wa7twlk\
ee
21
geg2-e・
69
-i
76
fi
(1994
ff)
"susrs
ll
ManualTherapyin
Practice*
RichardErhard"
Iam honored to be invited to
Japan
by Dr.Nara and Dr.Takahashi to address the annual PracticalAssembly
of theJapanese
Physical
Therapy
Associ-ation.
I
wouldlike
totake thisopportunity togive
special thanks to
Professor
Morinaga
andMr.
Harada for theirspecial assistance in making this
possible.
My
topictoday,Manual
Therapy in Prac-tice,along withMr.
Searle's
topic,History
and Pres-ent Circumstances of Manual Therapy in theWorld, has made me realize
how
the practice ofmanual therapy has changed in the nearly twenty
years since Iwas elected firstpresidentof IFOMPT.
In
order toillustrate
rnanual therapyin
practice,I
shall attempt to
follow
alew
back
pain patientfrorn
presentationin
theclinic tothe end of thetre-atment, including the history, behavior of
symp-toms and physical examination. Ialso hope to be
able toprovide you with
data
supporting manualtherapy. I noted in your
handout
yourdesire
for
perhapsincreasing
the scientificbasis
of physicaltherapy; we also have thisdesire, We regard itas our mission toelevate the status of manual therapy
to
a science. Ihopeto
be
ableto
alludeto
thissup-porting
data
as we go through thepresentation-something that
I
wouldn'thave
been
able todo
until very recently.
Because
of the many technicalchanges, manual
intervention
per se willbe
just
one component of the system that we now call
"manual
therapy". Inorder tofacilitateyour
under-standing
I
will use slides and pictures,.
eelastaoxwa
.. AAOMTE.IJ--ft
Vice President, A.A.O.M. T.,Center forSports cine and Rehabilitation,Universityof Pittsburgh
The Cathedral of Learning at the University of
Pittsburgh is where Ipractice with my colleague,
Dr.
Anthony
Delitto,
in
theDepartment
ofPhysical
Therapy,
School
ofHealth
and Rehabilitation Sci-ences.Low back pain is often regarded as a
practitioner's
dilemna,
thusit
enables the manualtherapist
to
tread upon ground where thereis
notgood scientific data.The main problem isthe
patho-physiology
for
low
back
painis
not well under-stood. Experts' estimate from 10 to20 per cent ofback pain can
be
attributed toan identifiablepatho-logical
entity,
What
we're going todo today isemphasizeclassi-fication,
notdiagnosis.
This
was coined by anor-thopedic surgeon, Dr.Mooney, in 1979 and we have
been trying since that time to utilize the
classifica-tion procedure
in
addressinglow
back
pain.The
first
order of classification is"Can
the patient bemanaged
independently
by physical therapy?", or `tDoes thepatientrequire referra} toanother
practi-tioner?",or "Dees
the patient require consultation
with another
health
care practitioner?"The
differ-ence
between
a referral.and
consultationis
that areferral
is
for
a patient who needs furthermedicalworkup, we suspect serious pathology or pain ef non musculoskeletal origin. Consultation,however,
can
be
for
apatient
who may be helpedby
ad-junctive
medication forexample, non steroidal antiinflammatories.
Finally,"Whatto
do
with a patient
who exhibits magnified illnessbehavior?" We have
found itisimportant toidentify these patients as early as
possible.
70
vee#kza{}k
Thefirst
step thenis
to classifythe
patient-acute versus chronic, physical versus psychosocial
or with psychological
factors,
serious pathologyversus mechanical
low
back pain.In
order todo
this,we must take a thorough historyand do a
care-ful
physical examination.The
subjectiveexamina-tion
is
very important inlowback
pain inparticu-lar
and the spinein
generaLWe
needto
have
apa-tient
history. The patient must be suitablefor
a mechanical diagnosis;therefore,we need a currenthistory
and historyof previous episodes as well assymptom
behavior
with activity and/orposture-what aggravates
the
patient,what easeshis
pain,what are the risk
factors?
For
example,is
the pa-tienta smoker, ishe involved in repetitive lifting,etc.
After
considering these,we must make apro-visional
diagnosis.
First
we startby
having
the
patientfi11out a self-assessmentform
called anOswestry.
Inour prac-ticewe havefound
thatif
a patienthas
a score of75% or more of totaldisability,thiswould
indicate
very severe involvement and poor prognosis. We
may need
to
use medical screenlng forthispatientor have magnified illness
behavior
investigated.Each
patient comingin
everyday
for
treatmentmust
fi11
out abody
diagram.
The
patientfilts
outthe body diagram where he feelspain, paresthesia,
or both. He also fillsout a visual analog scale.
This isnumbered from O
(no
pain)to 10(pain
assevere as could
be>.
In practice,we no longer usethe numbers,
just
the two definitionsbut for pur-poses of explanation today,I
have
included
thenumbers. Inpractice, we simply take a centimeter
stick, layiton the scale and number
it
after thepa-tienthas chosen
his
level
of pain.We
found
that staging thepatient
with low backpain
syndromeis
more related to the severity of
disability
than theduration of symptoms; thus,sometimes the terms "acute", "subacute"
and "chronic"
are lessuseful, in factmore diMcult, than not using these terms. If
you look at the current literature,thereare several
different
opinions as towhat constitutes thedifini-tionof acute, subacute and chronic.
We
trytohave
ee
21
gee
2
it
goal oriented. AStage
Imeans that the patient hasdiMcttlty
in performing the basic mechanicalfunctions
of standing, walking, sitting or all ofthose.
Stage
II
means the patientcan performbase
lineactivitiesbut
cannot do thisfor
any extendedperiod of time without recurrence or worsening of status of symptoms. In Stage IIIthe patientcan sit, stand or walk
indefinitely
but
is
unableto
form
the requiredduties
of employment or sport.Stage IV isprevention of occurrence or recurrence. The examination procedure then,after the history istaken, starts by the initialobservation of
ing
the
patientremovehis
shoes and socks.We
alsotrytoobserve the patientarising
from
a chairout him being aware that we are making such an observation. Itisa good idea tocall the patientin
from the waiting room yourself,enabling you to
observe
the
waythe
patient arisesfrom
the
chairor,
in
fact,that he may not even take thenity of sitting while awaiting your calL
Next,
we
look
at thepalpationof the pelviclandmarks
in
theweightbearing pelvic prone knee flexiontestis
tt
itive,we may then intervene and treatthe pelvis, return the patientto thestanding positiontosee if these landmarks
have
changed. Finally,we aregoing to perform movement testing-standing,
ting,supine and prone, todetermine which way we
should treatthispatient. The
lower
quarter screen isdesigned then to identify problems with thelower
extremity kinetic chain-is there a pelviccompenent; istherea leglengthdiscrepancy or are there problems arising
from
the hip area?These
we need toeliminate as soon as possibletogive us
a clear picture or what
is
occuringin
thelumbar
spine
itself.
The
specifics of examination then are tolook
at the signs, the symptoms, and mostportantly to us as
far
asdriving
treatment,has
the symptorn changed with response todifferent
ment?
After
evaluating allthesevariables, we thenrnust commit ourself toa provisional diagnosis. Is
thispatienta mechanical or non mechanical
lem;
is
he
aStage
I
or aStage
II;
perhapshe
needsftItszaoscwa
exam or
do
wehave
todo pain modulation beforeengaging inmovement testing, Let'stake an
exam-ple of a patient
in
Stage
I,
patients whodemon-strate a change
in
status withfunctional
activity ofsitting, standing and walking.
In
thisstage, our goalis
pain modulation.These
are thedfferent
syndromes thatwehave
identified
that exist intheStage
I,orPhase
I,
patient:extension, flexion, later-al shift, mobilization,traction,
immobilization,
orthe aforementioned
lower
extremityinfiuencing
pelvic involvement,
hip
and/orleg
Iength.
We wouid then subcategorize thesepatientsintoone ormore of thesevarious syndromes so that we can
in-itiate
treatment.
The
first
syndrome thatI
wouldlike
todiscuss
with you
is
one thatimproves
with avoidance ofmovement, the one we call immobilization. The
first
example wouldbe
a patientthat exhibitsun-stable spondylolisthesis;
this
wouldbe
described
as abony
instability,
however
you can also see that thereis
discal
instability
associated with thispar-ticularpatient
(making
reference tothe x-raybeing
observed).
The
next x-rays viewed are of adiffer-ent patient,
first
standing erect and second when asked to bend forward while inthe standingposi-tion.
From
the
x-ray, you can see hislordosishas
actuallyincreased
slightly comparedto
his erectstanding position.
The
next view showsthe
samepatient
in
forward
bending
after repeating4
for-ward bending movements. Now you can see that
with
the
protectivemuscle spasm inhibited,thepa-tient
has
now losthis lordosisand, in fact,hasex-hibited
what we call "Discalinstability",
that
is
tosay there
is
no real translationpresent
but
thedisc
has lostitsintegrity when asked to assume load
bearing with the
flexion
of the lumbar spine, Thefunctions of lumbar immobilizaiton are to serve as a rerninder
for
l)
restriction of movement; 2)toapply abdominal pressure to
decrease
loads
on thelumbar
spine; and3)
tomaintain a normallumbar
lordosis.
We
are of theidea thatwe can't trulyim-mobilize a spine,
but
we are goingto
preventit
from getting to the ends of the range of motion.
71
One
ofthe
severaldevices
we can usefor
thisistheMacNab
brace.
The
patientis
placedin
this
brace
which
has
a lumbar componerrt as well as athorac-ic
component. This enables thispatientto
remainimrnobilizedinthe standing positionas well as the
sitting. One of the
big
problems with usingexter-nal immobiLization iscompliance. One of the
ad-vantages of thisparticular
device
is
thatit's
easy toget
into
and out ofby
oneseLf.There
are also syndromes thatimprove withpas-sive movement. Remember we talked about the
immebilizaiton patient who actually improved
his
status with avoidance of movement.
Now
we are going totalk about those whoim-prove with passive movement, First,the
mobiliza-tionand tractionpatients.
Mobilization
and Manip-ulationSymptoms
IIrefers to thelumbar spinepa-tient.
We'11
talkaboutthe
pelvisa littlelater.The
history
is
frequently
acute, sudden onset, withoutdeformity-that
is,
when you see thepatient,
hehas
no shift orkyphosis.
Frequently
the pain hasoccurred during extension from the forward
bend-ing
positionand sometimes with rotation.There
is
unilateral pain and
if
referred painis
present,it
confined toabove the
knee.
Signs
presentin
this type of patientare negative or absent neurological signs, unilateral pain with flexionin
sidebending
tothe opposite side;
in
order tomake this diagno-sis, wehave
torule out muscle spasm, The otheroption isunilateral pain with extension and side
bending
onthe
same side; we rnust rule out manip-ulation and mobilizationL
The next x-ray isapa-tient standing, neutral position
(not
sidebend-ing).
Now
thepatientis
attemptingto
sidebend
to
the left;there issome motion in the iower lumbar segrnents as
he
attempts thismotion. Whenthe
pa-tientside bends to the right, the lefthip ispulled
up off the
floor,
16oking at L3, we can see aconsid-erable amount of motion istaking placebetween L
3
anclL4,
The
problemis
thatno motion is'takingplace at
L4,
L5
orL5,
SL
This
is
the opposite ofthe
immobilization
patient that we showed eariier
72
wa\mstw\
enough movement, This treatment isvery sirnilar
to
what Ian demonstrated earlier on his patient;inthis particularcase, we are doing soft tissueto
insure
that
this
patient'sproblem isnotjust
restric-tion of soft tissue. Note that we have him in the
leftside
bent
position.Moving on tea mobilization or manipulative procedure, we want toopen up the side opposite towhich heis
restricted. Inthe sametype of pattern shown on the x-ray, the patient would not close down on theside towhich he was
bending
and, in thiscase, after undergoing thesofttissueand the traction or opening maneuver, we
would
be
obliged to close down on the side towhich
he
is
restricted.We
haye
a verybig
problemin
thatdetermining
what workshas,
to date,been veryindividual
and, asMr.Searle
has
pointed out,has been emperical. There are a number of
differ-ent approaches,
but
we think itistime for us tobecome
more scientific, so wehave
to
determine
what works. Currently, we're using a consensus
panel opinion and what we want to
head
towardis
a peerreview publication,As we go
from
case study to quasi-experimentalstudy to true experimental studies, we have in-creasing diMculty in doing these types of studies.
On
the
otherhand,
the
relationship oftreatment
to
the outcome is
better.
We
think we have todo
allof the above,
but
ideally
we wouldlike
to
be
ableto do experimental studies. This
proves
muchmore dithcultin the clinic than most kinds of
'perlments.
First,we're going to use a case presentation.
This
is
something thatI
urge allof you todo.
It
was once considered thatcase presentation was not
scientific;
however,
if
you read medicaljournals,
inparticularorthopedic
journals,
they use casepre-sentations very well. We need to do more of these
-this
is
the
simplest method ofjustifying
what wedo.
This particularpatientisa manual laborerandpresented with
left
back
andleft
leg
pain.He
wasshifted away from his pain; he had flexion,side
bending
and rotation tothe right; he hadneurolog-icalsigns eminating from L4, L5; his straight leg
E21gee2g
raising on the leftwas 20"; his extensor hallisus
longus was weak and he had a
decrease
inhis
Achil-les refiex. This is the way he presented to the
clinic-he is
deviated
to
the
right, he isfixed
in
kyphosis, he isinright rotation, and heis
attempt-ing totake weight off
his
Ieft
lower
extremity.Fol-lowing the treatment categories that we discussed
earlier, we are going toplace him intothecategory
of lateralshift correction-very much inPhase
I.
A
lateralshift syndrome isa movement-related
symp-tom
behavior.
He
is
unable tositfor
prolongedperiods;
he
worsens with activityinvolving
fiexion;he
also worsens with walking. Sittingand walking are worse than standing. Usually a listisnoticea-blewhile standing. Very asymmetrtcal side
bend-ing,
this iskey to driving the treatment;he
has
to be able to side bend further in one directionthan the other.He
improves
with pelvic translocationand extension and
he
worsens with straight planeextension or flexionmovement. This isthe clinical
picture of the Iateralshift patient.
AsI mentioned earlier, some of the technical
ad-vantages have made manual techniques
just
a part,or component, of our approach now.
This
particu-lardevice,auto trac,isextremely useful
in
treatingthis
type
of patient.It
is
a system of mechanicallyfacilitated
passive movernents, which utilizescom-binations
of active muscle contractions, traction, and controlled spinal stabilizationin
orderto
expe-dite
return tonormal functionalactivity with whatwe callunloading and reloading.
The
systemcon-sists of an electrohydraulic table and its ac-cessories, a very simplified examination system and
specific treatment protocol. Originally
this
table
was manually controlled with largewheels and the greatest advantage to the more modern version is
the ability toreload thepatient.Inother words, it's a tilt
table.
Looking at our patient again,
he
is
in
antalgia, and thislargely
determines
how
we wilibegin
withhim on,the bable. The firststep istoaccomedate
his
defermity.
Since
he
wasin
antalgiain
theposi: tion described earlier, we do the same thing withftltazadiXwa
the tabletop toaccomodate te
his
deformity,
allow-ing the table to take responsibility forhis spasm.
Through
a gradual process of pulling and pushing,we correct the patienttaking
him
out ofhis
antal-gic posture and put
him
into
the restriction ofhis
deformity. This iscalled the corrected step,
Following the successful completion of those two
steps, we put
him
in
a gradual reloading position,inother words what made
it
possibletomake thesecorrections was the
fact
that wehad
taken gravityaway. Now, having made thiscorrection, we had to
be
very cautious and careful about resuming the effect of gravity. Afterthe
patient has achievedfullweightbearing, we make sure that,as
he
comes offthe
table,
he stays in the erect position,main-taining
his
correction as much as possible,as well as the lordosis.Then we'11have
the patientambu-late.
That was an example of a case study using one
particularcategory
(that
of thelateral
shiftcorrec-tion) in Stage I where our primary goal ispain
modulation.
We
are able toiRustrateseveralexam-ples: the patient who
is
inacute pain thereforequa-lifyingas Stage I,utilizing a case study and
being
able todemonstrate theeffectiveness of(in
thispar-ticularca$e) the auto tractabletreatment of Iateral
shift correction.
Next,
we're going to move toward a more73
cult
but
morepowerful
form
ofjustification,
andthatistheexperimental process. For the most part
today there are more studies done on manipulation
than any Qther modality ef treatment
in
the spine,and
in
particular, thelumbar
spine.However,
theprocess has been to take the patients,divide them intotreatment groups and comparison groups; give
one group treatment with manipulation and anoth-er group treatment with some placebo or other
type of treatment.・
The
big
diMculty
with thispro-cess isthat
you
don't
have
a classification, thatis
tosay this
is
not the way we practice.We
want todetermine what patientisgoing torespond towhat
treatment.
We
wouldn't think of putting allthe pa-tientsinto
one group anddoing
manipulation-there would have to be indication in this area,
Therefore, we have considered that intervention is
more than
just
treatment. Firstwe have todo clas-sification, then we put one groupin
an unmatchedtreatment and another group
in
a matched treat-ment.
In
the case of extension-type patientandmanipu-lationpatient,ifwe matched these patients with
the appropriate treatment, we should get a
better
outcome than
if
theyhad
unmatchedtreatment---thaVs the hypothesis. When we're matching
treat-ments by category, the matched treatment should
be more efficacious than the unmatched treatment.
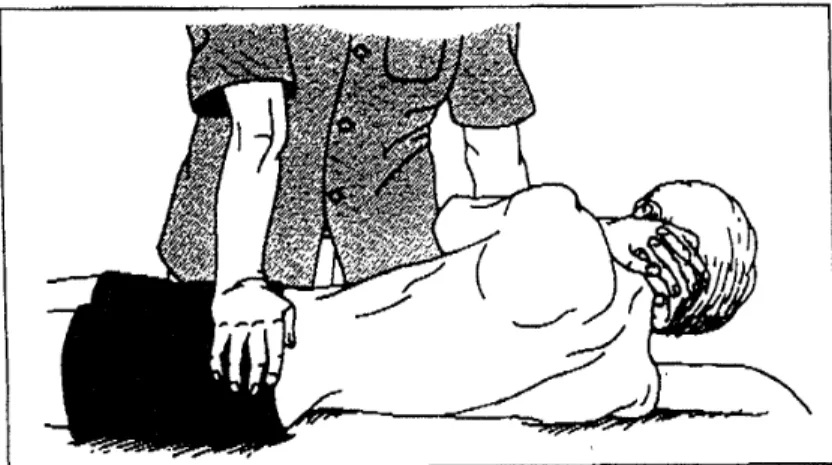
Fig. 1. The manipulative technique
for
the sacroiliacjoint.
<Reprinted
with perrnissionof AmericanPhysical
Therapy
Association frern
Cibulka
MT.
The treatment of thesacroili-ac
joint
component tolow
back
pain. a case report.Phys
74
ve\tsza\
Will
this resultin
earlier work return and,there-fore.
resultin
cheaperhealth
care costs.We
have alotof attention inthe United Statesnow regarding
the
cost of healthcare. We have tobe
able to'
onstrate that our treatments are not
just
effective,but
cost effective.
This
is
a study that was published inApril 1993in the
Journal
of theAmerican
Physical
Therapy
Association.
Our
group wasDr.Anthony
Delitto,
Michael Cibulka and
Janet
Tenhula of St.Louis,Richard
Bowling
of theUniversity
of Pittsburgh,and
I.
The
study was titled"Evidence forUse
of anExtension-Mobilization Category in
Acute
Low Back Syndrome:A
Prescriptive Validation Pilot Study." Inother words, we identifiedextension andmobilization patients and mobilization patient in
acute
low
back
pain anddivided
thosgby
the tossof a cein into treatment involving both
mobiliza-tionand extension
in
the experimental group.The
control group received treatment involving flexion
exercises as you shall see, The acute patientscame
into the clinic referred with low back pain
syn-drome.
We
then classified the patient and placedsorne of those patients
(determined
by
theflip
of a coin) jnto the designated treatrnentcategory. Theeg
21
geg
2
rest of those patients went intoa non specifie, but
acceptable, treatment-in this case, Williarns'
flexion
exercises.We
measured the outcomes ofthe two groups and compared one tothe other.
All
patients in the study were referred primarily for lowback
pain,that isthey could have hadthing else in addition, but the primary reason for referral was
low
back
pain.They
were all referred
by
physicians.Thirtynine
patients wereinitiallS
admitted; 24 were classified as the
lization
category. The remaining15
weremissed
from
thisparticularstudy.The
mean agewas 32±11,including 14men, 10women, and 4 tientswith symptoms below the knee;
the
der had symptoms stopping at the knee er above.
Thus,
only patientsassigned totheclassification ofextension and rnobilization were admitted. This
was a number thattotaled 24. Subjects were then randomly assigned totheirmatched group, zation/extension, or the unmatched group, flexion
exercise. The mobilization treatment was a
Grade
5
(manipulation)
purportedlydirected
tothe
iliac
joint.
The extension regimen was givenly as described by Mackenzie, including pressups and use of a lumbar roll. The flexionregimen
(the
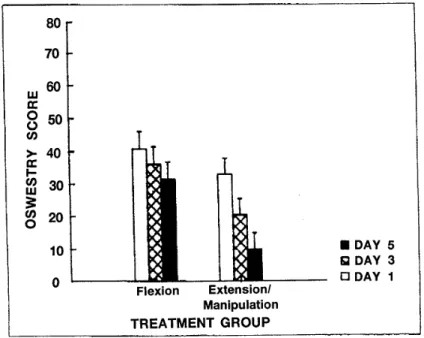
Fig.
2.
Between-group
comparison of.Oswestryquestion-naire scores
initially
and at 3-and 5-dayfollow-uPs.
(Error
eeE]!twVidi=wa
other
group)
wasgiven
a regimen exactly asde-scribed by Williams and the subjects were seen
three times per week fora
total
of one week,The
outcome measure was the Oswestry low
back
painquestionnaire,which
is
afunctional
self assessmentthat addresses the
diMculty
apatient
has withrou-tineactivities of daily living,such as sleeping,
wal-king,
standing, sitting,lifting
etc.One
ofthese
wasfi11edout
before
each visit and the treating thera-pistwas unaware of what theindividual
Oswestry
scores were on each patient. The way we assigned
these patientstoextension syndrome was
by
asses-singtheir
movements, soflexion
in
standing,supine and extension
in
standing and extension prone. were performed.Pelvic
translocation,both
directions,with pressup. Additionally, postural advice was given and the patientwas supplied with a
lumbar
rollto
maintain extension,The
data
anal-ysis
is
dene
by
2×3(treatment
group by treatmentperiod)
ANOVA,
Comparisons
with age, onsetperiod and initialOswestry scores were
done.
There was a significant differencebetween the two
groups
in
age,the
manipulation extension group was significantly older than the othergroup.
Therewere no other
differences.
A
bar
graph showingthe three treatments refiects the flexion group's Oswestry score at onset to be in the low 40s
(I
should say
that
the
Oswestry
is
like
golf-thelower
thescore, thebetter,
because
what you arelooking
for
is
the percentage ofdisability>.
The
secondbar
shows the second visit
in
theflexion
exercisegroup
and the thirdbar shows the thirdand final
Oswes-try score
in
this control group. Thefirst
day's
score of the extension/manipulation group was
done
before
any intervention,as wasthe
scorefor
the fiexionexercise group. When the patient
pre-sented
for
the second time,anOswestry
form
wasfi11edout beforethe treatment. Please note thatthe
second score
in
thisgroup waslower
than theulti-mate score
in
theflexion
exercise group.Finally,
the third
bar
represents thefifth
day
(final)
visit, inwhich case
the
Oswestry
scorein
the experimentalgroup was about 11%
(See
Fig. 2).We
recognize
75
that we
have
some severe limitation$,We
had
avery small N, so we called ita pilotstudy.
Only
one clinician classified the patients,therefore we
had
limited
generalizabi]ity. We did nothave
acontrot group, in other words,
it's
possible thatwhat we saw with the treatment group was the normal
process
oflow
back
pain inthe acute stage andby
givingfiexion
exercises, wejust
retardedthe progress inthe other greup,
With
no controlgroup, we really could not prove that was not the
case.
Finally,
there was no way of dissecting outthe effect of manipulation versus theeffect of exer-cise
because
in
the experimental group, wedid
both.
We then move
into
the next stage, which isPhase
II.
Please
note that we use these phasesrather than acute, sub acute and chronic because
the chronology
does
not always help us indetermi-ning which stage the patient isin.
What
We
have
to address here isto manage other things such as
checking
the
patient'sflexibility,
strength, leveloffitness,posture and occasionally we'11 try for
cor-rection of
identifying
positive factorssuch asleg
length discrepancy, poor posture, too much/too
littleflexibility,too littlestrength or poor
fitness.
This isthe
goal ofthe
second stage,We
have
pro-gressed technicallyso that we
have
somesophisti-cated products of exercise equipment
that
we can use when the patients still have some pain.Re-member the patient isno longer
in
Stage
L
but
thesephases are not permanently separated,
i.e.,
thepatient can fall
back
from
one stage tothe next.For example,
the
patient maybe
in
Stage
IIbutafter
doing
something athome,
he has a regressionwhich puts
him
back
in
Stage
I.
There isno clear cutdeliniation
betweenthese
stages.IVs
primarily forour purposes that we use these, In thisparticu-lar
type of equiptnent, we havethe
ability toutilizestrength training and also accommodate
for
painanywhere in the range of motion.
This
is
accom-plished through a series of weight6 allowing us to
maxirnize or minimize resistance at virtually any
76
Eeiktaza\
perform early strength
training
withoutaggravat-ing
thepatient's symptoms.Six to ten
per
cent of the totalnumber oflow
back pain patients that we see
have
tobe
placedinto
the
phaseIII
group. This includesjob
simula-tion;
for
example, inour areaa good percentage of our patients are underground coal miners so wehave a situation where thepatientsatthisstage go intothe work
hardening
facility
and practice sho-veling. We have simulated mining conditions thatthe patientcan use and gradually get back toa full
shift.
Coal
mining isa good example of a usefor
this
because
once the underground miner goesdown
on the mantrip,he
hasto
stay undergroundforthe remainder of
his
shift except incases of ab-solute emergency. Itisimpossible tohave
thepa-tient
workLess
than
a fullshift. When the patientreturns
to
work, he must be able teperform a fullshift of employment otherwi$e the company will
not take
him
back.
This isthe kind of thing we do as farasjob
simulation.We
also have other thingswe can do in thisapproach; the type of exercise equipment Ishowed you earlier isfor stabilization
-stabilizing
the
muscles and increasingendurance.When we get to this stage we have anether type of
equipment where
it
enables us to provide forcesthat are unexpected,
in
other words, more of thereal lifefunctionalexperience.
The
best exampleI
can give you wouLd bea wheelbarrow.
If
you were standing at a loaded wheelbarrow on a slightgrade
where the grade was running away from you, and
you picked the wheelbarrow up from the ground,
not onLy would you have toliftthe weight, but you
would
have
to controlit
from
rolling awayfrom
you.
On
the otherhand,
if
you werefacing
up thefi
21
igee
2
e
inc}ine,as you picked up the wheelbarrow, you would not only have tolift
the
weight but alsolean
intoitso that itdid not push you over backwards.
We
have
another group of exercise machines thatwe can use at thisstage toprepare the patientfor
more reaL functionalwork-type experiences.
Unlike
Stage
II
where we are looking at stabilization, we call thismobilization. You haveto
have a certainamount of stability already
before
you enterthis
stage or you willfall
back
tothe second stage very quickly. Incidentally,both
of these types ofequip-ment are
in
Japan.
To
continue then,wedo
workevaluation, sequence training
(which
iswhat wejust
talked about) and we also dojob
simulaiton.Sometimes inthis stage, itisimportant forus to
do
wellness.Some
of the studies wehave
found,
inthe
States
indicate
that many of the reasonspa-tientsdon't want to return to work aren't
just
having to do with theirphysical weil being
but
with theirrelationship
with their supervisor, fellowworkers, etc.
Finally,
Phase IV isfor anindividual
withoutback
pain or withlow
grade back pain. That couldbe
a person whois
tryingto prevent occurrence or one thatistryingtoprevent recurrence. Infact,ail of the patients go through Phases I,IIand IVbut
just
a very few go through Phase III.Some
of the thingswe mighthave
todo are a work siteevalua-tion,ergonomic assessment, work modification and
education. Very seldom do we
get
involved inthese components,
but
we invariablydo
educationforprevention of recurrence.
Ihope that Ihave covered some topicsand have
stimulated some questions