Comparison of the use of tablets containing a cysteine protease actinidin and tongue brushes for reduction of the bacterial load on the tongue
Naho Mugita
1, Kazuya Takahashi
2and Yutaka Komasa
21Graduate School of Dentistry (Geriatric Dentistry) and2Department of Geriatric Dentistry, Osaka Dental University, 8-1 Kuzuhahanazono-cho, Hirakata-shi, Osaka 573-1121, Japan
Tongue coating as an oral biofilm is responsible for 60% of all halitosis cases. It also in
terferes with gustatory perception, and is associated with periodontal disease and pneu
monia. As it is difficult to remove, the development of new cleaning methods is being promoted. We studied tablets containing actinidin, a cysteine protease, which has been reported to effectively remove this coating on the tongue. As tablets placed in the oral cavity are usually abraded by the tongue and palate to promote their dissolution, their ef
fect in the elderly is likely to be reduced because of decreased motor function of the tongue. However, there is no literature discussing this effect in the elderly or comparing tablets with tongue brushes. To evaluate the efficacy of tablets containing actinidin on reducing the bacterial load on the tongue, we compared the effect of tablets, tongue brushes, and a combination of both on reduction of the bacterial load on the tongue.
Tongue cleaning was performed for elderly individuals requiring assistance or care (the elderly group) and healthy young adults (the young group) using three methods : two tablets containing actinidin (the tablet method), brushing with a tongue brush (the brush
ing method), and the combined use of both (the combined method). The bacterial load on the tongue dorsum was measured before treatment, immediately after treatment, and at 1 and 2 hours after treatment. With the brushing method, neither the elderly nor young groups showed significant changes in the bacterial load until 2 hours after treatment. In contrast, a marked decrease in the bacterial load was observed in both groups immedi
ately after treatment using the tablets, and immediately after and at 2 hours after treat
ment using the combined method. The tablets were particularly effective for the young group, and decreases in the bacterial load were observed immediately and at 1 hour after treatment when they were administered alone or in combination with the tongue brush.
Furthermore, in the young group, the bacterial load immediately after and at 1 hour after treatment varied between the tablet and brushing methods.
In contrast, in the elderly group, although the bacterial load was significantly reduced with the tablet method, this decrease was not observed when treatment was combined with the tongue brush. In both groups, the decrease in the bacterial load was more marked even at 2 hours after treatment when the combined use was compared with the brushing method alone. These results demonstrated that tablets containing cysteine pro
tease are more effective than tongue brushes for reduction of the bacterial load, and that the effect lasts longer when the two methods are combined. (J Osaka Dent Univ 2016 ; 50 : 93101)
Key words : Actinidin ; Cysteine protease ; Tablet ; Bacterial load ; Tongue
INTRODUCTION
Volatile sulfides are considered responsible for physiologic halitosis,
1and 60% of the cases are caused by the putrefying activity of bacteria in the tongue coating. The tongue coating is the main cause of physiologic halitosis.
2Comprising a large number of papillae, the dorsal surface of the tongue is rough. The tongue surface, with its numerous pits, is an ideal niche for bacterial attachment and proliferation, reducing the effect of cleaning and consequently allowing the development of an ex
tensive oral biofilm.
3In the elderly, the tongue coat
ing tends to be particularly thick and difficult to re
move. Increased tongue coating levels may influ
ence gustatory perception. Winkler noted an en
hanced gustatory perception in elderly patients (particularly those using dentures) after removal of the thick plaque layer on their tongue.
4In addition, as a correlation has also been reported between bacteria in the tongue coating and the frequency of fever in the elderly,
5not only young individuals who are concerned about halitosis, but also elderly who have decreased tongue function require the re
moval of the tongue coating.
Currently, mechanical cleaning methods, such as using toothbrushes or tongue brushes, which are generally used to remove the tongue coating, are somewhat effective.
6, 7On the other hand, problems such as excessively abrasion of the mucous mem
brane of the tongue and triggering on the gag re
flex, have been noted. Quirynen et al. conducted a questionnaire survey after tongue scraping, and re
ported that some respondents had experienced vomiting.
8Considering these points, we focused on methods to chemically remove the tongue coating.
Oral mucosaderived detached epithelial cells and bacteria account for the majority of tongue coating components.
3, 9, 10Proteases are effective at removing such coating.
11, 12For example, Yoshi
matsu et al. confirmed the effectiveness of tablets containing the kiwifruitderived cysteine protease actinidin for removing the tongue coating and re
ducing halitosis.
11However, there is no literature comparing the tonguecleaning effect of such tab
lets with conventional mechanical cleaning meth
ods.
Furthermore, the elderly, defined as those requir
ing care based on the Longterm Care Insurance System in Japan, tend to face agerelated reduc
tions in motor function of the tongue as well as la
ryngeal and hyoid elevation, leading to difficulty in bringing the tongue dorsum into contact with the palate.
13, 14As tablets are moved between the ton
gue and palate in the oral cavity, sufficient effect may not be obtained when they are used by indi
viduals requiring care, who are likely to have de
creased tongue muscle strength. We studied the ef
fect of tablets and tongue brushes for cleaning the tongue dorsum of elderly individuals requiring as
sistance or care, and healthy young adults.
MATERIALS AND METHODS Subjects
We studied 10 elderly individuals requiring assis
tance or care (the elderly group : 2 males and 8 fe
males with a mean age of 83±5 years) and 10 healthy young adults (the young group : 7 males and 3 females aged 28±2 years) using the follow
ing exclusion criteria : the absence of tongue coat
ing ; their difficulty in performing oral care inde
pendently ; their inability to provide responses ; a reduced cognitive level ; and an increased risk of improperly ingesting the tablets. The cognitive level was evaluated using a Japanese scale to assess the degree of independence in daily activities for the elderly with dementia. Subjects were included who had cognitive levels corresponding to the cate
gories from “independent” (without dementia) to
“IIb” (mild level of dementia).
Study design
A 3group, 3treatment crossover (orthogonal Latin square) study was conducted, with a 1week wash
out period (Table 1). To examine the effects of
daily tongue cleaning, all subjects were instructed
to perform tongue and oral cleaning independently,
as they usually did, until noon on the measurement
day. Considering the stability of oral bacteria, the
first baseline measurement (T
0) of the bacterial load
on the tongue dorsum was performed more than 30 minutes after lunch. Subsequently, tongue cleaning was performed for the subjects using three meth
ods : use of two tablets (BREO EX
Ⓡ; Ezaki Glico, Osaka, Japan) containing the cysteine protease ac
tinidin (the tablet method), brushing the tongue with a tongue brush (Mini Moa Brush
Ⓡ; Oral Care, To
kyo, Japan) (the brushing method) ; and a combi
nation of the two (the combined method).
When using the tablet method, the subjects were given one tablet and instructed to suck, rather than chew it, moving the dorsal surface of their tongues until it dissolved naturally. The second tablet was administered in the same manner. The second (T
1) measurement was performed immediately after confirming that the second tablet had completely dissolved. When using the brushing method, the area for tongue dorsum cleaning was vertically di
vided into three sections in accordance with the size of the brush. The brush was moved back and forth along the long axis of the tongue in the cen
tral, right and left sections, in that order. The exam
iner repeated this procedure, abrading the tongue while applying a force of 50 to 60 g, 10 times. After treatment, the subjects gargled twice, and, subse
quently, the second (T
1) measurement was per
formed.
When the two methods were combined, the cleaning was done using the tongue brush after ad
ministration of the two tablets, followed by subse
quent measurements.
In short, when using the tablet or brushing me
thod, the bacterial load was measured four times : before treatment (T
0), immediately after treatment (T
1), and at 1 (T
1h) and 2 (T
2h) hours after treatment.
When using the combined method, it was meas
ured 5 times : before treatment (T
0), after tablet ad
ministration (T
1’) and after use of the tongue brush
(T
1), and at 1 (T
1h) and 2 (T
2h) hours after treatment.
The study was conducted with the approval of the director of the study facility and Osaka Dental Uni
versity Medical Ethics Committee (Approval num
ber : 110797).
Measurements
The bacterial load was measured using a simple oral bacterial load meter (Bacterial Counter
TM, Panasonic Healthcare, Tokyo, Japan). Sterile cot
ton swabs, attached to the Bacterial Counter, were reciprocated 5 times to abrade the tongue surface for collection of specimens from the point of inter
section of the line between both first molars and the midline of the tongue to approximately 1 cm for
ward, while applying a force of 20 g. This proce
dure was only done by two researchers to avoid procedural errors. The cotton swabs were soaked in 5 mL of sterile distilled water attached to the Bacterial Counter before bacterial detection.
Statistical analysis
The logarithm of the bacterial load for each treat
ment method, measurement time, and age, were determined. The distribution was normal in all cases using the ShapiroWilk test. An analysis of variance was performed, adopting a splitplot three
factorial design, in which repeated measures analy
sis of variance was performed based on the treat
ment method and measurement time, and an un
paired test was conducted based on age. As signifi
cant interactions were observed, twoway repeated measures analysis of variance was performed for all factors. Among these, only those showing sig
nificant differences were examined through multiple comparisons using Bonferroni’s method. The signifi
cance level was set at a reject rate of 5% (<5%).
We used IBM
ⓇSPSS
ⓇStatistics version 22, (IBM
Ⓡ,
Table 1 Treatment protocol (Williams’ Latin square 3×3)
Group Treatment
1 : 3 young and 3 elderly adults Tablet Tongue brush Tablet and tongue brush 2 : 4 young and 3 elderly adults Tongue brush Tablet and tongue brush Tablet
3 : 3 young and 4 elderly adults Tablet and tongue brush Tablet Tongue brush
Armonk, NY, USA) as statistical analysis software.
RESULTS
Bacterial load before treatment and carry-over effects
There were no significant differences at T
0in the bacterial load among the three treatment methods in the elderly or young groups (data not shown), confirming that there were no carryover effects in this crossover study (Fig. 1).
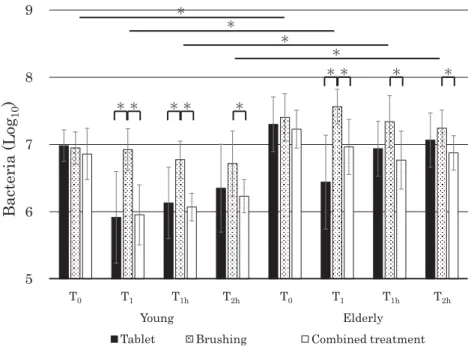
Comparison based on the measurement time among the treatment methods and age groups Regardless of the age, the bacterial load was mark
edly lower when using the combined method com
pared with the brushing method at T
1, T
1h, and T
2h(Fig. 1). In contrast, when using the tablets com
pared with the brushing method, the values were significantly lower at T
1in both age groups, and at T
1hin the young group. Furthermore, there were significant differences between the age groups, re
gardless of the treatment method or measurement time.
Comparison based on the measurement time For the young group (Fig. 2), compared with the values at T
0, the bacterial load was markedly lower at T
1and T
1hwith tablets, and at T
1, T
1hand T
2hwith the combined method. In contrast, there were no significant differences at any measurement time with brushing. For the elderly group (Fig. 3), com
pared with the values at T
0, the bacterial load was significantly lower at T
1with tablets, and at T
2hwith the combined treatment. Furthermore, the values with tablets were markedly higher at T
2hthan at T
1. With brushing, the values were significantly lower at T
2hthan at T
1.
Changes over time with the combined method When the bacterial load with the combined method was monitored over time, the values were markedly lower at T
1’, T
1hand T
2hthan at T
0in the young group, while this decrease was observed only at T
1’and T
2hin the elderly group (Fig. 4).
Fig. 1 Comparison of the number of bacteria on the tongue for various treatment methods and age groups. The elderly had higher bacterial loads than the young for all time periods. On the other hand, the bacterial load with the combined treatment was markedly lower than with brushing at T1, T1hand T2h. In contrast, the values of bacterial load with tablets alone were significantly lower than with brushing at T1in both age groups, and at T1hin the young group (*p<0.05).
Fig. 2 Number of bacteria on the tongues of the young healthy adults. Compared with the values at T0, the bacterial load was markedly reduced at T1and T1hwith tablets, and at T1, T1hand T2hwith combined treat
ment. In contrast, there were no significant differences at any measurement times with brushing treatment.
Fig. 3 Number of bacteria on the tongue of elderly receiving nursing care. Compared with the values at T0, the bacterial load was significantly reduced at T1with tablets, and at T2hwith the combined treatment.
Furthermore, with tablets, the values were markedly higher at T2hthan at T1. With the brushing method, the values were significantly lower at T2hthan at T1.
Fig. 4 Number of bacteria on the tongue with the combined treatment. The bacterial load with the com
bined treatment was markedly lower at T1’, T1hand T2hcompared with that at T0in the young group, while this decrease was observed only at T1’and T2hin the elderly group.
DISCUSSION
Experimental methods
Ito et al. reported that nylon brushes effectively re- move the tongue coating, while reducing care- related pain.
15We used the Mini Moa tongue brush in this study. The Bacterial Counter is a simple de- vice that was recently developed to conveniently examine the bacterial load in the oral cavity. The device automatically measures the bacterial load by the mechanism of electrophoresis of specimens collected using sterile cotton swabs in sterile dis- tilled water. The values obtained are highly accu- rate, and show a significant correlation with those obtained using quantitative polymerase chain re- actin (PCR) after collecting specimens from the tongue in the same manner using swabs, as indi- cated by Tashiro et al.
16The device is also light and portable, enabling researchers to take it to care facilities. The results can be obtained immediately after each measurement for specimens collected from the subjects. Specimen collection was per- formed using the method of Tashiro et al.
Comparison of the bacterial load at the baseline between the age groups
The bacterial load at T
0did not markedly vary among the treatment methods in either group. As this confirms that there had been no carry-over ef- fects in this crossover study, the inclusion criteria for each age group are likely to have been appro- priate. On the other hand, the bacterial load at T
0was significantly higher in the elderly than in the young group. Winkler et al.
4reported that the tongue coating tends to be greater in the elderly, suggesting that the bacterial load increases with the level of tongue coating.
Effects of the brushing method on the bacterial load
We examined the effect of tongue cleaning from before treatment to up to 2 hours after as a short- term trial. Tashiro et al.
16noted that in general there was a temporary increase in the bacterial load in the oral cavity immediately after oral care. Reports
on the bacterial load on the tongue dorsum after treatment vary widely. While Gilmore and Bhaskar
17reported that tongue cleaning reduced the bacterial load, Van der Velden et al.
18and Menon et al.
19noted that there were no significant differences in the colony forming unit (CFU) when they examined specimens collected immediately after tongue cleaning using swabs.
In the study by Hotta et al.,
20the bacterial load at T
1was unchanged or greater than the value at T
0in both groups when using the brushing method. This is consistent with reports by Van der Velden
18and Menon.
19In another study, the appropriate force when using tongue brushes was determined to be 50 to 100 g. In our study, tongue cleaning was per- formed by only two researchers who uniformly ap- plied a force of approximately 60 g during the pro- cedure after calibration using a meter. The results highlighted the fact that the bacterial load is not re- duced by abrading the tongue using brushes for tongue cleaning, even with application of an appro- priate force.
Quirynen et al.
8conducted experiments to exam- ine long-term changes in the bacterial load on the dorsum of the tongue after cleaning. They found that although tongue cleaning for two weeks de- creased the level of tongue coating, it did not much change the load. They observed that the complex surface properties of the tongue dorsum may have prevented tongue brushes from reaching deep into the grooves. Similarly, the higher bacterial loads that we observed after tongue cleaning using a tongue brush may be indicative of how difficult it is to remove bacteria with only mild abrasion of the tongue surface. Instead, such brushing may possi- bly have resulted in pushing the bacteria deeper into the tongue coating.
When time-dependent changes were observed
beginning immediately after treatment, there were
significant differences in the values at T
1and T
2hin
the elderly group. With time, bacteria and debris
that had surfaced as a result of cleaning using a
tongue brush may have been washed away and re-
moved from the tongue dorsum by the saliva and
tongue movements for up to 2 hours after treat-
ment. However, significant decreases in the bacte- rial load were not observed at any measurement time compared with T
0with the brushing method. In short, cleaning using tongue brushes may require several hours or days to visually affect removal of the tongue coating and reduce halitosis. It is not likely to significantly reduce the bacterial load.
Effect of tablets only and the combined method on bacterial load
The tablets were effective immediately after admini- stration. The bacterial load at T
1was markedly lower than at T
0. This was also true for the com- bined method in the young group. This decrease at T
1was also observed in the elderly group with the tablets although there was no significant difference with the combined method. The difference in the bacterial load immediately after treatment between the chemical and mechanical treatment methods may have been associated with variations in the actions of the tablets and tongue brushes in terms of bacterial removal.
Biofilms are composed of bacterial cells and ex- tracellular polymeric substances (EPS). EPS ac- count for 50 to 90% of all organic matter contained in biofilms, and they protect bacterial cells from physical stimulation when attached to their sur- faces. EPS comprise polysaccharides, DNA, and proteins.
21The tablets used contain the kiwi-derived cysteine protease actinidin with a low degree of substrate specificity, which is thought to effectively degrade proteins and detached epithelial cells, which are in the EPS and tongue coating. Com- pared with such tablets, mechanical cleaning meth- ods, including the brushing method, may be ineffec- tive for complex three-dimensional structures, rep- resented by the tongue surface.
Tablets are likely to be effective for both chemi- cal removal by enzymes and mechanical cleaning by the rough surface of the tablet. Motor functions are important in the latter mechanism, which occurs through abrasion by the tongue and palate. Sugi- moto et al. examined the ingredients in tablets and their effect in removing the tongue coating. They concluded that chemical cleaning is more effective
than mechanical cleaning.
22We observed significant decreases in the bacterial load in the care-de- pendent elderly who had reduced tongue function.
The effect of the tablets was even greater in young adults, and the bacterial load was reduced 90%.
With the combined method, the effect was differ- ent for the two age groups during the period be- tween T
0and T
1. While the bacterial load was sig- nificantly lower at T
1’after tablet administration, compared with that at T
0in both groups, it showed a marked increase at T
1only in the elderly when the tongue brush was used. Such an age-related difference in the bacterial load after tongue brush use may be explained by two factors. First, there was a higher tongue coating level and bacterial load of the elderly. As the bacterial load on the tongue dorsum was already significantly greater in them compared with the young group at T
0, the level of bacteria that had surfaced from the depth as a result of the tongue brushing may have ex- ceeded that removed by the tablet. The second fac- tor is the age-related difference in the motor func- tion of the tongue. The reduced tongue function of the elderly may have interfered with the effective removal by the tablets. In contrast, in the young group, time-dependent changes in the bacterial load were similar between the tablet and combined methods.
Although Nohno et al. reported that the admini-
stration of tablets containing actinidin for 7 days
was effective for reducing halitosis, their effect on
the bacterial load of the tongue dorsum was not ex-
amined.
12We found that compared with the values
at T
0, the bacterial load was significantly lower at
T
1hwhen using the tablet or combined method in
the young group, and at T
2hwhen using the com-
bined method in both groups. This indicates that
tablets were effective for reducing the bacterial load
for up to 1 hour after use in the young group, and
that this effect was prolonged for up to 2 hours
when the tongue brush was also used. In short, al-
though the effect of tablets is likely to last for a
shorter period in elderly who have reduced tongue
function, this effect may last for up to 2 hours when
the tongue brush is also used. We concluded that
the time needed for the treatment to be effective may be shortened, and the duration may be pro- longed in accordance with the level of debris re- moved with the tongue brush. Further study is needed to clarify the effect of the tablets for periods longer than 2 hours, and to examine methods of combination treatment to prolong this effect.
CONCLUSION
The effect on bacterial load on the tongue dorsum of the three treatment methods were similar, re- gardless of age. Compared with the tongue brush, the use of tablets was more effective at reducing the value for up to 1 hour after treatment in both the elderly and young groups. Furthermore, their combined use maintained this effect for at least 2 hours. These results indicated the effectiveness of combining tablets and tongue brushes for all age groups. On the other hand, even when using the combined method, the bacterial load was markedly higher at T
2hthan at T
1in the elderly group, and the time needed for this value to increase was less than in the young group. There were also differ- ences in the values at T
0and T
1between the two groups when this method was used. This suggests that the initial level of tongue coating also influ- ences the duration of the effect of the tablets.
Tashiro et al.
16discussed methods of aftercare to more effectively reduce the bacterial load. After oral care, a mass of detached bacteria is generally dis- charged from the oral cavity when gargling or swal- lowing, and most of the swallowed bacteria is killed by gastric acid. This emphasizes the importance of collecting detached contaminants, as well as re- moving debris, when performing oral care for the elderly who have difficulty gargling. When using the methods of the present study, it may be possible to further reduce the bacterial load after use of the tongue brush, and prolong the effects of treatment by initially wiping the tongue with gauze, or continu- ously performing tongue cleaning to lower the baseline values.
REFERENCE
1. Dadamio J, Laleman I, Quirynen M. The role of toothpastes in oral malodour management.Monogr Oral Sci 2013; 23: 45-60.
2. Quirynen M, Dadamio J, Van den Velde S, De Smit M, Dekeyser C, Van Tornout M, Vandekerckhove B. Character- istics of 2000 patients who visited a halitosis clinic.J Peri- odontol 2009; 36: 970-975.
3. Lang NP, Attstrom R, Lindhe J. Proceedings of the third European workshop on periodontology. Berlin : Quintes- sence, 1999 : 102-129.
4. Winkler S, Garg AK, Mekayarajjananonth T, Bakaeen LG, Khan E. Depressed taste and smell in geriatric patients. J Am Dent Assoc 1999; 130: 1759-1765.
5. Takeshita T, Tomioka M, Shimazaki Y, Matsuyama M, Koy- ano K, Matsuda K, Yamashita Y. Microfloral characterization of the tongue coating and associated risk for pneumonia- related health problems in institutionalized older adults. J Am Geriatr Soc2010; 58: 1050-1057.
6. Yaegaki K, Coil JM, Kamemizu T, Miyazaki H. Tongue brushing and mouth rinsing as basic treatment measures for halitosis.Int Dent J 2002; 52: 192-196.
7. Slot DE, De Geest S, van der Weijden FA, Quirynen M.
Treatment of oral malodour. Medium-term efficacy of me- chanical and/or chemical agents : a systematic review. J Clin Periodontol 2015; 42: 303-316.
8. Quirynen M, Avontroodt P, Soers C, Zhao H, Pauwels M, van Steenberghe D. Impact of tongue cleansers on micro- bial load and taste.J Clin Periodontol 2004; 31: 506-510.
9. Yaegaki K, Sanada K. Volatile sulfur compounds in mouth air from clinically healthy subjects and patients with peri- odontal disease.J Periodont Res1992; 27: 233-238.
10. Kojima K. Clinical studies on the coated tongue. Nihon Koukugeka Gakkai (Jpn J Oral Max Fac Surg) 1985; 1: 1659-1676. (Japanese)
11. Yoshimatsu D, Sugimura S, Ioka S, Shiraishi H, Yonetani S, Yamaga T, Miyazaki H. The effects of tablets including pro- tease on tongue coating removal. Koukueisei Kai Shi (J Dent Hlth) 2006; 56: 37-41. (Japanese)
12. Nohno K, Yamaga T, Kaneko N, Miyazaki H. Tablets con- taining a cysteine protease, actinidine, reduce oral malodor : a crossover study.J Breath Res2012; 6: 1-5.
13. Kays SA, Hind JA, Gangnon RE, Robbins J. Effects of din- ing on tongue endurance and swallowing-related outcomes.
J Speech Lang Hear Res2010; 53: 898-907.
14. Mendes AE, Nascimento L, Mansur LL, Callegaro D, Jacob Filho W. Tongue forces and handgrip strength in normal in- dividuals : association with swallowing.Clinics (Sao Paulo) 2015; 70: 41-45.
15. Ito K, Fukuhara T, Kouchi I, Inoue M. Relation between tongue cleaning effect and type of brush. Nihon Sessho- kuenge Riha Kaishi (Jpn J Dysphasia Rehabilitation) 2009; 13: 77-87. (Japanese)
16. Tashiro H, Tamura F, Hirabayashi M, Hamada R, Yone- yama T, Kikutani T. Development and clinical application of a novel rapid oral bacteria detection apparatus. Nihon Shogaisha Shika Gakkai (J Jpn Soc Disabil Oral Hlth) 2012; 33: 85-89. (Japanese)
17. Gilmore, EL, Bhaskar, SN. Effect of tongue brushing on bacteria and plaque formed in vitro. J Periodontol 1972; 43: 418-422.
18. Van der Velden U, Kippuw N, Petit M, Van Winkelhoff AJ, De Graaf J. Localization of microorganisms on the tongue and the effect of cleaning.J Dent Res1989; 68: 1007.
19. Menon MV, Coykendall AL. Effect of tongue scraping. J Dent Res1994; 73: 1492.
20. Hotta M, Nagai K, Imade S, Sano A, Yamamoto K. The safe use of tongue brush−Stained tongue brushing force in sub- jects−.Nihon Shika Hozon Shi (Jpn J Conserv Dent) 2007;
50: 332-337. (Japanese)
21. Flemming H-C, Wingender J. The biofilm matrix. Nat Rev Microbiol 2010; 8: 623-33.
22. Sugimoto J, Takahashi K and Komasa Y. Effect of a protease-containing tablet with rough surface on the number of bacteria on the tongue.J Osaka Dent Univ 2015; 49: 165-170.