緒 言
ア レ ル ギ ー 性 気 管 支 肺 ア ス ペ ル ギ ル ス 症(allergic bronchopulmonary aspergillosis,ABPA)は 1952 年に Hinson らにより初めて報告された1)疾患である.Asper- gillus がアトピー素因を持つ気管支喘息患者の気管支に 持続的に腐生して発症する.I 型及び III 型アレルギー 反応によると考えられているが,病因については不明な 点が多い.多彩な臨床像を呈し,近年注目されている疾 患であるが,今回 ABPA 治療中に胸水貯留により再燃 を来たした症例を経験したのでここに報告する.
症 例
症例:61 歳,男性.
主訴:喘鳴.
既往歴:小児期より気管支喘息.51 歳 上行結腸癌 にて手術.54 歳 癒着性イレウス,この時より HCV 抗 体陽性であることが判明した.
家族歴:特記事項なし.
喫煙歴:never smoker.
職歴:製紙業.
現病歴:昭和 56 年より気管支喘息にて当科通院中で,
Fluticasone 800
µ
g!
日,pranlukast 450 mg!
日,pro- caterol 100µg!
日にて加療していた.平成 13 年 11 月より左胸水,WBC 8,690
! µ
l(Eo 21.2%)と末梢血好酸球 増多を認めた.胸水細胞診では好酸球の出現が目立つが,悪性細胞は認めなかった.精査目的入院を勧めるも希望 されず外来にて経過観察となった.平成 14 年 4 月 2 日 の外来受診時に胸部 X 線写真上左中肺野に浸潤影を認 め,WBC 9,560!
µl(Eo 31.2%,2,982! µl)と好酸球も増
加したため,精査目的に 4 月 8 日に入院した.入 院 時 身 体 所 見:身 長 160 cm,体 重 53.4 kg,体 温 36.8℃,血 圧 150
!
108 mmHg,脈 拍 66!
分・整.貧 血・黄疸なし,頸部リンパ節触知せず,胸部:心音正常,呼 吸音 wheeze を全肺野にて聴取.腹部:肝・脾腫なし,
手術瘢痕あり.両上肢に振戦あり,ばち指なし,下腿浮 腫なし.
入院時検査所見:WBC 10,480
! µ
l(Eo 24.4%,実数 2,498!µl)と好酸球増加を認めた.CRP
2.0 mg!dl で,血 沈 は 45 mm
!
h と 亢 進 し て い た.IgE は 12,228 U!
ml と異常高値を示し,アスペルギルス沈降抗体が陽性で あった(Table 1).胸部 X 線写真では右上肺野に淡い浸潤影と左肋骨横 隔膜角の鈍化を認めた(Fig. 1).胸部 CT では右上葉に 直径約 20 mm の結節状の consolidation,右上葉枝の中 枢性気管支拡張像,左上葉大動脈弓脇にも consolidation,
さらに右中下葉と左下葉に小葉中心性の小粒状影を認め た(Fig. 2).他に左 下 葉 外 側 に は 板 状 の consolidation と胸膜肥厚像を認めた.入院時の喀痰細胞診では異型細 胞はなく,多数の好酸球を認めた.
臨床経過:4 月 9 日に気管支鏡を施行し,右 B3bより
●症 例
再燃時に胸水貯留を来たしたアレルギー性気管支 肺アスペルギルス症の 1 例
小笠原 隆
1)家里 憲
1)岡部 浩典
1)村田 研吾
1)小南 聡志
1)冨田 和宏
1)中村 秀範
1)要旨:症例は 61 歳の男性.小児期より気管支喘息あり,当科外来通院中であったが,末梢血好酸球増多,
胸部 X 線写真での移動する浸潤影を認め,精査目的で入院した.血清 IgE 高値,アスペルギルスに対する 即時型皮内反応陽性,血清沈降抗体陽性,胸部 CT での中枢性気管支拡張像を認め,アレルギー性気管支肺 アスペルギルス症(以下 ABPA)と診断した.prednisolone(以下 PSL)を 30 mg
!
日より開始,5 mg!
日 まで漸減したところで右胸水貯留を認めた.PSL 20 mg!
日まで増量し,抗真菌薬 itraconazole を併用した ところ胸水は減少した.ABPA に伴う胸水は数例が報告されているが,本症例のように再燃時に胸水貯留を 来たすことは非常に稀であり報告した.キーワード:アレルギー性気管支肺アスペルギルス症,胸水,イトラコナゾール,IgE
Allergic bronchopulmonary aspergillosis,Pleural effusion,Itoraconazole,IgE
〒430―8558 静岡県浜松市住吉 2―12―12
1)聖隷浜松病院呼吸器内科
(受付日平成 15 年 4 月 25 日)
Table 1 Laboratory findings
Pulmonary function tests Serology
Hematology
VC 2.04 l
CRP 2.0 mg/dl
WBC 10,480 / μ l
%VC 61.2 %
IgG 1,687 mg/dl
Neu 54.6 %
FEV1.0 0.84 l
IgA 387 mg/dl
Eo 24.4 %
FEV1.0% 51.5 %
IgM 127 mg/dl
Ba 0.3 %
BALF(2002. 4. 23)
IgE 12,228 U/ml
Mo 4.1 %
Recovery rate Bood gas analysis(room air)
Ly 16.6 %
40/150 ml(26.7%)
PH 7.411
Hb 14.9 g/dl
Total cell counts PCO2 45.8 torr
Plt 43.1 × 104 / μl
0.35 × 105 /ml
PO2 68.9 torr
Serum chemistry
Neu 10 %
HCO3− 28.4 mEq/l
TP 8.5 g/dl
Eo 4 %
β-D-glucan 11.3 pg/ml
Alb 4.8 g/dl
Ly 35 %
IgE(RAST)
GOT 21 U/l
M φ 51 %
Aspergillus: positive
GPT 15 U/l
CD4/8 3.08
Specific IgG antibody
LDH 195 U/l
Aspergillus: positive
ALP 271 U/l
Skin test γ-GTP 15 U/l
Immediate reaction: positive
T-Bil 0.9 mg/dl
Arthus reaction: positive
BUN 15 mg/dl
Cre 0.80 mg/dl
Na 137 mEq/l
K 4.5 mEq/l
Cl 103 mEq/l
気管支肺胞洗浄(BAL)を行った.回収率が悪く poor study であったが,洗浄液からは一般細菌,抗酸菌,真 菌のいずれも培養されなかった.気管支鏡後に喘息発作 を生じ,betamethasone 4 mg
!
日の点滴静注を 2 日間 行ったところ,喘息症状の改善とともに胸部 X 線写真 にて浸潤影は消失した. 4 月 23 日に気管支鏡を再検し,右 B4より BAL を行った.BAL 中の好酸球増加はなく,
真菌も検出されなかったが,リンパ球分画の増加を認め た(Table 1).
Fig. 1 Chest radiograph on admission to our hospital on April 8, 2002, showing infiltration in the right upper lung field.
Fig. 2 Chest CT scan on admission, showing nodular consolidations and central bronchiectasis in the right upper lobe.
以上より本症例は Rosenberg の診断基準の一次基準 をすべて満たし,ABPA と確定診断された.しかし,
入院中に耳鼻科にて慢性副鼻腔炎の合併を診断されたこ と,胸部 CT 上の小葉中心性の小粒状影の存在からびま ん性汎細気管支炎の合併も否定できないこと,BAL で は好酸球優位の所見が得られなかったこともあり,さら に両上肢の振戦や以前見られた下肢のしびれからはアレ
ルギー性肉芽腫性血管炎等も否定できず,患者本人も確 定診断を望んだため,5 月 14 日に胸腔鏡下肺生検(右 S2,S5)を施行した.
肺生検組織の HE 染色所見(Fig. 3)では間質内の著 明な好酸球浸潤を認め,導管部細気道の上皮下に好酸球,
リンパ球が中等度に浸潤していた.また,細気管支上皮 化生を示す虚脱した肺胞領域にもこれらの炎症細胞浸潤 が見られ,好酸球性肺炎の病理像に一致した所見と考え られた.一部には肺胞腔内および細気管支内線維化層を 認め,器質化肺炎の所見も認めた.血管炎の所見はなく,
アレルギー性肉芽腫性血管炎は否定された.以上より好 酸球性肺炎像は,ABPA に伴う肺病変と判断した.
術後喘息発作もあり,5 月 15 日より PSL 30 mg
!
日を 開始した.その後は呼吸状態も落ち着き,5 月 20 日に 退院した.外来にて PSL 5 mg
!
2 週の割合で漸減していったが,喘息発作や胸部 X 線写真での浸潤影の再燃はなく,IgE も順調に低下した(Fig. 4).9 月 19 日に PSL 5 mg
!
日 まで減量したところ,平成 14 年 10 月 17 日の外来受診 時に労作時の息切れ が 出 現 し 末 梢 血 好 酸 球 の 再 増 加(WBC 8,640
! µ
l,Eo 13.3%)を認めた.胸部 X 線写真上,右胸水の貯留を認めた(Fig. 5)ため同日胸腔穿刺を施 行した.血性胸水を計 960 ml 排液した.胸水は Table 2 に示すごとく滲出性で好酸球の増多を認めた.培養では 有意菌を検出せず,異型細胞も認めなかった.胸水中 ADA は 25.5 IU!
l
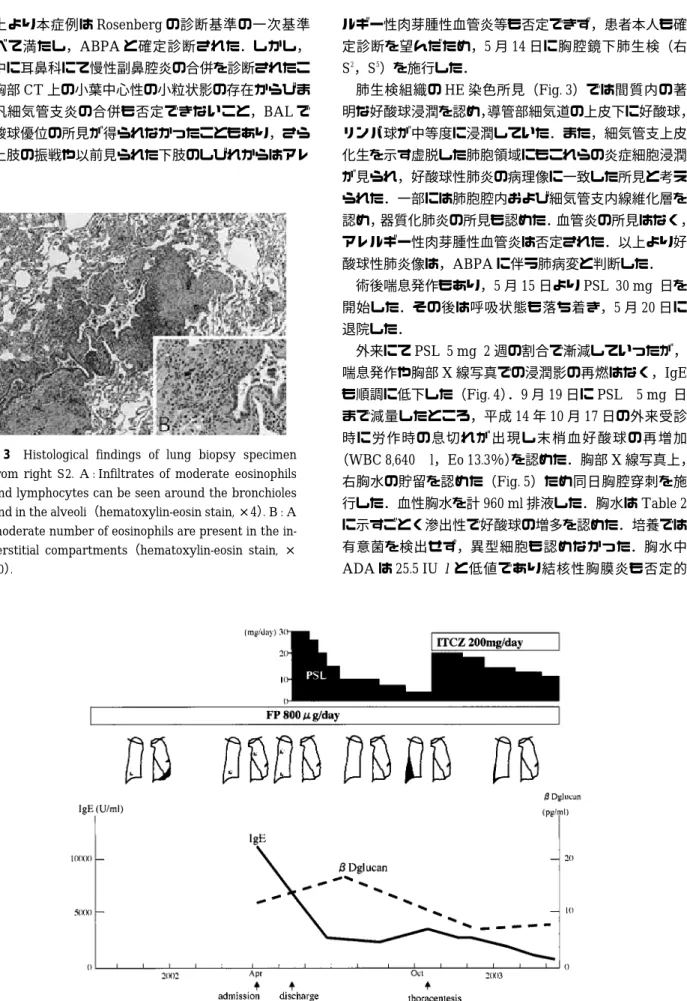
と低値であり結核性胸膜炎も否定的 Fig. 3 Histological findings of lung biopsy specimenfrom right S2. A : Infiltrates of moderate eosinophils and lymphocytes can be seen around the bronchioles and in the alveoli(hematoxylin-eosin stain, ×4). B : A moderate number of eosinophils are present in the in- terstitial compartments(hematoxylin-eosin stain, × 20).
Fig. 4 Clinical course
Table 2 Laboratory findings(2002. 10. 17)
Pleural effusion Hematology
WBC 1,570 / μ l
WBC 8,640 /μ l
Neu 35.9 %
Neu 53.8 %
Eo 13.5 %
Eo 13.3 %
Ba 2.3 %
Ba 0.5 %
Mo 5.8 %
Mo 5.7 %
Ly 42.5 %
Ly 26.7 %
Hb 2.2 g/dl
Hb 14.2 g/dl
Ht 7.1 %
Plt 32.7 × 104 / μl
TP 5.1 g/dl
Serum chemistry
Glu 57 mg/dl
TP 7.5 g/dl
LDH 918 U/l
Alb 4.1 g/dl
Amy 42 IU/l
GOT 16 U/l
PH 7.306
GPT 11 U/l
ADA 25.5 IU/l
LDH 199 U/l
CEA 1.4 ng/ml
ALP 221 U/l
hyaluronic acid 34.8 ng/ml γ-GTP 14 U/l
cytology class Ⅱ
T-Bil 0.8 mg/dl
acid-fast bacteria negative
BUN 12 mg/dl
other bacteria negative
Cre 0.90 mg/dl
Na 140 mEq/l
K 5.1 mEq/l
Cl 102 mEq/l
Serology
CRP 4.2 mg/dl
IgE 3,627 U/ml
であった.
同日の血清 IgE は 3,627 U
!
ml と再び著増しており,ABPA の再燃に伴う胸水の可能性を考え,10 月 24 日よ り PSL 20 mg
!
日に増量し,抗真菌薬イトラコナゾール(ITCZ)200 mg
!
日も併用開始した.その後,胸水は減 少し,IgE 値も低下していったため,外来にて PSL を 慎重に漸減中である.考 察
ABPA は Hinson らの報告1)以後,わが国では稀な疾 患として考えられていたが,疾患概念の普及につれ症例 報告数も増えている.
アレルギー性気管支肺真菌症の病理像としては気管支 内粘液栓子,気管支中心性肉芽腫症,好酸球性肺炎など の変化が観察される2).蛇沢ら3)はアレルギー性気管支肺 アスペルギルス症・真菌症の手術例 5 例の病理検討を 行っている.全例に著しい好酸球を伴う硬い気管支内粘 液栓子を認め,これにより気管支は限局的に拡張し,中 枢性気管支拡張像を呈していた.肺野末梢病変として,
気管支中心性肉芽腫症および黄色肉芽腫病変,好酸球性 肺炎,器質化肺炎などが認められた.これらは粘液栓子 から散布された真菌により引き起こされた二次的病変と 考えられると考察されている.本症例の生検組織が末梢 肺組織であったことから,気管支内粘液栓子を確認でき なかったが,蛇沢らの報告に一致する好酸球性肺炎や器 質化肺炎像を確認できた.この病理所見に加え,喘息の 既往,末梢血好酸球の増多,アスペルギルスの皮内反応 Fig. 5 Chest radiograph on October 17, 2002, showing
pleural effusion in the right lung.
陽性,アスペルギルス血清沈降抗体陽性,肺浸潤影,胸 部 CT での中枢性気管支拡張像の存在など,本症例は Rosenberg の診断基準を満たし ABPA と確定診断され た.
胸水を伴う ABPA の報告は少なく,Murphy ら4)の 2 例と O connor ら5)の 1 例である.本症例は平成 14 年 10 月 17 日の胸水細胞診で中等量のリンパ球と間葉系細胞 の出現が目立ち悪性所見は認めなかった.Murphy ら4)
の報告した 2 例いずれも胸水中にリンパ球と中皮細胞の 増 加 を 認 め,そ の 培 養 で 有 意 菌 は 検 出 し な か っ た.
O connor ら5)の報告例では胸水中の好中球が 95% と増 加していたが同様に培養では有意菌を認めなかった.こ れらの 3 例すべてステロイドにて治療を行い胸水の消失 を得ている.Murphy ら4)の報告した 2 例中の 1 例では PSL 減量中に胸水の再増加を認め,ステロイドを増量 し胸水は消失した.ABPA 症例における胸水貯留の機 序についてはいまだに明らかにされていないが,肺組織 の炎症に隣接した胸膜の炎症性反応により胸腔内滲出液 が貯留する5)という機序や,肺の虚脱により胸腔内の陰 圧が増し,胸水が貯留するといった機序6)が推察されて いる.本症例は入院前の平成 13 年 11 月にも左胸水貯留 を認めていたが,これも ABPA に伴う胸水であった可 能性が高く,今回の右胸水貯留は 2 回目であったと考え られる.胸腔鏡下肺生検の影響も疑われたが,術後時間 が経っていること,胸水貯留に伴って IgE の増加が見 られたこと,以前にも胸水貯留のエピソードがあること,
胸水が ABPA の治療に反応し減少したことから,ABPA に伴う胸水と判断した.
ABPA の治療としては急性期には全身ステロイド投 与が行われることが多い.しかし,ステロイドで一時的 な寛解は得られても,A. fumigatus が陰性化せず気管支 内で増殖することにより抗原刺激が持続すれば,再燃す る可能性が高い.再燃を繰り返している症例では徐々に 肺組織の破壊が進行し肺線維症に至る.さらにステロイ ド投与はアスペルギルスの易感染要因として重要視され ており,ステロイド長期投与がかえって侵襲性への病態 の移行を引きおこす可能性も示唆される7)〜10).本症例で も再燃時に PSL 増量に加え抗真菌薬 ITCZ を投与した.
ITCZ は肺組織中で高濃度となるため,アスペルギルス の抗原刺激を減少させることで効果を発揮するといわれ ている11).ITCZ を併用した方がステロイドの減量が速 く行うことができるという報告12)や,ステロイド剤依存 性の ABPA 患者に対し,ITCZ の追加投与がプラセボ に比べ明らかに有効である8)という報告もある.その後 も ABPA に対しての ITCZ の有効性が多数報告されて いる13)〜15).
ABPA の治療経過の観察の指標としては,血清総 IgE
値16)や胸部 X 線写真での浸潤影が有効とされている.本 症例でも PSL 投与によって IgE は著明に低下したが,
右胸水貯留時には IgE の再増加も認めた.さらに,PSL を増量し ITCZ を加えてからは,胸水減少とともに再び IgE 値は減少しており,病勢を反映しているものと思わ れた.血中(1→3)-
β
-D-グルカン値が ABPA の経過観察 指標になりうる可能性の報告17)もあり,本症例でも追跡 したが,明らかな関連性は見出せなかった.本症例は ABPA と診断後,PSL 減量中に右胸水貯留 にて再燃し,PSL 増量と ITCZ の併用にて良好に治療し 得た興味ある症例であり,ここに報告した.
文 献
1)Hinson KFW, Moon AJ, Plummer NS : Broncopul- monary aspergillosis. a review and a report of eight new cases. Thorax 1952 ; 7 : 317―334.
2)William D. Travis, Thomas V. Colby, Michael N.
Koss, et al : Non-Neoplastic Disorders of the Lower Respiratory Tract. 2002 ; 415―419.
3)蛇沢 晶,田村厚久,倉島篤行,他:手術例から見
たアレルギー性気管支肺アスペルギルス症・真菌症 の病理形態学的研究.日呼誌 1998 ; 36(4): 330―
337.
4)Murphy D, Lane DJ, et al : Pleural effusion in aller- gic bronchopulmonary aspergillosis : Two case re- ports. Br J Dis Chest 1981 ; 75 : 91―95.
5)Terence M. O connor, Aonghus O donnell, et al : Allergic bronchopulmonary aspergillosis : A rare cause of pleural effusion. Respirology 2001 ; 6 : 361―
363.
6)Panchal N, Bhagat R, et al : Allergic bronchopulmon- ary aspergillosis : The spectrum of computed to- mography appearances. Respir Med 1997 ; 91 : 213―
219.
7)河南里江子,河村哲治,中原保治,他:エリスロマ イシンとフルコナゾールが奏効したアレルギー性気 管支肺アスペルギルス症の 1 例.日呼誌 1999 ; 37
(4): 327―332.
8)Stevens DA, Schwartz HJ, Lee JY : A randomized trial of itraconazole in allergic bronchopulmonary aspergillosis. N Engl J Med 2000 ; 342 : 756―762.
9)Riley DJ, Mackenzie JW, Uhlman WE, et al : Allergic bronchopulmonary aspergillosis : evidence of lim- ited tissue invasion. Am Rev Respir Dis 1975 ; 111 : 232―236.
10)Rafferty P, Biggs BA, Crompton GK, et al : What happens to patients with pulmonary aspergilloma?
Analysis of 23 cases. Thorax 1983 ; 38 : 579―583.
11)Watkins DN, Badcock NR, et al : Itraconazole con-
centrations in airway fluid and tissue. Br J Clin Pharmac 1992 ; 33 : 206―207.
12)Mannes GPM, Van Der Heide S, et al : Itraconazole and allergic bronchopulmonary aspergillosis in twin brothers with cystic fibrosis. Lancet 1993 ; 341 : 492.
13)Wark PA, Hensley MJ, Saltos N, et al : Anti- inflammatory effect of itraconazole in stable allergic bronchopulmonary aspergillosis : a randomized con- trolled trial. J Allergy Clin Immunol 2003 ; 111(5):
952―957.
14)Moss RB : Allergic bronchopulmonary aspergillosis.
Clin Rev Allergy Immunol 2002 ; 23(1): 87―104.
15)Wark P, Wilson AW, Gibson PG : Azoles for allergic bronchopulmonary aspergillosis associated with asthma. Cochrane Database Syst Rev 2001 ;(4): CD 001108.
16)Patterson R, Greenberger PA : Management of al- lergic bronchopulmonary aspergillosis. In : Patter- son R, Green berger PA, Roberts ML, eds, Allergic bronchopulmonary aspergillosis. Ocean Side Publi- cations Rhode Island 1995 ; 35―38.
17)柴田和彦,藤村政樹:アレルギー性気管支肺アスペ ルギルス症における血中(1→3)-β-D-グルカン値の 検討.日呼誌 2001 ; 39(6): 383―388.
Abstract
A case of pleural effusion associated with allergic bronchopulmonary aspergillosis during a relapse of the disease
Takashi Ogasawara, Ken Iesato, Hirofumi Okabe, Kengo Murata, Satoshi Kominami, Kazuhiro Tomita and Hidenori Nakamura
Division of Respiratory Disease, Seirei Hamamatsu Hospital, 2―12―12 Sumiyoshi, Hamamatsu, Shizuoka 430―8558, Japan
A 61-year-old man with history of bronchial asthma since childhood was admitted to our hospital for examina- tion of eosinophilia and of lung infiltration seen in the chest radiograph. Allergic bronchopulmonary aspergillosis
(ABPA)was diagnosed on the basis of the following findings : elevated serum IgE level, positive immediate skin reaction to Aspergillus antigen, the presence of precipitating antibodies against Aspergillus antigen, and central bronchiectasis. Oral prednisolone administration(30 mg daily)was started. During the course of reducing the prednisolone dose by up to 5 mg per day, pleural effusion appeared in the right lung. It was speculated that this eosinophilic exudative effusion was associated with a relapse of ABPA. After treatment with the dose of predniso- lone increased to 20 mg per day and with oral itraconazole, the pleural effusion disappeared. We report a rare case of pleural effusion associated with ABPB on relapse.