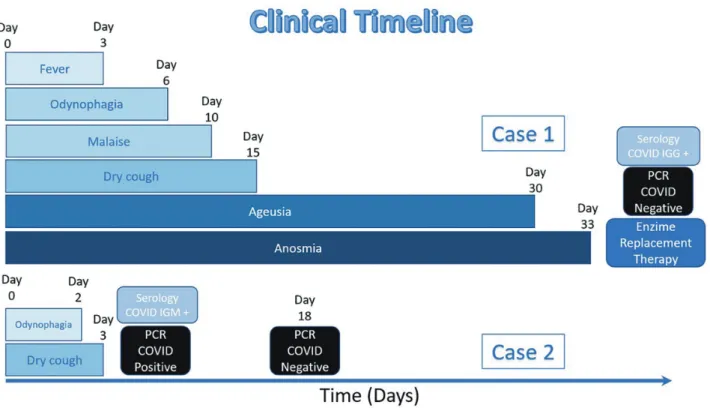
When Frequent (Pandemic) Occurs in a Non-Frequent Disease: COVID-19 and Fabry Disease: Report of Two Cases
5
0
0
全文
図
関連したドキュメント
High rates of long-term renal recovery in survivors of coronavirus disease 2019–associated acute kidney injury requiring kidney replacement therapy.. Figure 1Renal outcomes
This equation encompasses many important integral and functional equations that arise in nonlinear analysis and its applications, in particular integral equations (1.1), (1.2),
Atherosclerosis is a disease of the vasculature that is characterized by an accumulation of lipid-laden immune cells and apoptotic cells in the arterial wall.. Recently, the
7) CDC: Cleaning and Disinfection for Community Facilities (Interim Recommendations for U.S. Community Facilities with Suspected/Confirmed Coronavirus Disease 2019), 1 April, 2020
キーワード:感染症,ストレスマネジメント,健康教育,ソーシャルネットワーキングサービス YOMODA Kenji : Concerns and stress caused by the novel coronavirus disease
Protected Code Stroke: Hyperacute Stroke Management During the Coronavirus Disease 2019 (COVID-19) Pandemic. Temporary Emergency Guidance to US Stroke Centers During the
This thesis tries to examine the conflict between female desire and Victorian ideology in Bront ë’s novels through anal yses of colonial and foreign images.. It will show not onl
Remarks Begin applications prior to disease development and continue on a 7- to 14-day interval.. Use higher rate and shorter interval when disease pressure
