Actual Nursing Practice by Proficient Nurses
for Elderly M yocardial Infarction Patients
and Problems with Self-Care
Mayumi Ito
and Hisako Kamata
Purpose: The study was conducted to ascertain what was actually done for elderly myocardial infarction (hereafter MI)patients by proficient nurses and to identify problems with self-care that they encountered in their daily nursing practice. M ethods: A focus-group interview was carried out on proficient nurses in two hospitals. The interview was recorded and later transcribed for inductive qualitative analysis. Results: Content-wise problems with self-care that proficient nurses encountered in their nursing care were related to the issues of a low-salt diet,medication management,and activities,whereas method-wise problems were related to the issues of a decline in understanding and cognitive abilities,family functions, and continuity of nursing. The major place of nursing for patients was the hospital ward (treatment right after MI). Out of the features categorized into 15 extracted from my preceding study,the categories that were frequently confirmed by both groups were: Patients anxiety about recurrence, Reduction in the level and scope of activities, and Observation of the process up to coronary angiography after leaving hospital. This study added three categories as to issues in continuous nursing. Conclusions: In order to cope with difficulties in supporting elderly patients who had self-care problems in a limited period of hospitalization, important were the continuity of nursing in the ward, the outpatient depart-ment and a hospital stay for examination, and coordination with people in other domains such as registered dieticians and pharmacists.(Kitakanto Med J 2011;61:319∼326)
Key words: elderly person, myocardial infarction, social activity, proficient nurse, focus group interviews
I. Introduction
Together with a prolonged average life expectancy and declining birth rates, Japanese society has been increasingly aging. An expanding elderly population results in an increase in the number of elderly people who receive medical treatment. It is estimated that 3.6% of elderly people get hospitalized and 11.9% visit hospitals.
On the other hand, an increase in elderly popula-tion and a subsequent growth in the elderly people who receive medical treatment have inevitably expand-ed a population of elderly people who are in the neexpand-ed of social care services. The number of elderly persons who have been confirmed that they need social care
services under the care insurance system enforced in 2000 has sharply risen from 2.8 million people at the outset to 4.2 million people, i.e. 16% of an elderly population. The leading causes that have put them in conditions in the need of care services include cerebrovascular disease, dementia and bone/joint dis-orders which are followed by heart diseases. The Comprehensive Survey of Living Conditions of People on Health and Welfare reports that circulatory diseases including high blood pressure, heart diseases and cerebrovascular diseases ranked high as diseases that affect daily living among hospital visitors.
The administration of reperfusion therapy such as percutaneous coronary intervention, an improvement in emergency transportation systems, and the wide-1 School of Nursing, Faculty of Health Science, Gunma Paz College, wide-1-7-wide-1 Tonya-machi, Takasaki, Gunma 370-0006, Japan 2 Department of Nutrition and Nursing, Faculty of Health Care, Kiryu University, 606-7 Azami, Kasakake-machi, Midori, Gunma 379-2392, Japan
Received : May 20, 2011
Address: MAYUMI ITO School of Nursing,Faculty of Health Science,Gunma Paz College,1-7-1 Tonya-machi,Takasaki,Gunma 370-0006, Japan
spread use of CCU have contributed to a recent drop in the in-hospital mortality rate of acute myocardial infarctions to approximately 7%. Nonetheless, the mortality rate from myocardial infarction before hospi-tal arrival accounts for 14% of tohospi-tal myocardial infarc-tion patients. It is,therefore,estimated that the death rate during the acute phase of a myocardial infarction is still more than 20% today, and it is reported that an attack of myocardial infarction is an experience in which a person becomes acutely aware of his/her death.
The rehabilitation program for myocardial infarc-tions is divided into three stages, an acute phase from attack to release from hospital, recovery phase after leaving hospital, and maintenance phase after social rehabilitation. In 1983 A study on the development of rehabilitation system for heart diseases introduced an acute phase program of four weeks. Thereafter,in 1996 A study on the rehabilitation system for heart diseases proposed a short-term program of three weeks,being followed by the Guidelines on rehabili-tation for cardiovascular diseases of 2007 that put forward a two-week program, thereby making it pos-sible to discharge patients quickly after the onset. By shortening a period of hospitalization,the significance of recovery phase rehabilitation after leaving hospital has increased. However,Japan markedly lags behind in developing outpatient cardiac rehabilitation systems due primarily to problems with health insurance sys-tems, establishment of facilities and human resources development, which causes elderly patients who live at home with a heart disease serious problems from the viewpoint of maintaining the quality of life after leav-ing hospital, as pointed out by a study.
In many cases a myocardial infarction begins with sudden and intense chest pains. Hence, the patient has a gloomy foreboding that I m going to die, thereby frequently leaving an inerasable anxiety and fear in the patient and his/her family. Also it is reported that even the patients who leave hospital after a satisfactory process of recovery harbor anxiety about their lives in general and the expansion of their activ-ities after leaving hospital and that they suffer from psychological deterioration and stress. It is also reported,on the other hand,that even psychologically stable patients finally regain a sense of control over their feelings after various conflicts and processes.
The past studies on nursing for myocardial infarc-tion patients primarily focused on support to acute phase rehabilitation in hospital and education for patients. There are recent studies on,for example,the preparation and enforcement of a comprehensive clini-cal pathway including treatment, nursing care, and education in hospital in conformity to the
Guide-lines on rehabilitation for cardiovascular diseases and evaluation of a six months intervention study on outpatients. However,all these studies were carried out on middle-aged patients, and studies on elderly patients are limited only to the relationship between acute phase rehabilitation and physical functions and heart failure.
As to how nursing care should be and the methods with focus on the features of elderly myocardial infarc-tion patients who regularly visit the cardiology out-patient department, there are only a few practical reports on the recovery phase of rehabilitation,where-by validation still remains to be done.
II. Purposes
1. The study was conducted to ascertain what was actually done in nursing care for elderly myocar-dial infarction patients by proficient nurses work-ing in the cardiology ward and outpatient depart-ment and to identify problems with self-care that they encountered in their daily nursing practice. 2. The study was to verify through proficient nurses
the fifteen features of elderly myocardial infarc-tion patients extracted from previous case study.
III. M ethods
1. Sample populationThe population consisted of eight nurses working in the cardiology ward and outpatient department in hospital B and seven nurses working in hospital C, both of which have a cardiology ward and outpatient department located in prefecture A. These two hospi-tals are the core hospihospi-tals in the treatment of myocar-dial infarctions at acute phase in prefecture A. They are always ready to treat emergency cardiovascular disease patients and provide high quality specialized treatment and nursing care from acute phase to chronic phase.
The participating nurses were adequately experi-enced in nursing in cardiology and assumed leading positions in the ward and the outpatient department. I asked the head nurses of the ward and outpatient department to select the participants. The yardstick for selection was the fourth level of Benners five levels of clinical pragmatic abilities/skills of nurses. That is, nurses of the proficient level or above con-stituted the sample population.
Fourth level: A proficient-level nurse has the ability to have an overall grasp instead of a situational grasp based on a practical understanding,and his/her performance focuses on the core issue.
2. M ethods
method is characterized by two features: first, the researcher explores specific experiences of clinical nurses, and second, the interviewee narrates his/her bare experiences that he/she has undergone. The researcher led the interview to get responses from its participants.
3. Content
An interview guide was prepared to expound nursing scenes in which nurses provided care to elderly myocardial infarction patients and identify problems with self-care that they encountered in their daily nursing practice. The interview was conducted on the condition that it would focus only on the patients who underwent a normal process.
As to the second purpose to confirm the features, the interview guide excluded expressions about the 15-category features presented in previous study to prevent the participants from having preconceived ideas.
The contents of the interview guide include: (1) As to the problems with living daily lives after the
first myocardial infarction, what, when and how do they happen? Under such circumstances, when and what types of nursing care is provided to the patient? What is the result?
(2) Are there any differences in life and nursing methods among middle-aged patients, elderly patients of the same myocardial infarction? If so, what are the differences?
(3) Are any elderly myocardial infarction patients who have left strong impressions through their clinical experiences? What are the features of such cases?
(4) What types of continuous nursing care will be necessary, based on experiential knowledge learned from cases and practices, in order to sup-port the living of elderly myocardial infarction? As the basic data of the nurses who participated in the interview, I had collected data on age, sex, basic/ professional education on nursing, position, years of nursing experience, and years of nursing experience in cardiology.
As to the definition of super-elderly used in this interview, first, I asked each nurses perception on the age of the elderly. It was confirmed that the nurses of both groups shared the perception that the elderly are persons in their late 70s. This perception coin-cides with the result of the preceding study. Hence, in subsequent studies,super-elderly patients aged 75 or over have been referred to as the elderly.
The duration of the interview was 80 minutes in hospital A and 60 minutes in hospital B.
4. Analysis
The interviews were recorded and later transcribed with prior consent. The contents were put to induc-tive qualitainduc-tive analysis.
Analytical procedures (1) About the first purpose
①Data obtained through the interviews were grouped into the following categories.
i . Nursing care and considerations provided particularly to elderly patients
ii. Where the above services in i. were provided (hospital ward - treatment right after the attack, outpatient department, and hospital say for examination)
iii. Features of elderly patients
iv. Difficulties in nursing elderly patients and their reasons
② The content of nursing care was grouped based on commonality.
③ The data of the growped content of nursing care (②) are classified by the category, method and other.
④ The categorized data were further grouped by the ward (treatment right after the attack), the out-patient department,and a hospital stay for exami-nation
⑤As to the features of and difficulties about elderly patients, the data concerning acute phase treat-ment were excluded.
⑥ Similar contents were classified as a cluster and described as issues specific to elderly patients (2) About the second purpose
① The data obtained through the interviews were perused in comparison to the 15-category features. ② The content applicable to each feature was
con-firmed and reconcon-firmed.
③A feature that has been confirmed twice was classified as the feature confirmed,and the number of confirmation was checked.
In order to verify the analytical results, I asked each interview participant for their confirmation and also a geriatric nursing researcher and two supervisors of departmental head nurses in the cardiology ward (the fifth level of the five levels in clinical practical abilities, that is, the expert level nurse classified by Benner for their evaluation.
Fifth level=Expert : Through accumulated experiences and expertise, he/she is able to solve problems appropriately with practical wisdom in each situation.
5. Ethical considerations
approval from the Gunma PAZ College Ethics Com-mittee.
I explained the interview participants about its purposes and assured in writing that I would protect and keep in complete confidentiality the content of the interview, patients information provided in the inter-view and personal information of each nurse when the study is published. I also confirmed the principle of voluntary participation in the interview. I received an agreement signed by each participant.
IV. Results
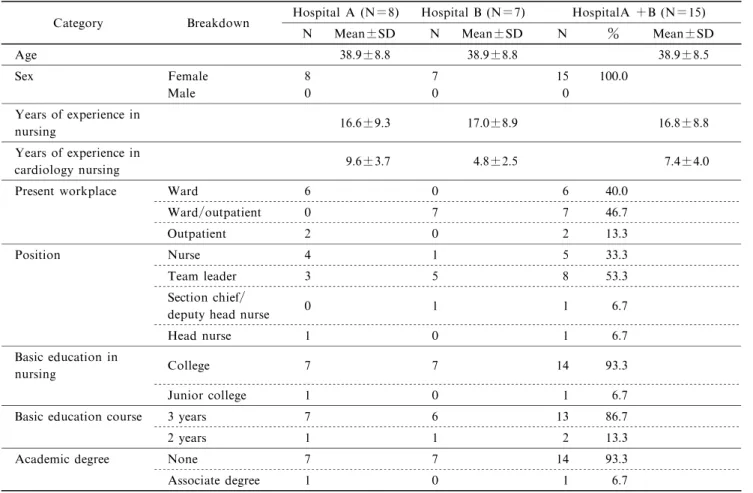
1. Outline of the sample population (Table 1) The sample population consisted of eight female nurses from hospital A and seven female nurses from hospital B. The mean age of the nurses was 38.9 (SD±8.8)for both hospitals. The mean years of their experience in nursing and in cardiac nursing were 16.8 (SD±8.8) and 7.4 (SD±4.0) respectively for both hospitals together. In hospital A six nurses worked in the ward and two in the outpatient department. Hospital B has adopted a system under which profi-cient nurses take turns in working in the outpatient department, thus concurrently working for the ward and the outpatient department. As to the positions assumed by the nurses in the two hospitals, five were nurses and ten were in managerial positions such as
head nurses or higher.
2. Actual nursing practice for elderly myocardial infarction patients (Table 2)
61 contexts were extracted in total from the tran-scriptions of the interviews. They were categorized into the place of nursing -ward (where treatment was given right after myocardial infarction), outpatient department and hospital stay for examination - and described the content of nursing care. Out of the 61 contexts,53 cases were related to nursing care provided in the ward. Nursing care was provided at the out-patient department in five cases and in three cases during a hospital stay for examination. The results of grouping the content of nursing care by category and by method indicated that the nursing care performed in the ward included 40 categories: medical treatment (6 cases), care related to treatment such as low salt diet and medication management (17 cases),care related to life such as activity and family support (14 cases),and disease management (3 cases). The nursing method taken in the ward included 11 cases in which the nurse provided care in response to the patients understand-ing ability, care in response to a feature of elderly patients, or care in response to a problem with cognitive function and understanding ability,and two cases in which the patients will was respected.
Table 1 Outline of interview participants
Category Breakdown Hospital A (N=8) Hospital B (N=7) HospitalA +B (N=15) N Mean±SD N Mean±SD N % Mean±SD
Age 38.9±8.8 38.9±8.8 38.9±8.5 Sex Female 8 7 15 100.0 Male 0 0 0 Years of experience in nursing 16.6±9.3 17.0±8.9 16.8±8.8 Years of experience in cardiology nursing 9.6±3.7 4.8±2.5 7.4±4.0 Present workplace Ward 6 0 6 40.0
Ward/outpatient 0 7 7 46.7
Outpatient 2 0 2 13.3
Position Nurse 4 1 5 33.3
Team leader 3 5 8 53.3
Section chief/
deputy head nurse 0 1 1 6.7
Head nurse 1 0 1 6.7
Basic education in
nursing College 7 7 14 93.3
Junior college 1 0 1 6.7
Basic education course 3 years 7 6 13 86.7
2 years 1 1 2 13.3
Academic degree None 7 7 14 93.3 Associate degree 1 0 1 6.7
Thus, the content of nursing care for elderly patients is distinguished by the issues of a low salt diet, medication management, and activity, and an appro-priate method was flexibly adopted according to each patients cognitive function and understanding ability. The features related to treatment at the acute phase but excluded from this analysis included senile delir-ium/restless syndromes, delay in recovery, complica-tions of heart failure,and risk of falling. Besides,the interviews revealed that an incorrect understanding of health information and an inappropriate use of health information were the features of and difficulties about elderly patients.
3. Confirmation of the features of elderly myocar-dial infarction patients (Tables 3)
Twelve categories out of the 15-category features of elderly myocardial infarction patients were con-firmed by interview data either of hospital A group or hospital B group. They are general features of elderly patients. The categories confirmed only by one group included 1) About one year before stability and 7) Change in quality of life. The following categories were confirmed in a greater number by both groups: 3) Patients anxiety about recurrence, 6) Reduction in the level and scope of activities,and 15)Observation of the process until coronary angiography after leaving
hospital.
The features that have not been validated by inter-view data of either hospital A or hospital B were the three categories, 8) Acceptance of restrictions in daily living,9)Earnest efforts to follow guidance/advice on living daily lives, and 12) A sense of liability for the burden imposed on the family by the attack and hospitalization. These are idiosyncratic features of elderly patients.
4. Newly extracted features (Table 4)
Three additional categories were extracted from the analytical results of interview data: 3) Talk after coronary angiography, 17) Follow-up after the talk, and 18) Establishment of counseling/support system. All these are related to the content of nursing care provided in the outpatient department and during a hospital stay for examination after being released from hospital.
V. Discussions
1. Nursing care for elderly myocardial infarction patients and problems with self-care
Some content-wise problems with self-care in elderly patients perceived by proficient nurses working in the ward and the outpatient department included a low salt diet, medication management, and activity.
Table 2 Actual nursing practice for elderly myocardial infarction patients ( ) Number of speaking Place of nursing Content of nursing care (Category/method)
A short hospital stay(5) Treatment (6)
Dementia (1) Low salt diet (10) Related to treatment (17) Medication management (7) Activity(5) Familys support (3) Category(40) Anxiety(2) Related to living (14) Ward (53) Rest (2) Meals (1) Life in general (1) Disease management (3) Responses for acute symptoms (2)
Regular medical treatment (1) Action in response to understanding ability(8) Cognitive function/
understanding ability(11)
Method (13) Action in response to the features of the elderly(3) Attitude of respect (2) Action with due respect (2)
Low salt (1) Related to treatment (2)
Category(3) Medication management (1) Outpatient (5)
Related to living (1) Activity(1)
Method (2) Action taken in the outpatient dept.(2) Opportunities of offering support (2) Related to treatment (1) Low salt (1)
Hospital stay for
examination (3) Category(3) Related to living (2) Activity(2) 61 cases in total
Method-wise problems were related to the issues of a decline in understanding and cognitive abilities,family functions, and continuity of nursing.
The revised edition of the Guidelines for secon-dary prevention of myocardial infarction evidentially demonstrated for the first time in Japan in 2000 the effectiveness of general treatments (non-drug treat-ments) represented by diet, exercise and non-smoking. The salt intake of Japanese dropped since the 1990s
and is now roughly 11∼12g per day. Notwithstand-ing,the revised Guidelines recommend that a daily salt intake should be further reduced from 7 g to 6 g or less as a target. It is assumed that it will need a consider-able effort for present elderly patients to keep a daily salt intake of 6 g or less. Thus,even during the period of hospitalization for the acute phase it is generally understood that it poses a difficult problem with self-care. Detailed data of the interviews revealed that
Table 3 Confirmation of features of elderly myocardial infarction patients
No. Content The number of confirmation Hospital A Hospital B 1 In general it takes about one year after leaving hospital before the
patients life becomes stable. ― 2 2 The patient adjusts his lifestyle to adapt to seasonal climate changes. 3 3 3 The patient has anxiety about a recurrence of paroxysms and symp
toms of acute myocardial infarction. 10 8
-4 The patient thinks that activity (exercise) is one of the factors to
induce a recurrence of paroxysms. 2 3 5 The patient tends to restrict activity(exercise) to avoid recurrence. 2 2 6 The level and scope of the patients activity(exercise) are reduced in
comparison to pre-myocardial infarction level and scope. 8 5 Changes in life and
social activity after leaving hospital
7 The patient understands that he/she will not be able to keep the same
lifestyle as before after myocardial infarction. ― 2 8 The patient thinks that he/she must accept restrictions in living due
to the disease, thanking a narrow escape from death. ― ― 9 The patient makes earnest efforts to follow the professional guidance/
advice on living. ― ―
10 The patients family has anxiety about a recurrence of paroxysms and
symptoms of acute myocardial infarction. 2 5 11 The patients family restricts or keeps an eye on the level and scope
of his/her activity(exercise). 7 3 12
The patient is aware that he/she has placed a burden on his/her family through the attack of myocardial infarction and subsequent hospitalization.
― ―
13 The patient tries to follow the restrictions and accept supervision
imposed by the family on his/her activities. 1 2
Issues in continuous nursing support
14
The patient has needs to talk about his/her life in general and anxiety about recurrence and wants to have consultation with the doctor when he/she visits the outpatient department for regular hospital visit.
7 5
15
It will be necessary to observe the process until cardiac catheterization examination and give counseling/support during that time after leaving hospital.
4 9
Note: -Indicates unconfirmed Table 4 New three categories extracted from the group interview
No. Content
16 It may be necessary to talk with the patient about life in general depending upon the result of cardiac catheterization examination.
Category to be added Issues in continuous nursing support 17
It may be necessary to continue counseling/support for a certain period of time depending upon the result of the talk.
18 New training will be necessary about follow-up counseling, consultation/ support skills, and the establishment of such a system.
proficient nurses responses were not necessarily in conformity to the principle in consideration for the complications of heart failure, appetite and meal intake, and quality of life. That is, proficient nurses make allowance for in each situation in their assis-tance towards recovery.
The nurses who participated in the interview pointed out that the cause of difficulties in medication management was related to a decline in understanding ability and cognitive functions. At the same time in scenes of continuous nursing, while they expected the familys role to make up for the difficulty in medica-tion management, they were also keenly aware of the problem of a short supply of human resources under the social circumstances in which the todays elderly were placed.
A family problem was recognized in relation to activity as well. Detailed data of the interviews demonstrated that the family tried to put restrictions on the patients activity even during hospitalization. The reason is,as indicated by the findings of Survey 1, anxiety about recurrence. A study has exposed,as to the process of chronic diseases,that a particular family pattern and the presence of a family aggravate the chronicity of a physical disorder. It is essential to provide continuous nursing support also to the family with a strong sense of anxiety.
A short hospital stay was pointed out as the content categorized under treatment proper among the support categories particular to super-elderly patients. The hospital stay has been increasingly shortened in recent years primarily because of the development of therapy technologies for myocardial infarctions and trends of medical policies. The Guidelines (2007 revised edition) on rehabilitation for cardiovascular diseases proposed a short-term rehabilitation pro-gram of two weeks,further shorter than the one recom-mended by the previous guidelines.
Both hospitals where the interview participants work have prepared a clinical pathway based on this short-term program and provide treatment and nursing care according to the pathway. In order to cope, within a limited hospital stay,with difficulty in educat-ing elderly patients who are perceived by proficient nurses that their cognitive functions and understanding ability have typically declined,it will be important to secure close coordination between nurses and people in other jobs as well as the congruity of nursing care from the ward (that provides treatment right after myocardial infarction) to the outpatient department and a hospital stay for examination.
The clinical pathways of the two hospitals include guidance/advice by registered dietician and pharmacist and are indeed put into practice. However,the issues
of a low salt diet and medication management are pointed out as major difficult issues in support and education. It is,therefore,assumed that the problems with treatment and living of elderly patients are recog-nized only among a team of nurses and not shared by people in other jobs. To provide support and educa-tion to patients by fully using expertise in each job,it is necessary to perform a post-evaluation of standard education laid down in the clinical pathway and share its results with people in other jobs as well as nurses so that measures can be taken to incorporate an in-dividualized education program from an early stage of hospitalization.
2. General features and idiosyncratic features of super-elderly myocardial infarction patients Among the 15-category features extracted by previ-ous study, there were three categories that have been confirmed neither by hospital A group nor by hospital B group : 8) Acceptance of restriction in living, 9) Earnest efforts to follow guidance/advice on living daily lives,and 12) A sense of liability for the burden imposed on the family by the attack and hospitaliza-tion. In the cases that led to extracting these features, the wife had deep anxiety about recurrence. In all likelihood, these three categories reflected the particu-larities of the sample population (applicable cases) of previous study. Only a longitudinal study that extends over a long time will be able to verify the category of 1) About one year before stability, out of the categories confirmed only by one group.
Among the categories that have been confirmed in a higher number by both groups, 15) Observation of the process until coronary angiography after release from hospital was confirmed by the group of hospital B many times. This is probably because the nurses who participated in the interview in hospital B work in the ward and the outpatient department concurrently, thereby enabling them to observe continually and understand their patients better.
3. Limit of and problems with this study
The participants in the focus group interviews conducted in this study were only 15 persons in two groups, and moreover the findings are based on only one interview. Hence, it is necessary to explore the same line of study by increasing the numbers of institu-tions, sample population, and interviews. Likewise, an important issue in the future will be to validate the results of the interviews by quantitative method.
Acknowledgements
My heartfelt gratitude is extended to the nurses who have contributed their precious time to participate
in the focus group interview and also the nurse admin-istrators of the hospitals for their cooperation.
References
1. Japan Aging Research Center: Basic data on ageing society 2009-2010 edition,32,Chuohoki Publishing Co.,Ltd.,2009 2. Cabinet Office: White paper on aging society (2009), 29,
Saiki Printing Co., Ltd., 2009
3. Cabinet Office: White paper on aging society (2009), 31, Saiki Printing Co., Ltd., 2009
4. Secretariat of Tokyo CCU Network : Performance report on Tokyo CCU Network, 29, 704-709, 2005
5. Nagao K, Hayashi S, Uemathu S. Cardiac arrest with ischemic heart disease. The Journal of the Japanese Society of Internal Medicine 2004; 93: 300-305.
6. Asajyra K. Bodily experiences of myocardial infarction survivors. Japan Journal of Nursing Science 1998; 18: 10-20.
7. Tojima H. A study on rehabilitation system development for heart diseases: entrusted by the Circulatory Disease Section, Ministry of Health, Labour and Welfare. Collec-tion of projects in 1982, 1983.
8. Saito M. Guidelines on rehabilitation for circulatory dis-eases, Report of the study entrusted by the Circulatory Disease Section, Ministry of Health, Labour and Welfare, 1996.
9. Saito M. History of cardio rehabilitation,compiled under the supervision of Japan Heart Club,Cardiac rehabilitation -Yesterday, today and tomorrow, 23, Saishin Igaku Com-pany, 2007.
10. Goto Y,Saito Y,Iwasaka H,et al. National factual survey on rehabilitation at the recovery phase after acute myocar-dial infarctions in Japan. Cardiac Rehabilitation 2006; 11: 36-40.
11. Aida N, Urano M, Saito K. Roles of and problems with nursing in integrated cardiac rehabilitation. Nursing Art and Science 2006; 52: 460-464.
12. Teramachi Y. Cardiac nursing, 31, 4, IGAKU-SHOIN, Ltd., 1997.
13. Kimura Y, Namasu Y, Fujii M, et al. Survey on the cardiac patients anxiety about daily activities after hospital discharge. Cardiac Rehabilitation 2008; 13: 154-157. 14. Masima T. Status quo and outlook of cardiac
rehabilita-tion nursing II - Psychological and social support for cardiac patients. Quality Nursing 2002; 8: 379-381. 15. Johnson JL, Morse JM. Regaining control - The process
of adjustment after myocardial infarction. Heart Lung 1990; 19 : 125-135.
16. Azechi M. Case study on effects of cardiac rehabilitation
-Ischemic heart diseases. Nursing Today 2009 ; 24: 24-31.
17. Moriyama M, Nakano M, Furui Y, et al: A study on the effectiveness of an integrated cardiac rehabilitation program towards regaining self-management ability. Japan Journal of Nursing Science 2008; 28: 17-26.
18. Yamamoto S, Matunaga A, Sawairi T, et al. A study on the maximum walking speed in in-hospital super-elderly cardiac patients. Cardiac Rehabilitation 2008; 13: 304-308.
19. Sawairi T,Masuda T,Matunaga A,et al. About influences on balance function of elderly ischemic heart disease patients by continuing recovery phase cardiac rehabilitation. Cardiac Rehabilitation 2008; 13: 322-325.
20. Ishibashi K, Yoshida M, Kubota M, et al. Trial of a cardiac rehabilitation program on elderly heart failure patients. Cardiac Rehabilitation 2007; 12: 163-166. 21. Yokoyama Y,Watanabe S,Kasahara Y,et al. Lower limb
muscle force and walking ability in elderly heart failure patients. Cardiac rehabilitation 2007; 12: 239-243. 22. Patricia Benner(translated under the supervision of Toshiko
Ibe): Excellence and Power in Clinical Nursing,new trans-lated edition, 23, IGAKU-SHOIN, Ltd., 2005
23. Ito M, Kamata H. Changes in life and social activity and their causes in elderly myocardial infarction patients over two years after the onset. The KITAKANTO Medical Journal 2011; 61: 307-317.
24. Shinozaki M, Sato K. Transition in degrees of health in old age and analysis of related factors. Study of Social Relations 1995; 1: 95-118.
25. Japan Circulation Society: Guidelines for secondary pre-vention of myocardial infarction (revised edition of 2006), Guidelines on diagnosis and treatment for circulatory dis-eases, Report by the 2004-2005 Joint Study Team, 2006. 26. Research Association of Health and Nutrition : Status quo
of national nutrition, Findings of the 2002 National Nutri-tional Survey by the Ministry of Health, Labour and Welfare, DAI-ICHI SHUPPAN Co., Ltd., 2004.
27. Neya T. Problems with self-care and nursing support for super-elderly outpatients for chronic heart failure. Journal of Japan Academy of Gerontological Nursing 2008; 13: 40-48.
28. Walsh, F, C.M. Anderson (translated under the supervi-sion of Takeshi Nonaka, Hiromi Shiraishi): Chronic dis-orders and the family, 163, 1994.
29. Japanese Circulation Society: Guidelines on rehabilitation for cardiovascular diseases(Revised edition of 2007),Report by the 2006 Joint Study Team on the Guidelines on diagno-sis and treatment for circulatory diseases, 2007.