第 12 回 春季大会記録
研究講演:私の研究検査生体内微量物質の高感度検出法の開発と臨床応用
札幌医科大学医学部臨床検査医学講座渡 辺 直 樹
はじめに
こ れ ま で , radioimmunoassay(RIA) 法 や enzyme-linked immuno-sorbent assay(ELISA)法 を用いて,生体内微量物質の測定が行われてきた. しかし,これらの測定法には検出感度の面で一定 の限界があり,いまだ基準値の設定すら出来てい ない物質も少なくない.特にサイトカインに関し ては,ごく微量で強い生物活性を発揮するため, 高感度検出法の開発が急務となっている. そこで,これまで我々は,各種生体内微量物質 を対象とし,Immuno-PCR を用いた高感度検出 法の開発を試みてきた. 本稿では,Immuno-PCR 法の歴史,測定手技, 臨床応用の実際および今後の展望に関し,tumor necrosis factor α(TNF α)の成績を中心に概説す る.1.Immuno-PCR 法の歴史(表1)
1992年,Sano ら1)は,あらかじめプレートに固 相化した BSA 分子とモノクローナル抗体とを 反応後,streptavidin-protein A 複合体を介して 表1 Immuno-PCR 法の歴史 目的抗原 増感度(倍) 1995 Maia M, et al. HBsAg 1×1031995 Sanna PP, et al. Mouse TNF α 1×102
1995 Sperlet J, et al. sTCR 1×104
1995 Suzuki A, et al. sICAM-1 1×103
1995 Joerger RD, et al. hTSH 1×103
hCG 1×102
1995 Mweene AS, et al. BHV1 1×107
1997 Numata Y, et al. ANP 11)
1997 Niemeyer CM, et al. HBsAg 1×103
1999 Ogunjimi AA, et al. E. coli O157:H7 12)
2000 Ren J, et al. MG7Ag 1×104
2000 Saito K, et al. TNF α 5×104
2000 Furuya D, et al. IL-18 5×104
2000 Sugawara K, et al. Angiotensinogen 2.5×105
2001 Zhang H-T, et al. p185her2/neu receptor 1×109
2001 Wu HC, et al. BTx-A 1×103
2001 Furuya D, et al. Osteoprotegerin 2.5×104
1)感度の上昇はないが,測定時間を 3 日から 4.5 時間に短縮 2)感度の上昇はないが,測定時間を 8 時間に短縮
reportor DNA(pUC 19)を結合させ,PCR 法で増 幅することにより検出感度の上昇を試みた.その 結果,reportor DNA の代わりにアルカリフォス ファターゼを用いた ELISA 法に比べ,約 10 万倍 検出感度の上昇が可能なことを見い出した.また, Zhou ら2)は streptavidin -protein A 複合体の代わり に,streptavidin と biotin を介して reportor DNA と結合させる測定法を確立した.Proto-oncogene ETS 1 を標的分子として検討し,ELISA 法に比べ 約 10 万倍の感度を得た.しかし,彼らの系は, いずれも抗原をあらかじめ固相化した基礎的な解 析であった. 本法の検出感度の高さに着目し,biotin 標識 2 次抗体を用いたサンドイッチ法で,血中抗原の検 出を試みたのが Maia ら3)である.彼らは,血清
中の hepatitis B surface antigen(HBsAg)の測定系 を確立し,RIA 法に比べ約 1,000 倍検出感度が上 昇することを明らかにした. その後,あらかじめ chemical crosslinker を用 いて reportor DNA を 2 次抗体に結合させておく 系4)や,アガロースゲル電気泳動による PCR 増幅 産 物 の 検 出 の 代 わ り に southern blot 法3)5)や ELOSA 法3),PCR -ELISA 法6)を用いる系など, 種々の改良および比較検討が進められ,現在に至 っている.また,感度の上昇ではなく,測定時間 の短縮を目的とした報告7)もあり,Immuno -PCR 法の応用範囲も多岐にわたっている.
2.Immuno-PCR を用いた血清 TNF
αααα
の高感度検出法
8) 1)測定原理および手順(図1) 抗 TNF α モノクローナル抗体を固相化した後,DNA の非特異反応を防ぐために,salmon sperma DNA 添加のブロックエースを用いてブロッキン グした.試料を反応させた後,2次抗体として抗 TNF α ポリクローナル抗体でサンドイッチし,3 次抗体のみビオチン標識抗ウサギ IgG 抗体を用 いた.反応終了後,ビオチン化 DNA(reporter DNA)をアビジンを介して結合させた.Reporter DNA は pBluescript をテンプレートとしてビオチ ン化 M13-20プライマー,M13 reverse プライマ ーを用いて増幅後,残存するプライマーおよびプ ライマーダイマーを除去して作製した.Reporter DNA の検出は,その内側にプライマーを設定し, denature 94℃(15秒),annealing 58℃(15秒), extention 72℃(30秒)で 40cycle 増幅した.増幅産 物 は , Et-Br を 含 む 1% ア ガ ロ ー ス ゲ ル で 10V/cm・55 分間電気泳動後,イーグルアイ II を 用いて解析した. 2)TNF αααα 測定系確立のための基礎的検討 Immuno-PCR 法において,良好な検出感度を 得るための重要なポイントは,いかにして至適な streptavidin および reporter DNA 濃度を決定する かである.
(1)至適 streptavidin 濃度の設定
Immuno-PCR 法を行うに際し,まずstreptavidin
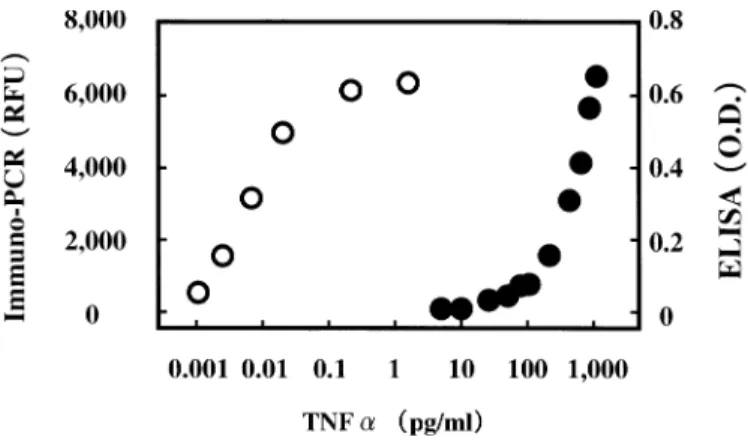
図2 Immuno-PCR 法(○)と ELISA 法(●)による TNF α 検出感度の比較 の至適濃度について検討した.すなわち,無標識
streptavidin の 代 わ り に HRP labeled strept-avidin(1,0.1,0.01µg/ml)を反応させ,OPD に より発色させた.その結果,1µg/ml ではブラン クの O.D.が 0.8 と非特異反応がみられ,さらに高 濃度域でプラトーとなった.また,0.01µg/ml で は感度に問題があったため,0.1µg/ml が至適濃 度と考えられた . (2)至適 reporter DNA 濃度の設定 Reporter DNA 濃度が非特異反応に及ぼす影響 を検討するため,TNF α を含まない 0.1%ゼラチ ン-PBS を 抗 原 と し て 使 用 し , 段 階 希 釈 し た reporter DNA(0.05∼5,000pg/ml)を反応させた. 反応終了後,増幅産物をアガロースゲルで電気泳 動したところ,加えた reporter DNA 濃度が低く なるにつれてバンドも薄くなり,0.5pg/ml では 認められなかった.すなわち,0.5pg/ml が至適 reporter DNA 濃度であると考えられた. 3)ELISA 法との感度の比較 Immuno-PCR 法と ELISA 法との検出感度の比 較を行ったところ,比較対照法に用いた ELISA 法の測 定下 限が 50pg/ml であ った のに 対し , Immuno-PCR 法では 0.001pg/ml までバンドが検 出され,約 5 万倍の感度上昇が確認された(図2). さらに,健常者の血清 TNF α 濃度も Immuno -PCR 法を用いることによりはじめて測定可能と なり,その基準範囲は 0.027±0.054pg/ml であっ た(図3).
図 3 健 常 者 と Duchenne muscular dystrophy (DMD) 患 者 に お け る 血 清 TNF α 濃 度 (Shaded area は ELISA 法での検出可能範囲 を示している)
3.臨床応用の実際
1)Duchenne muscular dystrophy(DMD) 患 者における検討 DMD は X 染色体劣性遺伝をとる疾患で,筋細 胞膜に局在するジストロフィン蛋白が欠損するた め,筋細胞膜が脆弱となり壊死に陥る. 従来,多くの患者は 10 歳前後で歩行不能となり, 呼吸筋や心筋が侵されるため,20%は心不全で死 亡していた.しかし,最近では人工呼吸器の使用 が普及し,患者の生命予後はやや改善している.
表2 Inflammatory bowel disease(IBD)患者における平均血清 TNF α 濃度 No. of samples TNF α(pg/ml) 潰瘍性大腸炎(UC) total 46 30.276 inactive 20 6.495 active 26 48.570 クローン病(CD) total 8 208.354 inactive 4 11.967 active 4 404.760 そこで,DMD 患者 65 例について血清 TNF α 濃 度 を 測 定 し た と こ ろ , そ の 平 均 濃 度 は 27.8pg/ml と,健常者に比べ約 1,000 倍高値を示 した(図3)12).さらに,筋組織の崩壊が完成する 20 歳未満の群における平均血清 TNF α 濃度が, 20 歳以上に比べ約 5 倍高値であったことから, TNF α の病態形成への密接な関与が示唆された. しかし,血清 TNF α 濃度と CK および Mb 濃度 との間には必ずしも相関関係はみられず,DMD における血清 TNF α 濃度の上昇は,単に筋崩壊 の結果とは考えられなかった.
2)Inflammator y bowel disease(IBD)患者に おける検討
潰瘍性大腸炎(Ulcerative Colitis : UC)とクロー ン病(Crohn's disease : CD)に代表される炎症性 腸疾患(IBD)は,血便,下痢便や腹痛を主訴とす る難治性の疾患である. その発症や病態の進展に,サイトカインをはじ めとする各種免疫異常の関与が示唆されているが, いまだ不明な点が少なくない.そこで,UC 患者 28 例および CD 患者 8 例の血清 TNF α 濃度につ いて調べた.その結果,平均血清 TNF α 濃度は, それぞれ 30.3pg/ml,208.4pg/ml と,健常者に比 べ UC で約 1,100 倍,CD で約 7,700 倍高値であ った(表2)13).しかし,36 例中 ELISA 法で測定可 能であったものは 4 例(11.1%)にすぎなかった. また,血清 TNF α 濃度は,活動期に比べ非活動 期では明らかに低下し,その推移は病態を良く反 映していた.
4.Immuno
-PCR
法が抱える問題点
1)プロゾーン現象 Immuno-PCR 法は高感度である反面,測定レ ンジが若干狭いという問題点を有している.我々 の TNF α の 測 定 系 で も , 最 小 検 出 感 度 が 0.001pg/ml で あ る の に 対 し , 抗 原 濃 度 が 0.1pg/ml を越えるとプロゾーン現象を起こす. このため,ELISA 法の併用や,検体の希釈系列を 同時測定することが必要である. 2)測定手技の煩雑さ Immuno-PCR 法は反応ステップが多く,最終 的に PCR 反応で増幅するため,洗浄操作におけ る小さなミスが結果として大きな測定値のバラツ キ と な る . そ の た め , 熟 練 を 要 す る . 今 後 , Immuno-PCR 法が研究レベルから一般的な測定 法となるためには,自動分析装置の開発が必要と 思われる.おわりに
Immuno-PCR 法の歴史,測定手技,臨床応用 の実際および今後の展望に関し,我々の成績も含 めて概説した. Immuno-PCR 法は基本的に標準物質と抗体が あれば,どのような物質に対しても応用可能であ る.我々も,TNF α 以外に angiotensinogen15),Interleukin-18(IL-18)14)や Osteoprotegerin16)につ いて,既に測定系を確立している.なかでも, angiotensinogen は同一のポリクローナル抗体で 抗原をサンドイッチする系であり,必ずしも異種 動物由来の 2 種の抗体とそれを利用した 3 次抗体
の存在が,必須ではないことを示唆している. 今後,本法を用いて各種生体内微量物質の高感 度検出系が開発され,新たな知見が得られること を期待したい.
文 献
1) Sano T, Smith CL and Cantor CR: Immuno-PCR: very sensitive antigen detection by means of specific antibody-DNA conjugates. Science, 258, 120-122(1992)
2) Zhou H, Fisher RJ and Papas TS: Universal immuno-PCR for ultra-sensitive target protein detection. Nucleic Acids Res., 21, 6038-6039 (1993)
3) Maia M, Takahashi H, Adler K, et al.: Development of a two-site immuno-PCR assay for hepatitis B surface antigen. J. Virol. Methods, 52, 273-286(1995)
4) Joerger RD, Truby TM, Hendrickson ER, et al.: Analyte detection with DNA-labeled antibodies and polymerase chain reaction. Clin. Chem., 41, 1371-1377(1995)
5) Suzuki A, Itoh F, Hinoda Y, et al.: Double determinant immuno-polymerase chain reaction: a sensitive method for detecting circulating antigens in human sera. Jpn J. Cancer Res., 86, 885-889(1995)
6) Niemeyer CM, Adler M and Blohm D: Fluorometric polymerase chain reaction(PCR) enzyme-linked immuno assay for quantification of immuno-PCR products in microplates. Anal. Biochem., 246, 140-145(1997)
7) Numata Y and Matsumoto Y: Rapid detection of alpha-human atrial natriuretic peptide in plasma by a sensitive immuno-PCR sandwich assay. Clin. Chim. Acta, 259, 169-176(1997)
8) Sanna PP, Weiss F, Samson ME, et al.: Rapid induction of tumor necrosis factor alpha in the
cerebrospinal fluid after intracerebroventricular injection of lipopolysaccharide revealed by a sensitive capture immuno-PCR assay. Proc. Natl. Acad. Sci. USA, 92, 272-275(1995)
9) Sperl J, Paliwal V, Ramabhadran R, et al: Soluble T cell receptors: detection and quantitative assay in fluid phase via ELISA or immuno-PCR. J. Immunol. Methods, 186, 181-194(1995) 10) Mweene AS, Ito T, Okazaki K, et al.: Development
of immuno-PCR for diagnosis of bovine herpesvirus 1 infection. J. Clin. Microbiol., 34, 748-750(1996)
11) Saito K, Kobayashi D, Sasaki M, et al.: Detection of human serum tumor necrosis factor-alpha in healthy donors using a highly sensitive immuno-PCR assay. Clin. Chem., 45, 665-669(1999) 12) Saito K, Kabayashi D, Komatsu M, et al.: A
sensitive assay of tumor necrosis factor α in sera from duchenne muscular dystrophy patients. Clin. Chem., 46, 1703-1704(2000)
13) Komatsu M, Kobayashi D, Saito K, et al.: Tumor necrosis factor-α in serum of patients with inflammatory bowel disease as measured by a highly sensitive immuno-PCR. Clin. Chem., 47, 1297-1301(2001)
14) Furuya D, Yagihashi A, Yajima T, et al.: An immuno-polymerase chain reaction assay for human interleukin-18. J. Immunol. Methods, 238, 173-180(2000)
15) Sugawara K, Kobayashi D, Saito K, et al.: A highly sensitive immuno-polymerase chain reaction assay for human angiotensinogen using the identical first and second polyclonal antibodies. Clin. Chim. Acta, 299, 45-54(2000)
16) Furuya D, Kaneko R, Yagihashi A, et al.: Immuno-PCR assay for homodimetric osteo-protegerin. Clin. Chem., 47, 1475-1477(2001)