by dropped gallstones after cholecystectomy :
Four cases diagnosed with multimodality
imaging.
著者
SATO Shigetaka, INOUE Akitoshi, OTA Shinichi,
FURUKAWA Akira, MIYAGAWA Yoshihiro, WAKAMIYA
Makoto, HIROSE Tomohiro, FURUICHI Kenji,
WATANABE Yoshiyuki
journal or
publication title
Radiology Case Reports
volume
15
number
9
page range
1480-1484
year
2020-09
URL
http://hdl.handle.net/10422/00012755
doi: 10.1016/j.radcr.2020.05.073(https://doi.org/10.1016/j.radcr.2020.05.073)
This is an open access article under the CC BY-NC-ND license.
(http://creativecommons.org/licenses/by-nc-nd/4.0/)
R a d i o l o g y C a s e R e p o r t s 1 5 ( 2 0 2 0 ) 1 4 8 0 – 1 4 8 4
Available
online
at
www.sciencedirect.com
journal
homepage:
www.elsevier.com/locate/radcr
Case
report
Foreign-body
granulomas
and
abscesses
caused
by
dropped
gallstones
after
cholecystectomy:
Four
cases
diagnosed
with
multimodality
imaging
✩
,
✩✩
Shigetaka
Sato,
MD
a,
Akitoshi
Inoue,
MD,
PhD
a,∗,
Shinichi
Ota,
MD,
PhD
a,
Akira
Furukawa,
MD,
PhD
b,
Yoshihiro
Miyagawa,
MD
c,
Makoto
Wakamiya,
MD,
PhD
c,
Tomohiro
Hirose,
MD,
PhD
d,
Kenji
Furuichi,
MD,
PhD
d,
Yoshiyuki
Watanabe,
MD,
PhD
a aDepartmentofRadiology,ShigaUniversityofMedicalScience,Seta,Tsukinowa-cho,Otsu-city,Shiga,520-2192,Japan
bDepartmentofRadiologicalScience,TokyoMetropolitanUniversity,7-2-1,Higashioku,Arakawa-ku,Tokyo,
116-8551,Japan
cDepartmentofRadiology,NagahamaCityHospital,313,Oinui-cho,Nagahama-city,Shiga,526-8580,Japan dDepartmentofRadiology,SaiseikaiNoeHospital,1-3-25,Furuichi,Joto-ku,Osaka-city,Osaka,536-0001,Japan
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received17April2020 Revised20May2020 Accepted21May2020 Keywords: Foreign-bodygranuloma Droppedgallstone Laparoscopiccholecystectomy Spilledgallstonea
b
s
t
r
a
c
t
Fourcases(agerange,60-78years,male:female=1:3)whohadundergonecholecystectomy presentedwithfever(n=1),rightabdominalpainwithfever(n=1),appetitelosswithfever (n=1),andabsenceofsymptoms(n=1).Computedtomography(CT)showedan irregular-shapedinvasivemassorfluidcollectionintherightMorrison’spouch,rightparacolicgutter, gallbladderfossa,subphrenicspace,orabdominalwall.CTandultrasoundrevealed gall-stonesinthegranulomain3casesandanabscessinonecase.Theinflammatoryprocess inducedbydroppedgallstonesmaymimicperitonealmalignancies.Awarenessof chole-cystectomyandthedetectionofgallstonesinthelesionareessentialforthediagnosisof droppedgallstones.
© 2020TheAuthors.PublishedbyElsevierInc.onbehalfofUniversityofWashington. ThisisanopenaccessarticleundertheCCBY-NC-NDlicense. (http://creativecommons.org/licenses/by-nc-nd/4.0/)
Introduction
Gallstones are a common digestive disorder, witha preva-lenceofapproximately 10%-20% inNorthAmerica and Eu-ropeand<10%inAsia.Mostindividualswithgallstonesare
✩ Acknowledgements:Nofundingwasreceivedforthisstudy.TheauthorswouldliketothankEnago(www.enago.jp)fortheEnglish languagereview.
✩✩DeclarationofCompetingInterest:Theauthorshavenocompetingintereststoreport. ∗Correspondingauthor.
E-mailaddress:[email protected](A.Inoue).
asymptomatic;however,severesymptomsandcomplications developinapproximately1%-3%ofasymptomaticormildly symptomatic patientsannually [1].Acute cholecystitis pre-dominantly occurs as a complication of gallstone disease, and laparoscopic cholecystectomy is widely accepted as a standard surgical procedure, even for patients with acute
https://doi.org/10.1016/j.radcr.2020.05.073
1930-0433/© 2020The Authors.Publishedby ElsevierInc.on behalfof UniversityofWashington.Thisisanopenaccessarticleunderthe CCBY-NC-NDlicense.(http://creativecommons.org/licenses/by-nc-nd/4.0/)
Fig.1– A67-year-oldwomanwithdroppedgallstones(case1).NumerousgallstoneswereseenonnoncontrastCTbefore laparoscopiccholecystectomy(a:arrow).Anirregular-shapedsoft-tissuemasscontainingpunctatecalcificationswas observedintherightMorrison’spouchonnoncontrastCT(b:arrow).Themassinvadedintotheliverparenchymaand abdominalwall.Theotherirregular-shapedsoft-tissuemasswithnodularcalcificationwasseenintherightparacolic gutteronnoncontrastCT(c:arrow).Thenodularcalcification(c:arrow)wassimilartothegallstonesonCTbefore laparoscopiccholecystectomy(a:arrow).ThetraceraccumulatedintherightMorrison’spouchlesion(SUVmax;9.3)(d: arrow)andrightparacolicgutterlesion(SUVmax;8.0)(e:arrow)120minutesafterintravenousadministrationofthetracer on18F-fluorodeoxyglucosepositronemissiontomographywithCTimages.SUVmax;maximumstandarduptakevalue
cholecystitis associated with high-grade inflammation [2]. Dropped gallstones, also known as spilled gallstones, dur-ingcholecystectomyisaninevitablecomplicationinpatients withcalculouscholecystitisduetoabrittlegallbladder.In ad-dition,itischallengingtoretrievegallstonesintheabdominal cavity.Mostcaseswithdroppedgallstonesareasymptomatic; however,onceabscessesorgranulomasdevelop,patients suf-ferfromgeneralfatigue,fever,pain,andweightloss.The imag-ingfindingsmaymimicotherperitoneallesions,suchas tu-berculosis,actinomycosis,peritonealloosebody,andprimary andsecondaryperitonealtumor[3].Therefore,thecorrect di-agnosisisrequiredforappropriatemanagement.Wereport 4 cases offoreign-body granulomas and abscesses caused bydroppedgallstones,anddemonstratethevariousimaging findingsandclinicalcourse.
Case
presentation
Case1
A67-year-old woman underwent laparoscopic cholecystec-tomybecause ofbiliarycolic causedbygallstones (Fig. 1a). Becauseofthepatient’sperforatedgallbladder,thegallstones droppedintotheperitonealcavityduringlaparoscopic
chole-cystectomy, and they were retrieved as much as possible. Shepresentedwithpersistentlow-gradefever8months af-terlaparoscopiccholecystectomy.Computedtomography(CT) images revealed anirregular-shaped soft-tissuemass with invasive growth into the liver parenchyma and abdominal wallthatcontainedpunctateandnodularcalcificationinthe rightMorrison’spouchandrightparacolicgutter,respectively (Figs.1bandc).18F-Fluorodeoxyglucosepositronemission
to-mographywithCT(FDG-PET/CT)revealedhighFDGuptakein thesoft-tissuemasses(Figs.1dande).OnCT,theappearance ofcalcificationinthesoft-tissuemassintherightparacolic gutter(Fig.1c)wassimilartothatofthegallstonesona pre-viouspreoperativeCT(Fig.1a),whichsuggestedforeign-body granulomascausedbydroppedgallstonesduringthe previ-ouslaparoscopiccholecystectomy.Pathologicalspecimen ex-amination obtainedby percutaneous biopsy confirmed the foreign-body granuloma associated with fragments of pig-ment gallstonesand chronicsuppurative inflammation.No bacteriaweredetectedbytissueculture.Thepatient under-wentantimicrobialtreatment,andfollow-upCTat5months revealedaslightenlargementoftherightMorrison’spouch lesionandadecreaseinthesizeoftherightparacolic gut-terlesion.Biochemicalexamination3yearsaftersurgery re-vealedprogressionoftheinflammatorycondition,and percu-taneousdrainagewasperformed.Sincethen,thepatienthas beenasymptomatic.
1482
R a d i o l o g y C a s e R e p o r t s 1 5 ( 2 0 2 0 ) 1 4 8 0 – 1 4 8 4Fig.2– A60-year-oldwomanwithdroppedgallstones(case 2).Thecalcifiedgallstonewasseenintheinflamed
gallbladderonnoncontrastCT(a:arrow).Thecalcified stonewasmovedtotherightsubphrenicspaceon noncontrastCT4daysafterthesurgery(b:arrow).Newly developedenhancedsofttissuearoundthecalcifiedstone oncontrast-enhancedCTat3monthsafterthesurgery (c:arrow).Thelesiondevelopedintoanabscesson contrast-enhancedCT1yearafterthesurgery(d:arrow).
Case2
A60-year-oldwomanpresentedwithfeverandright abdom-inal pain and wasdiagnosed withnecrotizing cholecystitis based onCT findings (Fig. 2a).She underwent open chole-cystectomy,afterwhich perforatedgallbladder and abscess spreadaroundthegallbladderwereobserved.Fourdaysafter surgery,CTrevealedacalcifiedstoneintherightsubphrenic space,whichwassimilartothegallstoneneartheperforated gallbladder(Fig.2b).However,sincedischarge,thepatienthas experiencedno symptoms,and noabnormalfindings have beendetectedonbloodtests.Afollow-upCT3monthsafter surgeryshowedanewlydevelopedenhancingsoft-tissue le-sionaroundthe calcifiedstone thatwasinvadingthe right diaphragm and liver parenchyma (Fig. 2c). A diagnosis of foreign-bodygranulomacausedbyadroppedgallstonewas madebasedontheshapeofthecentralcalcifiedstone,which resembled the gallstone observed on the preoperative CT (Fig.2a).Thepatientwasseenwithoutanyspecifictreatment; however,rightabdominalpainappearedsevenmonthsafter surgery.Althoughhersymptomsimprovedusingantibiotics, theyrecurredaftercessationofantibiotictreatment.Oneyear aftersurgery,anabscessinthe rightsubphrenicspacewas foundon CT(Fig.2d),and opensurgical drainagewas per-formed.Bacteroidesfragiliswasdetectedinthedrainagefluid byaculturetest.
Case3
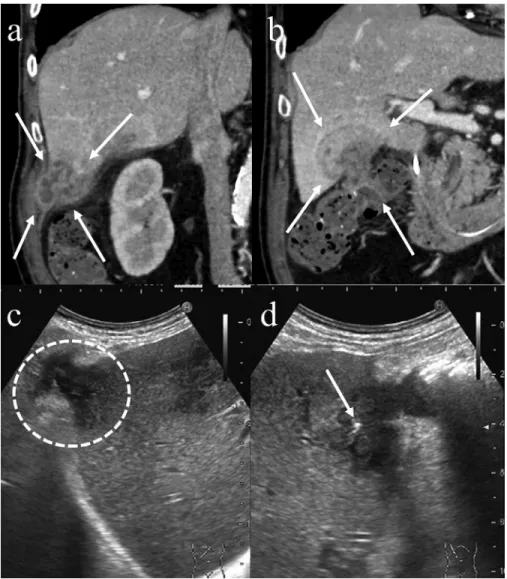
A78-year-oldmanpresentedwithappetitelossandright up-perquadrantpain5monthsafterlaparoscopic cholecystec-tomy for calculous cholecystitis. Contrast-enhancedCT
re-vealed2irregular-shapedlesionswithmultilocularfluid col-lectionandthickseptationintherightMorrisonpouchand gallbladderfossainvadingtheliver,abdominalwall,andcolon (Figs.3aand b).Nocalcificationwasdetected insidethe le-sions on noncontrast CT. Ultrasound (US) examination re-vealeda hyperechoiclesion,which suggestedgallstones in theselesions within the gallbladder fossa (Figs.3c and d). Colonoscopydemonstrated no tumor inthe colon. An ab-scesscausedbythedroppedgallstoneswasdiagnosed clin-icallybasedonCTandUSfindings.Percutaneousbiopsywas performed,andgranulomawithabscessformationwas iden-tifiedon thehistopathologic examination.Thepatientwas treatedwithantibiotics,andclinicalsymptomsand inflam-matoryfindingsimproved.
Case4
A67-year-old woman underwent laparoscopic cholecystec-tomyforcalculouscholecystitiscausedbygallstones(Fig.4a). Duringthesurgery,gallstonesdroppedintotheperitoneal cav-ityasaresultofgallbladderwallperforation.Becausethe pa-tienthadnosymptomsorabnormalfindingsinablood ex-amination,shewasobservedwithouttherapy.CTobtained3 monthsaftersurgerydemonstratedasoft-tissuelesionwith calcificationadjacent totherightrectusabdominalmuscle, possiblyintheportsiteofthelaparoscopy(Fig.4b).The calci-ficationwithinthelesionresembledgallstonespresentedon thepreoperativeCT(Fig.4a);therefore,adiagnosisof foreign-bodygranulomacausedbydroppedgallstoneswasmade.CT obtained6monthsaftersurgeryrevealedthatoneofthe calci-fiedfocihaddisappeared,andthesizeofthesurroundingsoft tissuehaddecreased(Fig.4c).Thepatientcurrentlypresents withnosymptomsandisstillunderobservation.
Discussion
Gallbladderperforationanddroppedgallstonesduring chole-cystectomyhavebeenreportedtooccurin6%-40%andin 1%-20%ofcases,respectively[4–8].Droppedgallstonesmaycause furthercomplications,includinggranulomasand abscesses in20% ofcaseswithdroppedgallstonesand in0.08%-2.9% ofalllaparoscopiccholecystectomycases[5,6,8].Theretrieval ofdroppedgallstonesaftergallbladderperforationisdifficult, particularlyduringlaparoscopicsurgery,becausethe opera-tivefieldviewislimited.Patientsmaydevelopvarious non-specificsymptoms,suchasfever,pain,andweightloss,with adurationofmonthsoryearsaftercholecystectomy,withone casedevelopingcomplications10yearsaftersurgery[9–11].
Granulomas and abscesses from dropped gallstones are thoughttodevelopasaresultofmechanicalpressurecaused bythestones,reactiontoforeignbodies,stimulationofbile, andinfectionofbacterialspeciespresentinthegallstone.The typeofgallstonecanalsoinfluencedevelopment;in partic-ular,pigmentgallstones present ahigher riskthan choles-terolstonesbecausetheformeroftencontainbacterial micro-colonies[12].Alargersize(>1.5cm)andnumber(>15stones) ofdroppedgallstonesandolderpatientagearealsorisk fac-tors[4,8,13].Antibiotictreatmentandpercutaneousdrainage
Fig.3– A78-year-oldmanwithdroppedgallstones(case3).Twoirregular-shapedmasseswithmultilocularfluidcollection andthickseptationthatinvadedtheliver,abdominalwall,andcolonwereseenintherightMorrison’spouch(a:arrow)and thegallbladderfossaoncontrast-enhancedCT(b:arrows).ThehypoechoicmassintherightMorrison’spouchinvadedboth theliverparenchymaandabdominalwallonUS(c:circle).Thehypoechoicmassinthegallbladderfossainvadedtheliver parenchymaandrevealedahyperechoiclesiononUS(d:arrow).
Fig.4– A67-year-oldwomanwithdroppedgallstones(case4).Severalgallstoneswereseeninthedistendedgallbladder withathickenedwallonnoncontrastCT(a:arrows).Themasscontaining2calcifiedfoci,whichinvadedthesurrounding softtissue,wasobservednexttotherightrectusabdominalmuscleonnoncontrastCTatthreemonthsafterthesurgery(b: arrow).Themassdecreasedinsize,andoneofthecalcificationsdisappearedonnoncontrastCT6monthsafterthesurgery (c:arrow).
1484
R a d i o l o g y C a s e R e p o r t s 1 5 ( 2 0 2 0 ) 1 4 8 0 – 1 4 8 4are oftenselected asthe initial steps for management. In caseswithprotractedinflammationassociatedwithresidual stones,opensurgerymayberequiredtocompletelyremove the droppedgallstones and preventrecurrence.Fistula for-mationisknowntobeanunusualcomplicationofdropped gallstones[3].Gallstonesmaymigratethroughafistulatothe extra-abdominalcavity,suchasthegastrointestinaltract, di-aphragm,andabdominalwall.Thegallstonemayberemoved naturallythrough afistula(asinoneofourcurrent cases), with the dropped gallstone found in the abdominal wall (case4).
Inimagingstudies,granulomasandabscessesrelatedto droppedgallstonesaretypicallyseenasasoft-tissuemassand fluidcollectionthatsometimesinfiltrateintothesurrounding structures.Differentialdiagnosismayincludeperitonealloose body,primary and secondary peritoneal neoplasms, malig-nantlymphoma,andsarcomaforgranulomatypeandsimple abscess,actinomycosis,tuberculosis,andnecrotizingtumors forabscesstype[3].However,ahistoryofcholecystectomyand theidentificationofdroppedgallstones withinthe granulo-masorabscessesonimagingarecrucialfordiagnosisthe eti-ology.Inthiscaseseries,theuseofCTenabledtheclear visu-alizationofthegranulomasorabscessesinall4cases,and cal-cifiedfocicorrespondingtodroppedgallstoneswereidentified ashigh-densitystructuresin3of4cases.Thereasonforthisis thatcholesterolgallstonesorlow-calciumgallstonesare iso-denseonCT [14].However,USsuccessfullyrevealed a gall-stoneincase3.Thus,USexaminationisvaluablefordetecting stonesthatfailtobeidentifiedonCTsoessentialforthe diag-nosisofdroppedgallstones[15].Inthecurrentcaseseries,the lesionswerefoundintherightcolicgutter(case1),Morison’s pouch(case1and3),rightsubphrenicspace(case2), gallblad-derfossa(case3),andabdominalwall(case4).Accordingtoa previousreport,gallstonesoftendropintherightsubphrenic space,Morison’spouch,gallbladderfossa,and pelviccavity. However,unusuallocations,suchastheretroperitoneum, gas-tricwall,rightthorax,abdominalwall,andtheincisionaland trocarsites,havebeendescribed[11,16].Calcifiedfociinthe massorfluidcollectiononCTandUSisessentialfor diagnos-ingthisetiology,especiallyinanunusualsite.
18F-FDG-PET/CTdemonstratedhighFDGuptakeinthe
le-sion inonecase, presumablyrepresenting the presenceof high-gradeactiveinflammationormalignanttumors(case1).
18F-FDG-PETalsodemonstratedavariousdegreeofFDG
up-take in foreign-body granulomas caused by dropped gall-stones [17]. Thus, 18F-FDG-PET studies may have limited
valueindifferentiatinggranulomasandabscessesrelatedto droppedgallstonesfromothermalignanttumors.
Conclusion
Wehavereportedcasesofforeign-bodygranulomaswithand without abscesses caused by droppedgallstones. Gallblad-derperforationanddroppedgallstonesarepossible compli-cationsofcholecystectomy.Inpatientswhohaveundergone cholecystectomy in whom an irregular soft-tissue mass or fluidcollectioninfiltratingthesurroundingtissueisdetected onimaging,foreign-bodygranulomasorabscessescausedby
droppedgallstonesshouldbeconsidered.Theidentificationof droppedgallstoneswithinthelesionisessentialfor differen-tiatingthisconditionfromothermimickingdiseases.
R E F E R E N C E S
[1]FriedmanGD.Naturalhistoryofasymptomaticand symptomaticgallstones.AmJSurg1993;165(4):399–404.
[2]KhalidM, RashidM.Gallstoneabscess:adelayed complicationofspilledgallstoneafterlaparoscopic cholecystectomy.EmergRadiol2009;16(3):227–9.
[3]NayakL, MeniasCO, GayerG.Droppedgallstones:spectrum ofimagingfindings,complicationsanddiagnosticpitfalls.Br JRadiol2013;86(1028):20120588.
[4]ZehetnerJ, ShamiyehA, WayandW.Lostgallstonesin laparoscopiccholecystectomy:allpossiblecomplications. AmJSurg2007;193(1):73–8.
[5]SchäferM, SuterC, KlaiberC, WehrliH, FreiE, KrähenbühlL. Spilledgallstonesafterlaparoscopiccholecystectomy.A relevantproblem?Aretrospectiveanalysisof10,174 laparoscopiccholecystectomies.SurgEndosc 1998;12(4):305–9.
[6]MemonMA, DeeikRK, Maffi TR, FitzgibbonsRJ.Theoutcome ofunretrievedgallstonesintheperitonealcavityduring laparoscopiccholecystectomy.Aprospectiveanalysis.Surg Endosc1999;13(9):848–57.
[7]RammohanA, SrinivasanUP, JeswanthS, RavichandranP. Inflammatorypseudotumoursecondarytospilled intra-abdominalgallstones.IntJSurgCaseRep 2012;3(7):305–7.
[8]WoodfieldJC, RodgersM, WindsorJA.Peritonealgallstones followinglaparoscopiccholecystectomy:incidence, complications,andmanagement.SurgEndosc 2004;18(8):1200–7.
[9]MorrinMM, KruskalJB, HochmanMG, SaldingerPF, KaneRA. Radiologicfeaturesofcomplicationsarisingfromdropped gallstonesinlaparoscopiccholecystectomypatients.AJRAm JRoentgenol2000;174(5):1441–5.
[10]SinghK, WangML, OforiE, WidmannW, AlemiA, NakaskaM.Gallstoneabscessasaresultofdropped gallstonesduringlaparoscopiccholecystectomy.IntJSurg CaseRep2012;3(12):611–13.
[11]BartelsAK, MuraliAR, ZamoraJG.Subhepaticsterileabscess 10yearsafterlaparoscopiccholecystectomy.ACGCaseRepJ 2015;2(2):113–15.
[12]StewartL, SmithAL, PellegriniCA, MotsonRW, WayLW. Pigmentgallstonesformasacompositeofbacterial microcoloniesandpigmentsolids.AnnSurg 1987;206(3):242–50.
[13]BrockmannJG, KocherT, SenningerNJ, SchürmannGM. Complicationsduetogallstoneslostduringlaparoscopic cholecystectomy.SurgEndosc2002;16(8):1226–32.
[14]SinghAK, LevensonRB, GervaisDA, HahnPF, KandarpaK, MuellerPR.Droppedgallstonesandsurgicalclipsafter cholecystectomy:CTassessment.JComputAssistTomogr 2007;31(5):758–62.
[15]VieraFT, ArmelliniE, RosaL, RavettaV, AlessianiM, DionigiP, etal. Abdominalspilledstones:ultrasound findings.AbdomImaging2006;31(5):564–7.
[16]HortonM, FlorenceMG.Unusualabscesspatternsfollowing droppedgallstonesduringlaparoscopiccholecystectomy. AmJSurg1998;175(5):375–9.
[17]GorospeLuis.Intraperitonealspilledgallstonespresentingas feverofunknownoriginafterlaparoscopiccholecystectomy: FDGPET/CTFindings.ClinNuclMed2012;37(8):819–20.