IRUCAA@TDC : Congenital Epidermoid Cyst Arising in Soft Palate Near Uvula: A Case Report
6
0
0
全文
(2) 207. Bull Tokyo Dent Coll (2010) 51(4): 207–211. Case Report. Congenital Epidermoid Cyst Arising in Soft Palate Near Uvula: A Case Report Kenichiro Suga, Kyotaro Muramatsu, Takeshi Uchiyama, Nobuo Takano and Takahiko Shibahara Department of Oral and Maxillofacial Surgery, Tokyo Dental College, 1-2-2 Masago, Mihama-ku, Chiba 261-8502, Japan. Received 12 May, 2010/Accepted for publication 21 June, 2010. Abstract Aberrant ectodermal tissues during the fetal period or acquired aberrant epithelial tissue due to trauma or surgery are thought to cause dermoid and epidermoid cysts. Their incidence is 7.0% in the head and neck region and only 1.6% in the oral cavity, where they mostly present in the floor of the mouth. On the other hand, they are extremely rare in the soft palate and uvula, and only six cases have been reported. Epidermoid cysts grow slowly and asymptomatically, and thus rarely cause oral dysfunction. However, cysts arising in the floor of the mouth can lead to developmental disorders due to impaired suckling and swallowing. This report describes a 4-week-old boy in whom an epidermoid cyst developed in the midline region of the soft palate close to the uvula. Decreased suckling ability led to a poor in body weight, so resection was performed at an early age. The histopathological diagnosis was epidermoid cyst. Key words: Epidermoid cyst— Congenital cyst— Soft palate—Uvula— Neonate. Introduction Dermoid and epidermoid cysts are thought to be caused by aberrant epithelial components of ectodermal tissues during the fetal period or by aberrant epithelial tissue acquired due to trauma and surgery. Such cysts can arise anywhere in the body, but the incidence in the head and neck region accounts for only 7.0% of the total3). Among cysts of the head and neck, incidence in the stomatognathic region is highest in the floor of the mouth and lowest in the soft palate9). To the best of our knowledge, only six reports have. described cysts involving the uvula or soft palate1,2,5,8,10,11). Cysts often develop slowly and asymptomatically, but when they arise in the floor of the mouth of infants, respiration and feeding disorders can result7). We describe herein a neonate in whom suckling was decreased due to a congenital epidermoid cyst in the soft palate.. Case A 4-week-old boy who was delivered normally in September 2004 was brought to our. 207.
(3) 208. Suga K et al.. Fig. 1 Intraoral condition at first examination Revealed small, whitish, domed mass under mucous membrane.. Fig. 2 Intraoral condition during surgery a: Mass was located in medial soft palate, behind uvula (arrows). b: Border between mass and surrounding tissue was clear (arrows).. Fig. 3 Excised lesion Spherical cystic lesion measured 7⳯8⳯8 mm.. Fig. 4 Histopathological findings Cystic wall was lined with flat, stratified squamous epithelium with slight keratinization; keratinous materials were evident inside cyst. Epidermoid cyst was diagnosed..
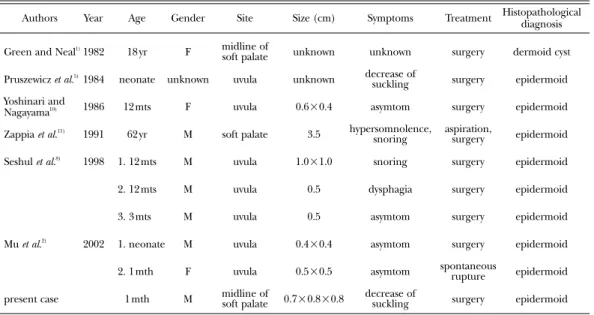
(4) 209. Epidermoid Cyst of the Soft Palate. hospital for an intraoral medical check-up at the age of 4 weeks. He appeared to have developed normally, and his nutritional status was favorable. A soft elastic, soybean-shaped mass was observed in the soft palate at the base of the left side of the uvula. The extremely thin oral mucosa covering the mass allowed visual confirmation of a white hemispherical mass beneath (Fig. 1). The lesion was asymptomatic, and because suckling volume and behavior appeared normal and no clinical malignancies were evident, the patient was only monitored. However, at the age of 8 weeks, the lesion had slightly increased and the patient had gained insufficient weight due to poor suckling ability. A further examination led to a diagnosis of a benign soft palate tumor, and resection was scheduled. Surgery proceeded under general anesthesia with oral intubation in accordance with benign tumor resection procedures. The surgical field was brightened using a Dingman mouth gag, and the lesion could be visualized from the posterior base of the uvula to the posterior edge of the soft palate. The uvula was pulled using a nylon suture, and mucosal resection included the mucosa covering the. mass along the base of the mucosa (Fig. 2-a). The border between the mass and surrounding tissue was clear, which facilitated its separation and resection from the surrounding tissue (Fig. 2-b). Because a deep part of the mass reached the muscle coat of the tensor veli palati and levator veli palatini muscles, each muscle bundle was sutured after resecting the mass and the surgical wound was closed by suturing. Since his systemic condition stabilized and suckling improved postoperatively, the patient was discharged in good health seven days later. The patient has remained free of recurrence for five years. The excised spherical mass measured about 7⳯8⳯8 mm, and the surface was flat and smooth (Fig. 3). A histopathological examination showed that connective tissue had formed a cystic cavity covered by keratinized stratified squamous epithelium. The cyst wall was slightly keratinized and was lined with keratinized stratified squamous epithelium, and the cyst itself contained keratinous materials (Fig. 4). No evidence of dermal appendages presented in the cyst wall. Based on the above findings, the lesion was diagnosed as an epidermoid cyst.. Table 1 Published cases of dermoid/epidermoid cyst of palate or uvula Year. Age. Gender. Site. Size (cm). Symptoms. Treatment. Histopathological diagnosis. Green and Neal1) 1982. 18 yr. F. midline of soft palate. unknown. unknown. surgery. dermoid cyst. Pruszewicz et al.5) 1984. neonate. unknown. uvula. unknown. decrease of suckling. surgery. epidermoid. 12 mts. F. uvula. 0.6⳯0.4. asymtom. surgery. epidermoid. aspiration, surgery. epidermoid. Authors. Yoshinari and Nagayama10). 1986. Zappia et al.. 1991. 62 yr. M. soft palate. 3.5. hypersomnolence, snoring. Seshul et al.8). 1998. 1. 12 mts. M. uvula. 1.0⳯1.0. snoring. surgery. epidermoid. 2. 12 mts. M. uvula. 0.5. dysphagia. surgery. epidermoid. 3. 3 mts. M. uvula. 0.5. asymtom. surgery. epidermoid. 1. neonate. M. uvula. 0.4⳯0.4. asymtom. surgery. epidermoid. 2. 1 mth. F. uvula. 0.5⳯0.5. asymtom. spontaneous rupture. epidermoid. 1 mth. M. midline of soft palate. 0.7⳯0.8⳯0.8. decrease of suckling. surgery. epidermoid. 11). Mu et al.2). present case. 2002.
(5) 210. Suga K et al.. Discussion Dermoid and epidermoid cysts can arise anywhere in the body, and according to the study of New and Erich3), the most common location was the anus (44.5%) followed by the ovary (42.1%) in 1,495 patients. The incidence in the head and neck region was 6.9%, which accounted for only a small fraction of the total. Furthermore, of 103 patients with head and neck dermoid and epidermoid cysts, the most common locations were the orbit (46.6%), followed by the floor of the mouth and submental region (23.3%), nose (12.6%), neck (10.7%) and lip (2.9%). Only six dermoid and epidermoid cysts in the soft palate or uvula have been reported (Table 1). Acquired factors include aberrant epithelial components in deep tissue due to trauma, and inflammation and surgical complications may be mechanisms of onset, but dermoid and epidermoid cysts are usually congenital. The most frequent congenital cause is aberrant ectoderm in the fusion area of the branchial arch and groove at the fetal age of 3–4 weeks, but cleaved cells can be ectopically reactivated during the fetal period3). In stomatognathic areas other than the palate, most cysts arise in the midline region where the left and right branchial arches fuse. Several investigations have localized such cysts arising in the soft palate or uvula in the midline region. The secondary palate that comprises the palate and soft palate is formed when the left and right palatine shelves of the maxillary process fuse at the fetal age of around 7 to 9 weeks, supporting the notion that epidermoid cysts arising in the soft palate or uvula are due to congenital causes involving aberrant ectoderm in the fused area. The mass in the present patient extended slightly laterally from the midline region, and it is impossible to ascertain which congenital factor(s) was involved in the cyst. However, the mass was confirmed soon after birth, and the cyst was already present at the age of one month. Therefore, congenital factor(s) were indicated by the absence of trauma in this case. The basic treatment for epidermoid cysts. is total excision. Ronald6) treats extremely large masses via fine-needle aspiration to reduce the content and then performs the excision. However when the objective of such surgery is unclear, palliative treatments such as fine-needle aspiration and fenestration can lead to infection, which potentially causes pain and exacerbation4). Therefore fineneedle aspiration should be performed as a diagnostic tool, and total excision should be promptly performed if epidermoid cysts are diagnosed clinically. While various theories have been proposed for the timing of surgery for these cysts, surgery for neonates should be performed when safe to do so under general anesthesia. The findings in the present patient did not indicate malignancy the mass was quite small at first examination and dysfunction was absent. Hence we originally planned to wait for the patient to mature before proceeding with more thorough testing. However, because suckling had become mildly impaired by the age of 8 weeks, we decided to resect the mass sooner than planned under strict perioperative management. The results in this case indicate that surgery performed at an early age without fine-needle aspiration helped facilitate a marked improvement in suckling and increase in body weight.. References 1) Green JD, Neal CL (1982) Dermoid cyst of the soft palate. South Med J 75:1029. 2) Mu SC, Sung TC, Yeh ML, Hsu ST, Lin MI, Chen HY (2002) Solitary epitherial cyst the uvula in the neonate: case reports and review of the literature. Pediatr Emerg Care 18:93–94. 3) New GB, Erich JB (1937) Dermoid cysts of the head and neck. Surg Gynecol Obstet 65:48–55. 4) Ochiai A, Iino T, Ota F, Kato T (2006) Dermoid cyst on oral floor in an infant. Oto-RhinoLaryngology, Tokyo 49:131–136. (in Japanese) 5) Pruszewicz A, Sobala M, Sobocznski ´ A (1984) Case of epithelial cyst of the uvula situated in the nasopharynx in a newborn infant. Otolaryngol Pol 38:529–531. (in Portuguese) 6) Ronald CK (1994) Dermoid cyst in the floor of the mouth. Oral Surg Oral Med Oral Pathol 78:567–576..
(6) Epidermoid Cyst of the Soft Palate. 7) Sato T, Yoshimoto K, Nin S, Yasuda M, Uno T, Hisa Y (2004) Congenital dermoid cyst of the floor of the mouth in an infant: report of a case. Otolaryngology-Head and Neck Surgery 76:387–389. (in Japanese) 8) Seshul M, Tseng E, Wiatrak B, Kelly D (1998) Isolated epitherial cysts of the uvula in children: a report of three cases. Ann Otol Rhinol Laryngol 107:717–719. 9) Turetschek K, Hospdka H, Steiner E (1995) Case report: epidermoid cyst of the floor of the mouth: diagnostic imaging by sonography, computed tomography and magnetic resonance imaging. Br J Radiol 68:205–207. 10) Yoshinari M, Nagayama M (1986) Epidermoid. 211. cyst of the uvula: report of a case. J Oral Maxillofac Surg 44:828–829. 11) Zappia J J, Carrol WR, Wolf GT (1991) Palatal inclusion cyst: an unusual complication of uvulopalatopharyngoplasty. Ear Nose Throat J 70:538–539. Reprint requests to: Dr. Kenichiro Suga Department of Oral and Maxillofacial Surgery, Tokyo Dental College, 1-2-2 Masago, Mihama-ku, Chiba 261-8502, Japan.
(7)
図

関連したドキュメント
Report of two cases. Post-operative herpes simplex virus encephalitis after surgical resection of acoustic neuroma: a case report. Herpes simplex virus reactivation
Tsujimoto, Yuichi; Satoh, Mototaka; Takada, Tsuyoshi; Honda, Masahito; Matsumiya, Kiyomi;. Fujioka, Hideki;
Kurosaka, Shinji; Irie, Akira; Ishii, Junichiro; Minei, Sadatsugu; Takasima, Rikiya; Kadowaki, Kazuomi;. Morinaga, Shojiroh;
Prostatic cyst arising around the bladder neck-cause of bladder outlet obstruction: two
patient with apraxia of speech -A preliminary case report-, Annual Bulletin, RILP, Univ.. J.: Apraxia of speech in patients with Broca's aphasia ; A
Key words: random fields, Gaussian processes, fractional Brownian motion, fractal mea- sures, self–similar measures, small deviations, Kolmogorov numbers, metric entropy,
Usefulness of positron emission tomography (PET) in a retroperitoneal primary non- seminomatous germ cell tumor: a
In this paper we will examine self-accelerating in terms of convergence speed and the corresponding index of efficiency in the sense of Ostrowski - Traub of certain standard and
