多発乳がんを合併した抗TIF1-γ抗体陽性皮膚筋炎の1例
7
0
0
全文
(2) Clin Rheumatol Rel Res, 33: 41〜47, 2021. 42. Here, we report a patient with DM with an-. trunk(Fig. 1). Her manual muscle testing. ti-TIF1-γ antibody who had multiple breast. showed very low; 2/5 of Neck flection, 4/5. cancer. Although she underwent cancer re-. (Right), 4/5(Left)of deltoid, 3/5,3/5 of bi-. section, DM activity remained and she treated. ceps, 3/5,3/5 of triceps, 3/5,3/5 of iliopsoas,. with prednisolone and Intravenous immune. 3/5, 3/5 of hamstrings. She did not have ar-. globulin therapy. After the treatment, her an-. thritis and dysphagia.. ti-TIF1-γ antibody was negative, and DM and. A blood test showed leukocyte count of. breast cancer have been sustained with no re-. 7400/μl, hemoglobin of 13.2 g/dL, platelet 16.6. lapse for 3 years.. x104/μl, erythrocyte sedimentation rate of 52 mm/hour, C-reactive protein of 1.09 mg/dL, al-. Case Presentation. anine aminotransferase of 137 U/L, aspartate. A previously healthy 71-year-old Japanese. aminotransferase of 55 U/L, lactate dehydro-. woman was admitted to the department in. genase(LDH)of 591 U/L, creatine phosphoki-. the hospital with a 2-month history of rash.. nase(CPK)of 2010 U/L, aldolase of 40.9 U/L,. She had muscle pain and muscle weakness.. and ferritin of 632.6 ng/ml, but negative test-. She did not have fever, arthralgia, dyspnea,. ing for anti-nuclear, anti-DNA, anti-RNP, an-. Raynaud phenomenon, and dysphagia. She. ti-SS-A, and anti-SS-B antibody. Her urine test. had no history of skin disease. She did not. showed no proteinuria and occult hematuria.. have a family history of malignancy and did. Her myositis specific antibody showed that. not take drugs and no allergy to drugs and. positive testing for anti-TIF1-γ antibody. food.. (MBL, Nagoya, Japan), but negative testing. On admission, the skin examination re-. for anti-aminoacyl tRNA synthetase(ARS),. vealed Heliotrope rash, Gottron’s sign of elbow. anti-Mi-2, and anti-melanoma differentiation-as-. and knee joints, and erythroderma of the. sociated gene 5 antibody(MDA-5). Her anti-. Figure 1 Cutaneous skin manifestation showed Heliotrope rash, Gottron’s sign, and erythroderma..
(3) 臨床リウマチ, 33: 41〜47, 2021. 43. Figure 2 Magnetic resonance imaging(MRI)of lower limbs showed a higher degree of signal intensity on T2-weighted images.. Figure 3 Computed tomographic(CT)scans test showed one tumor of the right breast and two tumors of the left breast.. TIF1-γ antibody titer was 99. Skin biopsy. Computed tomographic(CT)scans showed. showed lymphocyte infiltration in the dermis. no interstitial pneumonia, but triple breast tu-. with liquefaction degeneration. Magnetic reso-. mors including one tumor of the right and. nance imaging(MRI)of lower limbs shows a. two tumors of the left breast(Fig. 3). Tumor. higher degree of signal intensity on T2-weight-. markers showed CEA of 3.3 ng/mL(normal. ed images, but no sign of fasciitis(Fig. 2).. range < 5.0) , CA 15–3 of 20.6 U/mL(normal. Electromyography revealed myogenic change.. range <30), CA 125 of 12.1 U/mL(normal.
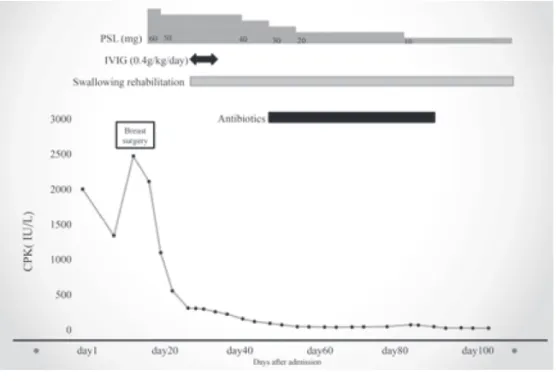
(4) Clin Rheumatol Rel Res, 33: 41〜47, 2021. 44. Figure 4 Clinical course The clinical course of a DM patient with anti-TIF1-γ antibody with triple breast cancer who was treated with immunosuppressive therapy and breast surgery. Abbreviations: CPK, creatine phosphokinase; IVIG, intravenous immunoglobulin; PSL, Prednisolone.. range <15) , and CA 19–9 of 136.4 U/mL(nor-. required tube feeding and started swallowing. mal range <37). Mammography showed a. rehabilitation on day 24. She also started In-. spiculated mass. She was referred to Breast. travenous immune globulin(IVIG) (0.4 g/kg/. Surgery. The needle biopsy showed the left. day)for 5 days combined with PSL on day. and right tumor were class V. All cancer stag-. 36. After IVIG therapy, her CPK was normal,. es were T1cN0M0(Stage1). She was diag-. however, severe dysphagia remained. She. nosed as having DM based on Peter and Bo-. started balloon dilation for severe dysphagia. han criteria4) and also diagnosed as having. on day 65. The expression of the estrogen and. the right of invasive ductal carcinoma and left. progesterone receptors and HER-2/neu pro-. breast cancers of invasive ductal carcinoma. tein of three breast cancers were all positive.. and invasive micropapillary carcinoma. The. However, she did not receive hormone thera-. clinical course is shown in figure 4. On day 16,. py due to severe dysphagia. She developed. she underwent a total mastectomy of both. chest abscess on day 42 and received antibiot-. breasts. However, her rash, CPK, and muscle. ics for 6 weeks. After the recovering chest. weakness did not improve and she started. abscess, she transferred to a different hospital. prednisolone(PSL)60mg/day on day 18. Al-. because of swallowing rehabilitation on day. though CPK decreased after the initiation of. 106. On day 227, her TIF1-γ was less than 8,. the PSL, she developed dysphagia on day 23.. which was the normal range. Her swallowing. She was referred to Otolaryngologist and. ability gradually improved and could eat food. Swallowing endoscopy showed aspiration. She. finally. Her PSL was discontinued on day 553..
(5) 臨床リウマチ, 33: 41〜47, 2021. 45. Her TIF1-γ and tumor markers have been. included psoriasis, atopic dermatitis, drug re-. still negative. Her DM and breast cancer have. actions, seborrheic dermatitis. Importantly,. been sustained with no relapse for 3 years.. erythroderma also has been considered a paraneoplastic manifestation secondary to. Discussion. cancer 10). Maruani reported a DM patient. We encountered a case of DM with an-. with erythroderma who had hepatocellular. ti-TIF1-γ antibody with triple breast cancer. carcinoma 11). Sung Woo Kim also reported. and anti-TIF1-γ antibody is from positive to. that 3 of 5 (60%) of DM patients with. negative after the immunosuppressive thera-. erythroderma had malignancy10). In our case,. py and surgical resection. Through our expe-. she had erythroderma at the onset of DM and. rience of this case, we can make two clinically. diagnosed as breast cancer concomitantly.. important observations.. This result suggested that erythroderma. Cancer is a life-threatening complication in. might be a predictive factor for cancer in pa-. patients with DM and the prevalence of can-. tients with DM. However, there have been a. cer in patients with DM was about 20% and. few reports regarding DM patients with. the pooled relative risk for patients with DM. erythroderma and more studies are required. was 5.50(4.31-6.70)compared to the general. to clarify the relationship of DM, erythroder-. population2, 5). Almost cancer-associated DM. ma, and cancer.. 6). and. To the best of our knowledge, there is only. anti-TIF1-γ antibody was known as one of. one case of DM with anti-TIF1-γ antibody. myositis-specific antibody and was present in. with multiple cancer3). In this case, patient. 48% of patients with cancer-associated DM,. had papillary thyroid cancer, left breast can-. which is a useful tool to identify patients with. cer, and gastric signet-ring cell cancer3). She. 2). malignancy with DM . Mugii also reported. was treated with prednisolone and underwent. that almost DM patients with dysphagia had. surgery of all cancers, however, she died 18. patients had myositis-specific antibody. anti-TIF1-γ antibody7). Our patient was an-. months after the first visit3). According to the. ti-TIF1-γ antibody positive DM and had can-. autopsy in Japan, the proportion of cases with. cer and dysphagia, which is consistent with. DM or PM with double cancer and triple can-. .. cer was 1.5% and 0.9%, respectively12). On the. Several studies defined cancer-associated. other hand, the proportion of all cases with. myositis if the malignancy was diagnosed. double cancer and triple cancer was 6.9 % and. within 3 year before or after the onset of my-. 0.8%, respectively12). This result shows that. the previous studies. ositis. 2, 6, 7). 3, 8). . Cancer-associated myositis is charac-. DM and PM patients did not increase multiple. terized by older age, lack of interstitial lung. cancer. Furthermore, there has been only one. disease, resistance to treatment, severe mus-. case report with DM with anti-TIF1-γ anti-. cle weakness, dysphagia, skin ulcer, cutaneous. body positive who had multiple cancer, indi-. 9). necrosis . In addition, erythroderma is defined. cating that our case is rare and worthwhile.. as diffuse scaly erythema of the skin involving. The second clinically important thing is. more than 90 % of the total body skin surface. that anti-TIF1-γ antibody was from positive. area and is not a rare skin manifestation of. to negative after the treatment. TIF1-γ is a. DM10). Erythroderma can be caused by a vari-. transcriptional cofactor and is implicated in. ety of cutaneous and systemic diseases that. TGFβ signaling pathway that controls cell.
(6) Clin Rheumatol Rel Res, 33: 41〜47, 2021. 46. proliferation, differentiation, apoptosis, and tumorigenesis13). TIF1-γ can function as a tumor suppressor. Inoperable breast cancer, the role of TIF1-γ and its interaction with TGF. 1517. doi: 10.1111/ijd.13729. 4) Bohan A, Peter JB. Polymyositis and dermatomyositis. N Engl J Med. 1975; 13; 292 (7):344-7.. β1/SMAD4 signaling pathway is a prognos-. 5) Zaixing Yang, Feng Lin, Baodong Qin, et. tic factor and TIF1-γ expression showed a. al.Polymyositis/dermatomyositis and Ma-. 14). tendency towards poor outcome . However,. lignancy Risk: A Metaanalysis StudyJ. it is not clear the association between an-. Rheumatol 2015; 42(2):282-91.. ti-TIF1-γ antibody and prognosis in patients. 6) David F. Fiorentino, Lorinda S. Chung,. with DM with malignancy. In our case, the. Lisa Christopher-Stine, et al. Most Pa-. patient has remained remission with no re-. tients With Cancer-Associated Dermato-. lapse for 3 years and her anti-TIF1-γ anti-. myositis Have Antibodies to Nuclear Ma-. body and tumor markers have been also neg-. trix Protein NXP-2 or Transcription. ative. This result shows that the anti-TIF1-γ. Intermediary Factor 1γ Arthritis Rheum. antibody may be prognostic factor in patients. 2013; 65(11):2954-2962.. with DM who had anti-TIF1-γ antibody. Fur-. 7) Mugii N, Hasegawa M, Matsushita T, et. ther investigation is warranted to confirm our. al. Oropharyngeal Dysphagia in Dermato-. findings.. myositis: Associations with Clinical and. In conclusion, our findings suggest that. Laboratory Features Including Autoanti-. measuring anti-TIF1-γ antibody regularly. bodies. PLoS One 2016; 11(5): e0154746.. may be important for prognosis in patients. doi: 10.1371/journal.pone.0154746. eCollec-. with DM with malignancy who had anti-TIF1-γ. tion 2016.. antibody.. 8) Chinoy H, Fertig N, Oddis CV, et al. The diagnostic utility of myositis autoantibody. The authors declare no conflicts of interest associated with this manuscript. REFERENCE 1) Targoff IN, Mamyrova G, Trieu EP, et al. A novel autoantibody to a 155-kd protein is associated with dermatomyositis. Arthritis Rheum 2006; 54: 3682-3689.. testing for predicting the risk of cancer-associated myositis. Ann Rheum Dis 2007; 66: 1345-1349. 9) Zahr ZA, Baer AN. Malignancy in myositis. Curr Rheumatol Rep 2011; 13(3):20815. 10) Sung Woo Kim, Yoo Seok Kang, Sang Hoon Park, et al. A Case of Erythroder-. 2) Hida A, Yamashita T, Hosono Y, et al.. mic Dermatomyositis Associated with. Anti-TIF1-gamma antibody and can-. Gastric Cancer. Ann Dermatol 2009; 21. cer-associated myositis: a clinicohistopathologic study. Neurology 2016; 87: 299308. 3) Kikuchi N, Ohashi T, Miura T, et al. Tri-. (4):435-439. 11) Maruani A, Armingaud P, Nseir A, et al. Erythroderma and multiple cutaneous necrosis revealing a dermatomyositis. Ann. ple cancers concurrently detected in a. Dermatol Venereol 2003; 130: 353-356.. case of antitranscriptional intermediary. 12) Natume T, Chikenji H, Suzuki I, et al. A. factor-1γ antibody-positive dermatomyo-. Case of Dermatomyositis and Gastric. sitis. Int J Dermatol 2017; 56(12): 1516-. Cancer—With an Analysis of the Associa-.
(7) 臨床リウマチ, 33: 41〜47, 2021. 47. tion of Dermato- and Polymyositis with. mary Gland Biol Neoplasia 2001; 6(1):67-. Malignancy by Reviewing Nippon Boken. 82.. Shuho from 1975 until 1986. The Nishini-. Kassem L, Deygas M, Fattet L, et al. TIF14). hon journal of dermatology 1990; 52: 231.. 1gamma interferes with TGFbeta1/. 13) Wakefield LM, Piek E, Bottinger EP.. SMAD4 signaling to promote poor out-. TGF-beta signaling in mammary gland. come in operable breast cancer patients.. development and tumorigenesis. J Mam-. BMC Cancer. 2015; 15: 453.. ABSTRACT Anti-transcriptional intermediary factor 1-γ(TIF1-γ) antibody-positive dermatomyositis with triple breast cancers Shin-ichiro Ohmura Department of Respiratory Medicine, Allergy and Clinical Immunology, Nagoya City University Graduate School of Medical Sciences, Nagoya, Aichi, Japan Dermatomyositis(DM)is an autoimmune disease characterized by inflammation of the muscle, specific skin lesion, and autoantibody positivity. Each DM-associated autoantibody isiesare associated with clinical phenotype. Anti–transcriptional intermediary factor 1-γ(TIF1-γ) autoantibodyies has ve been described in adult DM and DM patients with anti-TIF1-γ antibody had a higher proportion of malignancy. We herein report the case of a 71-year-old Japanese woman with DM with anti-TIF1-γ antibody who had triple breast cancer. After cancer resection, she was treated with prednisolone, intravenous immune globulin. Breast cancer did not relapse and her TIF1-γ has been negative for 3 years. Our case suggests that measuring anti-TIF1-γ antibody regularly may be important for the prognosis..
(8)
図
関連したドキュメント
危険有害性の要約 GHS分類 分類 物質又は混合物の分類 急性毒性 経口 急性毒性 急性毒性-吸入 吸入 粉じん 粉じん/ミスト ミスト 皮膚腐食性
⑫ 亜急性硬化性全脳炎、⑬ ライソゾーム病、⑭ 副腎白質ジストロフィー、⑮ 脊髄 性筋萎縮症、⑯ 球脊髄性筋萎縮症、⑰
In the q -th row these differentials compute the homology of the quotient W/Γ with coefficients in the system of groups H q (Γ τ ). In fact, we claim that the coefficients are
For this case the proof seems especially natural. Suppose that Kµ is summable on ∂Γ with respect to the arclength. on ∂Γ with respect to the arclength. The statement presents a
Acknowledgement.This work was partially done while the second author was visiting the University of Texas at Austin and Texas A&M University, and in the Linear Analysis Workshop
Since the centre of any hypersphere tangent to γ at a point lies on the normal plane to γ at that point, the focal curve of γ may be parametrised using the Frenet frame (t, n 1 ,..
We note that Y Hagiwara [7] proved that genus three Heegaard splittings obtained by stabilizing the six Heegaard splittings are mutually isotopic.. This result together with
In Subsection 5.1 we show the continuity of the Dirichlet heat kernel associated with the killed LBM on a bounded open set by using its eigenfunction expansion, and in Subsection 5.2
