日本と世界の新生児医療
藤村正哲
名誉総長
大阪府立母子保健総合医療センター
On behalf of the Neonatal Research Network
Japan
0 5 10 15 20 25 30 35 1968 1970 1972 1974 1976 1978 1980 1982 1984 1986 1988 1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 日本 アメリカ イギリス イタリア オーストラリア オーストリア オランダ カナダ スイス スエーデン スペイン デンマーク新生児死亡率の推移
(死亡数 /1000 出生 )(年)
(楠田、2011)NICU疾患別入院数
(NICU全国調査から) 0 100 200 300 400 500 600 700 800 900 1000 極低出生体重児<500g 500-999g 1000-1499g 呼吸障害等1500g-1299g 2000-2499g 2500g-重症仮死 痙攣 交換輸血 外科疾患 先天性疾患 奇形症候群 神経疾患入院数/年
総合周産期母子医療センターネットワーク研究班 (楠田、2011)“日本の売り”
1. 世界でも最も低い
新生児死亡率
を40年以上維持している
こと。
2. 各国との新生児ネットワーク比較で、
1500g未満生存率
及び罹病率
が、おそらく最優秀。
3. 22週23週児
の救命経験が世界でもひと桁上を行っている
こと(売りかどうか異論もあるのは承知で)。
4. そしておそらく生存した超低出生体重児の
予後
も多少では
あるが優れている“らしい”ことである。
世界中の最先端NICUの回診やカンファレンスでは、毎日のように 超低出生体重児に関する課題が出ているだろう。その場で日本のデ ータが話題になるという状況があれば、日常的に日本の新生児医療 が意識上で存在しているということになる。 そういう状況をつくるためには、日本の新生児医療の「成果」が十 分に発信されていなければならない。さらにその成果を生み出して いる日本独自のシステムを、根拠を示しつつ発信することこそ、世 界に示しうるものではないか。 それができると、個々の研究者が発表する論文も、日本からの新生 児研究であるということで“軽視される”のでなく“選ばれて読ま れる”という状況もつくれるのではないか。 日本のNICU医療の集積結果が総体として成し遂げつつある成果は 、まだ他の国では入手できない先駆性をもっている。今というタイ ミングを大切にしたい。最近1年間の発信実績
新生児科関係部署の研究者から発表されていた新生児関連論文PubMed: newborn japan (limit: 1 year, Newborn 0-1 month)
2010 年10月—2011年9月 発表 治療 診断 病因 予後 ネットワーク・データベー スを活用した論文 1 0 0 2 単独施設における研究 1 5 7 *a 2 *b *a 1施設 総合周産期母子医療センター(一般病院) *b 2施設 総合周産期母子医療センター(こども病院)日本の新生児医療指標が国際的に最高水準にあるのに比し
て、日本発信のランダム化臨床比較試験(RCT)はあまり
にも少ない
=
新生児ジャパンの“売り”について根拠ある説明、
つまり世界への発信ができていない!
新生児臨床ネットワーク
NRN(neonatal research network)
1998年に設立「新生児臨床研究ネットワークの運営に関する研究班」
2001-2003年度世界へ発信の前提条件
①
臨床試験組織の構築
②
発表する「実体」を造り出せること
③
新生児集中治療施設が世界標準
④
新生児死亡率
-新生児医療のアウトカム①-⑤
新生児医療内容のベンチマーク
⑥
退院後の発達予後
-新生児医療のアウトカム②-⑦
研究能力、論文作成能
世界へ発信の前提条件
①
臨床試験組織の構築
研究計画立案と予備研究のあり方 試験のQuality Assurance、Quality Controlの方法 臨床試験機関のリクルート エンドポイントとして不可欠の発達予後の評価 研究資金 小児臨床試験の倫理のあり方 研究の効果的遂行 新生児臨床試験組織の育成と新生児用医薬品開発の科学性・倫理性 に関する研究 主任研究者 山崎俊夫 創薬ヒューマンサイエンス研究事業
「新生児臨床研究ネットワークの運営に関する研究班」
2001-2003/年度 http://nrn.shiga-med.ac.jp 試験計画・組織論 新生児臨床試験のあり方 藤村 正哲 新生児を対象としたランダム化比較試験の正しい構築 中西 範幸 インターネットを活用した新生児臨床試験のあり方 青谷 裕文 新生児臨床試験におけるコーディネーションの方法 平野 慎也 運営論・倫理 新生児臨床試験における説明と同意のあり方、および被験者のコンプライアン ス 近藤 裕一 新生児ランダム化試験におけるプラセボのあり方 梶原 真人 新生児臨床試験における診療当事者のコンプライアンス 板橋 家頭夫 地域周産期医療センターにおける新生児臨床試験実施の問題点 住田 裕「新生児臨床研究ネットワークの運営に関する研究班」
2001-2003/年度 http://nrn.shiga-med.ac.jp 各 論 新生児臨床試験における症例調査票の設計方法論に関する研究 市橋 寛 新生児臨床研究ネットワークの基礎データベース構築と評価方法に関する研究 楠田 聡 新生児臨床試験における医薬品評価と薬物動態研究の組み込みに関する研究 中村 秀文 新生児への吸入薬の臨床試験において生じる諸問題の研究 中村 友彦 新生児薬物動態研究におけるpopulation pharmacokineticsの妥当性に関する 研究 湯川 栄二 新生児臨床試験におけるエンドポイントとしての長期予後評価の方法に関する 研究 金澤 忠博新生児臨床研究ネットワークによる
多施設ランダム化比較試験
http://nrn.shiga-med.ac.jp/
Randomized controlled trial study period Result Prophylactic intravenous indomethacin for preventing mortality and
morbidity in preterm infants 1999-2003 effective Start feeding within 24 hours of birth in ELBW 2000-2003 discontinue Intravous phenobarbital for neonatal seizure 2005-2008 effective Fluticasone propionate for the prevention of CLD in ELBW 2006-2009 in analysis Doxapram hydrochrolide for apnea of prematurity 2007-2009 effective Umbilical cord milking for effective resuscitation of ELBW
2007-Erythropoietin for the prevention of brain injury of ELBW 2007-Japan
低用量インドメタシン予防投与による600g未満
群の予後改善効果
• 海外の先行論文は、予後に有意差なしと結論して終了
• 世界で初めて600g未満の研究が可能であった
世界へ発信
0 10 20 30 40 50 60 70 80 90 100Indomethacin
Placebo
Died
CP
No CP
Birthweight 400-599g
Cerebral Palsy or Death
% N= 22 27 P<0.02
NEONATAL RESEARCH NETWORK
(Hirano, Fujimura, 2010) 76.3 59.0 75.2 80.4 82.1 86.7 0.0 20.0 40.0 60.0 80.0 100.0 120.0
22-23W
24-26W
27W-p=0.042 p=0.06 p=0.06 12 9 101 88 67 72Comparison of Total Score DQ
Indomethacin Trial Follow-up at 3 years
(Hirano, Fujimura, 2010)
2011年4月30日からDenverで開催されたAsian
Society for Pediatric Researchで平野慎也先生
の発表(NRN脳室内出血班、22-23週出生児の3
歳児発達予後の改善)が
「ASPR Best Research Award」
に選ばれた
総合周産期母子医療センターネットワーク研究班 Better Developmental function at 3 years for infants born at 22-23wks
who participated in the Randomized Controlled Trial for the Prevention of Intraventricular Hemorrhage by Indomethacin in Japanese Extremely Low Birthweight Infants
世界へ発信の前提条件
②
発表する「実体」を造り出せること
NICU連合体としてのネットワークが構成されること それによって・・・ 短期間で症例数が集まる 研究資源が効率的に稼働する(費用対効果も良い) 熱意が持続する 研究条件の変動が少ない つまりアイデアだけでは駄目だということです 東京都88NICUs
(2011年11月現在)
沖縄Japan
アウトカムを指標としベンチマーク手法を用いた質の
高いケアを提供する「周産期母子医療センターネット
ワーク」の構築に関する研究班
2004ー
登録施設および≦1500g症例数
0 10 20 30 40 50 60 70 2003 2004 2005 0 500 1000 1500 2000 2500 3000 3500 No of ho sp it al s No of in fa n ts(year)
2006 2007 4000 80施設数
登録数
2008総合周産期母子医療センターネットワーク・データベース
Level 3 NICU数 施設当り 医師数 施設当り 入院数/年 総医 師数 総入院数 /年 医師一人 当り入院 数 日本 77 6.2 317 477 24,409 51.1 UK 45 15.5 524 697 23,580 33.8世界へ発信の前提条件
③
新生児集中治療施設が世界標準
NICUの類似性等 ー同じような土俵の上で、同じようなルールの医療ー医師一人当り入院数の日英比較
総合周産期母子医療センターネットワーク研究班Comparison between UK and Japan
22 weeks’ gestation Population 2006 Total Live birth 2006 stillbirth Live birth Admission to NICU Alive at day 28 Survival discharge UK EPICure 2006 (1year) 110 148 20 6 - 60,512,000 715,000 Japan our study 2006-2007 2years) 115 161 152 - 55 127,953,000 1,087,000Ratio of
stillbirth
:
Live birth
is very similar in two studies.
(山口、田村、2010) 総合周産期母子医療センターネットワーク研究班 0 1 2 3 4 5 6 7 8 レジデント級 医員級 指導医級 医長級総合周産期NICU (日) Level 3 NICU (UK)
NICU医師数の日英比較
レベル3のNICU当たり平均値
(英)A Survey of Current Neonatal Unit Organisation and Policy July 2005 Commissioned by BLISS The Premature Baby Charity
制定した主体 ガイドライン名 医師夜間必要数 看護師1人 当り担当児 数 (専門看護師) 厚生労働省 周産期医療体制整備指針 (総合周産期母子医療セン ター) 1人、16床以 上で2人以上 3床 新生児集中ケ ア認定看護師 周産期医療体制整備指針 (地域周産期母子医療セン ター) 病院内に常時 3床 British Association of Perinatal Medicine
Service Standards for Hospitals providing Neonatal Care 2010 レジデント1人、 registrar 1人 (2交代制)、 consultant on call 1床 Advanced Neonatal Nurse Practitioner American Academy of Pediatrics
Guidelines for Perinatal Care 2007 レジデント1人, フェロー on call 1-2床 Advanced-Practice Neonatal Nurse
NICU医師・看護師の配置基準
Frequency distribution of Nurse cot ratios at 186 NICUs (1996/7)
UK Neonatal Staffing Study
A prospective evaluation of risk-adjusted outcomes of neonatal intensive care in relation to volume, staffing and workload in UK neonatal intensive care units.
専従医師(研修医含む)の
新生児医療従事年数(兼務含む)
0 20 40 60 80 100 120 140 160 0- 2.5- 5- 10- 15- 20- 25- 30- 35-医 師 数( 人) 新生児医療従事年数(年) n 489 平均値 8.6 標準偏差 8.2 最大値 38 最小値 0 中央値 6(松浪、藤村, 2010)
周産期母子医療センターネットワーク
15 12 11 10 9 8 7 6 5 4 3 2 1 192 722 124 548 0 100 200 300 400 500 600 700 800 新生児専任医師数別の施設数 722 192 平成9年度 平成12年度 新生児未熟児病棟の医師勤務体制 新生児科専任医師 (常勤)が担当する施設 新生児専任医師数 50 45 40 35 30 25 20 15 10 5 0 新生児専任医師数 施設数 総合周産期母子医療センターネットワーク研究班<1500g死亡率と分娩数
死亡率
分娩数 2000 1500 1000 500 0 死亡 率 30 20 10 0分娩数
R=-0.304, P=0.045 総合周産期母子医療センターネットワーク研究班<1500g死亡率とNICU夜勤看護師数
NRNICUNT 9 8 7 6 5 4 3 2 1 死亡率 30 20 10 0NICU夜勤看護師数
r=-0.356, P=0.024死亡率
'Too small ' units which could
close ( 26 )
Friarage
Buckland
Middlesex
Central Middlesex
Horton Hospital
Epsom General Hospital
Queen Elizabeth the Queen Mother
Hospital, Margate
・・・・・・
Too small which need to stay
open for geographical reasons
( 5 )
Homerton
North Devon District, Barnstaple
Pilgrim Hospital, Boston
Cumberland Infirmary
West Cumberland, Whitehaven
Paediatric medical workforce model , RCPCH 2001
英国小児科学会のNICU戦略(例)
2004-世界へ発信の前提条件
④
新生児死亡率
-新生児医療のアウトカム①-(人口動態統計、新生児ネットワーク)
新生児医療のアウトカム 同業者なら関心を持たざるを得ない情報を提供することから始まる なぜアウトカムが異なる結果になるのか? 興味↑ お互いの比較が可能であろうという予感 関連する要因がある程度明示されているとさらに身近な比較へと関心が高まる
Itabashi, K. et al. Pediatrics 2009;123:445-450
aP < .05, bP < .01, and cP < .001 for comparisons between 2005 and 2000.
N=3,065 人口動態統計値の98.4%。
日本小児科学会・新生児委員会
Mortality Rates for Extremely Low Birth Weight Infants Born in Japan in 2005
在胎期間(週)別の生存率
大阪府立母子保健総合医療センター 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% 1981~1987 1988~1992 1993~1997 1998~2002 2003~2007 2008~2010 22 23 24 25 26 27 28 29~Mortality adjusted
Time of discharge in gestational weeks
Japan
(<1500g)
(<1500g)
Zzz
zzz
Zzz
zzz
⑤
新生児医療内容のベンチマーク
相互に比較可能なデータベースの存在
• VLBW Infants ≦1500 g
• Admitted within 28 days of birth,
• to the tertiary neonatal intensive care units in Japan
• including infants who died in the delivery room
世界へ発信の前提条件
NRN Japan & NICHD
*
network
---NICHD
NRN Japan
N of NICUs
18
77
---Years
1997~2002
2003~2006
Subjects
501-1500g
<1500g
N
18,153
11,183
Mean Birth wt(g)
1033±289
1031±303
Mortality(%)
15.1 10.0
---*
National Institute for Child Health and Human Development (楠田、2011)世界へ発信
米国NICHD*network(18 NICUs)
データベースとの比較
周産期因子
(%)
0 10 20 30 40 50 60 70 80 90 100 母体ステロイド 投与率 帝王切開率 出生時気管 挿管 1分Apgar<=3 5分Apgar<=3 日本 米国(NICHD)(楠田 2010)
(%)
0 10 20 30 40 50 60 70 80 90 100RDS Surfactant CLD 28d HOT PDA Indomethacin Ligation NRNJapan NICHD
米国NICHD*network(18 NICUs)
データベースとの比較
(≦1500g)
(楠田、2011)(%)
0 10 20 30 40 50 60 70 80 90 100IVH IVH grade 3,4 PVL NEC Sepsis NRNJapan NICHD
米国NICHD*network(18 NICUs)
データベースとの比較
(≦1500g)
(楠田、2011) 0.00% 2.00% 4.00% 6.00% 8.00% 10.00% 12.00% 14.00% 16.00%2003
2004
2005
2006
2007
2008
(Year)
VON
Japan
米国Vermont-Oxford Networkとの比較
死亡率の年次推移(≦1500g)
(楠田、2011)0 0.01 0.02 0.03 0.04 0.05 0.06 0.07 0.08 0.09 0.1 2003 2004 2005 2006 2007 2008 (Year) NEC/Perforation VON Japan 0 0.05 0.1 0.15 0.2 0.25 0.3 2003 2004 2005 2006 2007 2008 (Year) IVH VON Japan 0 0.05 0.1 0.15 0.2 0.25 2003 2004 2005 2006 2007 2008 (Year) Septicemia VON Japan 2003 2004 2005 2006 2007 2008 (Year) 0 0.01 0.02 0.03 0.04 0.05 0.06 Pneumothorax VON Japan
米国Vermont-Oxford Networkとの比較
罹病率の年次推移(≦1500g)
(楠田、2011) 罹患率:国際比較(CPQCC) 0 10 20 30 40 50 60 70 80 RDS PTx Sepsis(any) NEC IVH Cystic PVL (%) CPQCC JAPANCalifornia Perinatal Quality Care Collaboration
米国カリフォルニア州
127 NICUs
データベースとの比較
(2005)罹患率
(<1500g)
(楠田、2011)カナダの17NICUs施設別死亡率
(
1996ー1997)(死亡数795/極低出生体重児19,265)
(林
2008)
施設間のベンチマークによるアウトカムの
改善運動の成果??
• 米国Vermont-Oxford Networkとの死亡率の比較
• 日本の死亡率(≦1500g)は40%程度低い
• 2003年から2008年への改善率は
Vermont-Oxford Network
11%
NRN-Japan
24%
世界へ発信
• 2012 PAS Annual Meeting Boston, MA
• April 28-May 1, 2012
• Title:
Comparison of neonatal outcomes of VLBW
neonates between Canada and Japan
(投稿中!)Tetsuya Isayama,1, Shoo K Lee, 2, 3, Xiang Y Ye, 3, Rintaro Mori4, Satoshi Kusuda, Masanori Fujimura, 6and Prakesh S Shah, 2, 3.1Division of Neonatology, University of Toronto, Toronto, Ontario, Canada;2Pediatrics, Mount Sinai Hospital, Toronto, Ontario, Canada;3Pediatrics, Micare Research Centre, Mount Sinai Hospital, Toronto, Ontario, Canada;4Collaboration for
Research in Global Women's and Children's Health, Tokyo, Japan;5Department
of Neonatology, Perinatal Center, Tokyo Women's Medical University, Tokyo, Japan and6Osaka Medical Center and Research Institute for Maternal and Child
Health, Osaka, Japan.
• Objective:To examine the differences in neonatal outcomes between Canadian Neonatal Network (CNN) and Neonatal Research Network in Japan (NRNJ) among VLBW infants.
Comparison of neonatal outcomes of VLBW neonates
between Canada
(OR=1)
and Japan
5341 VLBW infants in CNN and 9812 in NRNJ Neonatal outcomes
Outcomes Univariable (OR, 95% CI) * Multivariable (OR, 95% CI) * Mortality or major morbidity 0.94 (0.88, 1.01) 0.91 (0.82, 1.00)
Mortality 0.59 (0.53, 0.67) 0.40 (0.34, 0.47)
Severe neurological injury ** 0.55 (0.49, 0.61) 0.46 (0.40, 0.54)
Severe ROP 1.21 (1.06, 1.38) 1.54 (1.32, 1.81)
BPD 1.33 (1.20, 1.47) 1.38 (1.21, 1.57)
NEC 0.25 (0.21, 0.30) 0.23 (0.18, 0.28)
PDA ligation 0.61 (0.53, 0.69) 0.60 (0.50, 0.72)
Late onset sepsis*** 0.26 (0.24, 0.30) 0.22 (0.19, 0.25)
* (OR, 95%CI): Odds ratio of NRNJ relate to CNN and 95% confidence interval,
** Severe neurological injury: IVH (grade 3 or above) /persistent parenchymal echogenicity or periventricular leukomalacia.
International Network for Evaluation of Outcomes
(iNeo)
of Neonates
A Quality Improvement Project via Collaborative
Comparison of Population-based International Health
Services for Neonatal Care
Australia – Canada – Israel –
Japan
- New Zealand –
Spain - Sweden - UK
Comparison of Mortality and Morbidity of Very Low
Birth Weight Infants Between Canada and Japan
Pediatrics. 2012 Sep 10. [Epub ahead of print]
AUTHORS: Tetsuya Isayama, MD, a Shoo K. Lee, FRCPC, Rintaro Mori, FRCPCH,c Satoshi Kusuda, MD, d Masanori Fujimura, FRCPCH, e Xiang Y. Ye, MSc,b Prakesh S. Shah, FRCPC, a,b and the Canadian Neonatal Network and the Neonatal Research Network of Japan a; Department of Paediatrics, University of Toronto, Toronto, Canada; b; Maternal-Infant Care Research Centre, Mount Sinai Hospital, Toronto, Canada; c: Department of Health Policy, National Center for Child Health and Development, Tokyo, Japan; d; Tokyo Women`s Medical University, Tokyo, Japan; and e; Osaka Medical Center and Research Institute for Maternal and Child Health, Osaka, Japan
WHAT’S KNOWN ON THIS SUBJECT: Mortality of very low birth weight infants varies widely between regions and countries; however, the variation in morbidities after adjusting for confounders has not been adequately studied.
WHAT THIS STUDY ADDS: Composite outcome of mortality or short-term morbidity for very low birth weight infants was lower in Japan than in Canada. However, marked variations in mortality and individual morbidity exist, revealing areas for improvement in each country.
Database Quality Improvement Conference(楠
田分担班)に出席して:
It was fascinating to be able to talk to people about the
very high survival rates of preterm babies on Japanese
units
- the most striking difference is how hard the doctors
work and their level of involvement with the hands on care
of the babies –
I fear we have gone too far the other way.
September, 2010
- Kate Costeloe –
Professor of Pediatrics.
Homerton University Hospital, London
世界へ発信の前提条件
⑥
退院後の発達予後
-
新生児医療のアウトカム②-日本の課題
1.フォローアップ率
ネットワーク全体のフォローアップ率はVermont-Oxfordと同率 約70% 研究プロジェクトに限定すると、フォローアップ率は劣る 90% vs 70%2.Cognitive function評価方法
心理士の意見統一が必要、その結果1994年に新版K式発達検査を採用 Bayley 乳幼児発達検査を推奨する動きOutcome at 3 years
<1500gm n=3104
No data No NDI NDI Died later NICU death 0 10 20 30 40 50 60 70 80 90 100% 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 39 139 196 263 277 278 387 386 329 268 199 125 110 52 38 13 4 1 (n) (wk) Japan (河野、2011)Extreme Preterm Outcomes
– Neonatal Research Network
Japan 3 years
– EPICure(1995, <26w)
England and Ireland
30mo
N Eng J Med 2000;343:378-84
– NICHD(1996-1999, <25w & 500~1000g) USA 18-22mo
Pediatrics 2005;115:1645-51
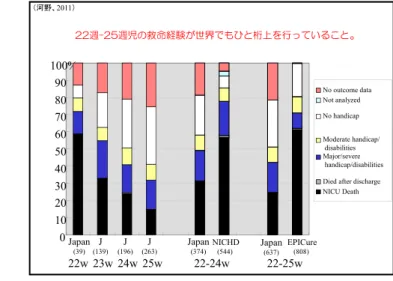
(河野、2011) 22週-25週児の救命経験が世界でもひと桁上を行っていること。
0
10
20
30
40
50
60
70
80
90
100%
Japan(39) (139)J (196)J (263)J Japan(374) NICHD(544) Japan(637)
EPICure (808) No outcome data Not analyzed No handicap Moderate handicap/ disabilities Major/severe handicap/disabilities Died after discharge NICU Death
22w 23w 24w 25w
22-24w
22-25w
(河野、2011)27, 28週児を1とした時の
下位週児のCP, DQ<70(3歳)の危険率(オッズ比)
CPの頻度は有意差がなく、DQ<70の頻度は週が小さくなるほど多い 0 1 2 3 4 5 6 7 8 9 10 27-28 25-26 22-24 27-28 25-26 22-24 27-28 25-26 22-24 27-28 25-26 22-24 (米本、河野、藤村 2010) 死亡/正常 CP /正常 DQ70未満/正常 データなし/正常 (週数) (オッズ比) P = <.0001 P = 0.009N=1,358
総合周産期母子医療センターネットワーク研究班The BAPM Annual General & Scientific Meetings
13 & 14 September 2012 Royal Welsh College of Music and Drama, Cardiff.
The larger risk of poor cognitive function than that of CP with
smaller gestation of preterm birth <29 weeks
Masanori Fujimura1, Yumi Kono2, Naohiro Yonemoto3, Satoshi Kusuda4. 1Osaka Medical Center for Maternal and Child Heath; 2Jichi Medical University, Shimotsuke; 3Translational Medical Center, National Center of Neurology and Psychiatry, Tokyo; 4Tokyo Women's Medical University; for the Neonatal
Research Network, Japan
Aims: Cognitive delay and cerebral palsy are the major risk of impairments in extremely preterm. This study tests the hypothesis that the risk
of poor cognitive function inversely correlates with gestation but weak correlation of cerebral palsy (CP) with gestation in infants born <29 weeks (w).
Methods: Subjects of study were 2520 infants <29 weeks born in 2003-2005 and cared for in the level III NICUs in Japan. They were
evaluated for their survival and neurodevelopmental impairment at three years in relation with gestation of birth. CP was assessed at follow up clinic by paediatricians. Children with developmental quotient <70 by the Kyoto Scale of Infant Psychological Development test and those being judged as delay by physicians were classified as cognitive delay.
Results: A total of 389 infants died and 1221 infants were assessed for CP and cognitive function at three years. They were classified into
three groups of 22-24w (n=259), 25-26w (n=412), and 27-28w (n=550). After adjusting sex, maternal age, plurality, outborn, prenatal steroids and delivery by cesarean section, the odds of CP and cognitive delay were calculated for each groups taking the 27-28w as a reference. Odds ratio (OR) (95% C.I.) of CP were 1.72 (1.08-2.73) in 22-24w and 1.14 (0.74-1.76) in 25-26w. Whereas, OR of cognitive delay were 5.03 (3.53-7.32) in 22-24w and 2.12 (1.51-2.97) in 25-26w. OR of death were 7.62 (5.61-10.33) in 22-24w and 2.36 (1.72-3.25) in 25-26w group.
Conclusions: The notion that “the smaller the gestation the larger the risk of impairment” may be translated to “the smaller the gestation the
larger the risk of cognitive impairment”. Factors which affect the cognitive function could be the target for extremely preterm infants in NICU care.
22-24w n=620 25,26w n=830 27,28w n=1070
Died, n(%) 209 (34) 112 (13) 68 (6) Survived, n(%) 411 (66) 718 (87) 1002 (94) Followed at 3yrs, n(%)* 304 (74) 502 (70) 659(66) Evaluated for CP and Cognitive delay, n (%)* 259 412 550
CP only, n(%)** 5 (2) 12 (3) 23 (4) Delay only, n(%)** 73 (28) 69 (17) 47 (9) CP and Delay, n(%)** 33 (13) 30 (7) 26 (5)
Table Numbers (%) of infants survived, followed and evaluation for impairments
(%)* of survived, (%)** of evaluated
死亡またはCP
23施設3952名 死亡382名 生存3570名 フォローデータなし 1151名(29%) CP評価あり 2350名 CP評価なし 69名 Median 19.1% (8.9~40.7%) 基準施設 施設ID 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% a b c d e f g h i j k l m n o p q r s t u v w 死亡またはCPの割合(%):調整前 CP 死亡 (米本、河野、藤村 2010) Japan 総合周産期母子医療センターネットワーク研究班NMCS Neonatologist’s Dinner
The 6
thWorld Congress of Perinatal Medicine
Sept 14, 2003, Rihga Royal Hotel, Osaka.
Ola Didrik Saugstad , Malcom I. Levene, Victor Yu, Henrik Hagberg
Jay Roberts, Jeffrey Maisels, Jeffrey Whitsett, Christian Speer,
Anne Greenough, Linda Wright, Peter Gluckman,
Berit H.Munkeby, Karin Nelson
International Neonatal Forum
“Personal view on the management of babies
born at less than 26 weeks‘ gestation”
23rd April, 2010 Hotel Metropolitan Morioka, MoriokaChair:
Masanori Tamura, Masanori Fujimura Speakers;
• Rintaro Mori, Yumi Kono, Satoshi Kusuda, Fumika Yamaguchi • Avroy A. Fanaroff
Professor, Rainbow Babies & Children's Hospital,
Department of Pediatrics, Case Western Reserve University, USA • Neil Marlow
Professor, Department of Neonatology, UCL Institute for Women's Health, UK President, European Society for Pediatric Research
総合周産期母子医療センターネットワーク研究班
Oriental Congress of Pediatrics
Quality improvement of neonatal care and
neonatal research network in Japan
Nov 11, Seoul
Oct 27-30, Shanghai
Quality improvement of neonatal care and
neonatal research network in Japan
Japan
世界へ発信の前提条件
⑦
研究能力、論文作成能力
生物統計、疫学等
• 「世界へ発信の前提条件①から⑥を着実の構築してゆけ
ば、最後の
⑦
へ到る道程の8割方達成していると考えら
れる。
• 「新生児医療の日本から世界への発信」を手順なしに漫
然と空想するのではなく、
戦略的に一歩一歩着実に
進め
ることが大切である。
Pediatrics. 2006 Oct;118(4):e1130-8. Epub 2006 Sep 1.
Morbidity and mortality of infants with very low birth weight in Japan: center variation.
Kusuda S, Fujimura M, Sakuma I, Aotani H, Kabe K, Itani Y, Ichiba H, Matsunami K, Nishida H; Neonatal Research Network, Japan METHODS:
A large multicenter neonatal research network that included level III NICUs from throughout Japan was established. A standardized mortality rate was formulated by giving a ratio of the observed deaths and the predicted deaths based on a 100-g birth weight interval mortality. A regression model was used to predict the factors that affect neonatal mortality.
RESULTS:
The network included 37 centers and 2145 infants weighing < or = 1500 g, born or admitted to the centers in 2003. The standardized mortality rate varied among the facilities (range: 0%-30%). Among all of the very low birth weight infants, 14% were outborn infants, 72% were delivered by cesarean sections, 27% had patent ductus arteriosus, 3% had gastrointestinal perforation, 8% had bacterial sepsis, and 13% had intraventricular hemorrhage. Medical interventions involved were: 41% antenatal corticosteroids, 54% surfactant therapy, 18% postnatal steroids for chronic lung disease, and 29% high-frequency oscillatory ventilation. We found variations in the medical interventions and the clinical outcomes among the centers.
CONCLUSIONS:
The overall survival rate for very low birth weight infants among neonatal centers in Japan was approximately 90%. However, differences in the morbidity and mortality were observed among these centers.
Pediatr Int. 2011 Dec;53(6):1051-8. Epub 2011 Nov 14.
Outcomes of very-low-birthweight infants at 3 years of age born in 2003-2004 in Japan.
Kono Y, Mishina J, Yonemoto N, Kusuda S, Fujimura M Source
Department of Pediatrics, Jichi Medical University, Shimotsuke, Tochigi, Japan. [email protected]
Abstract METHODS:
A total of 3104 VLBW infants born in 2003 and 2004 registered in a NICU-network database were followed in the study.
RESULTS:
A total of 257 infants died and follow-up data were obtained from 1826 infants. Of the 1826 infants, 155 (8.5%) had cerebral palsy, 25 (1.4%) had visual impairment, and 12 (0.7%) had hearing impairment. Of the 1197 infants in whom DQ was measured, 184 (15.4%) had DQ < 70. The proportion of NDI in the evaluated infants was 19.2% (n= 350), ranging from 11.9% (BW 1251-1500 g) to 42.0% (BW ≤ 500 g). Odds ratios (95%CI) of NDI or death against the group BW 1251-1500 g were 20.62 (13.29-31.97) in BW ≤ 500 g, 7.25 (5.45-9.64) in BW 501-750 g, 2.85 (2.12-3.82) in BW 751-1000 g and 1.18 (0.85-1.64) in BW 1001-1250 g.
CONCLUSION:
the incidence of NDI was similar to previous overseas cohort studies despite the higher survival proportion in our study.
Pediatr Int. 2011 Dec;53(6):930-5.
Neonatal correlates of adverse outcomes in very low-birthweight infants in the NICU Network.
Kono Y, Mishina J, Yonemoto N, Kusuda S, Fujimura M; NICU Network, Japan. Source
Department of Pediatrics, Jichi Medical University, Tochigi, Japan. [email protected] METHODS:
Subjects were infants with birthweight ≤ 1500 g who were cared for in the tertiary neonatal intensive care units in Japan
RESULTS:
Of the 3104 subjects, 257 died and 1826 were evaluated at 3 years of age. Cystic periventricular leukomalacia (PVL; OR, 23.9; 95%CI: 11.0-51.7), gastrointestinal perforation (OR, 8.5; 95%CI: 2.8-25.4), intraventricular hemorrhage (IVH) grade 3 or 4 (OR, 3.1; 95%CI: 1.3-7.2) and sepsis (OR, 2.6; 95%CI: 1.4-4.8) were neonatal factors significantly associated with an increased risk of death or CP. Significant correlates with death or developmental delay were cystic PVL (OR, 7.9; 95%CI: 3.7-16.8), gastrointestinal perforation (OR, 6.3; 95%CI: 1.9-20.8), sepsis (OR, 2.8; 95%CI: 1.6-4.8), IVH grade 3 or 4 (OR, 2.6; 95%CI: 1.2-5.7), chronic lung disease at 36 weeks of corrected gestational age (OR, 1.6; 95%CI: 1.1-2.4) and treatment for retinopathy of prematurity (ROP; OR, 1.5; 95%CI: 1.0-2.3).
CONCLUSION:
Cystic PVL, gastrointestinal perforation, IVH and sepsis correlated with both death or CP and death or developmental delay in VLBW infants. Chronic lung disease at 36 weeks and treatment for ROP were associated with death or developmental delay, but not with death or CP.
J Pediatr. 2011 Jul;159(1):110-114.e1. Epub 2011 Feb 22.
Antenatal corticosteroids promote survival of extremely preterm infants born at 22 to 23 weeks of gestation.
Mori R, Kusuda S, Fujimura M; Neonatal Research Network Japan. Collaborators (90)
Department of Global Health Policy, Graduate School of Medicine, The University of Tokyo, Tokyo, Japan. [email protected]
STUDY DESIGN:
We performed a retrospective analysis of 11,607 infants born at 22 to 33 weeks of gestation between 2003 and 2007 from the Neonatal Research Network of Japan. We evaluated the gestational age effects of ACS administered to mothers with threatened preterm birth on several factors related to neonatal morbidity and mortality. RESULTS:
By logistic regression analysis, ACS exposure decreased respiratory distress syndrome and severe intraventricular hemorrhage in infants born between 24 and 29 weeks of gestation. Cox regression analysis revealed that ACS exposure was associated with a significant decrease in mortality of preterm infants born at 22 or 23 weeks of gestation (adjusted hazard ratio, 0.72; 95% CI, 0.53 to 0.97; P=.03). This effect was also observed at 24 to 25 and 26 to 27 weeks of gestation and in the overall study population. CONCLUSIONS:
ACS exposure improved survival of extremely preterm infants. ACS treatment should be considered for threatened preterm birth at 22 to 23 weeks of gestation.
Pediatr Res. 2012 Aug 24. [Epub ahead of print]
Trends in morbidity and mortality among very low birth weight infants from 2003 to 2008 in Japan.
Kusuda S, Fujimura M, Uchiyama A, Totsu S, Matsunami K. Source
Department of Neonatology, Maternal and Perinatal Center, Tokyo Women's Medical University, Tokyo, Japan.
Abstract
Methods:This is a cohort study of VLBW infants born from 2003 through 2008. Results:Over the 6-year period, 19,344 infants were registered and analyzed. Crude mortality rates among the infants at discharge decreased significantly (from 10.8 to 8.7%) during the study period.
Significant increases were observed in some morbidities, including symptomatic patent ductus arteriosus with an odds ratio of 1.11 (1.09-1.13); late-onset adrenal insufficiency, 1.21 (1.17-1.26); and necrotizing enterocolitis/intestinal perforation, 1.10 (1.01-1.12). However, the severe form of intraventricular hemorrhage, with an odds ratio of 0.98 (0.92-0.99), decreased significantly. Risk-adjusted trends in other morbidities showed no significant change.
Conclusions:Mortality of VLBW infants decreased significantly over the 6-year study period. Decreasing morbidity is essential for further improvement in the outcomes in VLBW infants.