緒 言
が ん 患 者 に 対 す る 緩 和 ケ ア は, World Health Organization (WHO) によると患者およびその家族の quality of life (以下, QOL) を改善するためのアプローチと定義されている1). 海外では, 悪性腫瘍患者に対して緩和ケア介入による QOL の改善が報告されている2〜4). また, 肺がん患者に対する早期緩 和ケア介入効果による予後の延長が示された5) . わが国におい ても, 悪性腫瘍患者への緩和ケアに関する調査が行われてい る6) が, 前向きに QOL の前後比較を行った報告は少ない. 今回われわれは, 緩和ケアチーム介入効果について患者の QOL 変化を用いて前向きに検討した.
対象と方法
1 対 象 2009 年 11 月 1 日から 2010 年 3 月 30 日まで, 神戸大学医学 部附属病院 呼吸器内科および腫瘍・血液内科病棟に入院した 悪性腫瘍患者で, 緩和ケアチームが介入した患者を対象とし た. 適格基準は, 18 歳以上で入院時に悪性腫瘍と確定診断され ており, 日本語で質問用紙の回答が可能であることとした. 意 識障害や認知機能障害のため質問に回答困難な患者, 治療医が 不適切と判断した患者は除外した. 本研究開始時に書面にて同 意を取得した. 2 方 法The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 15 Palliative Care (EORTC QLQ− C15−PAL)7) は, 介入時と 1 週後, 4 週後または退院時の計 3 回, 病棟看護師が患者に用紙を配布し, 患者が自己記入した. 質問 用紙の回収は, 病棟看護師が行った. なお, 本研究は当院医学倫理委員会の承認後に行った. 3 EORTC QLQ−C−15−PAL
QOL 評価には, がん患者用の QOL 調査票である EORTC QLQC15−PAL を用いた.
EORTC QLQ−C15−PAL は, 緩和ケアを受けるがん患者に適 用できるように短縮されたQOL 尺度であり, 日本語での信頼 性と有用性も証明されている8, 9)
. スコアリングは, 15 の質問 項目がドメインに割り当てられ, global QOL (item 15), 2 つの 機 能 ス ケ ー ル〈physical functioning; PF (item 1〜3), emotional functioning; EF (item 13, 14)〉と 7 つの症状スケール〈fatigue; FA (item 7, 11), nausea and vomiting; NV (item 9), pain; PA (item 5, 12), dyspnea; DY (item 4), insomnia; SL (item 6), appetite loss; AP (item 8), constipation; CO (item 10)〉から scoring manual に従っ て計算した10). PF, EF, global QOL はスコアが高いほど良好であ
ることを示し, FA, NV, PA, DY, SL, AP, CO はスコアが高いほど 不良であることを示す.
短報
緩和ケアチーム介入によるがん患者
QOL の変化についての検討
新家 治子
1), 坂下 明大
1), 石橋 有希
1), 太田垣加奈子
1),
藤原 由佳
1), 五百蔵武士
1), 田宮 裕子
1), 小谷 義一
2),
向原 徹
3), 南 博信
3), 西村 善博
1, 2) 1) 神戸大学医学部附属病院 緩和ケアチーム, 2) 同 呼吸器内科, 3) 同 腫瘍・血液内科 受付日 2012 年 1 月 4 日/改訂日 2012 年 3 月 9 日/受理日 2012 年 4 月 15 日 【目的】 日本人がん患者を対象に, 緩和ケアチームの介入効果を QOL の変化によって明らかにする. 【対象と方法】 2009 年 11 月 1 日から 2010 年 3 月 30 日まで, 神戸大学医学部附属病院 呼吸器内科および腫瘍・血液内科病棟に入院中の患 者を対象とし, 緩和ケアチーム介入前後の QOL をアンケート形式で前向きに評価した. QOL の評価は介入時, 介入 1 週後 および 4 週後に EORTC QLQ−C15−PAL を用いて行った. 【結果】 35 人の患者をエントリーし, 26 人の患者で 1 週後の評 価が, 15 人で 4 週後の評価が可能であった. 1 週後に, 15 の評価項目のうち, pain の改善がみられた (p<0.05). 4 週後に, dyspnea と pain の項目で改善が得られた (p<0.05). 【結語】 EORTC QLQ−C15−PAL を用いて緩和ケアチームの介入効果 を前向きに検討した. 介入が短期間であっても, 身体症状の改善は得られた.Palliat Care Res 2012; 7(2): 368−73
Key words: 緩和ケアチーム, QOL, EORTC QLQ−C15−PAL
Corresponding author: 坂下明大 神戸大学医学部附属病院 緩和ケアチーム 〒650−0017 兵庫県神戸市中央区楠町 7−5−2
緩和ケアチーム介入によるがん患者 QOL の変化 369 4 緩和ケアチームの介入 緩和ケアチームは, 患者の希望または治療医の依頼を受け, 書面による患者の介入同意を得た後, コンサルテーション型の 介入を開始した. 初回の面談は, 患者の病室または病棟で行い, 緩和ケア医, 専従看護師, 臨床心理士, 専任薬剤師が同席した. 面談後に, 依頼内容に従って必要な介入を行った. 2 回目以降 の面談は, 緩和ケアチームの判断で, 身体症状には緩和ケア医 と専従看護師が, 精神症状にはおもに臨床心理士が, 平日に 1 日1 回以上患者のもとへ訪室した. 面談後, 主治医への薬物推 奨やカウンセリングなどを行った. 主要評価項目は, Follwell らの報告4)と同様に各ドメインの1
週後, 4 週後のスコア変化量とした. PF, EF, global QOL につい ては1 ポイント以上の上昇を, また FA, NV, PA, DY, SL, AP, CO については1 ポイント以上の低下を改善とした. また, 観察期 間は対象患者が治療目的の入院が多く, 4 週間を最大期間と設 定した. 5 統 計 統計解析は, ドメインごとに介入前と 1 週後, および 4 週後 または退院時の差の検定を行った. まず, データが正規分布に 従うかどうかをShapiro−Wilk 検定で確認した. 正規分布に従う 変数は, 1 週後が PF, EF, FA, global QOL で, 4 週後が PF, PA, EF, LA, global QOL であった. これらの変数に対しては対応のある t 検定を, それ以外の変数は, Wilcoxon の符号つき順位和検定 を行った. すべての検定の有意水準は p<0.05 とした. すべて の統計解析に, SPAW statistics 18 を使用した.
結 果
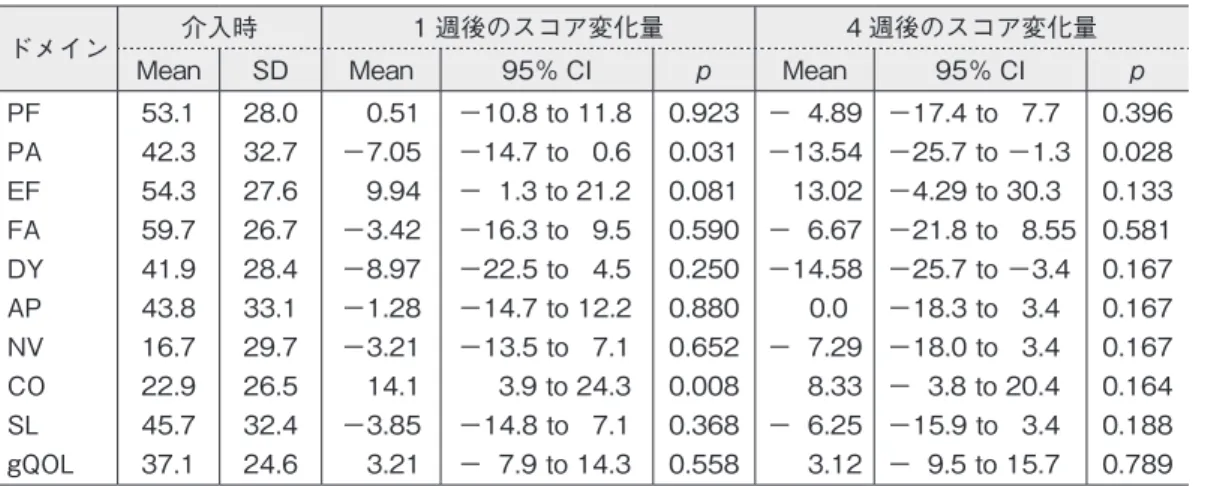
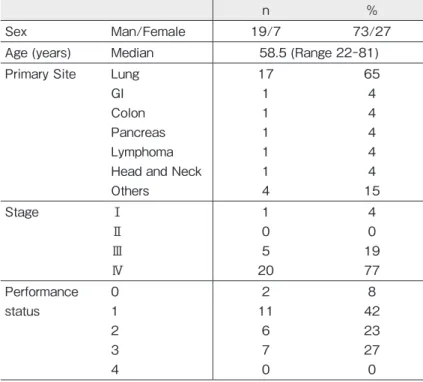
1 対象者 対象者の入院目的は, 2 例が疼痛コントロール目的で, 33 例 は化学療法や放射線療法のための抗がん治療目的であった. 対象者の介入依頼目的は, 疼痛が 14 件, 呼吸困難が 8 件, 倦 怠感・食欲低下が6 件, 悪心が 1 件, 不眠や不安など精神症状 が17 件であった. 35 人のうち, 1 週後追跡調査ができなかった 9 人を除く 26 人を本研究の検討対象とした. 追跡不可能であった理由は, 死 亡退院が1 人, 転院・自宅退院が 8 人であった. 脱落した 9 人 の背景要因は, 他の患者と有意差はなかった. 介入4 週後に, QOL 評価ができた人数は 16 人であった. 追 跡不可能であった理由は自宅退院・転院が9 人, 死亡が 1 人で あった. 未記入回答は, 同一人物による 4 週後の回答で item 2 およびitem 11 の 2 カ所のみであった. 緩和ケアチームの介入内容は, 1 週後で, 薬物調整 25 人, 精 神療法21 人, 放射線療法 2 人, 社会的支援 4 人, 家族ケア 4 人, スタッフ教育4 人であった. 4 週後では, 薬物調整 10 人, リン パマッサージ1 人, 精神療法 11 人, 放射線療法 2 人, 社会的支 援7 人, 家族ケア 4 人であった. 患者の背景を表 1 に示す. 2 症状マネジメント 介入時と介入後のスコアを表 2 に示す. global QOL は介入 後1 週間で 37.1 ± 24.6 から 3.21 上昇し, 4 週後には 3.12 上昇 したが, 有意な変化はなかった. 各ドメインのスコアの変化は, PA が 42.3 ± 32.7 から介入 1 週間で − 7.05 と, 有意に改善した (p=0.031). CO は有意に悪化した (p=0.008). 4 週後, PA, DY は 有意に改善した(p=0.028, 0.020). PA は, 介入 1 週後で 42.3% の患者で, 4 週後には 50%の患者で改善した. DY は, 4 週後に 62.5%の患者で改善がした. global QOL は, 介入後 1 週後には 30.7%の患者で, 4 週後には 37.5%の患者で改善した (表 3). 表 1 患者背景 n % 性別 男性/女性 19/7 73/27 年齢 中央値 58.5 (Range 22−81) 原発部位 肺 胃 大腸 膵臓 リンパ腫 頭頸部 その他 17 1 1 1 1 1 4 65 4 4 4 4 4 15 Stage Ⅰ Ⅱ Ⅲ Ⅳ 1 0 5 20 4 0 19 77 Performance status 0 1 2 3 4 2 11 6 7 0 8 42 23 27 0表 2 EORTC QLQ−C15−PAL 介入時, 1 週後, 4 週後のドメインスコア
ドメイン 介入時 1 週後のスコア変化量 4 週後のスコア変化量
Mean SD Mean 95% CI p Mean 95% CI p
PF PA EF FA DY AP NV CO SL gQOL 53.1 42.3 54.3 59.7 41.9 43.8 16.7 22.9 45.7 37.1 28.0 32.7 27.6 26.7 28.4 33.1 29.7 26.5 32.4 24.6 0.51 −7.05 9.94 −3.42 −8.97 −1.28 −3.21 14.1 −3.85 3.21 −10.8 to 11.8 −14.7 to 0.6 − 1.3 to 21.2 −16.3 to 9.5 −22.5 to 4.5 −14.7 to 12.2 −13.5 to 7.1 3.9 to 24.3 −14.8 to 7.1 − 7.9 to 14.3 0.923 0.031 0.081 0.590 0.250 0.880 0.652 0.008 0.368 0.558 − 4.89 −13.54 13.02 − 6.67 −14.58 0.0 − 7.29 8.33 − 6.25 3.12 −17.4 to 7.7 −25.7 to −1.3 −4.29 to 30.3 −21.8 to 8.55 −25.7 to −3.4 −18.3 to 3.4 −18.0 to 3.4 − 3.8 to 20.4 −15.9 to 3.4 − 9.5 to 15.7 0.396 0.028 0.133 0.581 0.167 0.167 0.167 0.164 0.188 0.789 PF: physical functioning, EF: emotional functioning, FA: fatigue, NV: nausea and vomiting, PA: pain, DY: dyspnea, SL: insomnia, AP: appetite loss, CO: constipation, gQOL: global quarity of life
考 察
本研究では, 緩和ケアチーム介入前後での QOL 評価を前向 きに行った. 緩和ケアチームの介入で PA, DY が 4 週後または 退院時に有意に改善した. 適切な薬物使用によって, 70〜90% で鎮痛を図ることが可能といわれており11), われわれの検討で も薬物療法や放射線療法が施された結果, 疼痛が軽減されたと 考える. また, 50%の患者で疼痛緩和が得られた本研究の結果 は, 先行研究とも一致する4〜12) . 1 週後に DY は有意な改善を認めなかったが, 4 週後の評価 では有意に改善した. 1 週後に DY が改善しなかった一因とし ては, 本研究では 65%が肺がん患者であり, 先行研究4)と患者 背景が相違していた点が挙げられる. PF, EF, CO に関しては, 悪化の傾向を示した. CO が悪化した 原因としては, オピオイドが影響していたと考えられる. EF が 改善しなかった原因としては, 観察期間の短さが考えられる. Temel らの報告5)では, the hospital Anxiety and Depression Scale (HAD−S) や, the Patient Health Questionnaire−9 (PHQ−9) を用いて,
気分の評価を行っているが, 緩和ケア介入群で 12 週後に有意 な改善がみられたとしている. 本研究では, 入院患者を対象と したため, 観察期間が 4 週間と短かったことが原因として考え られる. 一方, 改善した割合でみると, PF, EF ともに, 先行研究4) と類似した結果であった. global QOL に つ い て は, 有 意 な 改 善 が 得 ら れ な か っ た. Sasahara らの報告13) でも, 1 週後の評価では増悪しており, 本 研究と同様であった. 介入期間が 4 週と他の研究に比べて短期 間であったことやQOL 評価の手段が異なることが原因として
考えられる. EORTC QLQ C−15PAL では, global QOL と FA, EF, NV, CO, SL, AP が相関しているという報告もある8) . 本研究の 検討でもこれらの項目は有意な改善がみられず, QOL 改善に つながらなかったものと考えられる. Bakitas ら14)や Jakobsson ら15)は, 心理的側面, 気持のつらさが QOL に大きく影響する と述べており, EF の改善が得られなかったことが今回の結果 に影響している可能性がある. 本研究における問題点は, ①緩和ケアチームの非介入群を 設定しなかったこと, ② 1 施設での検討であること, ③緩和ケ 表 3 緩和ケアチーム介入による症状変化の割合 ドメイン 1 週後 (n=26) 4 週後 (n=16, PF/FA: n=15) 改善 変化なし 悪化 改善 変化なし 悪化 PF PA EF FA DY AP NV CO SL gQOL 10 (38.5) 11 (42.3) 12 (46.2) 10 (38.5) 11 (42.3) 6 (23.1) 5 (19.2) 2 ( 7.7) 9 (34.6) 8 (30.7) 7 (26.9) 11 (42.3) 5 (19.2) 7 (26.9) 11 (42.3) 13 (50.0) 16 (61.5) 13 (50.0) 12 (46.2) 9 (34.6) 9 (34.6) 4 (15.4) 9 (34.6) 9 (34.6) 4 (15.4) 11 (42.3) 5 (19.2) 11 (42.3) 5 (19.2) 9 (34.6) 6 (37.5) 8 (50.0) 4 (25) 7 (43.8) 10 (62.5) 6 (37.5) 4 (25.0) 2 (12.5) 4 (25.0) 6 (37.5) 3 (18.8) 6 (37.5) 4 (25) 3 (18.8) 4 (25.0) 3 (18.8) 10 (62.5) 8 (50.0) 11 (68.8) 5 (31.3) 6 (37.5) 2 (12.5) 2 (12.5) 5 (31.3) 2 (12.5) 7 (43.8) 2 (12.5) 6 (37.5) 1 ( 6.3) 5 (31.3) 表中の ( ) 内は%を示す.
PF: physical functioning, EF: emotional functioning, FA: fatigue, NV: nausea and vomiting, PA: pain, DY: dyspnea, SL: insomnia, AP: appetite loss, CO: constipation, gQOL: global quarity of life
緩和ケアチーム介入によるがん患者 QOL の変化 371 アチームが関与した患者がすべてのがん患者ではないこと, ④ 退院や転院などでデータの欠損があること, ⑤質問に回答する ごとに認知機能を評価しているわけではないこと, が挙げられ る. そのため, QOL の改善が真に有意であるかは評価できず, 今後の課題と考える. しかし, 別の観点からすると, 緩和ケア介 入効果はEORTC QLQ C−15PAL で十分に検出でき, 日常の緩和 医療での使用が勧められると考える.
結 語
われわれは, 日本人のがん患者を対象に緩和ケアチームの介 入の有効性を前向きに検討した. 今後, より長期間の QOL 評 価と, 症例数の増加により, 緩和ケアの介入による QOL の評 価がより正確に行われることが期待される. 謝辞 ご協力いただいた病棟の看護師の皆様および関係者 に心より感謝申し上げます. 文 献1) Sepúlveda C, Marlin A, Yoshida T, et al. Palliative Care: the World Health Organization’s global perspective. J Pain Symptom Manage 2002; 24: 91−6.
2) Rummans TA, Clark MM, Sloan JA, et al. Impacting quality of life for patients with advanced cancer with a structured multidisciplinary intervention: a randmized controlled trial. J Clin Oncol 2006; 24: 635−42.
3) Temel JS, JacksonVA, Billings JA, et al. Phase Ⅱ study: integrated palliative care in newly diagnosed advanced non−small−cell lung cancer patients. J Clin Oncol 2007; 25: 2377−82.
4) Follwell M, Burman D, Le LW, et al. Phase Ⅱ study of an outpa- tient palliative care intervention in patients with metastatic cancer. J Clin Oncol 2009; 27: 206−13.
5) Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non−small−cell lung cancer. N Engl J Med 2010; 363: 733−42.
6) Morita T, FujimotoK, Namba M, et al. Palliative care needs of cancer outpatients receiving chemotherapy: an audit of a clinical screening project. Support Care Cancer 2008; 16: 101−7.
7) Groenvold M, Petersen MA, Aaronson NK, et al. The develop-ment of the EORTC QLQ−C15−PAL: a shortened questionnaire for cancer patients in palliative care. Eur J Cancer 2006; 42: 55− 64.
8) Shin DW, Choi JE, Miyashita M, et al. Cross−cultural application of the Korean version of the european organization for research and treatment of Cancer Quality of Life Questionnaire−Core 15− Palliative Care. J Pain Symptom Manage 2011; 41: 478−84. 9) Miyazaki K, SuzukamoY, Shimozuma K, et al. Verification
of the psychometric properties of the Japanese version of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 15 palliative (EORTCQLQ− C15−PAL). Qual Life Res 2012; 21: 335−40.
10) Groenvold M, Petersen MA, the EORTC Quality of Life Group. Addendum to the EORTC QLQ−C30 Scoring Manual: Scoring of the EORTC QLQ−C15−PAL. European Organisation for Research and Treatment of Cancer, Brussels, 2006.
11) World Health Organization. Cancer Pain Relief, with a Guide to Opioid Availability,2nd ed. Geneva, 1996.
12) Strasser F, Sweeney C, Willey J, et al. Impact of a half−day multidisciplinary symptom control and palliative care outpatient clinic in a comprehensive cancer center on recommendations, symptom intensity, and patient satisfaction: a retrospective descriptive study. J Pain Symptom Manage 2004; 27: 481−91. 13) Sasahara T, Miyashita M, Umeda M, et al. Multiple evaluation
of a hospital−based palliative care consultation team in a university hospital: activities, patient outcome, and referring staff’s view. Palliat Support Care 2010; 8: 49−57.
14) Bakitas M, Lyons KD, Hegel MT, et al. Effects of a palliative care intervention on clinical outcomes in patients with advanced cancer: the Project ENABLE Ⅱ randomized controlled trial. JAMA 2009; 302: 741−9.
15) Jakobsson U, Hallberg IR, Westergren A. Exploring determi-nants for quality of life among older people in pain and in need of help for daily living. J Clin Nurs 2007; 16(3A): 95−104. 著者の申告すべき利益相反なし
Evaluation of QOL in cancer patients under
intervention by a palliative care team
Haruko Shinke
1), Akihiro Sakashita
1), Yuki Ishibashi
1), Kanako Otagaki
1),
Yuka Fujiwara
1), Takeshi Ioroi
1), Yuko Tamiya
1), Yoshikazu Kotani
2),
Toru Mukohara
3), Hironobu Minami
3)and Yoshihiro Nishimura
1, 2)Purpose: We assessed the efficacy of a palliative care team (PCT) in improving quality of life (QOL) among Japanese cancer patients. Patients and methods: This prospective study involved adult patients treated in the Division of Respiratory Medicine and Medical Oncology/Hematology at Kobe University Hospital between November 1, 2009 and March 30, 2010. Every patient had requested intervention by the PCT. Patients were asked to complete the EORTC QLQ−C15−PAL questionnaire at baseline and 1 and 4 weeks after initiation of the PCT intervention. Result: Of the 35 patients enrolled, 26 patients and 15 patients completed the assessments at 1 and 4 weeks after starting the intervention, respectively. Pain subscale (PA) was improved at 1 week after starting the intervention (p<0.05). Dyspnea subscale (DY) and PA were improved at 4 weeks after starting the intervention (p<0.05). Conclusion: We prospectively showed that QOL of cancer patients was improved with the intervention of the PCT, using the Japanese version of the EORTC QLQ−C15−PAL. Even if the PCT can only provide short−term care for cancer patients, this intervention appears worthwhile to improve QOL of cancer patients.
Palliat Care Res 2012; 7(2): 368−73
Key words: palliative care team, QOL, EORTC QLQ−C15−PAL
1) Palliative Care Team, Kobe University Hospital, 2) Division of Respiratory Medicine, ditto, 3) Division of Medical Oncology/Hematology, ditto
Short Communications
Table 1 Baseline characteristics of participants
n %
Sex Man/Female 19/7 73/27
Age (years) Median 58.5 (Range 22−81) Primary Site Lung
GI Colon Pancreas Lymphoma Head and Neck Others 17 1 1 1 1 1 4 65 4 4 4 4 4 15 Stage Ⅰ Ⅱ Ⅲ Ⅳ 1 0 5 20 4 0 19 77 Performance status 0 1 2 3 4 2 11 6 7 0 8 42 23 27 0
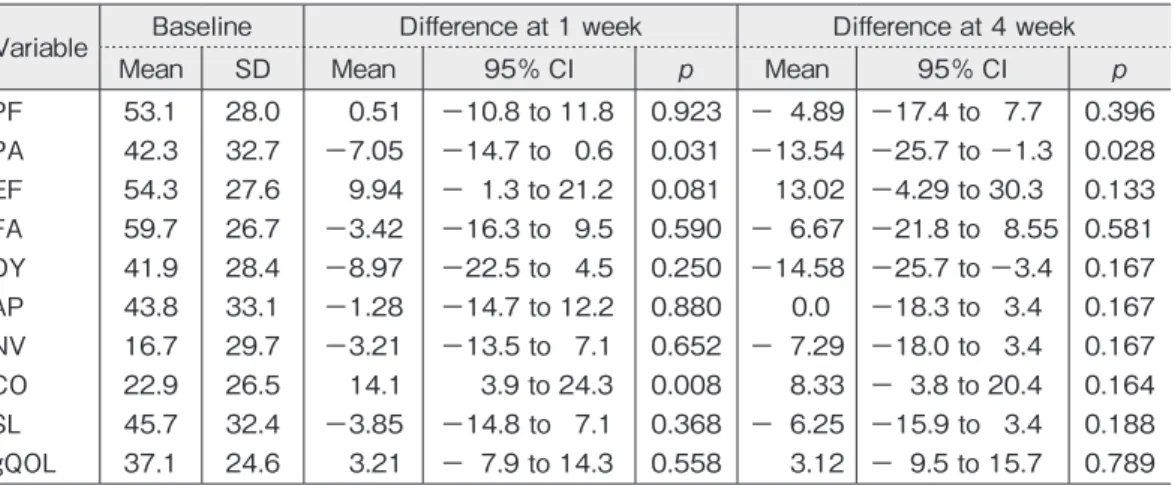
Evaluation of QOL in cancer patients under a palliative care team intervention 373 Table 2 EORTC QLQ-C15-PAL Domain Score at Baseline, at 1week, and at 4 week
Variable Baseline Difference at 1 week Difference at 4 week
Mean SD Mean 95% CI p Mean 95% CI p
PF PA EF FA DY AP NV CO SL gQOL 53.1 42.3 54.3 59.7 41.9 43.8 16.7 22.9 45.7 37.1 28.0 32.7 27.6 26.7 28.4 33.1 29.7 26.5 32.4 24.6 0.51 −7.05 9.94 −3.42 −8.97 −1.28 −3.21 14.1 −3.85 3.21 −10.8 to 11.8 −14.7 to 0.6 − 1.3 to 21.2 −16.3 to 9.5 −22.5 to 4.5 −14.7 to 12.2 −13.5 to 7.1 3.9 to 24.3 −14.8 to 7.1 − 7.9 to 14.3 0.923 0.031 0.081 0.590 0.250 0.880 0.652 0.008 0.368 0.558 − 4.89 −13.54 13.02 − 6.67 −14.58 0.0 − 7.29 8.33 − 6.25 3.12 −17.4 to 7.7 −25.7 to −1.3 −4.29 to 30.3 −21.8 to 8.55 −25.7 to −3.4 −18.3 to 3.4 −18.0 to 3.4 − 3.8 to 20.4 −15.9 to 3.4 − 9.5 to 15.7 0.396 0.028 0.133 0.581 0.167 0.167 0.167 0.164 0.188 0.789 PF: physical functioning, EF: emotional functioning, FA: fatigue, NV: nausea and vomiting, PA: pain, DY: dyspnea, SL: insomnia, AP: appetite loss, CO: constipation, gQOL: global quarity of life
Table 3 Proportions of Patients with changes in Symptoms by PCT intervention at 1 week and at 4 week
Variable 1 week (n=26) 4 week (n=16, PF/FA: n=15)
Improve Stable Deteriorate Improve Stable Deteriorate
PF PA EF FA DY AP NV CO SL gQOL 10 (38.5) 11 (42.3) 12 (46.2) 10 (38.5) 11 (42.3) 6 (23.1) 5 (19.2) 2 ( 7.7) 9 (34.6) 8 (30.7) 7 (26.9) 11 (42.3) 5 (19.2) 7 (26.9) 11 (42.3) 13 (50.0) 16 (61.5) 13 (50.0) 12 (46.2) 9 (34.6) 9 (34.6) 4 (15.4) 9 (34.6) 9 (34.6) 4 (15.4) 11 (42.3) 5 (19.2) 11 (42.3) 5 (19.2) 9 (34.6) 6 (37.5) 8 (50.0) 4 (25) 7 (43.8) 10 (62.5) 6 (37.5) 4 (25.0) 2 (12.5) 4 (25.0) 6 (37.5) 3 (18.8) 6 (37.5) 4 (25) 3 (18.8) 4 (25.0) 3 (18.8) 10 (62.5) 8 (50.0) 11 (68.8) 5 (31.3) 6 (37.5) 2 (12.5) 2 (12.5) 5 (31.3) 2 (12.5) 7 (43.8) 2 (12.5) 6 (37.5) 1 ( 6.3) 5 (31.3) The number in parentheses indicate %.
PF: physical functioning, EF: emotional functioning, FA: fatigue, NV: nausea and vomiting, PA: pain, DY: dyspnea, SL: insomnia, AP: appetite loss, CO: constipation, gQOL: global quarity of life