岩手医科大学 審 査 学 位 論 文
(博 士)
Clinical Science (2016)130, 1115–1124 doi: 10.1042/CS20160094
Dysregulation of ossification-related miRNAs in circulating osteogenic progenitor cells obtained from patients with aortic stenosis
Kan Takahashi*, Mamoru Satoh†, Yuji Takahashi*, Takuya Osaki*, Takahito Nasu*, Makiko Tamada‡, Hitoshi Okabayashi§, Motoyuki Nakamura‡ and Yoshihiro Morino*
*Division of Cardiology, Department of Internal Medicine, Iwate Medical University, 19-1 Uchimaru, Morioka, Iwate 020-8505, Japan
†Division of Biomedical Information Analysis, Institute for Biomedical Sciences, Iwate Medical University, 2-1-1 Nishitokuta, Yahaba-cho, Shiwa-gun, Iwate 028-3694, Japan
‡Division of Cardioangiology, Nephrology and Endocrinology, Department of Internal Medicine, Iwate Medical University, 19-1 Uchimaru, Morioka, Iwate 020-8505, Japan
§Department of Cardiovascular Surgery, Iwate Medical University, 19-1 Uchimaru, Morioka, Iwate 020-8505, Japan
Abstract
CAVD (calcific aortic valve disease) is the defining feature of AS (aortic stenosis). The present study aimed to determine whether expression of ossification-related miRNAs is related to differentiation intro COPCs (circulating osteogenic progenitor cells) in patients with CAVD. The present study included 46 patients with AS and 46 controls.
Twenty-nine patients underwent surgical AVR (aortic valve replacement) and 17 underwent TAVI (transcatheter aortic valve implantation). The number of COPCs was higher in the AS group than in the controls (P<0.01). Levels of miR-30cwere higher in the AS group than in the controls (P<0.01), whereas levels ofmiR-106a,miR-148a, miR-204,miR-211,miR-31andmiR-424were lower in the AS group than in the controls (P<0.01). The number of COPCs and levels of osteocalcin protein in COPCs were positively correlated with levels ofmiR-30aand negatively correlated with levels of the remaining miRNAs (allP<0.05). The degree of aortic valve calcification was weakly positively correlated with the number of COPCs andmiR-30clevels. The number of COPCs andmiR-30clevels were decreased after surgery, whereas levels of the remaining miRNAs were increased (allP<0.05). Changes in these levels were greater after AVR than after TAVI (allP<0.05).In vitrostudy using cultured peripheral blood
mononuclear cells transfected with each ossification-related miRNA showed that these miRNAs controlled levels of osteocalcin protein. In conclusion, dysregulation of ossification-related miRNAs may be related to the differentiation into COPCs and may play a significant role in the pathogenesis of CAVD.
Key words:aortic valve replacement, calcific aortic valve disease, calcification, osteocalcin, transcatheter aortic valve implantation.
INTRODUCTION
CAVD (calcific aortic valve disease) is the most common valv- ular heart disease in the aging population and is associated with significant morbidity and mortality [1]. CAVD represents a pro- gressive pathological process progressing from slight thickening of the aortic valve without obstruction of blood flow to aortic valve sclerosis and finally to AS (aortic stenosis) with severe cal- cification of the valvular leaflets, reduction in valve motion and
Abbreviations:APC, allophycocyanin; AS, aortic stenosis; AU, arbitrary units; AVC, aortic valve calcification; AVR, aortic valve replacement; BMP, bone morphogenetic protein; CAD, coronary artery disease; CAVD, calcific aortic valve disease; COPC, circulating osteogenic progenitor cell; Cy5.5,N,N-dicarboxypentyl-indodicarbocyanine-5,5-disulfonic acid; KDR, kinase insert domain-containing receptor; mAb, monoclonal antibody; MDCT, multidetector computed tomography; MFI, mean fluorescence intensity; oxLDL, oxidized low-density lipoprotein; PBMC, peripheral blood mononuclear cell; PE, phycoerythrin; PerCP, peridinin–chlorophyll protein complex; TAVI, transcatheter aortic valve implantation; t-BHP, t-butyl hydroperoxide.
Correspondence:Associate Professor Mamoru Satoh (email [email protected]).
obstruction of blood flow [1]. Previous studies have shown CAVD to be mediated by a chronic inflammatory disease process, with many similarities to the pathological process underlying ather- osclerosis which includes inflammatory cell infiltrates, lipopro- teins, extracellular bone matrix proteins and bone minerals [2].
A recent report implicates osteogenic processes as key mechan- isms in CAVD [3]. In particular, circulating osteogenic progenitor cells are involved in heterotopic ossification in the valve tissues [4,5]. G¨ossl et al. [6] have reported that high numbers of COPCs
(circulating osteogenic progenitor cells) indicate accelerated pro- gression of CAVD in humans. However, little is known of the mechanisms of the cellular and molecular components and pro- cesses of CAVD.
miRNAs are the most abundant family of small non-coding RNAs and these regulate mRNA translation of target genes through the RNAi pathway [7,8]. We have reported previously that expression of inflammation- or longevity-related miRNAs in endothelial progenitor cells is involved in the pathogenesis of coronary atherosclerosis [9,10]. Some studies have suggested that miRNAs play an important role in osteogenic differentiation from bone marrow stromal cells and mesenchymal cells [11,12]. In particular, it has been reported that ossification-related miRNAs, including miR-106a, miR-148a, miR-204, miR-211, miR-30a, miR-31andmiR-424 act as important endogenous negative or positive regulators of osteogenesis of human mesenchymal pro- genitor cells and bone marrow stromal cells [11,13,14]. However, it remains unknown whether expression of ossification-related miRNAs is related to osteogenic differentiation of circulating progenitor cells in patients with CAVD.
The aim of the present study was to determine whether ossification-related miRNAs are expressed with osteocalcin in COPCs obtained from patients with CAVD compared with con- trols. In addition, the present study evaluated the effects of sur- gical treatments on expression of ossification-related miRNAs and osteocalcin levels.
MATERIALS AND METHODS Study population
The present study was approved by the ethics committee of the Iwate Medical University School of Medicine (H26-46), and writ- ten informed consent was obtained from all subjects. A total of 46 patients with severe clinical and echocardiographic AS were re- ferred for pre-operative clinical examination. The severity of AS was determined by standard echocardiographic methods. Severe AS was defined as symptomatic AS or an aortic valve area of 1.0 cm2or an aortic valve area index of0.6 cm2/m2or mean aortic gradient>60 mmHg or peak aortic velocity>5 m/s [15].
Patients were excluded from the study if they had clinical signs of acute coronary syndrome, acute infection, severe renal failure (serum creatine levels over 3 mg/dl) or rheumatoid disease, or if they were suspected of having a malignant or primary wasting disorder.
As controls, 46 subjects were identified from a list of outpa- tients attending our university hospital for treatment of hyperten- sion, dyslipidaemia or arrhythmia, and showing no evidence of AS on history or physical examination. Subjects were selected from the case loads of clinicians who were not related to this study in order to reduce bias and were stratified according to sex and age to match each AS case.
Blood sampling
Fasting peripheral blood was collected from patients with AS in the morning after an overnight fast for baseline data before sur-
gical treatment and again 2 and 12 weeks after surgical treatment [AVR (aortic valve replacement) or TAVI (transcatheter aortic valve implantation)]. Fasting peripheral blood was also collected from controls in the morning after an overnight fast.
Staining protocol for COPCs
PBMCs (peripheral blood mononuclear cells) were isolated from heparinized blood samples obtained from all sub- jects by Ficoll–Paque density gradient centrifugation. PB- MCs were incubated with FITC-conjugated anti-CD133 mAb (monoclonal antibody) (Miltenyi Biotec), PerCP (peridinin–
chlorophyll protein complex)–Cy5.5 (N,N-dicarboxypentyl- indodicarbocyanine-5,5-disulfonic acid)-conjugated anti-human CD34 mAb (Becton Dickinson), PE (phycoerythrin)-conjugated anti-human KDR (kinase insert domain-containing receptor) mAb (R&D Systems), APC (allophycocyanin)-conjugated anti- human osteocalcin mAb (R&D Systems).
Flow cytometric analysis
Cell enumeration by FACS (Becton Dickinson) was performed immediately after the staining with all samples protected from light. To eliminate clumping, doublet discrimination was util- ized as a part of the FACS procedure. From each sample, a limit of 107 events was established. Events were gated for monocytes, live cells, dead cells and subcellular debris using forward-scattered and side-scattered lights. Live cells were gated for FITC-conjugated CD133-positive and CD34–PerCP–Cy5.5- negative and KDR–PE-positive cells. This subset was gated fur- ther for osteocalcin-positive cells for enumeration of COPCs. The numbers of COPCs among 106cells were counted using a FAC- Scan analyser. Isotype-matched irrelevant control IgG (PerCP, PE or APC) was used as a control (Becton Dickinson).
Osteocalcin levels in COPCs were measured using a FACScan flow cytometer (Becton Dickinson) and shown as MFI (mean fluorescence intensity).
Real-time PCR for ossification-related miRNAs Total RNA including the small RNA fraction was extracted from isolated PBMCs using a mirVanaTM Paris miRNA isolation kit (Ambion), according to the manufacturer’s instructions.
Extracted RNA from isolated COPCs was initially reverse- transcribed using a High Capacity cDNA Archive Kit (Ap- plied Biosystems) and then amplified in a 10μl PCR volume and primer set for amplification of human miR-106a (As- say ID 000578),miR-148a (Assay ID 000470),miR-204 (As- say ID 000508),miR-211(Assay ID 000514),miR-30c(Assay ID 000419), miR-31 (Assay ID 001100), miR-424 (Assay ID 000604) and U6 (Assay ID 001093) using TaqMan® miRNA assays (Applied Biosystems) according to the manufacturer’s re- commended protocol. The amplification steps consisted of denat- uration at 95◦C, followed by 40 cycles of denaturation at 95◦C for 15 s and then annealing at 60◦C for 1 min. All reactions were car- ried out on the 7500 real-time PCR system (Applied Biosystems) using the TaqMan®Universal PCR master mix and Assays on demand (Applied Biosystems). Relative quantification was car- ried out using theCT(threshold cycle) method for recurrent compared with primary with U6 as an endogenous control and
Dysregulation of ossification-related miRNAs in patients with CAVD
fold changes were calculated for each gene [16]. Replicates with CT>40 were excluded. The assay was run in triplicate for each case to allow for assessment of technical variability. To account for PCR amplification of contaminating genomic DNA, a con- trol without reverse transcriptase was included. To improve the accuracy of real-time RT (reverse transcription)–PCR for quan- tification, amplifications were performed in triplicate for each RNA sample.
Transfection with ossification-related miRNA mimic and inhibitor
Cultured PBMCs from five patients with AS (random sampling) were used for anin vitromodel transfected withmiR-106a,miR- 148a,miR-204,miR-211,miR-30c,miR-199a, miR-31ormiR- 424mimic and inhibitor. The protocol for cultured PBMCs was as described previously [9]. For these miRNA mimic and pre- cursor transfections, PBMCs were transfected with pre-miRTM miR-106a, miR-148a, miR-204, miR-211, miR-30c, miR-199a, miR-31ormiR-424precursor molecules (Ambion, 20 ng/ml) and anti-miRTMmiR-106a,miR-148a,miR-204,miR-211,miR-30c, miR-199a,miR-31ormiR-424inhibitors (Ambion, 20 ng/ml) us- ing the NeoFx transfection agent (Ambion). Those cells were used for experiments 24 h after transfection and were exposed at each passage to 0.1μM t-BHP (t-butyl hydroperoxide) (Sigma–
Aldrich) or PBS for an additional 48 h. Levels of these miRNAs and osteocalcin MFI were measured using the above methods.
Multidetector computed tomography imaging for assessment of aortic valve calcification
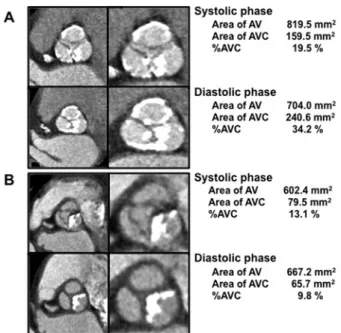
AVC (aortic valve calcification) was quantified from MDCT (multidetector computed tomography) scans according to the method originally described by Clavel et al. [17]. In brief, the degree of AVC was semi-quantitatively classified into no calci- fication and calcification according to the AVC values of 2065 AU (arbitrary units) in men and 1274 AU in women as the cut-off values to define AVC, and was evaluated in aortic valve short axis images at both systolic and diastolic phases [17]. The percent- age of AVC was expressed as a ratio of 100×an area of AVC/a total area of AV. The representative cases of MDCT in patients with severe AVC and moderate AVC are shown in Figure 1. The MDCT images were randomly evaluated by two independent ex- pert observers (K.T. and T.N.) who were blinded to all clinical characteristics.
Statistical analysis
All values are presented as means+−S.D. Kolmogorov–Smirnov analysis was performed to assess data distribution. An unpaired Student’sttest was performed for normally distributed data, and non-parametric Mann–Whitney test was performed where this was not appropriate. Statistical analysis of categorical variables was also carried out using χ2 analysis and Fisher exact ana- lysis. After 2 or 12 weeks of surgical treatments, comparisons between the two groups (AVR or TAVI) were analysed by two- way repeated-measures ANOVA for normally distributed vari- ables. When applicable, significant differences were analysed further with Dunnett’s post-hoc tests. Pearson’s correlation coef- ficients were used to examine the relationship between the num-
Figure 1 Representative cases of multidetector computed tomo- graphy in patients with severe AVC (A) and moderate AVC (B) (A) Echocardiographic findings showed an aortic valve area of 0.68 cm2 and mean aortic gradient of 45 mmHg. (B) Echocardiographic findings showed an aortic valve area of 0.77 cm2and mean aortic gradient of 53 mmHg.
ber of COPCs, miRNAs, osteocalcin protein levels and the de- gree of AVC. A value ofP<0.05 was considered statistically significant.
RESULTS
Baseline and clinical characteristics
Baseline characteristics of the study populations are shown in Table 1. There were no significant differences in age, percentage of males and BMI (body mass index) between the AS group and controls. There were significant differences in other parameters between the two groups (P<0.05) (Table 1). There were sig- nificant differences in some baseline and clinical characteristics between the AVR and TAVI groups (Table 1). The data from echo- cardiography and pressure studies are shown in Table 2. There were no findings of aortic calcification in the controls. There were significant differences in haemodynamic parameters between the AVR and TAVI groups (Table 2).
Numbers of COPCs in AS group and controls The number of COPCs (CD133-positive/CD34-negative/KDR- positive/osteocalcin-positive cells) was higher in the AS group than in the controls (55.0+−14.7 compared with 16.8+−10.8 per 106 events;P<0.01). There was no significant difference in the number of baseline COPCs between the AVR and the TAVI groups (53.6+−12.8 compared with 56.2+−16.5 per 106events;
not significant). In addition, there was no significant difference in the number of baseline COPCs between AS patients with CAD (coronary artery disease) (n=11) and those without CAD
Table 1 Baseline and clinical characteristics of the study population (1) Values are means+−S.D., or number of subjects (percentage).
AS group
Parameters Total (n=46) AVR (n=29) TAVI (n=17) Controls (n=46)
Age (years) 78.7+−7.9 77.6+−8.5 82.7+−3.1* 77.4+−8.1
Male,n(%) 13 (28) 10 (34)† 3 (18)* 14 (28)
BMI (kg/m2) 23.2+−3.7 22.7+−3.2 23.1+−4.5 22.9+−3.2
SBP (mmHg) 130.1+−15.6 132.5+−16.8 127.8+−12.5 130.8+−15.4
DBP (mmHg) 64.9+−12.9 64.1+−12.4 68.0+−12.4 70.4+−12.1
History
Hypertension,n(%) 31 (67)* 20 (70)* 11 (65)* 47 (94)
Diabetes mellitus,n(%) 14 (30)* 11 (38)*† 3 (18)* 13 (25)
Hyperlipidaemian(%) 24 (53)* 19 (66)*† 5 (29)* 26 (78)
Previous CAD,n(%) 11 (22)* 7 (22)* 4 (21)* 16 (44)
Smoking,n(%) 6 (14) 4 (14) 2 (12) 7 (19)
Laboratory findings
Haemoglobin A1c (%) 5.9+−1.2* 6.1+−1.3* 5.8+−1.0* 5.3+−0.4
HDL-C (mg/dl) 52.5+−15.6* 51.0+−13.8* 54.0+−17.3* 64.0+−19.3
LDL-C (mg/dl) 105.3+−30.2* 107.7+−33.2* 102.9+−27.1* 93.1+−26.8 Triacylglycerols (mg/dl) 101.6+−61.3 110.3+−67.3 75.9+−26.1 132.7+−80.6
hsCRP (mg/dl) 0.40+−0.24* 0.39+−0.26 0.41+−0.23 0.11+−0.12
Creatine (mg/dl) 0.79+−0.23 0.78+−0.27 0.81+−0.21 0.73+−0.15
BNP (pg/ml) 286.1+−281.5* 294.9+−281.7 357.5+−341.2 80.2+−65.7 Medication
ACEI/ARB,n(%) 16/22 (83)* 10 / 16 (90)*† 6 / 6 (71)* 7 / 10 (39)
Beta-blockers,n(%) 15 (32) 10 (34) 5 (29) 14 (31)
Calcium antagonists,n(%) 17 (36) 14 (48)*† 3 (18)* 18 (39)
Diuretics,n(%) 6 (14)* 4 (14)* 2 (12)* 3 (7)
ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; BMI, body mass index; BNP, brain natriuretic peptide; CAD, coronary artery disease; DBP, diastolic blood pressure; HDL-C, high-density lipoprotein-cholesterol; hsCRP, high-sensitivity C-reactive protein; LDL-C, low-density lipoprotein- cholesterol; SBP, systolic blood pressure; TAVI, transcatheter aortic valve implantation. *P<0.05 compared with controls. †P<0.05 compared with TAVI group.
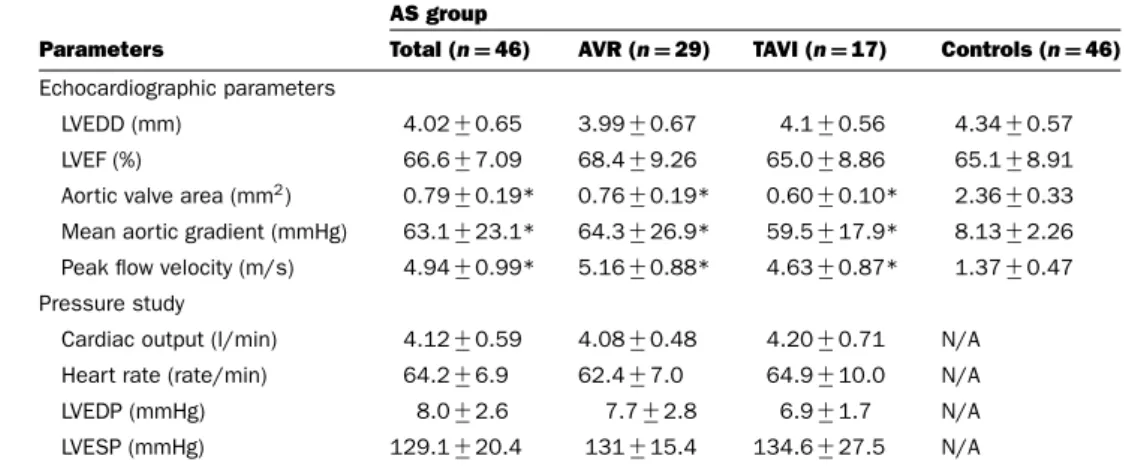
Table 2 Baseline and clinical characteristics of the study population (2) Values are means+−S.D., or number of subjects.
AS group
Parameters Total (n=46) AVR (n=29) TAVI (n=17) Controls (n=46) Echocardiographic parameters
LVEDD (mm) 4.02+−0.65 3.99+−0.67 4.1+−0.56 4.34+−0.57
LVEF (%) 66.6+−7.09 68.4+−9.26 65.0+−8.86 65.1+−8.91
Aortic valve area (mm2) 0.79+−0.19* 0.76+−0.19* 0.60+−0.10* 2.36+−0.33 Mean aortic gradient (mmHg) 63.1+−23.1* 64.3+−26.9* 59.5+−17.9* 8.13+−2.26 Peak flow velocity (m/s) 4.94+−0.99* 5.16+−0.88* 4.63+−0.87* 1.37+−0.47 Pressure study
Cardiac output (l/min) 4.12+−0.59 4.08+−0.48 4.20+−0.71 N/A Heart rate (rate/min) 64.2+−6.9 62.4+−7.0 64.9+−10.0 N/A
LVEDP (mmHg) 8.0+−2.6 7.7+−2.8 6.9+−1.7 N/A
LVESP (mmHg) 129.1+−20.4 131+−15.4 134.6+−27.5 N/A
LVEDD, left ventricular end-diastolic diameter; LVEDP, left ventricular end-diastolic pressure; LVEF, left ventricular ejection fraction; LVESP, left ventricular end-systolic pressure; N/A, not available. *P<0.05 compared with controls.
Dysregulation of ossification-related miRNAs in patients with CAVD
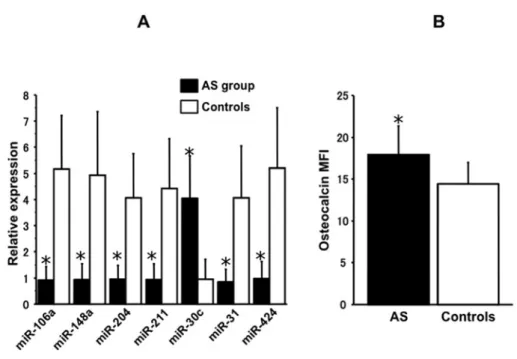
Figure 2 Levels of ossification-related miRNAs (A) and osteocalcin MFI (B) in AS group and controls
*P<0.01 compared with controls.
(n=35) (57.1+−16.8 compared with 55.0+−14.6 per 106events;
not significant).
Levels of ossification-related miRNAs and osteocalcin in AS group and controls
There was no difference in average CT of U6 between the AS group and the controls (26.8+−2.3 compared with 27.9+−1.9; not significant). Levels of miR-30cwere higher in the AS group than in controls (4.05+−1.62 compared with 0.96+−0.76; P<0.01) (Figure 2A). Levels ofmiR-106a, miR- 148a, miR-204, miR-211, miR-31 and miR-424 were lower in the AS group than in the controls (miR-106a, 0.92+−0.53 compared with 5.17+−2.05; P<0.01; miR-148a, 0.94+−0.61 compared with 4.93+−2.44; P<0.01; miR-204, 0.95+−0.53 compared with 4.07+−1.68; P<0.01; miR-211, 0.92+−0.62 compared with 4.43+−1.91;P<0.01;miR-31, 0.84+−0.50 com- pared with 4.07+−1.97; P<0.01; miR-424, 0.97+−0.66 com- pared with 5.20+−2.31;P<0.01 (Figure 2A). Osteocalcin MFI was higher in the AS group than in the controls (17.59+−3.52 compared with 14.53+−2.89; P<0.01) (Figure 2B). There were no significant differences in levels of ossification-related miRNAs and osteocalcin MFI between AS patients with CAD and those without CAD (miR-106a, 0.68+−0.44 compared with 0.94+−0.53;miR-148a, 0.82+−0.46 compared with 0.99+−0.67;
miR-204, 0.86+−0.56 compared with 1.00+−0.56; miR-211, 1.13+−0.68 compared with 0.91+−0.60; miR-31, 0.61+−0.25 compared with 0.90+−0.56; miR-424, 0.89+−0.48 compared with 1.08+−0.63; osteocalcin MFI, 18.35+−3.97 compared with 17.67+−3.42 not significant).
Levels ofmiR-30awere positively correlated with the num- ber of COPCs and osteocalcin MFI. On the other hand, levels of miR-106a,miR-148a,miR-204,miR-211,miR-31andmiR-424 were negatively correlated with the number of COPCs and os-
Table 3 Correlation between osteocalcin MFI, number of COPCs and ossification-related miRNAs
Osteocalcin MFI Number of COPCs
r Pvalue r Pvalue
miR-106a −0.45 <0.01 −0.075 <0.01 miR-148a −0.47 <0.01 −0.070 <0.01 miR-204 −0.42 <0.01 −0.68 <0.01 miR-211 −0.41 <0.01 −0.71 <0.01 miR-30c 0.48 <0.01 0.79 <0.01 miR-31 −0.43 <0.01 −0.075 <0.01 miR-424 −0.42 <0.01 −0.065 <0.01
teocalcin MFI (Table 3). The number of COPCs and levels of miR-106a,miR-148a,miR-204,miR-211,miR-30c,miR-31and miR-424were statistically correlated with haemodynamic pro- files including aortic valve area, mean aortic gradient and peak flow velocity (Table 4). The degree of AVC was weakly positively correlated withmiR-30clevels and negatively correlated with miR-106aand miR-424 levels (miR-30ccompared with AVC, r=0.48,P<0.01; miR-106acompared with AVC,r= −0.43, P<0.05;miR-148acompared with AVC,r= −0.29,P= 0.11;
miR-204 compared with AVC,r= −0.10, P= 0.60; miR-211 compared with AVC,r= −0.21,P= 0.24; miR-31compared with AVC,r= −0.23,P= 0.21;miR-424compared with AVC, r= −0.43,P<0.05).
Changes in COPCs and ossification-related miRNAs after surgical treatment
The number of COPCs and osteocalcin MFI were decreased 2 and 12 weeks after AVR or TAVI (Figures 3A and 3B). The
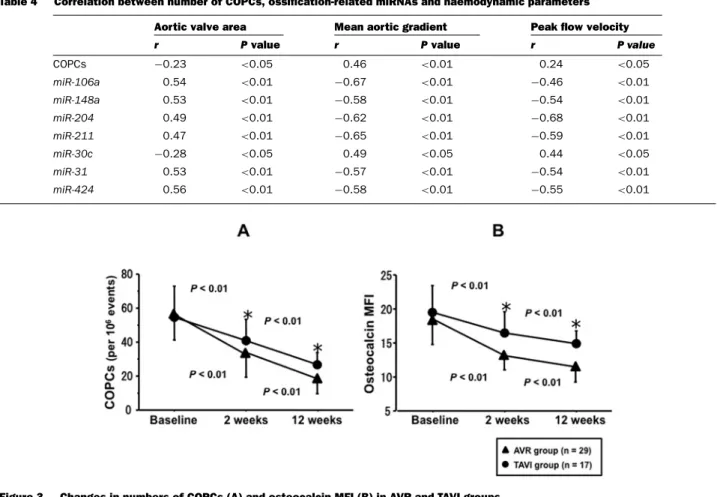
Table 4 Correlation between number of COPCs, ossification-related miRNAs and haemodynamic parameters Aortic valve area Mean aortic gradient Peak flow velocity
r Pvalue r Pvalue r P value
COPCs −0.23 <0.05 0.46 <0.01 0.24 <0.05
miR-106a 0.54 <0.01 −0.67 <0.01 −0.46 <0.01
miR-148a 0.53 <0.01 −0.58 <0.01 −0.54 <0.01
miR-204 0.49 <0.01 −0.62 <0.01 −0.68 <0.01
miR-211 0.47 <0.01 −0.65 <0.01 −0.59 <0.01
miR-30c −0.28 <0.05 0.49 <0.05 0.44 <0.05
miR-31 0.53 <0.01 −0.57 <0.01 −0.54 <0.01
miR-424 0.56 <0.01 −0.58 <0.01 −0.55 <0.01
Figure 3 Changes in numbers of COPCs (A) and osteocalcin MFI (B) in AVR and TAVI groups
*P<0.01 compared with TAVI group.
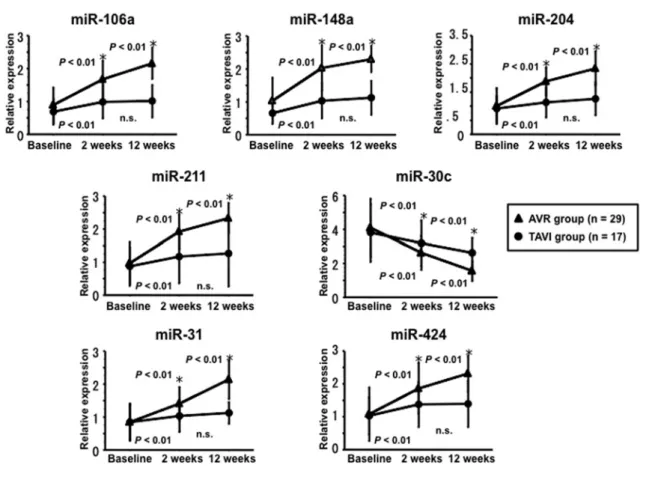
AVR group showed decreasedmiR-30clevels 2 and 12 weeks after AVR and increased levels of miR-106a, miR-148a,miR- 204,miR-211,miR-199a,miR-31andmiR-4243 and 12 weeks after AVR (Figure 4). The TAVI group showed decreasedmiR-30c levels 2 weeks after AVR and increased levels of the remaining miRNAs 2 weeks after AVR, whereas levels of these miRNAs did not change 12 weeks after TAVI (Figure 4). Fold changes in the number of COPCs, osteocalcin MFI and ossification-related miRNA levels were higher in the AVR group than in the TAVI group (Figure 4).
Cultured PBMCs transfected with
ossification-related miRNA mimic and inhibitor Cultured PBMCs were transfected with ossification-related miRNA mimic and inhibitor followed by challenge with t-BHP after 48 h. Levels ofmiR-106a, miR-148a,miR-204, miR-211, miR-30c, miR-31and miR-424 expression were higher in the mimic-transfected cells than in the mock-transfected cells (Fig- ure 5A). On the other hand, levels ofmiR-106a,miR-148a,miR- 204, miR-211,miR-30c,miR-31andmiR-424 expression were lower in the inhibitor-transfected PBMCs than in the mock- transfected PBMCs (Figure 5A). Cultured PBMCs transfected withmiR-106a,miR-148a,miR-204,miR-211,miR-199a,miR- 31andmiR-424mimic showed a reduction in levels of osteocalcin
MFI compared with mock-transfected cells (Figure 5B). PBMCs transfected withmiR-106a,miR-148a,miR-204,miR-211,miR- 199a,miR-31andmiR-424inhibitor showed an increase in levels of osteocalcin MFI compared with mock-transfected cells (Fig- ure 5B). On the other hand, PBMCs transfected withmiR-30c mimic showed an increase in levels of osteocalcin MFI compared with mock-transfected cells (Figure 5B). PBMCs transfected with miR-30cinhibitor showed a decrease in levels of osteocalcin MFI compared with mock-transfected cells (Figure 5B).
DISCUSSION
The main findings of the present study are: (i) the number of COPCs was higher in the AS group than in controls; (ii) levels of ossification-related miRNAs were shown to differ between the AS group and controls and to be statistically correlated with the number of COPCs; (iii) surgical treatment with TAVI or AVR generated markedly changed levels of ossification-related miRNAs and number of COPCs; and (iv)in vitrostudy showed that ossification-related miRNAs resulted in negative or positive regulation of osteocalcin maturation.
The cellular origin of ectopic AVC has been unclear for a long time, despite this being considered to be a major cause
Dysregulation of ossification-related miRNAs in patients with CAVD
Figure 4 Changes in ossification-related miRNAs in AVR and TAVI groups
*P<0.01 compared with controls.
of CAVD. Some reports have shown that COPCs were released from bone marrow and then recaptured into the bone microenvir- onment [3,18]. It has also been reported that COPCs which are osteocalcin-, bone alkaline phosphate- or type I collagen-positive PBMCs participate in ectopic osteogenic injury responses during fracture and valve ossification [4,19]. We have shown an increase in the number of COPCs exhibiting positive CD133, KDR and osteocalcin and negative CD34 in patients with AS compared with controls. In addition, the number of COPCs is positively correlated with the degree of AVC. It has been reported that an increase in COPCs is associated with unstable CAD and tends to predict further events [20]. However, there were no significant differences in the number of COPCs between AS patients with CAD and those without CAD. It has been speculated that a surge of COPCs may be released from bone marrow in response to aortic calcification. In agreement with our results, it has been reported that a high number of COPCs was associated with the severity of AS [6]. It has also been reported that COPCs (type I collagen-positive/CD45-positive) appear in human aortic valves during several phases of AS including the fibroproliferative and neovascularization phases [5]. These observations suggest that an increase in the number of COPCs may be involved in the progression of AVC.
Accumulating evidence suggests that some ossification- related miRNAs, such asmiR-106a,miR-148a,miR-204,miR- 211, miR-30c, miR-31and miR-424 are involved in the pro-
cess of heterotopic ossification modulating osteogenesis via up-regulation or down-regulation of these ossification-related miRNAs [11,13,14]. The present study demonstrates up- regulation ofmiR-30clevels and down-regulation ofmiR-106a, miR-148a,miR-204,miR-211,miR-31andmiR-424levels in pa- tients with AS compared with controls. Overexpression ofmiR- 30cinduces heterotopic ossification in mesenchymal stem cells via expression of several osteogenic mediators, such as ITGB1 (integrinβ1), CXCL12 (CXC chemokine ligand 12), FLT1 (Fms- like tyrosine kinase-1), CAMTA1 (calmodulin-binding transcrip- tion activator 1) or COL9A3 (collagen type IX alpha 3), and therefore acts as a positive regulator of osteogenesis [12,13].
On the other hand, it has been reported that miR-106a, miR- 148a, miR-204, miR-211, miR-199a, miR-31and miR-424act as negative mediators of osteogenesis via repression of several osteogenic mediators, such as RUNX2 (Runt-related transcrip- tion factor 2), BMPR2 (bone morphogenetic protein receptor type 2), CBFB (core-binding factor beta), BMP2 (bone morpho- genetic protein 2), BMP3 and BMP8B [12,13]. The present study has also shown that osteocalcin levels were higher in the AS group than in controls, and osteocalcin levels and AVC were correlated with levels of ossification-related miRNAs. Osteo- blasts produce osteocalcin and incorporate it into the bone matrix [21]. Osteocalcin is released into the circulation from the mat- rix during bone resorption and is considered a marker of bone turnover [21]. Ourin vitro study showed gain-of-function and
Figure 5 Levels of ossification-related miRNAs and osteocalcin in PBMCs transfected with ossification-related miRNA mimic and inhibitor
(A) Comparison of ossification-related miRNA levels between PBMCs transfected with ossification-related miRNA mimic and inhibitor. (B) Comparison of osteocalcin protein levels between PBMCs transfected with ossification-related miRNA mimic and inhibitor. *P<0.01 compared with mock.
loss-of-function approaches to ossification-related miRNAs, and transfection of each ossification-related miRNA into cultured PB- MCs resulted in regulation of osteocalcin expression, suggesting that these ossification-related miRNAs may play an important role in osteocalcin maturation. These observations suggest that abnormal profiling of ossification-related miRNAs may play an important role in osteogenesis in patients with AS. In addition, the present study shows that the degree of AVC is positively correl- ated withmiR-30clevels and negatively correlated withmiR-106a andmiR-424levels in patients with AS. It may be a novel find- ing that dysregulated profiling of ossification-related miRNAs is related to the degree of AVC. It has therefore been suggested that dysregulated profiling of ossification-related miRNAs may be involved in the progression of aortic calcification in patients with AS. Although the present study has not evaluated the effect of medications such as statins on aortic calcification in patients with AS, a recent study has demonstrated that oxLDL (oxidized low-density lipoprotein) increased the valve calcification-related signalling pathway by increasing extracellular bone matrix pro- tein, and atorvastatin also prevented any oxLDL-induced effects through the same pathway [22]. Further study will be needed to clarify the mechanism by which other miRNAs dysregulate osteogenesis in AVC among patients with AS.
Another important finding of the present study was thatmiR- 106a,miR-148a,miR-204,miR-211,miR-199a,miR-31andmiR- 424levels increased after surgical treatment with TAVI or AVR.
On the other hand,miR-30clevels and the number of COPCs were reduced after surgical treatment. There have been no reports con-
cerning the effect of surgical treatment on ossification-related miRNA expression and COPC count. From these observations, it may be speculated that surgical treatment ameliorated CAV by activating valvular endothelial cells and inflammatory cells and releasing the aortic pressure gradient of AS, and then termin- ating the osteogenic processes via dysregulation of ossification- related miRNAs. The present study has also shown that changes in ossification-related miRNA levels, the number of COPCs and osteocalcin MFI after surgical treatment were greater in the AVR group than in the TAVI group. This result may be explained by procedural differences between AVR and TAVI. Although AVR eliminated CAVD completely, TAVI left residual CAVD tissue around the artificial cardiac valve after the procedure, which may continue to activate the osteogenic process via dysregulation of ossification-related miRNAs. It is therefore suggested that TAVI may not terminate the process of osteogenesis completely. These observations suggest that the remaining COPCs and miR-30c after TAVI may be related to the progression of biological valve sclerosis and result in a worsening of long-term prognosis. It is also speculated that an increase in COPCs via dysregulation of ossification-related miRNAs may play an important role as a poor prognostic factor in severe AS patients without AVR or TAVI.
Bioprosthetic valve degeneration is a major complication after the implantation of biological prosthetic valves [23]. It has been reported that the incidence of structural valve degeneration was 3.6 % at 6 years and 5 % at 10 years after implantation [24].
A study involving microscopic analysis of explanted biopros- thetic heart valves revealed the presence of moderate to severe
Dysregulation of ossification-related miRNAs in patients with CAVD
calcification as well as CAVD [25]. A pathological study has demonstrated that bioprosthetic tissue valve calcification was similar to that of native valves [26]. These reports suggest that the osteogenic processes via dysregulation of ossification-related miRNAs may be involved in the pathogenesis of bioprosthetic valve degeneration. Further long-term follow-up studies will therefore be required.
CLINICAL PERSPECTIVES
• The osteogenic processes are involved in mechanisms in CAVD. Ossification-related miRNAs may play an important role in osteogenic differentiation from bone marrow stromal cells and the osteogenic processes in CAVD.
• The present study has suggested that dysregulation of ossification-related miRNAs such as miR-106a, miR-148a, miR-204,miR-211, miR-30a, miR-31and miR-424 may be related to differentiation into COPCs and thereby play an im- portant role in the pathogenesis of CAVD.
• Levels of ossification-related miRNAs and COPCs count were changed by surgical treatments and may be novel post- operative biomarkers.
AUTHOR CONTRIBUTION
The study was designed and conducted by Kan Takahashi, Yuji Takahashi, Mamoru Satoh and Yoshihiro Morino. Data analysis was performed by Kan Takahashi, Takuya Osaki, Takahito Nasu, Makiko Tamada, Motoyuki Nakamura and Yoshihiro Morino. The paper was written by Kan Takahashi, Mamoru Satoh and Yoshihiro Morino.
FUNDING
This study was supported by a Grant-in-Aid for General Scientific Research from the Japanese Ministry of Education, Science, Sports and Culture [grant number 25461138].
REFERENCES
1 Freeman, R.V. and Otto, C.M. (2005) Spectrum of calcific aortic valve disease: pathogenesis, disease progression, and treatment strategies. Circulation111, 3316–3326 CrossRef PubMed
2 Rajamannan, N.M., Evans, F.J., Aikawa, E., Grande-Allen, K.J., Demer, L.L., Heistad, D.D., Simmons, C.A., Masters, K.S., Mathieu, P., O’Brien, K.D. et al. (2011) Calcific aortic valve disease: not simply a degenerative process. Circulation124, 1783–1791CrossRef PubMed
3 Mohler, 3rd, E.R., Kaplan, F.S. and Pignolo, R.J. (2012) Boning-up on aortic valve calcification. J. Am. Coll. Cardiol.60, 1954–1955CrossRef PubMed
4 Egan, K.P., Kim, J.H., Mohler, 3rd. E.R. and Pignolo, R.J. (2011) Role for circulating osteogenic precursor cells in aortic valvular disease. Arterioscler. Thromb. Vasc. Biol.31, 2965–2971 CrossRef PubMed
5 Khosla, S. and Eghbali-Fatourechi, G.Z. (2006) Circulating cells with osteogenic potential. Ann. N.Y. Acad. Sci.1068, 489–497 CrossRef PubMed
6 G¨ossl, M., Khosla, S., Zhang, X., Higano, N., Jordan, K.L., Loeffler, D., Enriquez-Sarano, M., Lennon, R.J., McGregor, U., Lerman, L.O. and Lerman, A. (2012) Role of circulating osteogenic progenitor cells in calcific aortic stenosis. J. Am. Coll.
Cardiol.60, 1945–1953CrossRef PubMed
7 Bartel, D.P. (2004) MicroRNAs: genomics, biogenesis, mechanism, and function. Cell116, 281–297 CrossRef PubMed
8 Kim, V.N. (2005) Small RNAs: classification, biogenesis, and function. Mol. Cells19, 1–15CrossRef PubMed
9 Tabuchi, T., Satoh, T., Itoh, M. and Nakamura, T. (2012) MicroRNA-34a regulates the longevity-associated protein SIRT1 in coronary artery disease: effect of statins on SIRT1 and microRNA-34a expression. Clin. Sci. (Lond.)123, 61–81 CrossRef
10 Satoh, M., Takahashi, Y., Tabuchi, T., Tamada, M., Takahashi, K., Itoh, T., Morino, Y. and Nakamura, M. (2015) Circulating Toll-like receptor 4-responsive microRNA panel in patients with coronary artery disease: results from prospective and randomized study of treatment with renin–angiotensin system blockade. Clin. Sci.
(Lond.)128, 483–491CrossRef PubMed
11 Huang, J., Zhao, L., Xing, L. and Chen, D. (2010) MicroRNA-204 regulates Runx2 protein expression and mesenchymal progenitor cell differentiation. Stem Cells28, 357–364 PubMed
12 Li, Z., Hassan, M.Q., Volinia, S., van Wijnen, A.J., Stein, J.L., Croce, C.M., Lian, J.B. and Stein, G.S. (2008) A microRNA signature for a BMP2-induced osteoblast lineage commitment program. Proc. Natl. Acad. Sci. U.S.A.105, 13906–13911 CrossRef PubMed
13 Vimalraj, S. and Selvamurugan, N. (2014) MicroRNAs expression and their regulatory networks during mesenchymal stem cells differentiation toward osteoblasts. Int. J. Biol. Macromol.66, 194–202CrossRef PubMed
14 Bagl`ıo, S.R., Devescovi, V., Granchi, D. and Baldini, N. (2013) MicroRNA expression profiling of human bone marrow mesenchymal stem cells during osteogenic differentiation reveals Osterix regulation by miR-31. Gene527, 321–331 CrossRef PubMed
15 Nishimura, R.A., Otto, C.M., Bonow, R.O., Carabello, B.A., Erwin, 3rd, J.P., Guyton, R.A., O’Gara, P.T., Ruiz, C.E., Skubas, N.J., Sorajja, P. et al. (2014) 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol.63, e57–e185CrossRef PubMed
16 Livak, KJ. and Schmittgen, T.D. (2001) Analysis of relative gene expression data using real-time quantitative PCR and the 2−CT method. Methods25, 402–408CrossRef PubMed
17 Clavel, M.A., Pibarot, P., Messika-Zeitoun, D., Capoulade, R., Malouf, J., Aggarval, S., Araoz, P.A., Michelena, H.I., Cueff, C., Larose, E. et al. (2014) Impact of aortic valve calcification, as measured by MDCT, on survival in patients with aorticstenosis:
results of an international registry study. J. Am. Coll. Cardiol.64, 1202–1213CrossRef PubMed
18 Sacchetti, B., Funari, A., Michienzi, S., Di, Cesare, S., Piersanti, S., Saggio, I., Tagliafico, E., Ferrari, S., Robey, P.G., Riminucci, M.
and Bianco, P. (2007) Self-renewing osteoprogenitors in bone marrow sinusoids can organize a hematopoietic
microenvironment. Cell131, 324–336CrossRef PubMed 19 Eghbali-Fatourechi, G.Z., Lamsam, J., Fraser, D., Nagel, D., Riggs,
B.L. and Khosla, S. (2005) Circulating osteoblast-lineage cells in humans. N. Engl. J. Med.352, 1959–1966CrossRef PubMed 20 Flammer, A.J., G¨ossl, M., Widmer, R.J., Reriani, M., Lennon, R.,
Loeffler, D., Shonyo, S., Simari, R.D., Lerman, L.O., Khosla, S.
and Lerman, A. (2012) Osteocalcin positive
CD133+/CD34−/KDR+progenitor cells as an independent marker for unstable atherosclerosis. Eur. Heart J.33, 2963–2969CrossRef PubMed
21 Delmas, P.D., Eastell, R., Garnero, P., Seibel, M.J. and Stepan, J.
(2000) The use of biochemical markers of bone turnover in osteoporosis. Osteoporos. Int.11(Suppl. 6), S2–S17 CrossRef PubMed
22 Rajamannan, N.M. (2015) Atorvastatin attenuates bone loss and aortic valve atheroma in LDLR mice. Cardiology132, 11–15 CrossRef PubMed
23 Van Geldorp, M.W.A., Jamieson, E., Kappetein, P., Ye, J., Fradet, G.J., Eijkemans, M.J.C., Grunkemeier, G.L., Bogers, A. and Takkenberg, J. (2009) Patient outcome after aortic valve replacement with a mechanical or biological prosthesis: weighing lifetime anticoagulant-related event risk against reoperation risk.
J. Thorac. Cardiovasc. Surg.137, 881–886CrossRef PubMed
24 Joshi, V., Prosser, K. and Richens, D. (2014) Early prosthetic valve degeneration with Mitroflow aortic valves: determination of incidence and risk factors. Interact. Cardiovasc. Thorac. Surg.
19, 36–40CrossRef PubMed
25 Butany, J., Feng, T., Luk, A., Law, K., Suri, R. and Nair, V. (2011) Modes of failure in explanted Mitroflow pericardial
valves. Ann. Thorac. Surg.92, 1621–1627 CrossRef PubMed
26 Skowasch, D., Steinmetz, M., Nickenig, G. and Bauriedel, G.
(2006) Is the degeneration of aortic valve bioprostheses similar to that of native aortic valves? Insights into valvular pathology. Expert Rev. Med. Devices3, 453–462 CrossRef PubMed
Received 9 February 2016/16 March 2016; accepted 13 April 2016 Accepted Manuscript online 14 April 2016, doi: 10.1042/CS20160094