : 207
-213, 1985
19) Powers WJ, Grubb RL Jr, Darriet D, Raichle ME : Cerebral blood flow and cerebral metabolic rate of oxygen requirements for cerebral function and viabil- ity in humans. J Cereb Blood Flow Metab 5 : 600
-608, 1985
20) Takami T, Sunohara D, Kondo A, Mizukaki N, Suga- nami Y, Takei Y, Miyajima T, Hoshika A : Changes in cerebral perfusion in extremely LBW infants dur- ing the first 72 h after birth. Pediatr Res 68 : 435
-439, 2010
21) Elwell CE, Henty JR, Leung TS, Austin T, Meek JH, Deply DT, Wyatt JS : Measurement of CMRO2 in neonates undergoing intensive care using near infra- red spectroscopy. Adv Exp Med Biol 566 : 263
-268, 2005
22) Wong FY, Leung TS, Austin T, Wilkinson M, Meek JH, Wyatt JS, Walker AM : Impaired autoregulation in preterm infants identified by using spatially resolved spectroscopy. Pediatrics 121 : e604
-e611, 2008
23) Greisen G, Trojaborg W : Cerebral blood flow, PaCO 2
changes, and visual evoked potentials in mechanically ventilated, preterm infants. Acta Paediatr Scand 76 : 394
-400, 1987
24) Younkin DP, Reivich M, Jaggi JL, Obrist WD, Delivoria
-Papadopoulos M : The effect of hematocrit and systolic blood pressure on cerebral blood flow in newborn infants. J Cereb Blood Flow Metab 7 : 295
-299, 1987
25) Hudak ML, Koehler RC, Rosenberg AA, Traystman RJ, Jones MD Jr : Effect of hematocrit on cerebral blood flow. Am J Physiol 251 : H63
-70, 1986 26) Liem KD, Hopman JC, Oeseburg B, de Haan AF,
Kollée LA : The effect of blood transfusion and hae- modilution on cerebral oxygenation and haemody- namics in newborn infants investigated by near infra- red spectrophotometry. Eur J Pediatr 156 : 305
-310, 1997
27) Yoxall CW, Weindling AM : Measurement of cere- bral oxygen consumption in the human neonate using near
-infrared spectroscopy : cerebral oxygen con- sumption increases with advancing gestational age. Pediatr Res 44 : 283
-290, 1998
28) Van Hoften JCR, Verhagen EA, Keating P, Ter horst HJ, Bos AF : Cerebral tissue oxygen saturation and extraction in preterm infants before and after blood transfusion. Arch Dis Child Fetal Neonatal Ed 95 : F352
-F358, 2010
29) Tsuji M, Saul JP, du Plessis A, Eichenwald E, Sobh J, Crocker R, Volpe JJ : Cerebral intravascular oxygen- ation correlates with mean arterial pressure in criti- cally ill premature infants. Pediatrics 106 : 625
-632, 2000
30) Mullaart RA, Hopman JC, De Haan AF, Rotteveel JJ, Daniëls O, Stoelinga GB, De Haan AF : Cerebral blood flow fluctuation in neonatal respiratory distress and periventricular haemorrhage. Early Hum Dev 37 : 179
-185, 1994
31) Lemmers PM, Toet MC, van Schelven LJ, van Bel F : Cerebral oxygen extraction in the preterm infant : the impact of respiratory distress syn- drome. Exp Brain Res 173 : 458
-467, 2006 32) Ijichi S, Kusaka T, Isobe K, Islam F, Okubo K, Okada
H, Namba M, Kawada K, Imai T, Itoh S :
Quantification of cerebral hemoglobin as a function
of oxygenation using near
-infrared time
-resolved
spectroscopy in a piglet model of hypoxia. J
Biomed Opt 10 : 24026, 2005
近赤外時間分解分光装置を用いた早産児における生後 3 日間の 脳血液量の経時的評価
藤 岡 泰 生 高 見 剛 石 井 宏 樹 菅 波 佑 介 水 書 教 雄 近 藤 敦
春 原 大 介 星 加 明 德
東京医科大学小児科学講座
【目的】 移動式
3
波長近赤外時間分解分光法システム (NIR-TRS ; near
-infrared time
-resolved spectroscopy)
を用い た、早産児における生後3
日間の脳血液量 (CBV; cerebral blood volume)
の経時的変化の評価及び、CBVと脳組織 酸素代謝、血中二酸化炭素分圧 (PCO2
)、平均血圧との関連性の検討を目的とした。【対象および方法】 対象は在胎 週数28
-35
週の早産児31
例。NIR-TRS
のオプトードを前額部に設置し、生後3
-6、12、24、48、72
時間においてCBV、脳組織ヘモグロビン酸素飽和度
(cSO2
)、脳組織fractional tissue oxygen extraction
(FTOE)を計測した。NIR-TRS
計測と同時に、平均血圧、PCO2
、ヘマトクリット (Ht)を測定した。【結果】 CBVとcSO 2
は生後12
時間に一 過性に低下し、その後、72時間にかけ有意な上昇を示した (P < 0.01)のに対し、FTOE
は生後12
時間に一過性に上 昇し、その後、有意な低下 (P < 0.01)を示した。CBV
とcSO 2
の間に生後3
-6
時間 (P < 0.05、r=0.38)、12時間 (P< 0.01、 r=0.62)、 24
時間 (P < 0.05、r=0.36)において有意な正の相関を認めた。CBV
とFTOE
の間に生後12
時間 (P< 0.01、r=−0.58)において有意な負の相関を認めた。CBV
とHt
の間に生後3
-6
時間 (P < 0.01、r=−0.49)、48時 間 (P < 0.01、r=−0.51)、72時間 (P < 0.01、r=−0.38)において有意な負の相関を認めた。CBV
とPCO 2
、平均血圧 の間に有意な相関は認めなかった。【結語】 本研究により早産児における生後3
日間のCBV
の変化は脳における酸 素摂取率や血中Ht
に影響を受ける可能性が示唆された。〈キーワード〉 脳血液量 (CBV)、脳組織ヘモグロビン酸素飽和度 (cSO
2
)、FTOE、近赤外時間分解分光法
(NIR-TRS)、
早産児