* Department of Human Resources Development of the National Institute of Public Health, Ministry of Health
Department of Human Resources Development of the National Institute of Public Health, Ministry of Health, Labor & Welfare
Add: 3–6 Minami 2–chome, Wako city, Saitama Pref. 351–0197 JAPAN
E-mail: ttomoko@niph.go.jp
2 Department of Public Health Administration and Policy, National Institute of Public Health
3 The Administration Department, National Cardiovascular Center
4 Department of Education and Training Technology Development, National Institute of Public Health
COMPETENCES NECESSARY FOR JAPANESE PUBLIC HEALTH
CENTER DIRECTORS IN RESPONDING TO PUBLIC HEALTH
EMERGENCIES
Tomoko TACHIBANA1*, Shinji TAKEMURA2, Tomofumi SONE2,
Kiyotaka SEGAMI3, and Noriko KATO4
Objective To clarify the ``competencies'' required of public health center directors in ``public health emergency responses.''
Methods We selected as our subjects six major public health emergencies in Japan that accorded with a deˆnition of a ``health crisis.'' Their types were: (1) natural disaster; (2) exposure to toxic substances caused by individuals; (3) food poisoning; and (4) accidental hospital in-fection. Item analysis was conducted using the Incident Analysis Method, based on the ``Medical SAFER Technique.''
Results The competencies of public health center directors required the following actions: ◯1to esti-mate the impact on local health from the ``ˆrst notiˆcation'' of the occurrence and the ``ini-tial investigation''; ◯2to manage a thorough investigation of causes; ◯3to manage organi-zations undertaking countermeasures; ◯4to promptly provide precise information on coun-termeasures, etc.; and ◯5 to create systems enabling eŠective application of countermeas-ures against recurrence of incidents, and to achieve social consensus.
Conclusion For public health preparedness, public health center directors should have the follow-ing competencies: ◯1the ability to estimate the ``impact'' of public health emergencies that have occurred or may occur; ◯2be able to establish and carry out proactive policies; ◯3be persuasive; and ◯4have organizational management skills.
Key words:public health center directors, local health administrations, competence, public health emergency responses, emergency preparedness
I. Introduction
Recently in Japan, events that can be termed as health crises have often been encountered1,2,3).
Dis-seminating details of precautions against the
occur-rence or prevention of various kinds of health injury/ damage caused by such health crises has become ex-tremely urgent; therefore, the Ministry of Health and Welfare set up a discussion group in November 1998. The Ministry, working under the recommen-dations of the group, amended the Guidelines to Pro-mote Local Health Countermeasures (to be called the Guidelines hereafter) (See Figure 1). The Guidelines state that local government health facili-ties such as public health centers should fulˆll active and important core roles in local health crisis management. Emergency preparedness and responses have become an expectation of public health organizations and of individual public health practitioners.
In this study, we attempt to clarify the com-petencies required of directors of public health cen-ters managing local health administrations, (to be called simply ``public health center director(s)'' hereafter) in public health emergency responses.
In 2001, the Ministry of Health, Labour and Welfare decided to communicate health-damage caused by infectious diseases, food-poisoning, drinking water, pharmaceuticals, etc. among related departments and bureaus, in order to enable prompt and appropriate measures to be taken for health risk management.
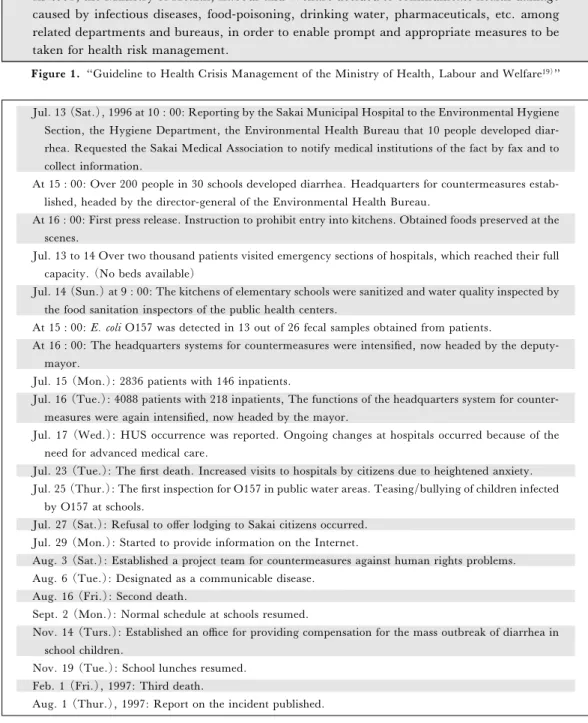
Figure 1.``Guideline to Health Crisis Management of the Ministry of Health, Labour and Welfare19)''
Jul. 13 (Sat.), 1996 at 10 : 00: Reporting by the Sakai Municipal Hospital to the Environmental Hygiene Section, the Hygiene Department, the Environmental Health Bureau that 10 people developed diar-rhea. Requested the Sakai Medical Association to notify medical institutions of the fact by fax and to collect information.
At 15 : 00: Over 200 people in 30 schools developed diarrhea. Headquarters for countermeasures estab-lished, headed by the director-general of the Environmental Health Bureau.
At 16 : 00: First press release. Instruction to prohibit entry into kitchens. Obtained foods preserved at the scenes.
Jul. 13 to 14 Over two thousand patients visited emergency sections of hospitals, which reached their full capacity. (No beds available)
Jul. 14 (Sun.) at 9 : 00: The kitchens of elementary schools were sanitized and water quality inspected by the food sanitation inspectors of the public health centers.
At 15 : 00:E. coli O157 was detected in 13 out of 26 fecal samples obtained from patients.
At 16 : 00: The headquarters systems for countermeasures were intensiˆed, now headed by the deputy-mayor.
Jul. 15 (Mon.): 2836 patients with 146 inpatients.
Jul. 16 (Tue.): 4088 patients with 218 inpatients, The functions of the headquarters system for counter-measures were again intensiˆed, now headed by the mayor.
Jul. 17 (Wed.): HUS occurrence was reported. Ongoing changes at hospitals occurred because of the need for advanced medical care.
Jul. 23 (Tue.): The ˆrst death. Increased visits to hospitals by citizens due to heightened anxiety. Jul. 25 (Thur.): The ˆrst inspection for O157 in public water areas. Teasing/bullying of children infected
by O157 at schools.
Jul. 27 (Sat.): Refusal to oŠer lodging to Sakai citizens occurred. Jul. 29 (Mon.): Started to provide information on the Internet.
Aug. 3 (Sat.): Established a project team for countermeasures against human rights problems. Aug. 6 (Tue.): Designated as a communicable disease.
Aug. 16 (Fri.): Second death.
Sept. 2 (Mon.): Normal schedule at schools resumed.
Nov. 14 (Turs.): Established an o‹ce for providing compensation for the mass outbreak of diarrhea in school children.
Nov. 19 (Tue.): School lunches resumed. Feb. 1 (Fri.), 1997: Third death.
Aug. 1 (Thur.), 1997: Report on the incident published.
Figure 2–A. ``Mass outbreak of diarrhea in school children in Sakai City''
II. Methods
1) We examined major public health emergen-cies that have occurred in Japan and for which the details of the situation and the progress in im-plementing countermeasures and control policies were recorded and available as reports. These con-stituted items from which details of judgments made
by directors of public health centers could be objec-tively identiˆed at times before and after the occur-rence, and until the ultimate crisis resolution. The period of item selection was subsequent to the publi-cation of the Guidelines to Health Crisis Manage-ment of the Ministry of Health, Labor and Welfare (to be called ``MHLW'') for Public Health Centers. The MHLW gave the deˆnition of a health crisis
il-Sept. 11 (Mon.), 2000 19 : 00: A second class emergency system of caution set up. Sept. 12 (Tue.): Sterilization of water requested by Nishibiwajima-cho to the Governor.
Sept. 13 (Wed.) at 7 : 00: Local headquarters for countermeasures against the disaster set up at Kojo, Nishibiwajima-cho and activities for the below carried out: prevention of epidemics, and visiting health counseling. Setting up of a health and hygiene counseling station as instructed by the prefectural government.
Sept. 14 (Thur.): The Disaster Relief Law applied to six cities, other than Kasuga City, Nishikasugai-gun.
Sept. 15 (Fri.) : A local headquarters for countermeasures for waste disposal was set up; Mental health care for visiting health counseling instituted.
Sept. 16 (Sat.) : 90% of water sterilization completed; distribution to homes completed.
Sept. 17 (Sun.): Sterilization work completed 15 : 00; Sterilization at nursery schools, etc. in Shinkawa-cho requested.
Sept. 18 (Mon.): Sterilization against worms in waste and after waste disposal requested by Kitabiwajima-cho; Health nurse requested for visiting health counseling by Shinkawa-cho.
Sept. 22 (Fri.): Meeting of medical rescue groups, etc. held in Nishibiwajima-cho. Sept. 26 (Tue.): Press report saying ``stress seen among preschool children due to ‰oods.''.
Figure 2–B‚ ``Activities of public health centers at the time of torrential rains in the Tokai region''
lustrated in Figure 1. Those selected as our subjects were six:
◯1 Item 1: Countermeasures against accidental hospital infection caused bySerratia marcescens4)
◯2 Item 2: Measures against Toxic Gas Poison-ing in Matsumoto City5)
◯3 Item 3: Measures against an outbreak of diar-rhea in school children in Sakai City ( Es-cherichia coli O157)6); (and see ``Mass
out-break of diarrhea in school children of Sakai City'' [Figure 2–A])
◯4 Item 4: Activities of public health centers at the time of torrential rains in the Tokai region; see [Figure 2–B]
◯5 Item 5: Emergency medical care activities in the JCO Co., Ltd. Tokai Plant's Critical Acci-dent at Tokai-mura7)
◯6 Item 6: Measures against the Wakayama poisoning cases8)
2) Item analysis was conducted using an Inci-dent Analysis Method designed by the authors and based on modifying the analysis method from the Medical SAFER Technique9), a model medical
qual-ity management system based on H2–SAFER10).
The Medical SAFER Technique was developed by the operators of atomic power plants in order to ana-lyze so-called Hiyari-hatto items that they ex-perienced. The authors method applied to this study is as follows11):
3) First, the progression of the incident was or-ganized from the viewpoint of the moments when some new factor became evident and when a person in charge of a public health center made, or should
have made, a decision. Various factors are then con-sidered such as the public reaction (citizens or the media), decisions of public health center o‹cials like section chiefs, decisions of public health center direc-tors, and the practical ability of the public health cen-ter director required to make the critical decision at each moment of time, selected from the results of the organization. After discussion by the authors and 20 research assistants, all doctors studying a specialist course (in 2004) at the National Institute of Public Health, the role of and abilities needed by people in charge (public health center directors) in health cri-sis management were identiˆed case by case, and then organized in a matrix table. In the table, a circle indicates an item in which the public health center director made a proper decision, while a cross indi-cates that in which such a decision was not made; there are also some comments. A blank column in the table indicates that an objective determination of whether or not such a decision was made was not possible from the reports.
4) From the summary of the 6 items, we ana-lyzed and organized by time intervals health crisis management abilities needed by directors of public health centers as common factors for health crises in general, regardless of the type of health crisis in-volved.
III. Results
1) Item analyses: ◯
1 Item 1: [See Table 1–◯1]
Tabl e 1 ◯ 1 . Co unter m easures ag ai nst acci d ental h o spita l infecti o n s caus ed b y Serr at ia marcescens ; Inc ident progression Publi c reaction Dec ision of relevant public he alth ce nt er o‹cial (s) Dec ision of the p ub lic h ealth ce nt er direc to r Bac kground and p rac tic al de ci sion-m aki n g ab ility re-qu ired of the p u b lic h ealth cen-te r d ir ec to r L ega l g ro und s What to not e ex po st fa cto A t th et im eo ft h e o cc u rr en cea n d im m ed ia te lya ft er Ja n. 15 ( Tu e. ) , 2002 at 17: 30: The ˆ rst n otiˆc ation was m ade to the p ublic h ea lth ce n te r b y th eh o sp it ali nq u es ti o no fc o n -tinuous D IC-like symptoms af-te r h igh fe v er, inc ludi ng seve r-al de at hs. Inve stig at ion w as requ est ed. Un ide n ti ˆed collec tive in fe ct i-ous d isease (S /O ); Se ct ion chie f jud g ed an in it ial inve sti g at ion req uire d, ta ki ng int o co nsid erati o n the possi ble sp re ad o f th eo u tb re akt oo u t-side th e h ospit al. S / O = suspec t o f Art. 15 Posi tive ep id em iologi c inve s-tigation of co mmuni -cab le D is ea se s an d M edical C are L aw Init ial in v est igat ion at th e sit e P ossible co llec tive h o spital in-fec ti o ns due to some p ath ogen-ic or ga ni sm, in cl u d ing re sid ent mi crobi ota → Not iˆe d the dire c-to rb y p h o n e af te rm id n ig h t. Prom ptly de cid ed o n an in te r-n al eme rgen cy mee ti n g for d is-cu ssion to be he ld th e n ex t morn in g. Abilit y to u n d erst and ``hospital in fe ct ions inc ludi n g that aris-in g from resid en t mi cro bi ot a'' an d p romptly est im ate the sca le o f impact o n m ed ical care and loc al pub lic healt h Ja n. 16 ( We d. ) , 2002 at 8: 30: Int ern al em erge nc y m ee tin g of all sec ti ons for co untermeas-ure s Ju dged req u est for te ch nic al supp ort for a tec hnical in vesti-gation ( FETP ) to be re-qui re d . FETP = F ield E pid emiology Tra ining Program M ade arran g em en ts w ith th e Tokyo M etropolitan G over-nm en t' s B ure au o f P ubli c He alt h an d the Nat io n al In -st it ut e o f In fec ti ous D is ease s (NIID ). A b ili ty to und erst an d th e ne ed fo r co o peration requ est fo r te ch n ical inv es ti g at io n s and ou tsid e o rgan izat ion ; an d con-cr et ene ss o f arran g em en t o f the organizati on T h e ˆ rst m eet in g o f th e co m -m itt ee fo r cou nt erm ea su res an d technical in vest igation group ( ch ie fo ft h e co m m it te e: th e p ublic h ealth center d irec-tor, an d chief of the g roup : director of th e Informati on Cen ter of NIID ) Im me dia tely d ec ide d to es ta b-li sh a commi tt ee fo r cou nt er-me asu res and a te chnical in v es -ti ga tion group o n the day after th e init ia l n o tiˆ ca ti o n. A b il it yt op re si d e o v era n d co ntrol speci al is t g roups ( in-fectious disease epid emiology , med ical care, bac teriology, et c. ) Sit e inve stig at ion (pat ien t sa mples / en vi ro nme n tal inve s-tigations ) by the p u b lic h ealth ce nt er an d m on it oring o f m edi -cal care b y the Metropolitan Government. T he site in vesti-gation lasted for a tota l o f 2 0 d ays th er eaf ter. U n derstand ing an d in terpreta-ti on of the resu lts o f th e tec hni -cal inve stig at ion ( ˆe ld ep idemi o logy, bacteri o logy, et c. ) A b il it yt ou n d er st an d th e me ani n g o f th e re sul ts o f a te ch n ical in v est igati on th at ca n ch ange rapidly , an d the abili ty for imme d ia te d ec is io n-maki ng as regards changes need ed in co un termeasures
Ta b le 1 ◯ 1 . C ountermeasures agains t accident al h ospital infections caused by Serratia m arcesce ns ; ( co ntin ued ) Inc ident progression Publi c reaction Dec ision of relevant public he alth ce nt er o‹cial (s) Dec ision of the p ub lic h ealth ce nt er direc to r Bac kground and p rac tic al de ci sion-m aki n g ab ility re-qu ired of the p u b lic h ealth cen-te r d ir ec to r L ega l g ro und s What to not e ex po st fa cto Esti mat ions m ad e b y the head of th e o rganiz at ion ( 1) Est ablishi ng the syst em respond ing to resid ents' pr ob le ms ; (2) In ternal co nn ec tion s o f the o rgan izat ion; ( 3) Exte rnal AŠ airs ( the mu ni ci p al asse mb ly , o r-ganizations w ithin the jurisdi ction, n eigh boring loc al governments, and the T okyo and n at iona l gov ernments ) ; ( 4) Response to the m edi a; an d o the rs `` Se rr ati a' ' was foc used on in the inve sti g at ion .→ Th e C o m m u -nic able D isea se an d M ed ica l Ca re La w w as no lo nge r th e basis o f the inve sti g at ion . Est ablishi ng a syste m to respond systematic ally Re spond ing to th e m ed ia : con d uc te d b y p er sonn el at a man age men t le ve l o nl y; fac ts w hi ch bec o m e know n ar et ob ea n n o u n ce d to th e pu blic , as n ec essary , as soon as po ssible after d iscussions of th e T ech n ic al Investig a-ti on Group an d th e com mi t-te e for co un te rme asu res The M ed ic al Se rvic e Law O n e to two m o nt hs aft er the oc cu rren ce Possibi lity of a large n u mb er o f de at hs d u e to me d ic al acc id en ts; iat ro g en ic hospit al in -fe ct ion rep orte d b y T V an d n ews p ape rs → `` T h e hospit al has a co n tami-nated and sloppy sys-te m' '. F ro m th ev ie w p o in t o f th ec u rr en t si tu at io no fJ ap an es em ed ic al ca re, it w as es tim ate d ( i) that th ere is are seri ous h ospita l in fec -tion s o f resi d en t mi crobi ota ,a n d (ii )that u n favorable pe rce p ti ons tha t th ere is `` n o n ee d to n oti fy the aut h orit ie s' ' w ould spread , if the h o spit al in q ue sti o n alon e was the sub jec t o f m ed ia re ‰ec ti o n, an d the inc lin at ion to con ce al me dic al acci den ts, et c. wou ld sp read w it h in the Japane se m ed ical world, → th u s,i tw as n o tag o al` `t o pun ish the h o spital in q ue sti o n an d have it re ce ive b ad publi cit y' ', but `` to en cou rage all m ed ic al inst it uti o ns w it h in th e jurisdi ct ion to co nst ruc t a p rec au ti on an y syst em aga in st hosp ital in fections' ', an d `` establi sh a support system fo r in d ep en d en t p rec au ti ona ry ac-tivi ties by medic al p rofessiona ls' ', not ``m o n it ori n g' ', as very im -port an t. ( a) Abilit y to u n d erst an d the mea n in g o f h osp ital in-fe ct ion s du e to resid ent mi cr ob io ta and to evalu at e th e im p ac t o f suc h inf ec-ti ons o n the en ti re me d i-cal car e sy ste m ( b ) Abilit y to u nde rstan d th e n ec essa ry in trod uc ti on of hea lth p romotio n p oli-cie s fo r m ed ical ca re im -provement Lon g -t erm p ersp ec ti ve Aime d at p rom o ting a local health systems that ca n sup p ort ind epe nde n t act ivit ie s o f local medic al associ at ions for prev ent ion of hospi ta l in fe c-tio n s. Fu tu re prec au ti ons aga in st rec u rren ce o f h osp ital infec-tion s sho uld b e, in ste ad o f tradit ion al `` m onit orin g' ' b y the p u b lic h ealth center, in -dep end en t p rec aut ions of ta ke n by m edic al inst it u ti ons. Est ab lishm en t o f ac cid en t precautions in coop erati o n w ith loc al m ed ic al associ at ion s A b il it yt oe x p la in co u n te r-me asure s aime d at lo cal he alth to me di ca l as so ci at io n s and othe r o rgan izat ions an d arran -gement of several p ro fessi onal organizati ons
Ta b le 1 ◯ 1 . C ountermeasures agains t accident al h ospital infections caused by Serratia m arcesce ns ; ( co ntin ued ) Inc ident progression Publi c reaction Dec ision of relevant public he alth ce nt er o‹cial ( s) Dec ision of the p ub lic h ealth ce nt er direc to r Bac kground and p rac tic al de ci sion-m aki n g ab ility re-qu ired of the p u b lic h ealth cen-te r d ir ec to r L ega l g ro und s What to not e ex po st fa cto Pre ca u ti o n s initiat ed by loca l medic al associ at ions: ( a) Di sp at ch of me mb er ( s) to th e com mi tt ee fo r co un termeasures and p la y ing a role in develop-in g p re ca ut io n act iv it ie s from the results of inv es-tigation of ca uses; ( b ) L ec tu res o n p reve n ti on against h ospital infe c-ti ons ( tw ic e in th e ˆrst y ear an d as su ch to b e co nt in ued ) ; (c) Se tt in g u p a co mmi tt ee fo r coun te rme as ures against in fe ctions, m ade up o f med ical assoc ia-ti ons; ( d ) Pre p aring and dist ribut -in g a m anu al of precau -ti on s against in fe ct ious dise ases an d crisis m ana ge me nt ; and ( e) Int en si v e self -c h ec k o f pr ec au ti on s ag ai n st h o spit al inf ect ion s by th e medic al associates; Public h ealth ce nt ers should coord inate various indepen-den t ac ti viti es o f m ed ica l o r-ganiza tions such as d evelop ing infec tion control nurse courses by the Japane se N ursin g As-sociation. R ecomme nd at io ns of th e com-m itt ee fo r co unt erm easu res to national and p rivate organi za-ti ons (me dic al eq u ipm ent ma ke rs, etc .) as well as lo cal medi cal assoc iations fo r th e purpose o f d eveloping p re cau-ti ons against hosp ital in fe ct ions A b il it yt ou n d er st an d an d re al -iz e that the pub lic healt h ad-ministration should aim at making and continuously m aint ainin g loc al he alth sys-te m s u n de r w hich pu blic he alt h an d m ed ical care are clo se ly rela te d to each o th er
Practical decision-making competencies required of the public health center director (to be called the ``Decision-making competencies'' hereafter) are: A) to understand hospital infections, including that aris-ing from residentmicrobiota and promptly estimate the scale of the impact on medical care and local pub-lic health; B) to understand the need for cooperation requests for technical investigations and with outside organizations; C) to preside over specialist groups (infectious disease epidemiology, medical care, etc.); D) to make a decision immediately as regards changes in countermeasures; E) to understand the meaning of hospital infection due to resident microbio-ta and to evaluate the impact on the entire medical care system; F) to understand the necessary in-troduction of health promotion policies for medical care improvement; G) to explain the countermeas-ures aimed at local health to medical associations and other organizations; and H) to understand and real-ize that the public health administration should aim at making and continuously maintaining local health systems.
◯2 Item 2
This type was exposure to toxic substances caused by individuals. Decision-making competen-cies are: A) to give accurate instructions about or-ganizing information; B) to set up a crisis manage-ment system; C) to request cooperation from outside organizations; D) to understand the meaning of threatened spread of an air polluting substance and to estimate the impact scale promptly; E) to move forward and control the responses of the center; F) to give due consideration to resident anxiety regarding unidentiˆed causes of incidents and to give a relevant press release; G) to understand the results of techni-cal investigations and to implement concrete coun-termeasures; H) to estimate the environmental im-pact of agents like sarin and to decide the necessity of follow-ups; I) to estimate the impact of agents like sarin on health from the viewpoint of medical care and public health and to decide on necessity and coordination of surveys; J) to investigate in liaison with universities; K) to promote local health meas-ures; and L) to release precise information to resi-dents.
◯3 Item 3: [See Figure 2–A]
This type was food poisoning. Decision-making competencies are: A) to build a network; B) to judge large scale food poisoning to have occurred and to decide on the establishment of a countermeasure headquarters and to select necessary personnel; C) to decide on who takes ˆrst preference for investiga-tion; D) to gauge resident anxiety and promptly respond to it; E) to cooperate with local medical care systems; F) to decide on who takes the ˆrst priority
for home visits; G) to provide exploration so that citizens can understand the situation and have their anxieties relieved, taking human rights into con-sideration; H) to decide on declarations of safety given the various data on the situation; and I) to de-cide on the range of compensation.
◯
4 Item 4
This type was a natural disaster. Decision-mak-ing competencies are: A) collectDecision-mak-ing and providDecision-mak-ing precise information; B) to estimate promptly what countermeasures are required and for what area; C) to arrange and coordinate the personnel placement and unify intentions in the center; D) to promptly carry out countermeasures aimed at helping the most vulnerable; E) to devise diversiˆed approaches to cope with mental stress; F) to be able to make arran-gements and coordinate with technical organizations promptly when necessary; G) to understand coun-termeasures that can be rapidly changed without no-tice and e‹ciently respond; H) to make arrange-ments among various organizations to secure human resources; I) to be able to switch in peacetime to an emergency mode when responding to a situation; J) to promptly conˆrm the situation and to consider ap-propriate responses; and K) to recognize the necessi-ty for long-term follow-ups such as PTSD.
◯
5 Item 5
This type was exposure to radiation caused by an accident. Decision-making competencies are: A) to understand the meaning of a nuclear accident and to estimate how large the impact might be; B) to conˆrm in advance how the public health center should cope with the situation; C) to take the impact on residents into consideration and to consider or-ganizing systems inside the center; D) to recognize the necessity for collecting information and decide on countermeasures urgently; E) to shift from a peace-time system to a crisis management one in accord with the changing situation; F) to give appropriate instructions according to the site situation; G) to take specialists' opinions into consideration when making decisions; H) to understand the situation and estimate which is better, commanding the center or inspecting the site; I) to organize the center sys-tem to provide for long-term actions; J) to under-stand necessary requests for cooperation with outside organizations; K) to understand residents' anxieties and appropriately attend to them; and L) to acquire knowledge of nuclear items relevant to daily life.
◯
6 Item 6
This type was also exposure to toxic substances caused by individuals. Decision-making competen-cies are: A) to maintain and control the system un-der which emergency communication is possible; B) to understand and foresee the big picture of the scale
Tab le 2 Summ ar y. T h eS u m m ar y of th e` `S p ec ia l A b il it yC h ar ac te ristics' ' of Directors d u rin g H ealth C rises H o spit al inf ec tio n in Setagaya Toxic G as Poison-ing C ase in M at -sumoto Inac curate ins p ection of O 157 at K P ublic Heal th Cen ter Ma ss outbr eak of di-ar rhea in school chil-dren of Sakai C ity A ctivit ies at the tim e of torrential rains in Tok ai region The JCO Critica l Acc ide nt in Tokai-mu ra Poiso n in g C ase in Wakayama 1. The initial stage P reparat io n in p ea -ce tim e No co nc ept o f coun -te r-me as ure s aga in st h ea lth proble m s be tw ee n la w and or d er and agre em en ts an d ar-ran g em en ts ? Is the appro v al ste p to ord er collection th es am ea st h ato f other p u b lic h ea lth ce nt er s? ◯ There w as the Nu cl ea r D is as te r Preve n ti on Manual. Promptly conˆ rm th er o leo fe ac h o‹ cial Conne ct ion syst em ◯ As li g h td el ay o f no tiˆ ca ti o n from th e st aŠ to the di re c-tor (?) ×? There w as a syst em w h er eby approval fr om th e v ic e-d ir ec-to r w as possi ble. ◯ Dec ision to shif t to em erge nc y syst em : Esti mat ion ab ilit y of im p ac t ◯ Im me dia te d ec i-sions after d iscus-sions at m eetings in-si d e th e cen te r ◯× The p re dic ti o n that a m ajor qu an tity of goo ds would b e recalled in th e su m-mer g if t season △? Abilit y to th ink of gravest O 157 cases; to remem-ber p rec ed ing cases; and to fore-see H US oc cur-ren ce w as desi red. The d ec ision to set u p a head-quart ers fo r cou n te r-me as ures across the w hole cit y w as p ro mp t. ◯ Early ac ti o ns to pro -te ct th e m o st v ul-ne rab le in the di s-ast er ◯× D ec ision on the d ispatc h of o‹ -cials b ase d on the esti mation of the in ci d ent w h er e food poisoning is qu es ti o n ab le ; To suspect the or-di n ar y an d u se common sen se 2.
Prevention strategies against
h ea lth in ju ry /dam age sp read; surv ey m ana ge me nt for inve sti ga-tion of causes Ca rryi n g o ut of p re v en ti ve ac ti vi ti es ag ai nst h ea lt h in ju-ry /dam age sp read ◯◯ ? × Th e p re v ent io n o f seco nda ry infe ct ion should have been sta rte d at the tim e of the d ecisi o n o n school closi n g. ◯ Plac em en t o f X -r ay tech nologi st an d hea lth nurses, etc. Dec ision on th e nec essi ty an d prom ptn ess of th e init ial invest igat ion ◯◯× ◯◯ △ ? Phones should no t be re lied on for tran sf er of co mp li -ca te d inf o rmat ion
Tabl e 2 Summa ry . T h e S u m m ar y o f th e ``S pecia l A b ility C h ar acteristics '' o f D ir ecto rs d u rin g H ea lth C ri ses ( co n tinued ) H o spit al inf ec tio n in Setagaya Toxic G as Poison-ing C ase in M at -sumoto Inac curate ins p ection of O 157 at K P ublic Heal th Cen ter Ma ss outbr eak of di-ar rhea in school chil-dren of Sakai C ity A ctivit ies at the tim e of torrential rains in Tok ai region The JCO Critica l Acc ide nt in Tokai-mu ra Poiso n in g C ase in Wakayama Un derst andin g o f te chn ical inve stig a-tion /survey; arran-gement, coordina-tion an d co n tro l w ith ou tsi d e o rgan i-za ti ons ◯◯ En try inspe ct ion the ne xt da y; w ea th er, speciˆ c substa n ces in air, to xic sub-sta n ces, etc. △? Conta ct s and n ot iˆ-catio n s w ere prom pt. T ec hn ic al inve stig at ion s w ere carried ou t o n e-w ay, fro m CDC, an d the ce nt ra l government ◯ Site in spec tio n based o n the es tim a-tion of th e site si tua-tion an d ac cordi ng to th ea d v ic eo ft h e central government 3. Organizatio n m ana ge me nt Organi zati on arran-ge me nt in th e p ub -lic h ea lth center an d ad mi nistra tion or-ga niza tion ◯◯× ◯◯ Instruc tio ns ac cord-in gt ot h e si tu at io n △ Although a h ead-qu arte rs for cou n-te r-me asu res was set u p, the stand-b y personn el g roup was d issolved before verifyi n g settle-me nt . o f th e si tu a-ti on Arra n g em en t an d coordi nati on with out side o rganiz a-tion s (med ic al as-sociations, nei g hbori ng mu nic ipalit ie s, the central govern-me nt , et c. ) ◯◯× Sup porte d by volun te er ac tivi tie s throu g h the holi day me dic al ex am ina -tion n etw ork o f me dic al inst itu ti ons ◯ Ac ce ptan ce of volunteers, etc . ◯ Show in g p re sen ce as a comman d in g o‹c er ◯ Ab ilit y to se t co un -te r-me asu re targe ts an d to ex p la in grounds for decisi on ma kin g ◯×
Tabl e 2 Summa ry . T h e S u m m ar y o f th e ``S pecia l A b ility C h ar acteristics '' o f D ir ecto rs d u rin g H ea lth C ri ses ( co n tinued ) H o spit al inf ec tio n in Setagaya Toxic G as Poison-ing C ase in M at -sumoto Inac curate ins p ection of O 157 at K P ublic Heal th Cen ter Ma ss outbr eak of di-ar rhea in school chil-dren of Sakai C ity A ctivit ies at the tim e of torrential rains in Tok ai region The JCO Critica l Acc ide nt in Tokai-mu ra Poiso n in g C ase in Wakayama 4. Ro le as exter-nal spokesper-son Establi shm ent o f cle ar syste m o f responsibili ty an d simple process o f dec ision -m aking ◯◯ P rom pt ly p ro v idi n g prec ise informa tion based o n the fac ts foun d ◯× △ ? Ma king use o f the Internet inf o rma-tion , th o ugh th e me dia app are n tl y took th e lead o n th is issue △ The m ed ia resp onse imme di at el y af te r th e in ci d en t; Con -fu se d af te r th e inc i-de nt oc cu rred. Po si ti v e re le as e o f co un te r-mea sur es polic y ◯△ T h e m essa ge s w er e re le as ed by the loca l gover n ment, n ot th e pub lic hea lt h ce nter 5. Follow-up af ter th e coun te r-mea sure s; E s-ta blishm en t o f co nt inu o us pr ev en ti v e mea sure s against recur-renc e Fo ll o w -u p o f res i-d ent s and th e m ost vuln erable in soci e-ty ◯? ◯ Fo llo w-up health ex am in at ion × Req u ire d co nsid er-at ions of hea lth problems of volun-te ers an d p erson nel of the center ◯◯ Est ablishm en t o f a system supported by psyc hiat ri sts, et c. Ad mi nis tr atio n s ab ilit y to re ali ze sy s-tem improvements to p re v en t rec u r-renc e ◯× The p o w er of th e d irec tor of the p ubic he al th ce n te r w as act u ally tr an sfe rred to th e d ep art m en t man ager o f th e lo ca l gov ernment. Role of o v erall evaluation on a s-erie s o f cou nt er-me as ures in th e form of w ritt en reco rds and artic les ◯◯× ◯◯◯◯ ac ir cl e (◯ ) in dic ate s an ite m in w h ich th e p ubli c h ea lth cent er d ire ct o r m ad e a prope r de ci sion a cross (×) in di cate s that in w hi ch suc h a d eci sion w as not m ad e A b lank co lum n in th e table in dic at es that an o bje ct ive det erm in ation o f w het h er or n o t suc h a d ec ision was m ade w as no t p ossible from the re port s.
(i) Estimation of switches from peacetime to emergency systems
(ii) Technical knowledge about medical and public health sciences, administration techniques, and situations within the jurisdiction and (i.e. a fund of knowledge and experience to estimate impact)
(iii) Power to perform prevention countermeasures against health injury/damage spread (often at the same time as the initial investigation)
(iv) Ability to collect information necessary for impact estimation (v) Power to perform the initial stage of an epidemiological investigation
(vi) Arrangement of, coordination with, and management ability of organizations engaged in technical investiga-tions and surveys (local institutes of public health, the central government, CDC, etc.)
(vii) Power to control the internal organization (decisions, instructions)
(viii) Arrangement and coordination ability among outside organizations (medical associations, neighboring municipalities, and central government.)
(ix) Ability to set targets for countermeasures and explain grounds for decisions inside and outside of one's own or-ganization
(x) Establishment of a system with clear responsibility and a simple decision-making process
(xi) Ability to promptly explain about necessary matters to victims, neighboring residents, media or politicians, based on precise medical knowledge and a sound scientiˆc viewpoint
(xii) Let others know about the lessons learnt from countermeasures from a positive perspective, not with a passive attitude
(xiii) Knowledge of actions for PTSD and how to protect the most vulnerable in society
(xiv) Power to achieve the realization of systematic improvements for residents after taking countermeasures (xv) Ability to summarize a series of countermeasures in the form of reports and articles
Figure 3. Competencies required of public health center directors can be generalized into 15 elements (i)–(xv):
of the incident and its outlines; C) to decide on set-ting up headquarters for countermeasures; D) to ex-plain the situation to the media; E) to recognize that the case might be a crime; F) to recognize the gravity of the situation and to act cautiously before the course of the incident becomes clear; G) to ask tech-nical organizations outside the center for cooperation and to arrange that cooperation; H) to foresee long-term health injury/damage to residents; I) to ar-range and coordinate the cooperation of psy-chiatrists, schools, civil volunteers, universities, medical associations, and others; J) to consider ex-penditure; and K) to acquire technical knowledge to prepare a relevant manual.
Summary of theRole and Special Ability Character-istics of Directors of Public Health Centers managing Local Health Administrations during Health Crises as seen in ˆve of the subjects [see Table 2–Summa-ry]
2) Summary of theCompetencies of Public Health Center Directors in Responses to Public Health Emergencies by time intervals:
In analyzing the competencies required of pub-lic health center directors and needed for Pubpub-lic Health Emergency Responses, it was found that they could be generalized into 15 elements [See Figure
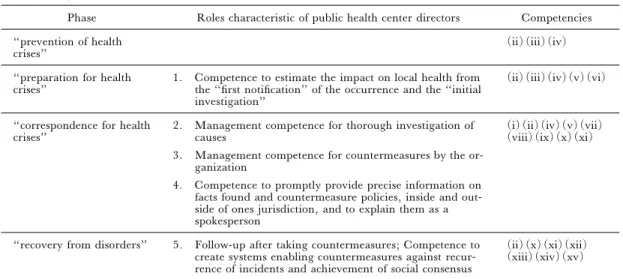
3]. These were here summarized under the phases prevention of a health crisis, preparation for a health crisis, correspondence of health crises, and recovery from a disorder. [See Table 3].
IV. Discussion
Emergency preparedness is an expectation of public health organizations and individual public health practitioners12,13). Both the process of
govern-ing and public administration systems have been un-dergoing radical changes in the course of the last quarter of a century all over the world14,15).
Decision-making competencies for health crisis management can be generalized into ˆfteen groups and concrete descriptions of the competencies and roles can be gained from approapiate analysis. Whatever acci-dents caused by agents or the computerized Y2K where a health hazard did not, any likelihood of problems is a matter of concern for health crises in-cluded in the guideline deˆnition. Although such situations are considered to be important and might require intervention by health centers concrete ex-amples were not found and so these subjects were not included in the present study.
Table 3. Summary of the ``Competencies'' of Public Health Center Directors for Public Health Emergency Responses by time point:
Phase Roles characteristic of public health center directors Competencies ``prevention of health
crises'' (ii)(iii)(iv)
``preparation for health
crises'' 1. Competence to estimate the impact on local health fromthe ``ˆrst notiˆcation'' of the occurrence and the ``initial investigation''
(ii)(iii)(iv)(v)(vi)
``correspondence for health
crises'' 2. Management competence for thorough investigation ofcauses 3. Management competence for countermeasures by the
or-ganization
4. Competence to promptly provide precise information on facts found and countermeasure policies, inside and out-side of ones jurisdiction, and to explain them as a spokesperson
(i)(ii)(iv)(v)(vii) (viii)(ix)(x)(xi)
``recovery from disorders'' 5. Follow-up after taking countermeasures; Competence to create systems enabling countermeasures against recur-rence of incidents and achievement of social consensus
(ii)(x)(xi)(xii) (xiii)(xiv)(xv)
safeguard the public and resolve the problem with a top-down command system in an organization head-ed by a public health center director16,17), who is
ex-pected to be an individual with the competencies dis-cussed above.
Competence to estimate the ``impact'' of public health emer-gencies that have occurred or may occur
The impact of a health crisis can be formulated as a function of the following four parameters:
Impact (u, t)=F{Quantity (u), Magnitude (u), Velocity (u), Vagueness (u), t}
i) Quantity: Maximum injury/damage, includ-ing the numbers of victims, damaged houses and buildings
ii) Magnitude: Maximum injury/damage level, ranging from light serious and including death
iii) Velocity: Speed of the spread of injury/ damage (a space element such as the spread of the injury/damage area and the time element, such as how much time it will take for the injury/damage to reach the maximum)
iv) Vagueness: Uncertainty about the occur-rence point, cause, injury/damage to subjects, ac-tions)
The four parameters, except for time, have ``uncertainty (u)'' as a common element, with the most serious situation of uncertainty being that in the initial stage of a crisis. To assess the degree of this uncertainty, the proper collection of information is essential. Instead of the passive response of waiting for information, it is necessary for staŠ to be instruct-ed to proactively collect information; this includes
giving advice about how information should be col-lected. In practice, the ability to estimate the impact of a health crisis, and proof of knowledge/technology related to medical knowledge and epidemiological practice is indispensable, because ˆeld epidemiology is necessary when all the variables are to be esti-mated.
Competence in establishing and carrying out proactive policies i) Actions in response to a health crisis must start to be taken in parallel with the occurrence of the crisis; that is, before the impact has been deter-mined. As such, a policy of primary action needs to be decided and implemented.
ii) After carrying out primary actions, reactions to events inside and outside the center, and informa-tion collected to establish the impact up to that point need to be re-examined; the suitability of the prima-ry actions should be evaluated, the action policy cor-rected and the strategy for secondary actions decided and implemented.
iii) The process in ii) is repeated and several more actions may be implemented. Ultimately, ˆnal actions and policy must be decided and implement-ed. Based on the assessed impact, which would be es-tablished as a peacetime action.
Competency in acquiring persuasiveness
Directors must show victims, neighboring resi-dents and groups that they have a scientiˆc under-standing of the problems that have occurred, and must show adequate conˆdence backed by relevant knowledge. When the total picture of the situation is not clear and the most important aspects are still unknown, much more strict evaluation must be made. Wisdom to judge a situation and properly
an-swer questions about symptoms and the phenomena presented, along with responsibility and potential medical and other knowledge are all required.
This holds true for explanations to politicians and media of the situation and interim responses. For a public health center to take an active role in achieving people's trust, the director must satisfy the external requirement of being a doctor and the re-quirement of having the competence to explain ap-propriately all necessary matters based on precise medical knowledge and a sound scientiˆc back-ground.
Competence in organization management
In health crisis management, the competence required of the person in charge of managing an or-ganization can be divided into two categories18): one
involving control inside the organization (=internal control) and the other control of outside organiza-tions (=external control).
The target of control inside the organization is mainly the internal structure of the municipal or-ganization. To keep up with a situation that might be changing every moment of a health crisis, securing a correct and prompt communication route for infor-mation and establishing a clear decision-making process is indispensable. Also to be clariˆed is the system for sharing roles within the inside organiza-tion, particularly with regard to management of technical facilities within the public health center in respect to the scientiˆc investigation of causes during a health crisis.
In contrast, the control of outside organizations covers prevention of health injury/damage spread, response to and arrangement of organizations within the jurisdiction (residents, local medical associa-tions, etc.), arrangement and coordination among outside organizations (technical institutes, munici-palities, etc.). For these functions to be e‹ciently carried out, extensive medical knowledge and man-agement competence are required.
V. Conclusion
The characteristics and extent of health crisis management competencies required of public health center directors can be summarized as:
(1) Competence to estimate the impact from the viewpoint of local health, based on the ˆrst notiˆ-cation of the occurrence of a health crisis and the results of the initial investigation.
(2) Competence to manage the investigation of causes.
(3) Competence to manage the administra-tive organizations for carrying out countermeasures. This entails the ability to be an eŠective spokesman.
(4) Ability to oversee the establishment of a system that allows for continuous precautions to be taken against the recurrence of similar cases within the center's jurisdiction.
Acknowledgments
We thank Dr. Wakasugi, Hideshi (Toyota City Public Health Center) who provided us with the item related to ``Torrential Rains in the Tokai Region,'' and the researchers below, as students of a Specialist Course at the National Institute of Public Health, for their invaluable opinions, which con-tributed to the discussions in this article: Cooperative researchers: Tomoyasu Ikeno (Chito Public Health Center), Hirotaka Oishi (Wakkanai Public Health Center); Hiroshi Kurusu (Utsunomiya Public Health Center), Tomoe Kodama (Okayama Uni-versity), Yasuhiro Sakamoto (Tomakomai and Muroran Public Health Centers), Hiroshi Sumi (Yamazaki Health and Welfare O‹ce), Hiroshi Takeuchi (Niigata Public Health Center), Naoki Terai (Nagano Integrated Health Center), Masahi-to Toshima (Asahikawa Public Health Center), Nobuhiko Nagai (Okatsu Area Promotion Bureau and Yuzawa Public Health Center), Yoko Nakaoka (Tobu Public Health Center), Yoshihiro Fukuda (Tatebayashi Health and Welfare O‹ce), Ryoji Matsumoto (Mobara Public Health Center), Masa-hiro Yanagimoto (Wakasa Health and Welfare Cen-ter), Eiji Yamazaki (Saitama Public Health Center), Isamu Yamamoto (Nishinomiya Public Health Center), Takanao Yoshimura (Abeno Health and Welfare Center)
References
1) Nishinomiya Public Health Center. Activities of Nishinomiya Public Health Center in the Great Han-shin-Awaji Earthquake Disaster. Hyogo: 1995. (in Japanese)
2) Study Group of Public Health Emergency ness. Handbook of Public Health Emergency Prepared-ness. Tokyo: Chuohoki, 2003. (in Japanese) 3) Maekawa K. Control study on patients physically
and psychiatrically aŠected by chronological stage of victims of the sarin gas attack on the Tokyo Subway, Research Report by Scientiˆc Research Subsidies of the Ministry of Health, Labor and Welfare in 1998. Tokyo, 1999. (in Japanese)
4) Setagaya Ward. The report of countermeasures aga inst accidental hospital infection caused by Serratia marcescens. Tokyo: Setagaya Ward, 2002. (in Japanese)
5) The Council of Comprehensive Regional Medical Care in Matsumoto City. The report of investigation into toxic gas poisoning case. Nagano: the Council of
Comprehensive Regional Medical Care in Matsumoto city, 1995. (in Japanese)
6) The headquarters of the countermeasures against outbreak of diarrhea in school children of Sakai. The report of outbreak of diarrhea in school children of Sakai City (Escherichia coli O157). Osaka: Sakai City, 1997. (in Japanese)
7) Ibaraki Prefecture. The record of emergency medical care activities in the JCO Critical Accident in Tokai-mura. Ibaraki : Ibaraki Prefecture, 2000. (in Japanese) 8) Wakayama-city public health center. The report of the incidence of poisoning cases in Wakayama. Wakayama: Wakayama-city, 2000. (in Japanese) 9) Kono R. Preparing for case analyses. In: Human
Er-ror in Medical Care. Tokyo: Igaku Shoin, 2004; 104–114. (in Japanese)
10) Yoshizawa Y. Development of a case analysis method for human error H2–SAFER and the analysis-support system FACTFLOW. Nihon Puranto Hyuman Fakuta Gakkaishi 2002; 7: 2–9. (in Japanese)
11) Tachibana T. Structural analysis of the ability and the technology which is necessary for the health risk management used in the 3a health crisis case. Annual Report of the Study Group on research about regional health risk management study and training. Japan: Mi-nistry of Health, Labor and Welfare, 2005. (in Japanese)
12) Lichtveld M, Cio‹ J, Henderson J, et al. People pro-tected―public health prepared through a competent workforce. J Public Health Manag Practice 2003; 9:
340–343.
13) Gebbie K, Merrill J, Hwang I, et al. The public health workforce in the year 2000. J Public Health Ma-nag Practice 2003, 9: 79–86.
14) Cerase F. The competencies required in Public management: a case study in Italy. In: Horton S, Hon-deghem A, Farnham D, editors. Competency Manage-ment in the Public Sector. Amsterdam: IOS Press, 2002; 135–153.
15) Jernigan JA, Stephens DS, Ashford DA, et al. Bioter-rorism-related inhalational anthrax: the ˆrst 10 cases reported in the United States. Emerging Infectious Dis-eases 2001, 7: 933–944.
16) Mores SS. Building academic-practice partnerships: the Center for Public Health Preparedness at the Columbia University Mailman School of Public Health, before and after 9/11. J Public Health Manag Practice 2003, 9: 427–432.
17) Gebbie K, Merrill J. Public health worker competen-cies for emergency response. J Public Health Manag Practice 2002, 8: 73–81.
18) Tachibana T. Competencies of the local public health administrators. Koshu Eisei 2005, 69: 522–523. (in Japanese)
19) The Ministry of Health, Labor and Welfare. The guideline to health crisis management of the Ministry of Health, Labor and Welfare (2001). In: Study Group of Public Health Emergency Preparedness. Handbook of Public Health Emergency Preparedness. Tokyo: Chuo-hoki, 2003. (in Japanese)