中村記念病院 脳神経外科・脳卒中センター(受稿日 2019. 1. 26)(脱稿日 2019. 5. 29)〔連絡先:〒 060-8570 北海道札幌市中央区南 1 条西 14 丁目 中村記念病院 脳神経外科・脳卒中センター 進藤孝一郎〕[Address correspondence: Koichiro SHINDO, M.D., Department of Neu-rosurgery and Stroke Center, Nakamura Memorial Hospital, South-1, West-14, Chuo-ku, Sapporo, Hokkaido 060-8570, Japan]
脳卒中の外科 49: 111 〜 118,2021
原 著
頚動脈血行再建術後の過灌流現象予測における
CT perfusion の有用性
進藤孝一郎,上山 憲司,荻野 達也,福田 衛
京納 正法,渕﨑 智紀,杉尾 啓徳,村橋 威夫
遠藤 英樹,渡部 寿一,大里 俊明,中村 博彦
Prediction of the Cerebral Hyperperfusion Phenomenon after
Carotid Endarterectomy or Carotid Stenting by Computed
Tomography Perfusion Imaging
Koichiro SHINDO, M.D., Kenji KAMIYAMA, M.D., Tatsuya OGINO, M.D., Mamoru FUKUDA, M.D., Masanori KYONOU, M.D., Tomoki FUCHIZAKI, M.D., Hironori SUGIO, M.D.,
Takeo MURAHASHI, M.D., Hideki ENDO, M.D., Toshiichi WATANABE, M.D., Toshiaki OOSATO, M.D., and Hirohiko NAKAMURA, M.D.
Department of Neurosurgery and Stroke Center, Nakamura Memorial Hospital, Sapporo, Hokkaido, Japan
Summary: Introduction: Single-photon emission computed tomography (SPECT) with acetazolamide challenge is useful in the prediction and assessment of post-carotid endarterectomy (CEA) or carotid stenting (CAS) cerebral hyperperfusion (CHP). However, serious adverse reactions to acetazolamide have been reported to date.
Purpose: The purpose of this study was to predict the CHP using computed tomography perfusion im-aging (CTP).
Methods: SPECT with acetazolamide challenge and CTP, as a preoperative study, were used in 116 pa-tients undergoing CEA or CAS from August 2015 to August 2018. Twenty-one papa-tients were deter-mined to be at risk of CHP by SPECT with acetazolamide challenge. After co-registration of the CTP and SPECT images, we assessed the relationship between the CTP parameters and SPECT findings in 21 patients regarded as having a high risk of CHP. CTP maps were assessed for cerebral blood flow (CBF), cerebral blood volume (CBV), mean transit time (MTT), time-to-peak (TTP), time-to-start (TTS), and time-to-drain (TTD).
Results: Increased CBV and delayed TTD and TTP were observed in all the 21 patients. Six of the 21 patients had a CHP. In these six patients, delayed MTT and delayed TTS were observed. The delay in MTT and TTS was strongly correlated with postoperative CHP (p < 0.05).
Conclusion: Preoperative CTP may be useful for the prediction of cerebral hyperperfusion.
Key words:
・ computed tomography perfusion imaging ・ hyperperfusion ・ carotid endarterectomy ・ carotid artery stenting Surg Cereb Stroke (Jpn) 49: 111-118, 2021
は じ め に
過灌流症候群(cerebral hyperperfusion syndrome:CHS) は,頚動脈高度狭窄に対する血行再建術の合併症として注 意すべき病態である.CHS の予測因子としては,術後の 高血圧や術直後から持続する過灌流現象(cerebral hyper-perfusion phenomenon:CHP)などが知られているが,術 前の画像診断における確立した危険因子は single photon emission computed tomography(SPECT)によるアセタゾ ラミド反応性の低下のみである12).そのカットオフ値は報 告によりさまざまであるが 10-20%といわれている2)4).一 方で,アセタゾラミドによる急性心不全や肺水腫などの重 大な副作用の報告があり,2015 年 4 月に日本脳卒中学 会,脳神経外科学会,日本神経学会および日本核医学会合 同委員会より「アセタゾラミド(ダイアモックス注射用)適 性使用指針」が作成・発表され,本検査は必要不可欠と考 えられる症例にかぎり使用すべきとされている.
当院では carotid endarterectomy(CEA)や carotid ar-tery stenting(CAS)の術前に plaque 診断のため computed tomography angiography(CTA)をルーチンで撮影してい る.CTA と同時に撮影している computed tomography perfusion imaging(CTP)とアセタゾラミド負荷 SPECT 検 査を比較し,CTP を用いた過灌流リスクの評価が可能か を明らかにし,アセタゾラミド負荷による検査件数を削減 できるかを検討する.
対象と方法
2015 年 8 月から 2018 年 8 月までの期間に当院で施行し た慢性期 CEA 85 例,CAS 55 例のうち,手術前に SPECT 検査と CTP を施行していた CEA 78 例,CAS 38 例を対象 とした.当院では SPECT 検査で cerebral vascular reserve (CVR)≦10%または/かつ安静時血流の対非患側 80%以下 であったものは CHP 発生のリスクが高いものとし,術後 鎮静を継続としている.術後鎮静を継続した場合は,手術 翌日に SPECT 検査を行い,CHP がなければ鎮静を解除 し,CHP を認めた場合は,2 日目以降の SPECT 検査や MRI(arterial spin labeling perfusion)検査の所見を参考に 鎮静解除のタイミングを症例ごとに判断している. 当院における CTP のワークフローは,以下の通りである. CT 装置は,128 スライス Siemens「SOMATOM Definition AS+」を使用しており,造影剤自動注入器を用いて 5 ml/s で造影剤 40 ml を急速静注し,生食 20 ml で後押ししてい る.解析は「syngo CT Workspace」に搭載された syngo VPCT Neuro により行われており,解析パラメータとし て cerebral blood flow(CBF),cerebral blood volume (CBV), mean transit time(MTT),time to peak(TTP),
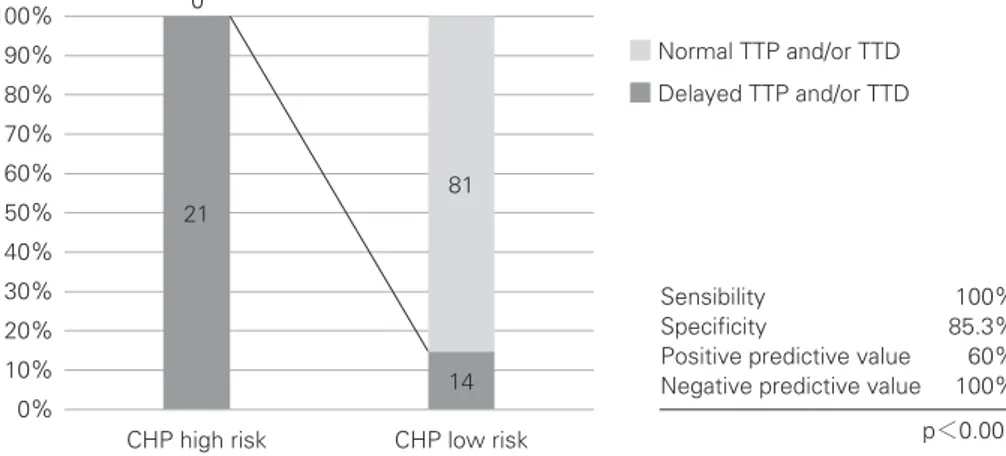
time to start(TTS),time to drain(TTD)が得られる.得 られた解析パラメータからカラーマップを作成し,定性的 評価を行っている. 術 前 の SPECT 検 査 所 見 と CTP の 解 析 パ ラ メ ー タ (CBV,MTT,TTP,TTS,TTD)を比較し,その関係を 評価した.CHP は,覚醒下では術後同側中大脳動脈領域 の安静時血流の 100%以上の上昇と定義し,鎮静下では対 側の中大脳動脈領域の安静時血流の 1.3 倍以上の上昇が前 者と相関があるとの報告があることから5),同基準を採用 した.同基準を採用した際に,1.3 倍以上の上昇がない場 合でも,鎮静解除後に過灌流症候群を呈した症例を経験し たため,対側比 1.0-1.29 倍のものに関しては高灌流現象 (high-perfusion phenomenon:HPP)と定義し,検討項目 に加えた.関心領域(region of interest:ROI)は,基底核 レベルと放線冠レベルの 2 スライスの中大脳動脈領域に設 定した.CTP における CBV 上昇や MTT・TTP・TTS・ TTD の延長は,カラーマップにおいて患側中大脳動脈の 分水嶺を除く皮質領域で,その存在が観察されたものを陽 性とした.CHP 発生のリスクが高い症例に対して,手術 翌日に123I-IMP-SPECT 検査を行い,術後 CHP の有無の 確認を行った.連続変数は平均値±標準偏差,その他は百 分率で示し,2 群間検定は Fisher 正確確率検定を用いた. 結 果 1.患者背景 SPECT 検査で CHP 発生リスクが高いと判断した症例 は 21 例(CEA 17 例,CAS 4 例)であった(Table 1).一方, CHP リスクが高くないと判断された症例は 95 例(CEA 61 例,CAS 34 例)であった.CHP 高リスクと判断した 21 例 の平均年齢は 75.9±4.7 歳,男女比は男性 19 例,女性 2 例 であった.症候性 17 例,無症候性 4 例で,NASCET 狭窄 率の平均は 89.5%で,術前のプラーク診断では 18 例で vulnerable plaque(MRI black-blood 法でプラーク信号強度 が胸鎖乳突筋比≧1.5 倍)と判断していた.21 例中 17 例で 術後鎮静を継続した(Table 2). 2.対象症例における術前 CTP 所見の検討 SPECT 検査で CHP 発生リスクが高いと判断した症例 は 21 例であり,21/21 例(100%)で TTP と TTD の延長, CBV の上昇を認めた.6/21 例で CHP を呈していたが, この 6 例すべてで TTS かつ MTT の延長を認めた(p= 0.023).CHP の criteria にはいたらなかったが HPP を認 めたものも 8 例あり,7/8 例で TTS の延長を認め,5/8 例で MTT の延長を認めた.術前に CHP 発生リスクが高 くないと判断された 95 例では,TTP・TTD の延長は 14 例でみられ,TTP・TTD の CHP 発生リスクが高い例を
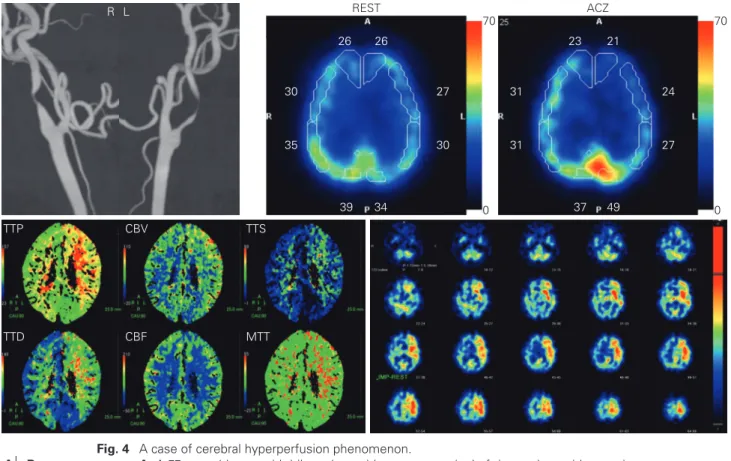
検出する感度 100%,特異度 85.3%,陽性予測率 60%,陰 性予測率 100%であった(Fig. 1).CHP 発生リスクが高く ないと判断した 95 例では,TTS および MTT の延長が 1 例あり,術後に HPP を認めた. 術後 CHP や HPP がみられた領域は TTS 延長や MTT 延長が確認された領域に一致しており,延長がみられな かった領域では認めなかった. 症 例 提 示 〈症例 1〉 82 歳,男性(Fig. 2). 症候性の右頚動脈狭窄症(NASCET 79%狭窄)で,CEA を 施 行 し, 術 後 CHP・HPP は 認 め な か っ た. 術 前 の SPECT 検査では,安静時血流が施設基準の 80%以上, CVR は 10%未満であり,SEE-JET Stage 1 と判断され た.CTP では TTP・TTD 延長,CBV 上昇を認めたもの の,TTS・MTT の延長は分水嶺に留まっていた.術後 HPP・CHP は認めなかった. 〈症例 2〉 78 歳,男性(Fig. 3). 両 側 の 頚 動 脈 狭 窄 症 で, 症 候 性 の 右 頚 動 脈 狭 窄 症 (NASCET 95%狭窄)に対して CEA を施行した.術前の SPECT 検査では,安静時血流が施設基準の 80%以上で SEE-JET Stage 1 と判断されていたが,CVR は 0%未満 で盗血現象を呈していた.CTP では TTP・TTD 延長, CBV 上昇を認め,TTS が皮質領域まで明瞭に延長してい た.MTT の延長は認めなかった.術後 HPP(鎮静下,対 側比 1.24)を認めており,HPP を呈していた領域は,TTS が延長している領域に含まれていた. 〈症例 3〉 77 歳,男性(Fig. 4). 両 側 の 頚 動 脈 狭 窄 症 で, 症 候 性 の 左 頚 動 脈 狭 窄 症 (NASCET 95%狭窄)に対して CEA を施行した.術前の SPECT 検査では,安静時血流が施設基準の 80%未満で, CVR は 10%未満であったため SEE-JET Stage 2 と判断さ れた.CTP では TTP・TTD 延長,CBV 上昇を認め,TTS が皮質領域まで明瞭に延長していた.皮質領域の CBF の 低下があり,MTT の延長も認めた.術後 CHP(鎮静下, Fig. 1 Relationship between CHP risk and TTP/TTD.
CHP: cerebral hyperperfusion phenomenon, TTP: time to peak, TTD: time to drain
Sensibility 100% Specificity 85.3% Positive predictive value 60% Negative predictive value 100% p<0.001 ■Delayed TTP and/or TTD ■Normal TTP and/or TTD 14 81 21 0
CHP high risk CHP low risk 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0%
Table 1 Distribution of the number of high-risk
cere-bral hyperperfusion cases in each surgical procedure
CEA (n=78) CAS (n=38) CHP high risk 17 4 CHP low risk 61 34 CHP: cerebral hyperperfusion phenomenon, CEA: ca-rotid endarterectomy, CAS: caca-rotid artery stenting
Table 2 Characteristics of all patients determined as a high-risk
ce-rebral hyperperfusion case
CHP high risk n=21 Age 75.9±4.7 Gender (male) 19 NASCET stenosis (%) 89.5±7.6 Postoperative sedation 17 Side (Right) 12 Symptomatic 17 Vulnerable plaque 18 CHP: cerebral hyperperfusion phenomenon, NASCET: North Ameri-can Symptomatic Carotid Endarterectomy trial
対側比 1.50)を認めており,CHP を呈していた領域は, TTS・MTT が延長している領域に含まれていた.
考 察
アセタゾラミド負荷 SPECT では,CVR が 10-30%か, 10 % 以 下 で も CBF が 正 常 範 囲 内 に あ る 場 合,Powers Stage10) 1 に相当するといわれており,JET study では同基
準が採用された3).cerebral perfusion pressure(CPP)の低
下に対するオートレギュレーションが破綻すると,脳梗塞 にいたるため,Powers Stage 2 は血行再建術のターゲッ トとなる.一方で,血行再建後の過灌流は Powers Stage 1 でも Stage 2 でも起こり得るとされている7). 頚動脈狭窄症に対する血行再建術において約 0.2-18.9% で CHS を認めると報告12)されており,術前の画像診断に おける確立した危険因子は SPECT 検査によるアセタゾラ ミド反応性の低下のみである12). また,CVR による過灌流予測率は,安静時脳血流測定 のみの場合と比べて精度が高いとされ,これは安静時脳血 流測定のみの場合は matched perfusion 例も含まれている ためと考えられている9). 一方で,アセタゾラミド負荷脳血流 SPECT 検査後の約 63%でなんらかの副作用が起きていると報告されてお り11),「アセタゾラミド(ダイアモックス注射用)適性使用 指針」に定められたように必要な症例にかぎり行うべきと Fig. 2 A case of non-cerebral hyperperfusion phenomenon.
A: An 82-year-old man with symptomatic right internal carotid artery stenosis (NASCET
79% stenosis).
B: Moderate hypoperfusion is observed in the preoperative resting SPECT, and cerebral
vascular reserve is less than 10%.
C: CTP shows an increase in the right TTP, TTD, and CBV increase, but no obvious
in-crease in right MTT and TTS.
D: Post-operative SPECT shows a non-cerebral hyperperfusion phenomenon.
NASCET: North American Symptomatic Carotid Endarterectomy trial, SPECT: single-photon emission computed tomography, CTP: computed tomography perfusion imag-ing, CBF: cerebral blood flow, CBV: cerebral blood volume, MMT: mean transit time, TTP: time-to-peak, TTS: time-to-start, TTD: time-to-drain
MTT CBF TTD TTS CBV TTP 43 41 41 64 65 67 58 52 ACZ 34 38 39 45 46 47 46 41 REST 90 0 90 0 R A B C D
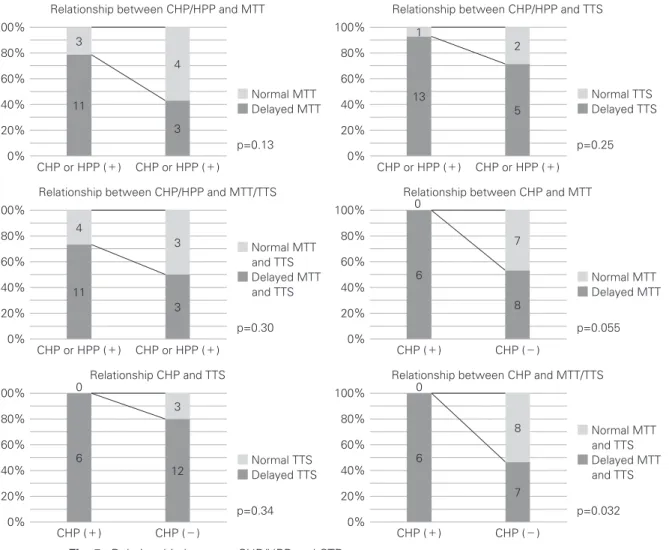
考えられる. これまで CHP は術前のアセタゾラミド反応性低下症例 の 40-60%で発生するとされている2)8)が,今回の CTP で の検討では TTS または/かつ MTT の延長を認めた症例 (19/21 例)では,CHP が 31.6%(6/19 例),CHP または HPP が 73.7%(14/19 例)で認められた.TTS と MTT の 両方が延長している症例については有意に CHP の発生率 が高い(p=0.032)ことも明らかになった(Fig. 5). 血行力学的重症度と CTP の比較では,Stage 1-2 で認 める CBV の上昇は CTP では伝達関数から定量的に算出 されるが,Stage 2 でみられる CVR の高度低下や oxygen extraction fraction(OEF)上昇は CTP では測定できない. し か し,CVR は MTT と 逆 相 関 に あ り6),OEF は MTT と相関関係にあると報告1)されており,MTT が Stage 2 の検出に貢献できる可能性があると考えられる. Siemens の解析ソフトでは独自のパラメータである TTD・TTS も 得 る こ と が で き る.TTS は bolus arrival time(BAT)とも呼ばれる造影剤の到達遅延時間で,入力 動脈から組織ボクセルへ造影剤が到達するまでの時間であ る.TTD は TTS+MTT で表現される概念で,造影剤が 入力動脈から組織ボクセルを通過後,静脈に排泄され始め る時間を表している.これらは非生理的なパラメータであ るが,虚血を鋭敏に捉えることができるとされている. 今回の検討から,TTP や TTD は CPP の低下を鋭敏に 捉えられるパラメータと考えられ,TTS は脳血管床の拡 張能の限界を迎え,CVR の高度低下や OEF の高度上昇を Fig. 3 High-perfusion phenomenon case.
A: A 78-year-old man with bilateral carotid artery stenosis. Right internal carotid artery is
symptomatic (NASCET 95% stenosis).
B: Moderate hypoperfusion is observed in the preoperative resting SPECT, and cerebral
vascular reserve is less than 0% (steal phenomenon is observed).
C: CTP shows an increase in the right TTP, TTD, CBV, and TTS, but no increase in MTT.
High-perfusion area is included in the area of the TTS increase.
D: Post-operative SPECT shows a high-perfusion phenomenon.
NASCET: North American Symptomatic Carotid Endarterectomy trial, SPECT: single-photon emission computed tomography, CTP: computed tomography perfusion imag-ing, CBF: cerebral blood flow, CBV: cerebral blood volume, MMT: mean transit time, TTP: time-to-peak, TTS: time-to-start, TTD: time-to-drain
MTT CBF TTD TTS CBV TTP 27 26 34 56 64 54 44 41 ACZ 32 39 42 46 54 46 40 41 REST 80 0 80 0 L R A B C D
きたし,CBF が低下し始める病態を鋭敏に捉えられるパ ラメータと考えられた. 今回,CHP 高リスク症例のスクリーニング検査として の CTP の有効性を検討した.TTP や TTD の延長がない 症例では,術後 CHP を呈した症例がなかったことから, TTP や TTD の延長のあるもののみにアセタゾラミド負 荷脳血流検査を行うことで,その検査件数を 1/3(35/116 例)程度に減らすことができるものと考えられた.TTP や TTD は OEF の上昇し始めを鋭敏に捉えることができる パラメータと考えられた.また,術後過灌流の予測におい て CVR<12%がカットオフ値2)とされているが,TTP・ TTD はこの病態を検出し得る有用なパラメータと考えら れ,盗血現象をきたし得る高度に CVR が低下した病態で は TTS の延長が目立つようになり,安静時 CBF が 80% 以下となる Stage 2 に相当する病態では MTT の延長が目 立つようになるものと考えられた. また,最近では time to maximum(Tmax)を灌流異常域 に用いることが増えてきており,急性期脳梗塞の虚血コア の検出に利用されている.当院の CT 装置では評価できな いが,Tmax は deconvolusion 法による残留関数のピーク までの時間であり,TTS を含み MTT の影響を受ける指 標であることから,TTS と MTT と同様に術後 CHP のリ スク評価に利用できる可能性があるものと考える. CBF や CBV,MTT は伝達関数から得られる定量パラ メータではあるが,カラーマップを作成し評価する場合は 視覚的(定性的)評価となってしまう.左右の大脳半球での 差を比較した際は,虚血の程度が同等である場合は過小評 価となってしまうおそれがある点に留意が必要である. Fig. 4 A case of cerebral hyperperfusion phenomenon.
A: A 77-year-old man with bilateral carotid artery stenosis. Left internal carotid artery is
symptomatic (NASCET 95% stenosis).
B: Severe hypoperfusion is observed in the preoperative resting SPECT, and cerebral
vascular reserve is less than 0% (steal phenomenon is observed).
C: CTP shows an increase in the left TTP, TTD, CBV, TTS, and MTT. Cerebral
hyperperfu-sion area is included in the area of the TTS and MTT increase.
D: Post-operative SPECT shows cerebral hyperperfusion phenomenon.
NASCET: North American Symptomatic Carotid Endarterectomy trial, SPECT: single-photon emission computed tomography, CTP: computed tomography perfusion imag-ing, CBF: cerebral blood flow, CBV: cerebral blood volume, MMT: mean transit time, TTP: time-to-peak, TTS: time-to-start, TTD: time-to-bedrain
MTT CBF TTD TTS CBV TTP 23 31 31 37 49 27 24 21 ACZ 70 0 70 0 26 30 35 39 34 30 27 26 REST L R A B C D
TTP は造影剤の注入速度や心拍出量など体循環の影響を 受けやすく,絶対値を患者間で比較することができないパ ラメータであるため,相対値で評価する必要がある. TTD は TTS と MTT を足したパラメータであるが,陳旧 性の脳梗塞は TTD が延長した領域と判断されるため,術 前に広範な脳梗塞を認める場合は,過大評価となるため CT 検査や MRI 検査などの他のモダリティで脳梗塞の範 囲を確認する必要がある. CTP は,deconvolusion 法の違いにより若干のパラメー タ解析結果に違いが生じ7),評価者により若干の差異を生 じる可能性のある検査ではあるが,アセタゾラミド負荷を 行う前のスクリーニング検査として有用と考えられた. 結 語 TTP・TTD の延長,CBV の上昇を認める症例の中に術 後過灌流・高灌流現象を呈し得る症例が含まれており,そ の中でも TTS や MTT の延長を認めた場合は術後過灌 流・高灌流現象の高リスク症例と評価し得るものと考えら れた. 現時点では術後過灌流予測における golden standard は アセタゾラミド負荷による脳血流検査であり,必要な症例 においては行うべき検査と考えるが,TTP・TTD の延 長,CBV の上昇を認める症例に絞りアセタゾラミド負荷 による脳血流検査を行うことで,アセタゾラミドの使用頻 度を減じることが可能と考えられた. 本論文の要旨は,脳卒中の外科学会(2018 年,福岡)で 発表した. 著者全員は日本脳神経外科学会への COI 自己申告を完 了しています.本論文の発表に関して開示すべき COI は ありません.
Fig. 5 Relationship between CHP/HPP and CTP parameters.
CHP: cerebral hyperperfusion phenomenon, HPP: high-perfusion phenomenon, CTP: computed tomography angiography, MTT: mean transit time, TTS: time-to-start
7 8 6 0 12 3 6 0 8 7 6 0 3 3 11 4 5 2 13 1 p=0.13 ■Normal MTT ■Delayed MTT 3 4 11 3 CHP or HPP (+) CHP or HPP (+) 100% 80% 60% 40% 20% 0%
Relationship between CHP/HPP and MTT
p=0.25 ■Normal TTS ■Delayed TTS CHP or HPP (+) CHP or HPP (+) 100% 80% 60% 40% 20% 0%
Relationship between CHP/HPP and TTS
p=0.30 ■Normal MTT and TTS ■Delayed MTT and TTS CHP or HPP (+) CHP or HPP (+) 100% 80% 60% 40% 20% 0%
Relationship between CHP/HPP and MTT/TTS
p=0.055 ■Normal MTT ■Delayed MTT CHP (+) CHP (−) 100% 80% 60% 40% 20% 0%
Relationship between CHP and MTT
p=0.34 ■Normal TTS ■Delayed TTS CHP (+) CHP (−) 100% 80% 60% 40% 20% 0% Relationship CHP and TTS p=0.032 ■Normal MTT and TTS ■Delayed MTT and TTS CHP (+) CHP (−) 100% 80% 60% 40% 20% 0%
文 献
1) Carrera E, Jones PS, Iglesias S, et al: The vascular mean tran-sit time: a surrogate for the penumbra flow threshold? J Cereb Blood Metab 31: 1027-1035, 2011
2) Hosoda K, Kawaguchi T, Shibata Y, et al: Cerebral vasoreac-tivity and internal carotid artery flow help to identify pa-tients at risk for hyperperfusion after carotid endarterecto-my. Stroke 32: 1567-73, 2001
3) JET Study Group: Japanese EC-IC Bypass Trial(JET Study):中間解析結果(第二報).脳卒中の外科 30: 434-437, 2002
4) Kaku Y, Yoshimura S, Kokuzawa J: Factors predictive of ce-rebral hyperperfusion after carotid angioplasty and stent placement. AJNR Am J Neuroradial 25: 1403-1408, 2004 5) Kawamata T, Okada Y, Kawashima A, et al: Postcarotid
end-arterectomy cerebral hyperperfusion can be prevented by minimizing intraoperative cerebral ischemia and strict post-operative blood pressure control under continuous sedation. Neurosurgery 64: 447-453, 2009
6) Kim E, Sohn CH, Na DG, et al: Perfusion computed tomogra-phy evaluation of cerebral hemodynamic impartment in patients with unilateral chronic steno-occlusive disease: a comparison with the acetazolamide challenge 99mTc-hexamethylpropyleneamine oxime single-photon emission computed tomography. J Comput Assist Tomogr 33: 546-551,
2009
7) 木下俊文:脳の perfusion CT.臨床画像 32: 502-512, 2016 8) Ogasawara K, Yukawa H, Kobayashi M, et al: Prediction and
monitoring of cerebral hyperperfusion after carotid endarter-ectomy by using single-photon emission computerized to-mography scanning. J Neurosurg 99: 504-510, 2003
9) Oshida S, Ogasawara K, Saura H, et al: Does preoperative measurement of cerebral blood flow with acetazolamide chal-lenge in addition to preoperative measurement of cerebral blood flow at the resting state increase the predictive accu-racy of development of cerebral hyperperfusion after carotid endarterectomy? Results from 500 cases with brain perfusion single-photon emission computed tomography study. Neurol Med Chir(Tokyo) 55: 141-148, 2015
10) Powers WJ, Press GA, Grubb RL Jr, et al: The effect of dynamically significant carotid artery disease on the hemo-dynamic status of the cerebral circulation. Ann Intern Med 106: 27-34, 1987
11) Saito H, Ogasawara K, Ogawa A, et al: Adverse effects of in-travenous acetazolamide administration for evaluation of cerebrovascular reactivity using brain perfusion single-photon emission computed tomography in patients with major cerebral artery steno-occlusive disease. Neurol Med Chir(Tokyo) 51: 479-483, 2011
12) van Mook WN, Rennenberg RJ, Schurink GW, et al: Cerebral hyperperfusion syndrome. Lancet Neurol 4: 877-888, 2005