1
Differences in lesion characteristics and patient background associated with the medium-term clinical outcomes of bare-metal and first-, second- and third- generation drug-eluting stents
Masayuki Nakamura 1 , Amane Ike 1* , Yuta Kato 1 , Makito Futami 1 , Takashi Kuwano 1 , Makoto Sugihara 1 , Atsushi Iwata 1 , Akira Kawamura 1 , Yasunori Suematsu 1 , Shin- ichiro Miura 1,2*
1 Department of Cardiology, Fukuoka University School of Medicine, Fukuoka 814-0180, Japan, and 2 Department of Cardiology, Fukuoka University Nishijin Hospital, Fukuoka 814- 8522, Japan
Short title: Outcomes with bare-metal and drug-eluting stents
Disclosures: The authors declare that there are no conflicts of interest.
IRB information: Fukuoka University Hospital EC/IRB:10-1-08(09-105)
*Co-corresponding authors:
Amane Ike, MD, PhD and Shin-ichiro Miura, MD, PhD, Professor and Chairman, Fukuoka University School of Medicine, 7-45-1 Nanakuma, Jonan-ku, Fukuoka 814-0180, Japan.
Telephone: +81-92-801-1011 Fax: +81-92-865-2692
E-mail: [email protected] (A.I.) and [email protected] (S.M.)
2 Abstract
We investigated the lesion characteristics and patient background factors associated with the medium-term incidence of major adverse cardiac events (MACEs) for bare-metal stents (BMS) and 1 st -, 2 nd - and 3 rd -generation drug-eluting stents (DES) using the PCI-Registry (FU-Registry). Between January 2003 and March 2016, 2967 cases/ 3508 lesions for which percutaneous coronary intervention was performed at Fukuoka University Hospital and related facilities were enrolled. Patients were divided into BMS and 1 st -, 2 nd - and 3 rd - generation drug-eluting stent (DES) groups. The incidence of MACEs in the BMS group (26.2%) was significantly higher than those in the 1 st -, 2 nd - and 3 rd -DES groups (18.0%, 12.5%, and 11.0%, respectively). The incidence of MACEs in the BMS group was strongly associated with insulin use, hemodialysis, low high-density lipoprotein cholesterol, stent minimum lesion diameter, stent length, severe calcification and a small vessel diameter of less than 2.5 mm. Some of these factors showed no association with MACEs among the drug- elution groups, and only hemodialysis, arteriosclerosis obliterans and severe calcification showed a strong correlation in the 2 nd -DES group. In the 3 rd -DES group, none of the factors considered were associated with MACEs. In conclusion, in stent implantation, the number of factors associated with MACEs has gradually decreased as the stent generation increased.
Keywords: major adverse cardiac events; bare-metal stent; drug-eluting stent; percutaneous
coronary intervention.
3 Introduction
Since the advent of coronary stents used in percutaneous coronary intervention (PCI), this technology has been repeatedly improved and many issues have been overcome. The development of the first-generation drug-eluting stent (1 st -DES) markedly decreased the incidence of in-stent restenosis (ISR). However, 1 st -DES increased the rate of very late stent thrombosis (1). To solve this problem, a second-generation drug-eluting stent (2 nd -DES) was developed. Although 2 nd -DES is safer than 1 st -DES, there are still some issues, such as ISR and stent thrombosis. Bioabsorbable polymers that disappear with drug elution were
introduced in third-generation DES (3 rd -DES) (2, 3). However, many reports have stated that 2 nd -DES and 3 rd -DES have similar clinical outcomes (4, 5). In fact, no strong clinical impacts were noted in the RESERCH (6) tests, which compared BMS and 1 st -DES. ISR is
unavoidable regardless of which stent is placed in cases where it is impossible to secure a large inner diameter in the coronary vessel due to high calcification or small vessel diameter.
In terms of in-stent neointimal proliferation, it has been proven that stent late lumen loss with BMS remains in the range 0.7-1.0 mm regardless of the stent size and target vessel diameter (7, 8). In the SPIRIT II (9), III (10) and EXAMINATION trials (11), stent late lumen loss was around 0.1-0.4 mm with 1 st -DES (12, 13), and around 0.2 mm with 2 nd -DES. In a direct comparison, 3 rd -DES gave slightly better results than 2 nd -DES (4).
Stent late lumen loss was minimal with 1 st -DES, and tended to increase in further
generations. The neointimal inhibitory effect reflected in stent late lumen loss and the stent
structure of polymers differs significantly between BMS and each DES generation. This
difference may be a cause of the difference in the factors related to clinical outcomes and
relevance.
4
Thus, many studies have been conducted on the therapeutic results and factors related to MACE after stent implantation. However, few reports have clarified which issues have been overcome and which factors remain as issues in the course of the history of the improvement and development of various stents. This understanding is important for the future evolution of PCI. Therefore, we investigated the lesion characteristics and patient background factors associated with the medium-term clinical outcome for each stent generation using the PCI- Registry (FU-Registry) at Fukuoka University.
Methods
Study Design
Between January 2003 and March 2016, 2967 cases/3508 lesions for which PCI was performed at Fukuoka University Hospital, Fukuoka University Chikushi Hospital and Fukuoka Hakujuji Hospital were enrolled (Figure 1). The targets were 2587 cases/3081 lesions, from which 420 lesions/353 cases without stent placement and 7 cases/7 lesions for which medium-term clinical follow-up was impossible due to unknown whereabouts were excluded. The 2587 cases/3081 lesions were divided into four groups according to stent generation: BMS, 1 st -DES (Cypher® sirolimus-eluting stents and TAXUS® paclitaxel- eluting stents), 2 nd -DES (durable polymers with high biocompatibility)
(Xience®/PROMUS® everolimus-eluting and Resolute® zotarolimus-eluting stents), and 3 rd - DES (bioabsorbable polymers) (SYNERGY™, Ultimaster™ sirolimus-eluting stents and Orsiro™). The data used for this analysis did not include NOBORI® or BIOFREEDOM®.
The primary endpoint was the occurrence of major adverse cardiac events [MACEs, all-cause
death, myocardial infarction (MI), and target lesion revascularization (TLR)]. MI was defined
as symptoms that included both ST-T elevation MI and non-ST-T elevation MI, and showed
5
either a clear ischemic ECG change or an elevation of cardiogenic enzymes (positive simple troponin T, CK greater than twice the reference value, and CK-MB exceeding the upper limit of the reference value). Follow-up CAG was supposed to be performed on all lesions 6-9 months after PCI. However, it was actually performed on only 2582 of 3081 lesions (83.8%) due to rejection by the patient, high age, death, deterioration of renal function, etc. The average follow-up period was 279.2 ± 249.9 days (median: 212.0 days) at the time of MACE assessment. For patients who were unable to undergo follow-up CAG, clinical outcomes were investigated through outpatient consultation and telephone contact. Also, based on the
definition reported by the ARC (Academic Research Consortium), all cases of Definite, Probable, and Possible were included in stent thrombosis. We performed data analysis using the database from the FU-Registry (UMIN000005679). This study was conducted in
accordance with the Declaration of Helsinki and approved by the Independent Review Board (IRB) of Fukuoka University Hospital [Fukuoka University Hospital EC/IRB:10-1-08(09- 105)].
PCI and intravascular ultrasound (IVUS) procedures
PCI was performed on patients with chest symptoms with 50% or greater stenosis on
angiogram, or with evidence of ischemia obtained through noninvasive testing and fractional
flow reserve. In addition, TLR was performed in patients with ISR who had chest symptoms,
evidence of ischemia, and/or 90% or more coronary restenosis as assessed by angiogram,
despite a lack of evidence of ischemia. The endpoint of the procedure was set to the point
where there was no dissection that caused blood flow disorder, TIMI III flow was available,
and the degree of angiographic stenosis was 10% or less. Although IVUS was performed for
over 70% of procedures, in many cases measurements were made after ballooning or rotation
coronary atherectomy. Moreover, IVUS is not generally applied without revascularization
6
when follow-up CAG is performed. Thus, IVUS data were not used for the analysis in this study.
Medication (antiplatelets)
Administration of aspirin (81 mg/day), ticlopidine (200 mg/day) or clopidogrel (75 mg/day), and prasugrel (5 mg/day) was started at least 48 hours before stent insertion in all cases. In an emergency PCI, aspirin (162 mg/day), clopidogrel (300 mg/day), and prasugrel (20 mg/day) were provided orally before the procedure if the patient had not taken antiplatelets. In this study, DAPT was discontinued in accordance with various guidelines including the Guidelines for the Treatment of Non-ST Elevation Acute Coronary Syndrome (revised in 2012) and the Guidelines for the Treatment of ST-segment Elevation Acute Myocardial Infarction (revised in 2013).
Quantitative Coronary Angiography (QCA)
QCA was performed before the procedure in all cases. Follow-up CAG was performed in
83.8%. Follow-up QCA was possible in 70.7% (2178 of the total 3081 lesions). Follow-up
QCA could not be performed in cases where follow-up CAG was performed at another
hospital, and thus only MACE could be investigated. Quantitative and qualitative analyses
were performed at Fukuoka University, which is a core laboratory, using CMS-GFT and Q-
Angio (MEDES, The Netherlands), and pre-procedural, post-procedural, and follow-up
angiograms were analyzed respectively. All measurements were made on angiograms after
nitroglycerin injection. The segments were defined as in-stent, proximal edge, and 5 mm
from the distal edge of the stent. Late lumen loss was defined as the difference between the
minimum lesion diameters (MLD) on the post-procedural angiogram and the follow-up
7
angiogram. ISR at the time of follow-up was defined as the presence of 50% or greater percent diameter stenosis (%DS) with QCA.
Statistical analysis
Statistical analysis was performed at Fukuoka University using SAS software (Version 9.1 SAS Institute, Cary, NC, USA). For comparisons of categorical variables between groups, the chi-square test was used. Comparisons of continuous variables between groups were made with the Wilcoxon rank-sum test and the Student t-test, and the results are shown as the mean
±standard deviation. P-values of less than 0.05 (p<0.05) were considered statistically significant. In multi-group comparisons, the chi-square test was used for comparisons of categorical variables, and the analysis of variance (ANOVA) was used for evaluations of continuous variables. Continuous variables that showed significant differences by ANOVA were subjected to Scheffe's method. Categorical variables that showed a significant
difference by the chi-square test were subjected to another chi-square test for intergroup analysis. A multiple logistic regression analysis was used for multivariate analysis.
Results
The number of cases and lesions for each stent are shown in Figure 1. As shown in Figure 2A, the incidence of MACEs in BMS (26.2%) was significantly higher than those in 1 st -DES, 2 nd -DES and 3 rd -DES (18.0%, 12.5% and 11.0%, respectively) (Table 1). The incidences of MACEs in 2 nd -DES and 3 rd -DES were comparable (Figure 2A, Table 1).
BMS, 1 st -DES, 2 nd -DES, and 3 rd -DES were further divided into two groups based on the presence or absence of MACEs, and factors related to the clinical outcomes were analyzed.
With an increase in the generation, the number of factors that were significantly different
8
between the presence and absence of MACEs decreased (Table 1). In the BMS group, the values of ultrasonic echocardiography-left ventricular ejection fraction (UCG-LVEF) and high-density lipoprotein cholesterol (HDL-C) in MACEs(+) were significantly lower than those in MACEs(-). The frequencies of prior MI, diabetes mellitus (DM), arteriosclerosis obliterans (ASO), and hemodialysis (HD) in MACEs(+) were significantly higher than those in MACEs(-) (Table 1). As for medications at the time of PCI, the rate of insulin use was significantly higher in MACEs(+).
In 1 st -DES, there was a higher percentage of males in MACEs(+) compared to MACEs(-), and significantly lower values for UCG-LVEF and HDL-C. As for medical history and complications, prior MI, prior coronary artery bypass grafting (CABG), DM, and HD were significantly more frequent in MACEs(+). The rate of insulin use was significantly higher in MACEs(+) (Table 1).
In 2 nd -DES, UCG-LVEF and HDL-C were significantly lower in MACEs(-), and the rates of ASO, DM and HD in MACEs(-) were significantly higher than those in MACEs(+). The rate of insulin use in MACEs(+) was significantly higher than that in MACEs(-), as with BMS and 1 st -DES (Table 1). In 3 rd -DES, there were no significant differences between MACEs(-) and MACEs(+). In the BMS group, there was no difference in the incidence of acute coronary syndrome (ACS) between MACEs(-) and MACEs(+) (Table 1).
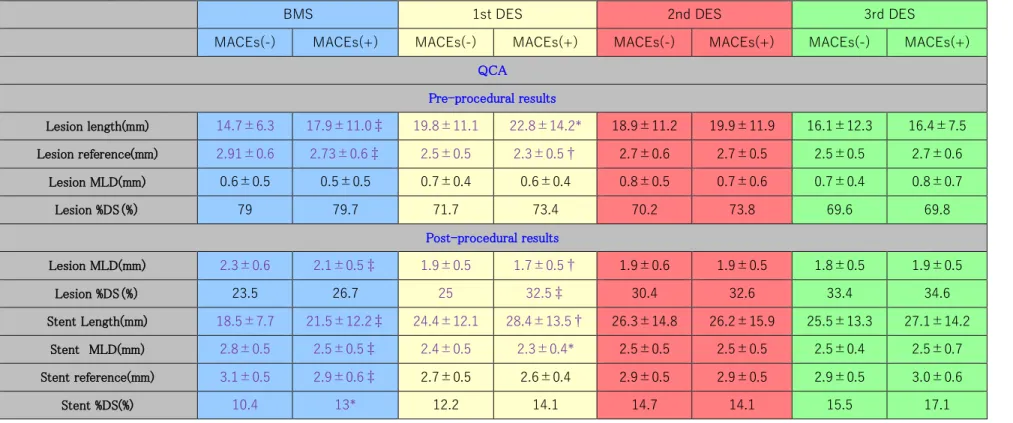
As the stent generation increased, the number of lesion characteristics that showed significant differences decreased (Tables 1 and 2). In BMS, the rates of American Heart Association/American College of Cardiology (AHA/ACC) type B2+C and severe calcification were significantly different between MACEs(-) and MACEs(+) (Table 1).
Among QCA pre-procedural results, longer lesion length and smaller lesion reference were
found in MACEs (+). Among QCA post-procedural results, lesion MLD, stent MLD, and
9
stent reference were significantly smaller and stent length was longer in the MACEs(+) group (Table 2).
In 1 st -DES, the rates of type B2+C and severe calcification were again significantly higher in MACEs(+) (Table 1). As in BMS, among QCA pre-procedural results, longer lesion length and smaller lesion reference were found in MACEs(+). Among QCA post-procedural results, lesion MLD and stent MLD were significantly smaller and stent length was longer in
MACEs(+). In contrast to the BMS group, there was no difference in stent reference diameter (Table 2).
In 2 nd -DES, the rates of type B2+C and severe calcifications were significantly higher in MACEs(+), as with BMS and 1 st -DES (Table 1). There were no significant differences among QCA pre- or post-procedural results between MACEs (-) and MACEs (+) (Table 2).
The lesion characteristics in 3 rd -DES were similar to those in 2 nd -DES (Tables 1 and 2).
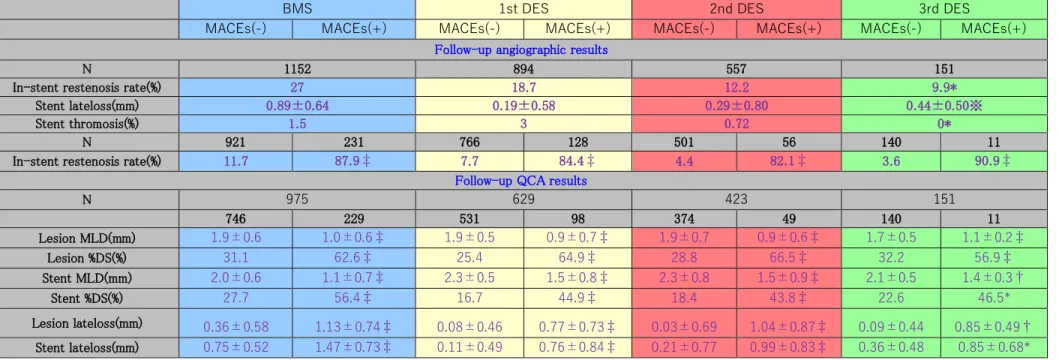
Regarding QCA follow-up results, the rate of ISR in BMS (27.0%) was significantly higher than those in 1 st -DES, 2 nd -DES, and 3 rd -DES (18.7%, 12.2%, and 9.9%, respectively) (Figure 2B). The incidence of ISR in 2 nd -DES was comparable to that in 3 rd -DES.
Stent late lumen loss in BMS and 1 st -, 2 nd - and 3 rd -DES was 0.89±0.64 mm, 0.19±0.58 mm, 0.29±0.80 mm and 0.44±0.50 mm, respectively. In all four groups, the loss in MACEs(-) was significantly lower than that in MACEs(+) (Table 3).
The incidences of MACEs in BMS were 20.6% for all-cause death, 17.5% for MI and 63.9% for TLR-PCI. Those in 1 st -DES were 12.9% for death, 19.4% for MI and 79.1% for TLR-PCI. Those in 2 nd -DES further decreased to 23.6% for death, 8.3% for MI and 55.6%
for TLR-PCI. Finally, the incidences of MACEs in 3 rd -DES were 16.7% for death and 83.3%
for TLR-PCI (Table 4).
A multi-group analysis of stent late lumen loss for each stent generation showed significant
differences between BMS and 1 st -, 2 nd - and 3 rd -DES, and between 1 st -DES and 3 rd -DES
10
(Figure 2C). BMS had the greatest late lumen loss, and 1 st -DES had the smallest. The stent late lumen loss increased as the generation of DES increased. Stent thrombosis was 1.5% in BMS, 3.0% in 1 st -DES, 0.72% in 2 nd -DES, and 0% in 3 rd -DES. 1 st -DES showed the highest incidence of stent thrombosis in the multi-group comparison (Figure 2D).
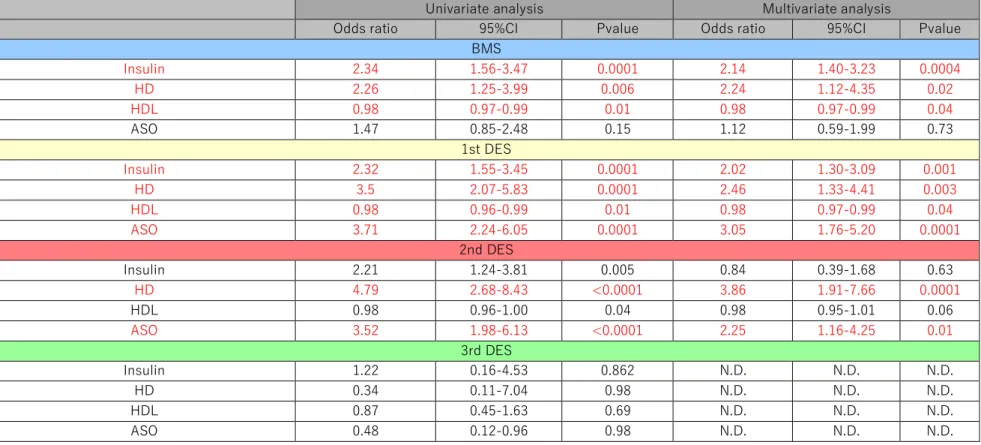
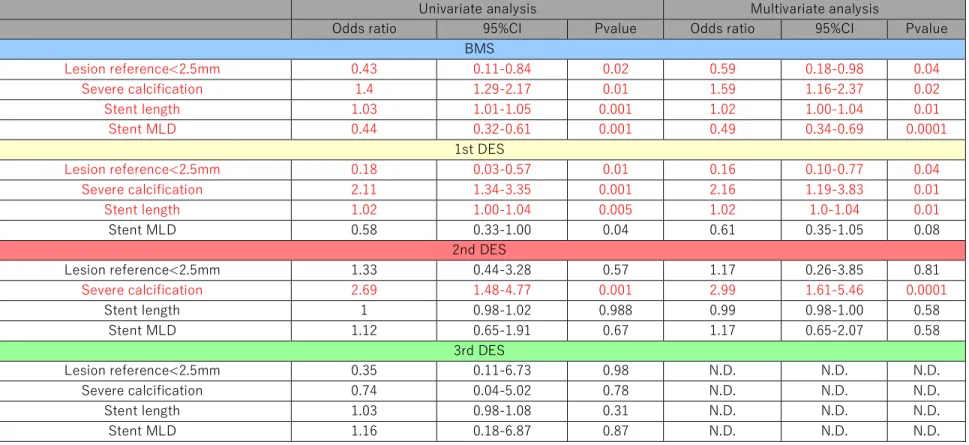
Univariate and multivariate analyses were performed to evaluate the differences in the type and relevance of factors related to the occurrence of MACEs in each generation, from BMS to 3 rd -DES (Tables 5 and 6). Insulin use, HD, HDL-C, and ASO were selected as patient background factors, and lesion reference<2.5 mm, severe calcification, stent length and stent MLD were selected as lesion characteristics, since these factors showed significant
differences among the four generations. Since the number of patients in MACE(+) for 3 rd - DES was small, only a univariate analysis was performed.
In BMS, insulin use, HD and HDL-C, but not ASO, were significantly associated with MACEs by both univariate and multivariate analyses (Table 5). As for the lesion
characteristics in BMS, all of the factors examined showed strong correlations with MACEs by a univariate analysis (Table 6). By the multivariate analysis, stent MLD, stent length, severe calcification and small blood vessel diameter with lesion reference<2.5 mm were all strongly associated with MACEs (Table 6).
In 1st DES, all of the patient background factors were significantly associated with
MACEs by a univariate analysis. MACEs were associated with HD, HDL-C, insulin use and ASO by a multivariate analysis (Table 5). Regarding lesion characteristics in 1 st -DES, while significant associations were observed for all factors by a univariate analysis, the multivariate analysis did not show an association between stent ML and MACEs. On the other hand, lesion reference<2.5 mm was still significantly associated with MACEs (Table 6).
In 2 nd -DES, all of the factors examined were associated with MACEs by a univariate
analysis. However, by a multivariate analysis, while HD and ASO showed strong correlations
11
with MACEs, no associations were observed for insulin use or HDL-C (Table 5). In the analysis of lesion characteristics, the presence of small blood vessels with lesion
reference<2.5 mm and stent length were not associated with MACEs in the univariate analysis, while only severe calcification was significantly associated with MACEs by a multivariate analysis (Table 6).
Although only a univariate analysis was performed in 3 rd -DES, no association with MACEs was observed for any of the patient background factors or lesion characteristics (Tables 5 and 6).
Discussion
Various coronary risks related to MACEs accompany PCI. However, these risks have been reduced by advances in stent devices. In the evaluation of mid-term clinical outcomes, BMS had the highest incidence of MACEs (26.6%) and 3 rd -DES had the lowest (11.0%) (Figure 2A). The incidence of MACEs in 3 rd -DES was similar to that in 2 nd -DES (12.5%). This result is considered to be a reasonable clinical outcome based on the inclusion of many cases at high risk of MACEs, such as those with HD, DM, complex lesions, and development of TLRs.
Bioabsorbable polymers are generally used in 3 rd -DES, and the stent struts are designed to
be thinner for quicker coating by endothelial cells. Such differences in stent structure were
expected to bring improvements, such as a reduction of stent thrombosis and shortening of
the DAPT period. However, many reports have shown identical mid-term clinical outcomes
between 2 nd -DES and 3 rd -DES, as observed in this study (4, 5). A possible explanation for
this result is that the stent struts of 2 nd -DES are 89-81µm, which is much thinner than those of
1 st -DES (132-140µm) and comparable to those of 3 rd -DES (60-81µm). Since the polymers in
12
2 nd -DES were already highly biocompatible, there may be no difference in medium-term results compared to those with third-generation bioabsorbable polymers, which are absorbed in 3-4 months. However, late catch-up remains an issue with 2 nd -DES. Since this is
considered to be due to neoatherosclerosis, this symptom should be suppressed. Nakazawa et al. reported that neoatherosclerosis was observed 4 to 5 years after BMS implantation, whereas it appeared about 3 months after DES implantation (14). Likewise, in 2 nd -DES, TLR is required in around 2% of cases per year (15), to reach around 20% in 10 years. Although the long-term results with 3 rd -DES have not been confirmed, we are eager to see whether late catch-up can be suppressed or not. In any case, evaluations and reviews of the long-term follow-up results are indispensable.
MACEs are the most important mid-term clinical outcomes after PCI, and many of these are TLRs caused by ISR. The QCA measurement value that is most relevant to ISR is stent late lumen loss. In this study, the incidence of ISR was BMS>1 st -DES>2 nd -DES=3 rd -DES (Figure 2B), while the incidence of stent late lumen loss was BMS>3 rd -DES=2 nd -DES>1 st - DES. Apparent significant differences were observed between BMS and 1 st -DES, 2 nd -DES, and 3 rd -DES, and between 1 st -DES and 3 rd -DES (Figure 2C). Despite having the lowest incidence of stent late lumen loss, 1 st -DES had the second-highest incidence of ISR.
Conversely, despite having the second-highest incidence of stent late lumen loss, 3 rd -DES had the lowest incidence of ISR. However, Asano et al. (16) reported that late lumen loss ≤0.5 mm cannot be a predictor of TLR. The stent late lumen loss values in BMS and 1 st -, 2 nd -, and 3 rd -DES were 0.89±0.64 mm, 0.19±0.58 mm, 0.29±0.80 mm and 0.44±0.50 mm,
respectively. For all of the DES, the values were ≤0.5 mm. The levels of stent late lumen loss
will not cause TLR in 2 nd - or 3 rd -DES, which reflects a good coating of the stent struts and is
considered to be the result of a favorable healing process as a result of the improvement in
polymers and fewer drugs. With this good coating of stent struts, the overall incidence of
13
stent thrombosis in the present study was higher than those in other studies due to the inclusion of all Definite/Probable/Possible as defined by ARC. However, the incidences of stent thrombosis in BMS, 2 nd -DES, and 3 rd -DES were significantly lower than that in 1 st - DES. Similar results have been reported by Kim et al. (17), who stated that very late stent thrombosis was caused by the delayed reendothelialization of the stent surface, incomplete endothelialization, and the influence of inflammation on stent polymers (18). Although the exact mechanism is still unknown, this clearly shows improvements with stent advances, leading to a shift toward short-term DAPT.
The ideal stent may be the one that is not influenced by the patient background or lesion
characteristics. A multivariate analysis indicated that some issues are being resolved with
advances in stent design. DM (19), HD (20), dyslipidemia (21) and ASO (22) have been
reported as risk factors for MACEs after PCI. Our FU-Registry has also reported the effect of
DM, especially insulin (23). In terms of lesion characteristics, small vessel diameter, severe
calcification, stent (lesion) length, and complex lesions (Type B2+C) are often reported as
important risk factors for post-PCI MACEs (24). In this study, a multivariate analysis was
performed to analyze significant differences between MACEs(+) and MACEs(-) in the four
stent generations. In BMS, many factors showed strong correlations with MACEs (Tables 5
and 6). However, with an increase in the generation, the factors associated with MACEs
decreased. In 2 nd -DES, while HD and ASO were still strongly correlated with MACEs,
insulin use and HDL-C were not associated with MACEs (Table 5). As for the lesion
characteristics, lesion factors that were strongly associated with MACEs in BMS and 1 st -
DES, such as small vessel diameter (lesion reference<2.5 mm) and stent length, were not
associated with MACEs in 2 nd -DES (24). Although a multivariate analysis could not be
performed due to the low number of patients in MACEs (+) in 3 rd -DES, none of the factors
examined were associated with MACEs in the univariate analysis. 3 rd -DES represents an
14
improvement over 2 nd -DES. As described above, the clinical outcomes for 2 nd -DES and 3 rd - DES are less susceptible to the patient background and lesion characteristics than those for BMS and 1 st -DES, as indicated in several studies, including SPIRIT III (10), XAMI (25), and RESET (26). Among all of the lesion factors, small vessel diameter has been deemed to be a strong predictor of angiographic restenosis based on the belief that the restenosis risk
increases by 60% for every 0.50 mm decrease in the reference vessel diameter (27).
However, since the second generation, it has often been reported that a small vessel diameter is not always a strong risk factor for the development of MACEs (28), which is consistent with the finding of this study. This may be related to the direct influence of stent thickness on restenosis, as reported in ISAR-STEREO (29) and ISAR-STEREO-2 (30) in the BMS era.
Although it has been reported that the incidence of restenosis in the case of complex lesions
increases with an increase in the thickness of stent struts (14.5 vs. 29.0%), the stent thickness
may have a greater influence on the stenting of small vessels. As mentioned above, stent
struts have become thinner from generation to generation: 132-140 µm for 1 st -DES, 89-81 µm
for 2 nd -DES, and 60-81 µm for 3 rd -DES. Bangalore et al. reported that the medium-term
clinical outcome of 3 rd -DES with a thickness of <70 µm was better than that of the thicker
2 nd -DES (31). Stent length was also deemed to be an important risk factor for MACEs
including TLR, as well as a risk factor for stent thrombosis in 1 st -DES. However, it has been
reported that even with stent lengths longer than 32 mm, no significant difference was
observed in the occurrence of MACEs when compared to shorter stent lengths (32), and no
association with MACEs or stent thrombosis was indicated in this study. On the other hand,
even with generations after 2 nd -DES, HD, ASO and severe coronary calcification are still
residual risks. While problems such as ISR and stent thrombosis have not yet been resolved,
coronary stents have been improved little by little, and the clinical outcomes are getting less
susceptible to the patient background and lesion characteristics.
15 Study Limitations
This was a retrospective registry study for patients who underwent PCI from January 2003 to March 2016 with subsequent medium-term follow-up. Regarding the 3rd-DES NTV PCI rate, the 3VD rate is also around 20%, and it may be unreasonable to consider that the rate of residual lesions was high. After all, 33.3% of MACE (+) is considered to be influenced by the fact that the number of patients in the MACE (+) group was relatively small. More detailed changes in clinical outcomes and changes in long-term clinical outcomes should be obtained by increasing the total number of 3 rd -DES cases and extending the overall follow-up period.
Medications have changed during the study period. Since the era when the stent was used varies depending on its generation, the influence of the differences in medical procedures cannot be ruled out. Also, score-based lesion evaluations such as SYNTAX scores 1 and 2 were not performed. Moreover, since 1 st -DES is not currently available on the market, direct comparisons with other generations are not possible. In this study, 2 nd -DES and 3 rd -DES were defined according to the polymer type. Biocompatible polymers were used in 2 nd -DES, and bioabsorbable polymers were used in 3 rd -DES. However, there are differences in stent design, even among devices in the same generation. Therefore, direct comparisons between stents might yield different outcomes.
Conclusions
Coronary stents have been improved little by little over time. Since the second generation, medium-term clinical outcomes have become less susceptible to patient background and lesion characteristics. As a result, it has become possible to maintain good outcomes.
However, even in 2 nd -DES, HD, ASO and severe coronary calcification are still residual risks
16
for the occurrence of MACEs. Problems such as ISR and stent thrombosis have not been entirely overcome.
Source of Funding None.
Disclosures
The authors declare that there are no conflicts of interest.
17 References
1. Finn AV, Joner M, Nakazawa G, Kolodgie F, Newell J, John MC, Gold HK, Virmani R (2007) Pathological correlates of late drug-eluting stent thrombosis: strut coverage as a marker of endothelialization. Circulation 115:2435-2441
2. Loffi M, Tousek P, Budesinsky T, Lisa L, Santangelo A, Widimsky P, Kocka V (2018) Optical coherence tomography in STEMI with bioresorbable scaffold: possible cause of coronary flow impairment? A sub-study from the Prague 19 trial. Heart Vessels 33: 1282- 1287
3. Wan Ahmad WA, Nakayoshi T, Mahmood Zuhdi AS, Ismail MD, Zainal Abidin I, Ino Y, Kubo T, Akasaka T, Fukumoto Y, Ueno T (2020) Different vascular healing process between bioabsorbable polymer-coated everolimus-eluting stents versus bioresorbable vascular scaffolds via optical coherence tomography and coronary angioscopy (the ENHANCE study: ENdothelial Healing Assessment with Novel Coronary tEchnology).
Heart Vessels 35: 463-473
4. Saito S, Valdes-Chavarri M, Richardt G, Moreno R, Iniguez Romo A, Barbato E,Carrie D, Ando K, Merkely B, Kornowski R, Eltchaninoff H, James S, Wijns W;CENTURY II Investigators (2014) A randomized, prospective, intercontinental evaluation of a bioresorbable polymer sirolimus-eluting coronary stent system: the CENTURY II (Clinical Evaluation of New Terumo Drug-Eluting Coronary Stent System in the Treatment of Patients with Coronary Artery Disease) trial. Eur Heart J 35:2021-2031
5. Iglesias JF, Heg D, Roffi M, Tüller D, Noble S, Muller O, Moarof I, Cook S, Weilenmann
D, Kaiser C, Cuculi F, Häner J, Jüni P, Windecker S, Pilgrim T (2019) Long-Term Effect
of Ultrathin-Strut Versus Thin-Strut Drug-Eluting Stents in Patients With Small Vessel
18
Coronary Artery Disease Undergoing Percutaneous Coronary Intervention: A Subgroup Analysis of the BIOSCIENCE Randomized Trial. Circ Cardiovasc Interv 12:e008024 6. Lemos PA, Serruys PW, van Domburg RT, Saia F, Arampatzis CA, Hoye A, Degertekin
M, Tanabe K, Daemen J, Liu TK, McFadden E, Sianos G, Hofma SH, Smits PC, van der Giessen WJ, de Feyter PJ (2004) Unrestricted utilization of sirolimus-eluting stents compared with conventional bare stent implantation in the “real world”: the
RapamycinEluting Stent Evaluated At Rotterdam Cardiology Hospital (RESEARCH) registry. Circulation 109: 190-195
7. Stone GW, Rizvi A, Newman W, Mastali K, Wang JC, Caputo R, Doostzadeh J, Cao S, Simonton CA, Sudhir K, Lansky AJ, Cutlip DE, Kereiakes DJ; SPIRIT IV Investigators (2010) Everolimus-eluting versus paclitaxel-eluting stents in coronary artery disease. N Engl J Med 362:1663-1674
8. Natsuaki M, Kozuma K, Morimoto T, Kadota K, Muramatsu T, Nakagawa Y, Akasaka T, Igarashi K, Tanabe K, Morino Y, Ishikawa T, Nishikawa H, Awata M, Abe M, Okada H, Takatsu Y, Ogata N, Kimura K, Urasawa K, Tarutani Y, Shiode N, Kimura T; NEXT Investigators (2013) Biodegradable polymer biolimus-eluting stent versus durable polymer everolimus-eluting stent: a randomized, controlled, noninferiority trial. J Am Coll Cardiol 62:181-190
9. Garg S, Serruys P, Onuma Y, Dorange C, Veldhof S, Miquel-Hébert K, Sudhir K,
Boland J, Huber K, Garcia E, te Riele JA; SPIRIT II Investigators (2009) 3-year clinical
follow-up of the XIENCE V everolimus-eluting coronary stent system in the treatment of
patients with de novo coronary artery lesions: the SPIRIT II trial (Clinical Evaluation of
the Xience V Everolimus Eluting Coronary Stent System in the Treatment of Patients
with de novo Native Coronary Artery Lesions). JACC Cardiovasc Interv 2:1190-1198
19
10. Stone GW, Midei M, Newman W, Sanz M, Hermiller JB, Williams J, Farhat N, Mahaffey KW, Cutlip DE, Fitzgerald PJ, Sood P, Su X, Lansky AJ; SPIRIT III
Investigators (2008) Comparison of an everolimus-eluting stent and a paclitaxel-eluting stent in patients with coronary artery disease: a randomized trial. JAMA 299:1903-1913 11. Sabate M, Cequier A, Iñiguez A, Serra A, Hernandez-Antolin R, Mainar V, Valgimigli
M, Tespili M, den Heijer P, Bethencourt A, Vazquez N, Gómez-Hospital JA, Baz JA, Martin-Yuste V, van Geuns RJ, Alfonso F, Bordes P, Tebaldi M, Masotti M, Silvestro A, Backx B, Brugaletta S, van Es GA, Serruys PW (2012) Everolimus-eluting stent versus bare-metal stent in ST-segment elevation myocardial infarction (EXAMINATION): 1 year results of a randomised controlled trial. Lancet 380:1482-1490
12. Ike A, Shirai K, Nishikawa H, Iwata A, Yahiro E, Sugihara M, Kawamura A, Uehara Y, Zhang B, Ogawa M, Mori K, Miura S, Saku K (2015) Associations between different types of hypoglycemic agents and the clinical outcome of percutaneous coronary intervention in diabetic patients-From the FU-Registry. J Cardiol 65:390-396
13. Nagata I, Ike A, Nishikawa H, Zhang B, Sugihara M, Mori K, Iwata A, Kawamura A, Shirai K, Uehara Y, Ogawa M, Miura S, Saku K (2015) Associations between lipid profiles and MACE in hemodialysis patients with percutaneous coronary intervention:
from the FU-Registry. J Cardiol 65:105-111
14. Nakazawa G, Vorpahl M, Finn AV, Narula J, Virmani R (2009) One step forward and two steps back with drug-eluting-stents: from preventing restenosis to causing late thrombosis and nouveau atherosclerosis. JACC Cardiovasc Imaging 2:625-628 15. Gada H, Kirtane AJ, Newman W, Sanz M, Hermiller JB, Mahaffey KW, Cutlip DE,
Sudhir K, Hou L, Koo K, Stone GW (2013) 5-year results of a randomized comparison
of XIENCE V everolimus-eluting and TAXUS paclitaxel-eluting stents: final results
from the SPIRIT III trial (clinical evaluation of the XIENCE V everolimus eluting
20
coronary stent system in the treatment of patients with de novo native coronary artery lesions). JACC Cardiovasc Interv 6:1263-1266
16. Asano T, Serruys PW, Collet C, Miyazaki Y, Takahashi K, Chichareon P, Katagiri Y, Modolo R, Tenekecioglu E, Morel MA, Garg S, Wykrzykowska J, Piek JJ, Sabate M, Morice MC, Chevalier B, Windecker S, Onuma Y (2018) Angiographic late lumen loss revisited: impact on long-term target lesion revascularization. Eur Heart J 39:3381-3389 17. Kim JS, Kim BK, Jang IK, Shin DH, Ko YG, Choi D, Hong MK, Cho YK, Nam CW,
Hur SH, Choi JH, Song YB, Hahn JY, Choi SH, Gwon HC, Jang Y (2012) Comparison of neointimal coverage between zotarolimus-eluting stent and everolimus-eluting stent using optical coherence tomography (COVER OCT). Am Heart J 163:601-607
18. Otsuka F, Vorpahl M, Nakano M, Foerst J, Newell JB, Sakakura K, Kutys R, Ladich E, Finn AV, Kolodgie FD, Virmani R (2014) Pathology of second-generation everolimus- eluting stents versus first-generation sirolimus- and paclitaxel-eluting stents in humans.
Circulation 129:211-23
19. Park GM, Lee SW, Park SW, Kim YH, Yun SC, Cho YR, Ahn JM, Lee JY, Kim WJ, Park DW, Kang SJ, Lee CW, Lee BK, Lee NH, Cho YH, Suh J, Shin WY, Lee SJ, Lee SW, Park WJ, Kim HS, Lee SG, Cheong SS, Her SH, Park MW, Kim CJ, Park SJ (2013) Comparison of Zotarolimus-Eluting stent versus Sirolimus-Eluting stent for de novo coronary artery disease in patients with diabetes mellitus from the ESSENCE- DIABETES II trial. Am J Cardiol 112:1565-1570
20. Otsuka Y, Ishiwata S, Inada T, Kanno H, Kyo E, Hayashi Y, Fujita H, Michishita I
(2011) Comparison of haemodialysis patients and non-haemodialysis patients with
respect to clinical characteristics and 3-year clinical outcomes after sirolimus-eluting
stent implantation: insights from the Japan multi-centre post-marketing surveillance
registry. Eur Heart J 32:829-837
21
21. Adachi H, Niwa A, Shinoda T (1995) Prevention of restenosis after coronary angioplasty with low-density lipoprotein apheresis. Artif Organs 19:1243-1247
22. Yamazaki T, Goto S, Shigematsu H, Shimada K, Uchiyama S, Nagai R, Yamada N, Matsumoto M, Origasa H, Bhatt DL, Steg PG, Ikeda Y; REACH Registry Investigators (2007) Prevalence, awareness and treatment of cardiovascular risk factors in patients at high risk of atherothrombosis in Japan. Circ J 71:995-1003
23. Ike A, Shirai K, Nishikawa H, Iwata A, Yahiro E, Sugihara M, Kawamura A, Uehara Y, Zhang B, Ogawa M, Mori K, Miura S, Saku K (2015) Associations between different types of hypoglycemic agents and the clinical outcome of percutaneous coronary intervention in diabetic patients-From the FU-Registry. J Cardiol 65:390-396
24. Moses JW, Leon MB, Popma JJ, Fitzgerald PJ, Holmes DR, O'Shaughnessy C, Caputo RP, Kereiakes DJ, Williams DO, Teirstein PS, Jaeger JL, Kuntz RE; SIRIUS
Investigators (2003) Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med 349:1315-1323
25. Hofma SH, Brouwer J, Velders MA, van't Hof AW, Smits PC, Queré M, de Vries CJ, van Boven AJ (2012) Second-generation everolimus-eluting stents versus first-
generation sirolimus-eluting stents in acute myocardial infarction. 1-year results of the randomized XAMI (XienceV Stent vs. Cypher Stent in Primary PCI for Acute
Myocardial Infarction) trial. J Am Coll Cardiol 60:381-387
26. Kimura T, Morimoto T, Natsuaki M, Shiomi H, Igarashi K, Kadota K, Tanabe K,
Morino Y, Akasaka T, Takatsu Y, Nishikawa H, Yamamoto Y, Nakagawa Y, Hayashi Y, Iwabuchi M, Umeda H, Kawai K, Okada H, Kimura K, Simonton CA, Kozuma K;
RESET Investigators (2012) Comparison of everolimus-eluting and sirolimus-eluting
coronary stents: 1-year outcomes from the Randomized Evaluation of Sirolimus-eluting
Versus Everolimus-eluting stent Trial (RESET). Circulation 126:1225-1236
22
27. Cassese S, Byrne RA, Tada T, Pinieck S, Joner M, Ibrahim T, King LA, Fusaro M, Laugwitz KL, Kastrati A (2014) Incidence and predictors of restenosis after coronary stenting in 10004 patients with surveillance angiography. Heart 100:153-159
28. Siontis GC, Piccolo R, Praz F, Valgimigli M, Räber L, Mavridis D, Jüni P, Windecker S (2016) Percutaneous Coronary Interventions for the Treatment of Stenoses in Small Coronary Arteries: A Network Meta-Analysis. JACC Cardiovasc Interv 9:1324-1234 29. Kastrati A, Mehilli J, Dirschinger J, Dotzer F, Schühlen H, Neumann FJ, Fleckenstein M,
Pfafferott C, Seyfarth M, Schömig A (2001) Intracoronary stenting and angiographic results: strut thickness effect on restenosis outcome (ISAR-STEREO) trial. Circulation 103:2816-2821
30. Pache J, Kastrati A, Mehilli J, Schühlen H, Dotzer F, Hausleiter J, Fleckenstein M, Neumann FJ, Sattelberger U, Schmitt C, Müller M, Dirschinger J, Schömig A (2003) Intracoronary stenting and angiographic results: strut thickness effect on restenosis outcome (ISAR-STEREO-2) trial. J Am Coll Cardiol 41:1283-1288
31. Bangalore S, Toklu B, Patel N, Feit F, Stone GW (2018) Newer-Generation Ultrathin Strut Drug-Eluting Stents Versus Older Second-Generation Thicker Strut Drug-Eluting Stents for Coronary Artery Disease. Circulation 138:2216-2226
32. Yano H, Horinaka S, Ishimitsu T (2018) Impact of everolimus-eluting stent length on
long-term clinical outcomes of percutaneous coronary intervention. J Cardiol 71:444-451
23 Figure legends
Figure 1.
Patient flow chart.
POBA: plain old balloon angioplasty; BMS: bare metal stent, MACEs: major adverse cardiovascular events, CAG: coronary angiography, 1 st -DES: first-generation drug-eluting stent, 2 nd -DES: second-generation drug-eluting stent, 3 rd -DES: third-generation drug-eluting stent.
Figure 2.
Comparison of the incidences of major adverse cardiovascular events (MACEs) (A), in-stent restenosis (ISR) (B), in-stent late lumen loss (C) and stent thrombosis (D) among the bare metal stent (BMS) and 1 st -, 2 nd - and 3 rd -generation drug-eluting stent groups (1 st -DES, 2 nd - DES and 3 rd -DES).
*p<0.05 by Chi-square test. ※ p<0.05 by Scheffe test.
Fu-Registry(3,081 lesions/2,587patients)
373 patients were not deployed any stent (only POBA etc).
7 patients were unable to clinical follow up because of unknown information.
BMS(1,304 lesions/1,111 patients) 1 st DES(956 lesions/772 patients) 2 nd DES(667 lesions/575 patients) 3 rd DES(154 lesions/132 patients)
MACEs(-) 1.006 lesions 820 patients
MACEs(+) 298 lesions 291 patients
MACEs(-) 809 lesions 633 patients
MACEs(+) 147 lesions 139 patients
MACEs(-) 585 lesions 503 patients
MACEs(+) 82 lesions 72 patients
MACEs(-) 142 lesions 120 patients
MACEs(+) 12 lesions 12 patients
BMS(1,152 lesions/1,111 patients) 1 st DES(894 lesions/772 patients) 2 nd DES(557 lesions/575 patients) 3 rd DES(151 lesions/132 patients) Clinical follow up rate:100%
Follow up CAG enforcement rate:83.8
rejection by patients, high age, death, deterioration of renal function, etc)
MACEs(-) 921 lesions 820 patients
MACEs(+) 231lesions 291 patients
MACEs(-) 766 lesions 633 patients
MACEs(+) 128 lesions 139 patients
MACEs(-) 501 lesions 503 patients
MACEs(+) 56 lesions 72 patients
MACEs(-) 140 lesions 120 patients
MACEs(+) 11 lesions 12 patients
Fu-Registry(3,508 lesions/2,967patients)
Pre-procedural Patient background/Lesion background data
Angio graphical/clinical follow-up data
Figure 1.
Figure2: The comparison between multiple groups
(A) MACEs incidence. (B) ISR incidence. (C) In-stent late lumen loss. (D) Stent thrombosis incidence.
(A), (B), (D) multi-group comparisons: P=0.0001. * P<0.05 by Chi-squaree test.
(C)multi-group comparisons: P=0.0001(ANOVA). ※P<0.05 by Scheffe test.
MACEs: major adverse cardiovascular events, BMS: bare metal stent, 1 st DES: first generation drug eluting stent, 2 nd DES: second generation drug eluting stent, 3 rd DES:
third generation drug eluting stent.
0 5 10 15 20 25 30
BMS 1st DES 2nd DES 3rd DES
(%)
* *
P=0.00010 5 10 15 20 25 30
BMS 1st DES 2nd DES 3rd DES
(%)
*
P=0.0001*
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9
BMS 1st DES 2nd DES 3rd DES
(mm P=0.0001(ANOVA)
0 0.5 1 1.5 2 2.5 3 3.5
BMS 1st DES 2nd DES 3rd DES
(%)