Table 1 Laboratory findings(1)
<ESR>
<Serum Chemistry>
< Urinalysis>
mm/hr 82 g/dL
7.5 TP
(+)
Protein
<Serology> g/dL
3.5 Alb
(-)
Glucose
mg/dL 10.0 CRP
mg/dL 0.4 T-Bil
(±)
Occult blood
(-)
STS U/L
83 AST
< Blood count>
(-)
TPHA U/L
160 ALT /μL
9020 WBC
(-)
HBs Ag U/L
189 LDH
% 70 N
(-)
HCV Ab U/L
480 ALP
% 15 L
mg/dL 1571 IgG
U/L 124 γGTP
% 11 M
mg/dL 367 IgA
mg/dL 8.8 BUN
% 1 E
mg/dL 68 IgM
mg/dL 0.6 Cr
% 2 B
U
< 30 ASLO
mEq/dL 133 Na /μL
449×104 RBC
<Tuberculin skin test> mEq/dL
4.4 K
g/dL 13.7 Hb
mEq/dL 99 Cl
% 4.6 Ht
mg/dL 8.6 Ca /μL
61.1×104 Plt
mg/dL 101 Glu
15×150×0(+)
結核性胸膜炎の経過中にアナフィラクトイド紫斑病を併発した 1 例
新小倉病院内科
久保井 礼 野 村 秀 幸
(平成 17 年 10 月 24 日受付)
(平成 17 年 11 月 21 日受理)
Key words : anaphylactoid purpura, tuberculous pleuritis, anti-tuberculous treatment
序 文
結核の治療中に発熱や皮膚病変など種々の合併症が みられることは稀ではない
1)2).アナフィラクトイド紫 斑病は Henoch-Sch nlein 紫斑病などとも呼ばれ,溶 血性連鎖球菌感染症との関連が深いとされているが,
結核治療中の発症は稀である
3).今回,結核性胸膜炎 の治療中にアナフィラクトイド紫斑病を合併した症例 を経験したので報告する.
症 例
症例:46 歳 男性.
主訴:発熱,胸痛.
既往歴:39 歳 虫垂炎手術.
生活歴:焼酎水割 2 杯! 日,10 年前より禁煙(以前 は喫煙 40 本! 日).
家族歴:特記事項なし.
現 病 歴:2004 年 5 月 9 日 よ り 38℃ 台 の 発 熱 が 持
続,近医にて抗生物質の投与を受けていた.5 月 14 日頃より右胸痛が出現,右胸水を指摘され,他院に入 院した.胸水検査が施行され,各種の抗菌薬が使用さ れたが,発熱と胸痛が続き,5 月 24 日 新小倉病院 を紹介され転院となった.
入 院 時 現 症:身 長 165.2cm,体 重 67.2kg,体 温 37.6℃,血圧 144! 90mmHg,心拍 94! 分,整,呼吸数 16! 分.眼瞼結膜に貧血なし,眼球結膜に黄疸なし.
胸部:心音に異常はない.右下肺野に呼吸音の減弱を 認める.腹部:右季肋部に軽度圧痛あり,腫瘤は触知 しない.
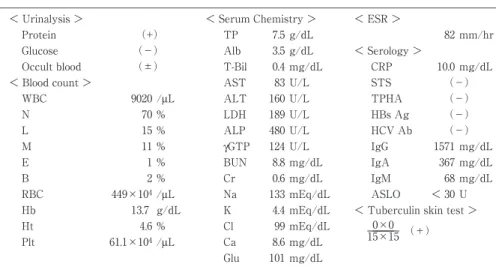
入院時検査所見(Table 1):尿蛋白陽性,軽度の白 血球増加,血小板増加,著明な血沈の促進,CRP の 上昇,肝機能異常を認め,ツベルクリン反応は陽性で あった.
胸部 X 線検査(Fig. 1):大量の右胸水が認められ,
症 例
別刷請求先:(〒803―8505)北九州市小倉北区金田1―3―1
新小倉病院内科 久保井 礼
Fig. 1 Chest X-ray on admission showing a massive right pleuraleffusion.
Fig. 2 Computed tomography scans ofthe chest after thoracocentesis showing a right pleu- raleffusion,pleuralthickening,and high-density shadows in both lungs.
入院の翌日に胸腔穿刺および胸膜生検を施行した.
胸水検査(Table 2):胸水の色調は黄色混濁を呈 し,その性状は滲出液で,胸水のアデノシンデアミナー ゼ(ADA)は 61.7U! Lと上昇,培養では一般細菌,
抗酸菌とも陰性であった.
胸部 CT(Fig. 2):胸腔穿刺・胸水排液後の胸部 CT では,右胸水貯留,胸膜肥厚,肺野に索状および斑状 の濃度上昇を認めた.
胸膜生検病理組織所見(Fig. 3):組織球の集簇,
リンパ球浸潤,線維素性滲出物を伴う肉芽組織で,類
上皮細胞や乾酪壊死はなく,悪性の所見も認められな かった.
当院での胸水の抗酸菌塗抹・培養は陰性で,胸膜生 検でも特異的な所見は認められなかったが,前医での 胸水検査において結核菌 PCR が陽性であったこと,
ツベルクリン反応が陽性であったことなどから,結核 性 胸 膜 炎 と 診 断 し,5 月 26 日 よ り 抗 結 核 薬 4 剤
(RFP,INH,EB,PZA)を開始した.翌日より発 熱はみられなくなり,胸痛も軽減した(Fig. 4).
5 月 30 日頃から両下肢に径 3mm前後の赤紫色の小
Fig. 3 Histological appearance of the pleural biopsy specimen showing a the granulation tissue with aggre- gates of histiocytes, a lymphocytic infiltrate, and fibri- nous exudate.
Fig. 4 Clinicalcourse Table 2 Laboratory findings(2)
< Pleuraleffusion>
Appearance:Yellow and turbid 1.040 S.G.
mg/dL 102 Glucose
g/dL 5.4 Protein
(+)
Rivalta
U/L 501 LDH
U/L 61.7 ADA
/mL(L 99%,N1%)
930 WBC
Mycobacteria:Smear(-),Culture(-)
M.tuberculosisPCR(-)
Cytology:class I I
発疹が出現(Fig. 5),皮膚科にてアナフィラクトイ ド紫斑病を疑われ,皮膚生検が行われた.
皮膚生検病理組織所見(Fig. 6):真皮上層に白血 球の集簇を伴う血管炎を認め,アナフィラクトイド紫 斑病に矛盾しない所見であった.
皮膚病変に対してステロイド外用薬による治療が開 始され,一時皮疹の拡大がみられたが,その後は次第 に改善した.抗結核薬による副作用は特にみられず,
6 月 26 日に退院,当院外来で抗結核薬による治療を 継続した.胸部 X 線では,右胸膜の肥厚,右肺下葉 に索状影を認めるが,胸水は減少,消失した.CRP,
血沈や肝機能も改善した.尿蛋白や尿潜血反応が陽性 の時期もあったが,最終的には正常化した(Fig. 4).
2005 年 3 月中旬から抗結核薬を中止したが,胸膜炎 やアナフィラクトイド紫斑病の再発はみられていな い.
考 察
本症例にみられたアナフィラクトイド紫斑病は糸球 体メサンギウムと皮膚の小血管壁への IgA 沈着が特 徴とされる
4)5).血管病変の主体は,真皮上層の細小血 管の壊死性血管炎(leukocytoclastic vasculitis)で,
その発症機序は明らかではないが,IgA 免疫複合体が
Fig. 5 Skin eruption on the right foot.
Fig. 6 Histologicalappearance ofthe skinbiopsy speci- men showing leukocytoclastic vasculitis in the upper dermis.
血管壁に沈着,これを白血球内に取り込むことによる 血管内皮障害の可能性が想定されている
6)7).抗原抗体 反応の原因として感染症,膠原病,悪性腫瘍などがあ げられている
6).三大主徴は,皮膚症状・腹部症状・
関節症状で,大部分は小児にみられ,特に男児に多い とされているが,成人にもみられることがある.皮膚 病変は下肢に好発し,随伴症状には関節痛,発熱,浮 腫,腹痛,血尿(肉眼的,顕微鏡的)などがあげられ る
8).本症例では両下肢の紫斑以外の症状は特に認め られなかった.30〜80% の症例において連鎖球菌,
アデノウイルス,パルボウイルス,EB ウイルス,水 痘ウイルス,マイコプラズマ等による呼吸器感染症が 先行しており
4)9)10),特に溶血性連鎖球菌感染症との関 連が指摘されているが,結核は稀とされている.本症 例では Anti-streptolysine O(ASLO)の上昇などは なく,溶連菌との関連は指摘できなかった.多くの症 例では血清 IgA の上昇を認めるが
11),本症例では明ら かではなかった.
抗結核薬がアナフィラクトイド紫斑病の発症に関係 していると考えられる症例も報告されている
12).本症
例では,抗結核薬を開始した後に紫斑が出現している が,抗結核薬を減量・中止することなく紫斑が消失し ており,薬剤との関連は考えにくいと思われる.抗結 核療法開始後に,結核菌の菌体成分が何らかの免疫学 的機序で紫斑病の原因となる血管病変を発生させた可 能性が考えられる.
結核に合併したアナフィラクトイド紫斑病は稀とさ れているが,本症例は,結核菌感染とアナフィラクト イド紫斑病の発症との関連を示唆する興味深い症例と 考えられた.
文 献
1)Duncan WC, Rudolph AH:Tuberculosis and at- ypical mycobacterial disorders. In : Cutaneous aspects of internal disease. Year Book Medical Publishers, Inc, Chicago. 1981;p. 343―52.
2)Kennedy C, Knowles GK:Miliary tuberculosis presenting with skin lesions. Br Med J 1975;
3:356.
3)Washio M, Nanishi F, Onoyama K, Fujii K, Oh- chi N, Fujishima M:Recurrence of Henoch Sc- hoenlein purpura nephritis associated with tu- berculous pleuritis. Japanese J Nephrology 1988;30:1087―9.
4)Counahan R, Cameron JS:Henoch Schoenlein nephritis. Contr Nephrol 1977;7:145―65.
5)Andre C, Berthoux FC, Gillon J, Genin C, Sa- batier JC:Prevalence of IgA2 deposits in IgA nephropathies : A clue to their pathogenesis.
New Engl J Med 1980;303:1343―6.
6)Sloane PD, Tardell R:Palpable purpura in leu- kocytoclastic vasculitis. Am Fam Physician 1986;33:197―200.
7)Ekenstam E, Callen JP:Cutaneous leukocytocl- astic vasculitis. Clinical and laboratory features of 82 patients seen in private practice. Arch Dermatol 1984;120:484―9.
8)三 島康 男,竹 内 誠,神 坂 謙,岡 田千 春,多 田敦彦,河原 伸,他:肺結核治療経過中に He- noch-Sch nlein 紫 斑 病 を 合 併 し た 1 例.結 核 1994;69:21―5.
9)Tizard EJ:Henoch-Schoenlein purpura. Arch Dis Child 1999;80:380―3.
10)Islek I, Muslu A, Totan M, Gok F, Sanic A:He- noch-Schonlein purpura and pulmonary tubercu- losis. Pediatr Int 2002;44:545―6.
11)Trygstad CW, Stiehm ER:Elevated serum IgA globulin in anaphylactoid purpura. Pediatrics 1971;47:1023―8.
12)Chan CHS, Chong YW, Sun AJM, Hoheisel GB:Cutaneous vasculitis associated with tuber- culosis and its treatment. Tubercle 1990;71:
297―300.
A Case of Anaphylactoid Purpura Associated with Tuberculous Pleuritis Satoshi KUBOI & Hideyuki NOMURA
Department of Internal Medicine, Shin-Kokura Hospital