THE THESIS OF DOCTOR OF PHILOSOPHY
Study on a Novel Type of the
Robot-assisted Endovascular
Catheterization System
Linshuai Zhang
Graduate School of Engineering Kagawa University
I
Abstract
For vascular tumors, thrombosis, vascular malformations, vascular contractions, vascular sclerosis, and other vascular diseases, endovascular interventional procedure is found to be the most effective treatment method. Compared with traditional open surgery, endovascular interventional procedure has many advantages: smaller incisions, quicker recovery and fewer complications. Nonetheless, some potential challenges also have been introduced in: repeated exposure radiation of the surgeon to X-ray causes occupational hazards; the surgeon must be highly skilled and specialized due to the high risks involved.
In recent years, the robot-assisted technology has become a hot study topic. To solve these challenges mentioned above, a master-slave robotic catheterization system, which can assist the surgeon to operate the catheter from a safe space, has made a great contribution to reduce the X-ray radiation and filter out the physiological tremors of a surgeon, as well as improve the position accuracy of the catheter. Despite their increased application and interest in this area, few systems have considered the ergonomic design to fit the natural behavior and operation modes of experienced surgeons during the traditional endovascular procedures. Inadequate force feedback and collision warning while operating surgical tools elevate the risk of endovascular procedures.
II
Inspired by such motivations, this thesis proposes a robot-assisted endovascular catheterization system that augments surgeon’s actions using conventional surgical tools, as well as generates feedback in order to ensure safety during the procedure. To implementation this, firstly, a novel slave manipulator based on electromagnetic braking is designed to realize adaptive, lossless and stable clamping for catheters/guidewires. A high-precision force sensor is embedded in the slave manipulator to measure the reaction force and realize the effective force feedback. Secondly, a theoretical model for collision protection based on the proposed clamping mechanism is established to alleviate the collision trauma to blood vessels, and the performance of the collision protection mechanism is validated by the in vitro experiments, which implies the realization of relative safe catheterization. Thirdly, the motion input unit based on the rack and pinion mechanism with two rotary encoders is presented as the master manipulator to transmit the motion information, which can take full advantage of natural manipulation skills for surgeons. The performance of bilateral operation is evaluated by experiments. The results illustrate that the transmission accuracy of axial and radial motion can meet the requirements of surgery. Fourthly, in order to improve the safe operation consciousness of surgeons, it is necessary for tip collision cues to be transmitted quickly to the operator in haptic cues except force feedback. The application of the master haptic interface based on magnetorheological (MR) fluids and the
III
high-precision force sensor makes the collision warning in haptic cues possible. The performance of collision warning in haptic cues is evaluated by the integrated system in the Endo Vascular Evaluator (EVE) model and the results demonstrate its effectiveness for reminding the surgeon of tip collision happened. Finally, to increase the operation dexterity and the success rate of the task in complex surgeries, two slave manipulators are implemented to realize the cooperative motion of a catheter and a guidewire. The performance evaluation experiments in vitro are performed by the EVE model. The results demonstrate that the proposed collaborative insertion has high dexterity and efficiency compared with no collaborative insertion. Thus, this research provides important insights into the development of ergonomic, safe and intelligent robotic catheter/guidewire operating systems incorporating effective real-time force feedback and haptic feedback for endovascular procedures.
V
Acknowledgements
First and foremost, I would like to express my sincere gratitude to my supervisor Professor Shuxiang Guo for his guidance and support throughout my Ph.D. studies. Besides the guidance of academic research, I would like to appreciate him for his great help and encouragement on my life. Meanwhile, I would like to express my thanks to vice-supervisor Professor Hideyuki Hirata and Professor Keisuke Suzuki for their precious advice in each year’s progress report and pre-defense meeting. I also would like to thank Professor Huadong Yu in Changchun University of Science and Technology for his academic advice and help in life.
I wish to thank all the members of our lab, Dr. Shuoxin Gu, Dr. Liang Zheng, Dr. Yu Song, Dr. Zixu Wang, Dr. Yi Liu, Dapeng Song, Wei Wei and Miao Yu, for the good memories of studying abroad. Discussions with them are of great help to the progress of my research. I also would like to thank Dr. Wenxiong Zhang in Kagawa University for his help in my life.
I would like to thank Kuraoka Shougakukai Foundation ((公財)
倉岡奨学会) in Japan for providing the scholarship, which makes me
has time to focus on my research.
At last, I would like to thank my parents and my father-in-law as well as my mother-in-law, because they provide me with strong
VI
spiritual and financial support while studying in Japan. For the most importantly, my profound gratitude and love go to my wife Shuoxin Gu. Your love, company, smile, support and encouragement give me confidence and perseverance to finish my studies. Without you, I could not imagine how I would spend this challenging learning career.
I sincerely wish my relatives, teachers, classmates and friends are
VII
Declaration
I hereby declare that this submission is my own work and that, to the best of my knowledge and belief, it contains no material previously published or written by another person nor material which to a substantial extent has been accepted for the award of any other degree or diploma of the university or other institute of higher learning, except where due acknowledgment has been made in the text.
IX
Table of Contents
Abstract ... I Acknowledgements ... V Declaration ... VII Table of Contents... IX Chapter 1 Introduction ... 1 1.1 Background ... 11.2 Current and Emerging Techniques for Endovascular Procedures 5 1.2.1 Endovascular Imaging and Navigation ... 5
1.2.2 Robot-assisted Operating Systems for Endovascular Procedures ... 7
1.3 Force Feedback and Haptic Feedback for Robotic Endovascular Procedures ... 11
1.3.1 Force Feedback in Robotic Endovascular Procedures ... 12
1.3.2 Haptic Feedback in Robotic Endovascular Procedures ... 14
1.4 Research Objectives ... 16
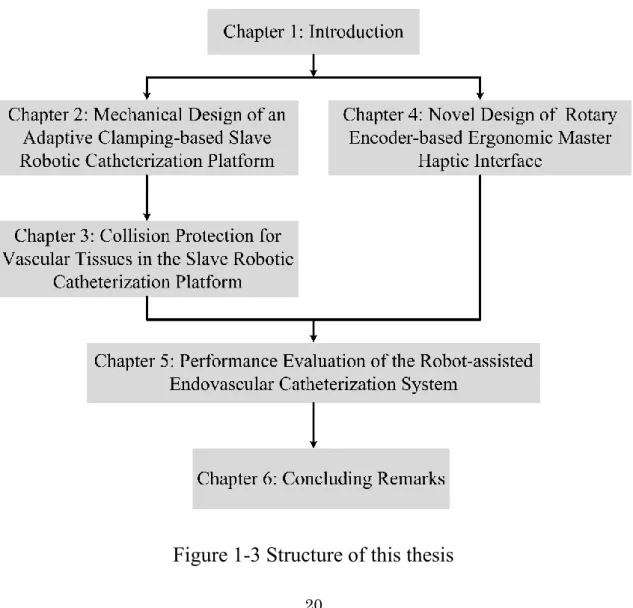
1.5 Thesis Overview ... 17
Chapter 2 Mechanical Design of an Adaptive Clamping-based Slave Robotic Catheterization Platform ... 21
Chapter 3 Collision Protection for Vascular Tissues in the Slave Robotic Catheterization Platform ... 23
X
Chapter 4 Novel Design of Rotary Encoder-based Ergonomic
Master Haptic Interface ... 27
Chapter 5 Performance Evaluation of the Robot-assisted Endovascular Catheterization System ... 31
Chapter 6 Concluding Remarks... 35
6.1 Contributions and Achievements ... 35
6.2 Future Research Directions ... 38
Publication List ... 41
1
Chapter 1
Introduction
1.1 Background
According to a report from the American Heart Association (AHA), cardiovascular and cerebrovascular diseases have become one of the three major causes (heart disease, stroke and vascular diseases) of death in human beings. Even in developed countries, the number of deaths from cardiovascular diseases is still up to 34% each year, which is a serious threat to human health [1]. Historically, these diseases have been addressed exclusively by vascular surgeons through open surgeries. Until 1963, the field of interventional radiology which was first proposed by pioneers such as Dr. Charles Dotter through advancements in medical imaging and catheter technology laid a solid foundation for the development of endovascular procedures [2].
Endovascular interventional procedure is performed with the help of imaging technologies (most commonly X-ray 2D fluoroscopy) for diagnosis and treatment of abnormalities inside blood vessels [3]. During this procedure, the catheters and guidewires are manipulated to access a lesion target followed the human vascular vessels from the small incisions in the neck, arm or groin area. The surgeon achieves
2
Figure 1-1 Endovascular procedures and tool manipulation [4-7] this operation through the combination of insertion, retraction, and twisting at the proximal end of the tools in different directions based on the real-time image data. This process of endovascular therapy is presented in Figure 1-1.
After more than fifty years of development, endovascular procedures have played a significant role in the diagnosis (angiography) and treatment (percutaneous transluminal angioplasty, stent graft insertion and catheter ablation) of vascular diseases, because of the smaller incisions, quicker recovery and fewer
3
complications [8]. The visualization and safe manipulation of the catheters and guidewires by using the medical imaging equipment (most commonly 2D fluoroscopy) make these procedures possible. Angiography is the most commonly used method to diagnose vascular diseases. It is the rapid injection of contrast agent into the heart or blood vessel through a catheter, so that the heart and blood vessel lumen can be developed under X-ray irradiation. The situation of blood flow containing contrast agent can be seen by the results of angiography, thus judging the pathological changes of the heart and blood vessels. The percutaneous transluminal angioplasty (PTA) is a technique for dilating and recanalizing atherosclerotic or other vascular stenosis or occlusive lesions by means of catheters and other instruments with an inflatable, annular balloon. For the endovascular treatment of aneurysmal diseases, following angiography the stent grafts (sheathed stents) are inserted and deployed by catheters over the length of the aneurysm to support blood vessel stenosis and keep blood flow unobstructed, thus relieving the blood pressures on the weak aneurysm wall. Data on endovascular repair of abdominal aortic aneurysm show that the overall technical success rate is greater than 90% [9]. For cardiac arrhythmias, especially with rapid rhythms, including atrial fibrillation and atrial flutter, the catheter ablation is a common and effective treatment method. It applies the high temperature generated by radiofrequency, ultrasound, or laser energy
4
standard approach is to use catheterization techniques to diagnose the electrical activities of the heart, determine the location and path of an arrhythmia, and then adopt the catheter ablation to treat the rapid rhythm [10]. As such, the field of endovascular procedure continues to be one of the most revolutionary and effective treatment methods for vascular diseases [11].
Nonetheless, several potential clinical challenges also have been introduced in. Firstly, the visualization guidance is achieved by using X-ray fluoroscopy, thus long term and repeated exposure radiations to X-ray cause occupational hazards to the surgeon like cancers and cataracts [12-14]. Even though he/she has already put on protective apparel (lead aprons), the face and hands can not be completely covered. Moreover, the heavy protective apparel with long standing hours can cause surgeon's fatigue as well as neck and back pain [14]. Secondly, the actions of the surgeon are conventionally guided by using 2D fluoroscopic images, hence some significant information on the 3D vascular anatomy is lost to the surgeons. Thirdly, the experienced surgeons sense the small axial forces by the fingertips during the endovascular catheterization, but for the novices, inadequate force feedback while operating surgical tools (catheter and guidewire) elevate the risk of endovascular procedures [15]. Fourthly, Surgeons often rely on visualization to avoid major vascular collision in the endovascular procedures. It is difficult to determine whether a vascular collision occurs, due to the absence of depth perception and
5
low definition of the fluoroscopic images [16].
As a result, numerous research and commercial organizations have turned towards robot-assisted technologies to improve the current state of endovascular procedures and more recently the imaging and navigation with computer-assisted interventions are achieved to provide pre-operative diagnosis and intra-operative guidance for endovascular procedures.
1.2 Current and Emerging Techniques for
Endovascular Procedures
In recent few decades, a number of research and commercial robot-assisted catheter operating systems were developed to address the clinical challenges of manual operation for endovascular procedures. In addition, more advanced imaging and navigation systems have also been developed to provide the critical information of the live 3D anatomy while reducing large doses X-ray radiation to the patient as well as the clinicians. The systems used in clinical trials have showed the notable advantages which include reduced X-ray fluoroscopy [17-19], less radiation exposure to patients and surgeons as well as improved stability and precision [20-22].
1.2.1 Endovascular Imaging and Navigation
Endovascular procedures are commonly performed by the surgeon with the help of fluoroscopic dyes and X-ray imaging. The
6
imaging devices can guide a tool which is operated by the surgeon to the lesion location by the visual feedback. However, some critical information of the live 3D anatomy will be lost if the intra-operative guidance relies on the 2D angiography. Motivate by such consideration, numerous vascular imaging methods are proposed, such as computed tomography angiography (CTA), Optical Coherence Tomography (OCT), intravascular ultrasound (IVUS) and intracardiac echocardiography (ICE), as well as magnetic resonance (MR) imaging techniques [23].
CTA is one of the pre-operative techniques used in recent years, which can reconstruct the fault plane image with computer 3D technology. Integration of these re-created 3D radiological medical images into intervention can help diagnose and evaluate blood vessel diseases or related conditions, such as aneurysms or blockages [24]. OCT as an emerging imaging modality is used to diagnose plaque within the coronary through the high-resolution in vivo images of coronary arteries and deployed stents [25-26]. IVUS is another modality using a special catheter to evaluate the morphology of vessel wall and determine both plaque volume in the coronary arteries and the degree of arterial stenosis, especially for angiographic imaging which is considered unreliable [27]. ICE is another promising imaging modality able to provide real-time visualization with high-resolution for cardiac structures, monitoring of radiofrequency energy delivery during ablation and catheter location, recognition of procedural
7
complications including pericardial effusion or thrombus formation [28-29]. Another technique for providing high-resolution images to visualize soft tissue features is MR angiography [30]. MR imaging techniques have shown the potential advantages in recent years for cardiovascular imaging, such as improved soft tissue contrast, reduced contrast agent injection and no X-ray radiation. However, most catheters and catheter operating systems in MR environment need to be made of non-magnetic materials and non-conductive components, which limits the wide application of this technology for intra-operative guidance of cardiac interventions [31]. Currently, the catheter robotic manipulator suitable for MR environment has been developed [32]. In the near future, MR imaging techniques will become the indispensable imaging and navigation system for endovascular procedures.
1.2.2
Robot-assisted
Operating
Systems
for
Endovascular Procedures
The major commercial robotic catheterization systems currently used in clinical practice, as shown in Figure 1-2, are four systems
including AmigoTM remote catheter system, Stereotaxis Epoch®,
8
Figure 1-2 (a) AmigoTM remote cathetersystem (Catheter Robotics Inc.,
NJ, USA) [33], (b) Stereotaxis Epoch® (Stereotaxis Inc., MO, USA)
[34], (c) MagellanTM robotic system (Hansen Medical Inc., CA, USA)
[35], (d) CorPath®200 robotic system (Corindus Vascular Robotics, MA, USA) [36].
The Amigo TM remote catheter system (Catheter Robotics, Inc.,
NJ, USA) can position the mapping catheter into the right atrium and ventricle. The navigation of the catheter is performed by a wired hand-held controller with four elements including rotation, catheter tip deflection, advance and withdraw. The performance and safety of the system are evaluated by the clinical trials [37]. Stereotaxis Epoch® (Stereotaxis Inc., MO, USA) is the one of main commercial robotic
9
system for electrophysiology applications. The system uses a magnetic field to navigate the specialized catheters and guidewires, and the tip orientation and linear position can be realized by a combination of a joystick, roller wheels and a mouse [38]. The MagellanTM robotic
system (Hansen Medical Inc., CA, USA) is geared towards cannulation of peripheral vascular vessels. After validating versus manual catheterization [39], the system has been successfully used for fenestrated endovascular aneurysm repair [40], treatment of iliac and femoral artery lesions [41], as well as uterine artery embolization [42]. The CorPath® 200 robotic system (Corindus Vascular Robotics, MA, USA) is another remote-controlled robotic system to address some procedural challenges and enhance the degree of precision and control for endovascular procedures. The robotic system can synchronously operate guidewires and stent/balloon catheters by using the joysticks or touch screen buttons for percutaneous coronary intervention (PCI) [43-44]. After validating its performance by clinical trials [43], the robotic system is licensed by the United States’ Food and Drug Administration (FDA) in 2012.
Researchers at institutes and universities around the world have also developed numerous other devices and have contributed a lot of work to improve the technology for endovascular procedures. Thakur et al. proposed a novel remote catheter navigation system, which can reduce the physical stress and irradiation to operators under the X-ray 2D fluoroscopy for image guidance. And it had the ability to sense and
10
replicate motion within 1 mm and 1° in the axial and radial directions, respectively [45]. Guo et al. proposed a novel master-slave robotic catheter operating system to train the unskilled surgeons to perform the vascular interventional surgery with visual feedback [46]. The evaluation of dynamic and static performance and the synchronization for the robot-assisted catheter system were conducted by [47]. Tavallaei et al. developed a novel remote catheter navigation system with 3 degrees of freedom (DoFs), which allowed the interventionalist to remotely steer a conventional catheter from a safety place. The system evaluation was performed ex vivo and the safety of the system was demonstrated by the in vivo experiments [48]. More recently, an assembly-type, low cost and easy human interface catheter driving system with 4 DoFs was proposed to reduce radiation exposure. The performance of bilateral control was evaluated by the optical tracking experiments [49]. Bao et al. proposed a remote-controlled vascular interventional robot based on an electromagnetic clutch to perform the catheter insertion. Also, two identical slave manipulators were in series to achieve the coordinated movement of the catheter and guide wire [50]. Furthermore, the operation evaluation in-human of this proposed system was performed [22].
Currently, the virtual reality (VR)-based technology as a potential method was equipped with robot-assisted catheter systems [51-53]. The vasculature [54-55] and catheter [56-57] models can be built by the VR simulator and the visual images of surgical region can be
11
displayed in the meantime. For the sake of improving the skill of catheter manipulation for novices, Wang et al. developed a training system integrated cooperation of VR simulator and haptic device to train the surgeon and improved the coordination of surgeon’s eye-hand [53]. These robotic systems can drastically reduce radiation exposure and improve the stability of catheter operation by replacing human effort for high radiation exposure procedures. However, surgeons have to face several challenges to advance the catheter in the complicated and delicate vascular structure of human beings, especially under the fragile and tortuous blood vessels. It has been reported that the tortuosity of vessels is one of the main failure reasons in endovascular procedures [58].
Therefore, it is extremely urgent to apply the force sensing for robotic catheter systems to provide the surgeons with haptic cues during endovascular procedures because excessive forces could rupture the blood vessel walls and result in bleeding.
1.3 Force Feedback and Haptic Feedback for
Robotic Endovascular Procedures
In manual endovascular interventional procedures, the experienced surgeon can achieve the haptic cues of catheter-tissue through sensing the small axial forces and torques at the fingertips while operating the surgical tools (catheters and guidewires) access different arteries of the patient. The risk of vascular perforation in the
12
tortuosity can be reduced through a combination of insertion, retraction, and rotation at the proximal end of the tools in different directions under the help of real-time image data. However, in robotic endovascular procedures, surgeons can not directly operate tools, and can not obtain haptic information. It is difficult to determine whether a vascular collision occurs in the bending regions of vessels, relying solely on visual assistance [16]. Thus, the application of force/torque sensing devices is extremely critical for tele-operated robotic catheter systems to remind surgeons to adjust the direction of surgical tools in time when the catheter tip collides with the vessel wall.
1.3.1 Force Feedback in Robotic Endovascular
Procedures
To reflect the force information between the catheter and the vessel walls more intuitively during the operation, some researchers have implemented all kinds of the force measuring devices for robot-assisted catheter systems to generate force feedback to avoid vessel puncture caused by excessive forces at the catheter tip, or to maintain a suitable contact force between the ablation catheter tip and the myocardial wall for cardiac ablation procedures. Fiber-optic based sensors have been applied on the catheter tip to provide force feedback to the operator [59-60]. The potential of this technology has been demonstrated by the clinical studies [61-62]. Fu et al. embedded four micro force sensors (FSS1500NS, Honeywell) into the active
13
wheel in a master-slave catheterization system to obtain the advancing force assisted surgeons to operate the catheter under the 3D guiding image [63]. Due to the high sensitivity of the strain gauge, it has been used to measure the force information. J. Payne et al. designed a novel master-slave force feedback system by using two strain gauges close to the tip on opposite sides of the catheter and two micro force sensors (FSS1500NS, Honeywell) on the master actuator, and it reduced the magnitude and duration of contact forces exerted on the vessel walls according to the force feedback during a simulated endovascular procedure [16]. To get the force information directly without any mechanical transmission, a compact, cost-effective force-sensing device based on strain gauges was placed at the front end of the slave manipulator, thus increasing the accuracy of force measurement [64-66]. Commercialized force sensors, especially those (ATI Nano 17 sensor, ATI Industrial Automation, Inc.) with multi-directional measurements, have been widely used in catheter systems to provide force feedback. A force transducer (TEAC, TU-UJ, Japan) was adopted in a novel master-slave robotic catheter operating system to detect the force signals in the axial direction to train the unskilled surgeons to perform the vascular interventional surgery with force feedback and visual feedback [22], [46], [50], [67-71].
14
1.3.2 Haptic Feedback in Robotic Endovascular
Procedures
The haptic cues of the fingers refer to a force perception that the object returns to the person when the fingers touch the object. It is very important for the surgeons to judge the interaction of the tool and vascular tissues during endovascular procedures. In conventional endovascular intervention, surgeons can obtain the haptic cues by directly manipulating the surgical tools. However, the haptic cues are missing in robotic endovascular procedures, which increases the risk of vascular perforation during surgeries. With such consideration, numerous robotic catheter operating systems have been proposed with the commercialized haptic devices to provide haptic feedback that would be felt by the operator [22], [49-50]. Despite the increased use of robotic systems, the most existing commercial haptic devices are joysticks or phantom controllers without considering natural manipulation techniques practiced by surgeons. As a result, researchers are moving towards the development of haptic interfaces that conform to the experience-related skills of surgeons.
In recent years, some haptic devices based on intelligent materials have been utilized to increase the effectiveness of human-machine interfaces. The magnetorheological (MR) fluids is the most typical representative because of high permeability and low hysteresis. Its applications in haptic and force feedback devices have
15
been reported in the literature [72-73]. In these studies, haptic systems with MR fluids in the operation side were proposed to acquire tactile sensation for telerobotic surgery. Enlightenment based on the above application, in combination with the characteristics of the MR fluids in a magnetic field and the haptic desire of the robot-assisted catheter system, the haptic interface as the master manipulator which can provide immersive operation was developed. The interface can provide the haptic sensation generated by the resistance force which is determined by the viscosity of MR fluids [67], [74-78]. In addition, the motor-based haptic feedback has also seen significant advances in recent years [15], [49].
These systems offer potential advantages including reduced radiation exposure, increased precision and stability of actions, accurate force feedback and immersive haptic feedback. Nevertheless, up to now, the collision trauma during the catheterization remains unresolved, despite of the visual assistance. The fragile vessels (especially cerebral vessels) have the risk to be penetrated by the catheter tip when the collision occurs, because the novices have little experience to adjust the catheter manipulation rapidly. Motivated by such consideration, it is extremely urgent for tele-operated robotic catheter systems to provide patients with collision protection during endovascular catheterization procedures.
16
1.4 Research Objectives
Numerous studies have shown that the experienced surgeons with consummate manipulation skills and dexterous manipulation strategies are the critical factors for successful clinical outcomes. This highlights the importance of incorporating natural manipulation skills for the rising robot-assisted endovascular intervention systems, and further provides important insights into the design of compact and ergonomic robotic catheter systems incorporating conventional manipulation skills. Furthermore, the collaborative insertion of the catheter and the guidewire learned from conventional endovascular catheterization needs to be considered to achieve the complex procedures, the single operation fails to meet surgical requirements because of low dexterity [50], [79]. In addition, one of the main reasons for the failure of endovascular procedures is the blood vessel perforation caused by excessive forces which is one of the main challenges during endovascular procedures, especially for the tortuosity of vessels [58]. To enhance the safety of endovascular procedures assisted by the robotic systems, it is necessary to provide advanced collision warning in the master side which can remind the operator of tip collision and to embed critical collision protection mechanism in the slave side which can alleviate the collision trauma to vascular tissues.
The research purposes and approaches of this thesis are as follows:
17
1) Design a novel type of slave manipulator with high-precision force sensor for realizing accurate force feedback, as well as providing stable, adaptive, lossless clamping for catheters and guidewires.
2) Add the collision protection function in the slave manipulator to quickly release the catheter or the guidewire to alleviate the further collision trauma by using a flexible clamping mechanism, thus improving the safety operation of catheterization.
3) Propose a motion input device based on pinion and rack mechanism with two rotary encoders as the master manipulator that take full advantage of natural catheterization skills. The application of the haptic interface based on magnetorheological (MR) fluid incorporating the high-precision force sensor makes the effective collision warning in haptic cues possible.
4) The collaborative motion of a catheter and a guide wire will be realized by implementing two slave manipulators, thus increasing the operation dexterity and the success rate of the task in complex surgeries.
1.5 Thesis Overview
The outline of this thesis is as follows:
Chapter 2 presents a tapered collet-based adaptive clamping structure in the novel salve manipulator which can realize stable, adaptive, lossless clamping for catheters and guidewires. A
18
high-precision force sensor is integrated into the proposed slave manipulator to provide the accurate force feedback which can augments the surgeon’s judgement and actions during the robot-assisted endovascular procedures.
Chapter 3 proposes an electromagnetic braking-based collision protection mechanism in the novel slave manipulator to improve the safety operation of catheterization. The mechanism can alleviate the further collision trauma for blood vessels by quickly releasing the catheter or the guidewire when the measured force is greater than the setting threshold value which is determined by the characteristics of the vascular tissues.
Chapter 4 employs the pinion and rack mechanism with two high-precision rotary encoders as the ergonomic motion input device to take full advantage of natural manipulation skills. Furthermore, the collision warning in haptic cues is realized by the application of the haptic interface based on magnetorheological (MR) fluids in the master side.
Chapter 5 evaluates the performance of the robot-assisted endovascular catheterization system including bilateral operation, collision warning in haptic cues and collaborative motion of the catheter and the guidewire. Furthermore, the latter two items are evaluated in combination with in vitro experiments using Endo Vascular Evaluator (EVE) model.
19
Chapter 6 summarizes the main research results and contributions of the thesis and addresses the future work towards user feedback study by surgeons, and studies with animals leading to clinical trials of robot-assisted endovascular catheterization technologies.
The major contributions of this thesis:
Designing a novel clamping structure to realize the stable, lossless and adaptive clamping for the catheters and guidewires with different diameters.
Proposing a novel proximal force sensing platform based on high-precision force sensor to generate accurate force feedback to the operator.
Developing an electromagnetic braking-based collision protection mechanism in the slave manipulator to alleviate the further collision trauma for blood vessels, thus improving the safety of surgeries and reducing the psychological pressure of the operator.
Providing design insights for future development of
ergonomic robot-assisted catheterization systems
20 operators.
Validating the performance of collision warning in haptic cues which is realized by the application of the haptic interface based on magnetorheological (MR) fluids in the master side.
Demonstrating the potential advantages of collaborative
motion of the catheter and the guidewire by using robotic catheterization systems incorporating different performance metrics.
21
Chapter 2
Mechanical Design of an
Adaptive Clamping-based
Slave Robotic Catheterization
Platform
This chapter proposes a slave robotic catheterization platform based on adaptive clamping mechanism which can stably clamp the catheters or guidewires for different diameters. The proposed electromagnetic braking mechanism can realize the regulation of catheter clamping force by controlling the current, thus preventing the catheter from being damaged by excessive clamping force. Furthermore, the salve robotic platform incorporates a proximal force measuring unit without radial motion interference to achieve the accurate measurement of forces exerted on the vasculature and thereby providing important guidance for the actions of surgical tools manipulated by robotic platform. The performance evaluation for proximal force measuring unit is performed by experiments including
22
zeroing performance evaluation, step response evaluation and dynamic measurement evaluation, which has an important influence on the safety of surgeries. From the results, the hysteresis for force measurement is generated. An average value of 8.89mN for step response and a maximum value of 48.58mN for dynamic measurement are shown in Figure 2-10 and Figure 2-14, respectively. Such small hysteresis for the tolerance of human blood vessels can be accepted [95-96]. The results for evaluation experiments demonstrate the feasibility of the proposed force measuring unit due to its high stability and low hysteresis, as well as prove the potential of such a unit in realizing the accurate force feedback of robot-assisted catheterization systems. Furthermore, the design provides significant insights into the development of safe and reliable robot-assisted catheter systems while incorporating high precision and high stability force sensing platforms.
23
Chapter 3
Collision Protection for
Vascular Tissues in the Slave
Robotic Catheterization
Platform
Endovascular robotic technology is an effective and revolutionary method to reduce X-ray radiation and fatigue of a surgeon for endovascular catheterization. It can also improve the effectiveness of the procedure by precise positioning of the catheter and the force information. Nevertheless, few designs have taken the collision protection of the vessel walls and the catheter tip into account.
Therefore, in this paper, a novel robot-assisted catheter system with CPM was proposed. The collision protection threshold can be adjusted by the current. The CPM is based on electromagnetic braking to realize the vascular tissue protection. Once the measuring force exceeds the protection threshold which can be adjusted by the current,
24
the catheter will be released quickly. The relationship between the threshold value and the current, shown in Figure 3-4, was obtained by the experiment. Moreover, the performance evaluation experiments of the collision protection for the robot-assisted catheter system have been carried out. Figure 3-6 (a), (b) and (c) showed the evaluation results of the collision protection mechanism when the protection threshold was set as 0.38N, 0.61N and 0.75N, respectively. Although there was an error (shown in Figure 3-8) between the triggering force and the protection threshold, it was still within the threshold of safety operation. That suggests the CPM has taken effect to a certain extent for the tissue protection. And the stability of the collision protection mechanism had been verified as show in Figure 3-7. In the actual procedure, the collision protection threshold needs to be adjusted in real time, because a catheter sometimes passes through several curved areas and reaches the lesion area. Figure 3-10 displayed the experimental results for the real-time adjustment in a vascular model. The effectiveness of the real-time adjustment was summarized in Table 3.1. The further performance evaluation was performed in terms of success rate and elapsed time. And the results were shown in Figure 3-11 and Figure 3-12, respectively. Based on the results of these evaluation experiments, the CPM equipped the robot-assisted catheter system has made great contribution to remit the collision trauma. It can effectively improve the security of operation during the endovascular catheterization.
25
In the previous researches, some researchers tried to avoid the tip collision by simulation to plan the insertion path of the catheter [56-57]. And others contributed to robot-assisted catheter systems. Yin et al. [76] proposed a haptic interface based on MR fluid, which can dynamically amplify the collision force information as the alarm to remind the surgeon to retract or rotate the catheter. Also, the research on the visualization and haptic force equipped robot-assisted catheter system had been developed [53]. It took VR simulator and haptic interface to help the novice realize safety operation of a catheter. The directive notification module (DNM) will determine whether the catheter tip is in a safety operation area by the collision detection algorithm. And the signs (safe, warning or dangerous) will be transmitted to the operator by the form of tactile sensation. Although the vision and touch enable the operator to reduce collision frequency, they don’t avoid the risk of collision perforation. In view of this, Wang et al. [97] proposed a speed adjustable mechanism (SAM) on the basis of the previous training system. This mechanism adopts the principle of continuously variable transmission (CVT) to adjust the insertion speed of a catheter at the master side of the training system. And the evaluation results show that the collision frequency is greatly decreased. The goal of these previous studies is to alert the operator to do the response when a collision has occurred or is imminent. However, the operators sometimes could not respond fast enough to deal with such situations. According to the experimental results, the
26
proposed device in this research is capable of tissue protection and prevents vascular perforation, even if the operator does not take enough fast protection action.
Despite the promising results, it is important to note that the study is limited by the fact that the experiments of an in vitro were used to conduct the performance evaluation of the collision protection; the limitation is manifested in two ways. Firstly, the glass vascular model has great rigidity and can not produce vascular deformation when the catheter tip collides with the model. In addition, the curvature of the bend can not be changed during the catheterization, which will lead to the increasing of the contact area between the wall of the catheter and the wall of the model, thereby increasing the friction. Secondly, in this research, the viscous resistance of the blood is neglected, and it is an important component of the measuring force during the actual operation. And the friction between the catheter and the blood vessel also increases because of the lack of blood lubrication. Therefore, the direction for future research is to perform experiments
in vivo or with artificial vascular models which are more similar to the
27
Chapter 4
Novel Design of Rotary
Encoder-based Ergonomic
Master Haptic Interface
Numerous endovascular robotic systems have been successfully developed and demonstrated to perform various stages of studies with phantom, animal and clinical trials [15]. However, most of these systems have been designed with little consideration of operator behavioural patterns, thereby not fully taking advantage of natural manipulation skills which are obtained through practice and experience [90], [100]. In addition, the collision during the endovascular procedures leading to vascular injury or even perforation has been a concern of surgeons. Despite the growing interest of endovascular robotic systems in the safety of catheterization, these systems have mostly focused on force feedback [59-71] and haptic feedback [15], [67], [74-76]. They are very useful and have important guiding significance for experienced surgeons to make correct judgments. However, for novices, their contributions are diminished
28
because novices do not respond quickly enough and are not sensitive enough to haptic changes as well as lack of experience [100]. Thus, it is very essential to provide the obvious collision warning to decrease the further collision trauma and avoid vessel puncture effectively, especially for novices.
In this chapter, an ergonomic master haptic interface is designed to transmit conventional gestures of a surgeon while operating a surgical tool.
The rack and pinion mechanism with two rotary encoders is used as the motion input device to transmit and feedback the motion information, which can take full advantage of natural manipulation skills. The application of the master haptic interface based on magnetorheological (MR) fluids and high-precision force sensor makes the obvious collision warning in haptic cues possible. To verify the validity of collision warning in haptic cues, the magnitude of haptic force is quantitatively evaluated by the experiment. The results show that the change of haptic force is much greater than the human’s finger detection resolution [106]. Therefore, it can clearly remind the operator of collision, even for novices. In addition, during the endovascular procedure, as the catheter or guidewire inserts, the friction resistance it suffers will also increase, and different safety thresholds will correspond to different bending areas. Therefore, a threshold adjustment device in real-time is integrated into the master haptic interface to adjust the threshold for collision warning according
29
to the surgeon's experience combined with vascular characteristics, thus enhancing the safe operation for robot-assisted endovascular intervention. The design of the proposed master haptic interface provides significant insights for the future development of ergonomically optimized endovascular robotic systems incorporating force feedback, haptic feedback and collision warning, whilst taking full advantage of natural manipulation skills of the operators for endovascular procedures.
31
Chapter 5
Performance Evaluation of the
Robot-assisted Endovascular
Catheterization System
The endovascular procedure which is performed with the help of
imaging technologies like X-ray, CT scan [113], etc. is the effective and revolutionary technology to diagnose and treat vascular diseases. Nevertheless, for surgeons, long-term exposure to X-ray radiation and fatigue have been the potential occupational hazard. Therefore, a tele-operated endovascular robotic system is a solution to these challenges.
In the present work, a robot-assisted catheter/guidewire system with collision warning was proposed. It can augment a surgeon’s actions using conventional surgical tools, as well as generate force feedback to ensure the safety during the procedure. The precise positioning of the catheter/guidewire is the primary requirement for an endovascular robotic system. The experimental results of bilateral operation shown from Figure 5-3 to Figure 5-6 indicate that the
32
maximum absolute transmission error in axial and radial directions are 0.79mm and 1.7°, respectively. The transmission accuracy of axial and radial motion can meet the requirements of surgery. Tip collision is the main cause of vascular perforation. Thus, the collision warning in endovascular procedures is very necessary. In our proposed system, the haptic interface was adopted to remind surgeons of the tip collision in haptic cues. The evaluation results were shown in Figure 5-9. In mode 1, the measured force can be reduced obviously. The reason is that when the collision occurs, the haptic device produces the amplified resistance to remind the surgeon, at the same time, it will hinder the surgeon's further insertion, thus controlling the further increase of the collision force, and providing convenience for the surgeon to adjust the direction of the catheter in time. Validation trials were performed with 10 different subjects (non-medical) and the results for the average maximum force and the average elapsed time were summarized in Figure 5-10 and Figure 5-11. They indicate that the realization of relatively safe operation during endovascular catheterization by using the proposed system.
In the previous researches, some researchers tried to avoid the tip collision by simulation to plan the insertion path of the catheter [56-57]. Wang et al. [53] combined VR simulator with a haptic interface to help the novice realize safety operation. The collision detection algorithm was used to determine whether the catheter tip is in a safe operation area. Although the vision and touch can train the
33
operator to reduce collision frequency, they do not avoid the risk of collision perforation. In view of this, Wang et al. [97] proposed a speed adjustable mechanism (SAM) based on the principle of continuously variable transmission (CVT) in the master side to adjust the insertion speed of a catheter. The goal of these previous studies is to alert the operator to do the response when a collision has occurred or is imminent. However, the sensitivity of reaction force and reaction speed of operation for each operator are different. Therefore, it is necessary to amplify force awareness when a collision happens. According to the experimental results, the proposed system combined the high-precision force sensor with the haptic device in this research is capable of tissue protection and prevents vascular perforation.
Additionally, in some complex cerebrovascular procedures, the dexterity of the guidewire is reduced due to long-distance guidance, which leads to prolonged operation time and inaccurate location. For this reason, the guidewire and the catheter need to cooperate with each other. In this chapter, the performance evaluation for collaborative motion of a catheter and a guidewire by using two manipulators with a certain angle was conducted. The two metrics, success rate of the task and the average elapsed time of the task accomplishment are summarized in Figure 5-15 and Figure 5-16, respectively. The results indicate the proposed scheme of collaborative insertion has high dexterity and efficiency.
34
is limited by the fact that the experiments of an in vitro were used to conduct the performance evaluation of the collision warning; the limitation is manifested in two ways. Firstly, vascular tissues in the Endo Vascular Evaluator (EVE) simulates the condition of a healthy person's blood vessels. In real surgery, the characteristics of each patient's blood vessels vary depending on the condition and physical quality of the patients. Secondly, in this research, the threshold value of collision warning for the EVE model is set to 1N. However, in real surgery, the threshold for different vasculature areas is different and it needs to be adjusted in real time according to the judgement of experienced surgeons. For the collaborative motion, when the guidewire is coupled with the catheter through the Y-type connector, the friction force it receives will increase due to the existence of the angle between the guide wire and the catheter. Therefore, the direction for future research is to perform experiments in vitro with real blood or in vivo with animals to evaluate the performance of the endovascular robotic system. Furthermore, the more reasonable scheme of collaborative motion of the guidewire and the catheter need to be designed and demonstrated for the complex endovascular procedures.
35
Chapter 6
Concluding Remarks
6.1 Contributions and Achievements
With the rapid development of medical technologies, endovascular techniques, due to its smaller incisions, quicker recovery and fewer complications, has become the common practice for diagnosing and treating various cardiac and vascular diseases in recent decades. Nonetheless, some potential challenges also have been introduced including X-ray radiation, limited 3D imaging, lack of contact force sensing and haptic feedback from the conventional surgical tools. Numerous research and commercial robot-assisted catheter operating systems were developed to address the clinical challenges of manual operation for endovascular procedures. Previous studies have demonstrated the potential of these robotic systems in reducing radiation exposure and improving the stability of catheter operation by replacing human effort for high radiation exposure procedures. However, current endovascular robotic systems have been designed without considering several important themes including the natural manipulation skills for surgeons, collision protection for vascular tissues and obvious collision warning for operators
36
(especially for novices) as well as low operation dexterity in long-distance guidance with the single guidewire or catheter. Motivate by such consideration, the research presented in this thesis proposes the robot-assisted endovascular catheterization system for taking full advantage of natural manipulation skills, providing collision protection for vascular tissues and palpable collision warning for operators as well as investigating the advantages of collaborative motion for a specialized catheter and a matching guidewire.
The slave robotic catheterization platform is presented in Chapter 2, which can provide the stable, adaptive, lossless clamping for catheters and guidewires by using a tapered collet-based adaptive clamping structure. A high-precision force sensor is integrated into the proposed slave manipulator to provide the accurate force feedback. By evaluating different performance metrics, the results demonstrate the potential of the platform towards adaptive clamping for catheters/guidewires with different diameters and achievement of accurate force feedback which can augments the surgeon’s judgement and actions during the robot-assisted endovascular procedures.
An electromagnetic braking-based collision protection mechanism is proposed in Chapter 3, based on extending clamping structure in Chapter 2. Once the measuring force exceeds the protection threshold which can be adjusted by the current, the catheter will be released quickly. And the relationship between the threshold value and the current has been obtained by the experiment. Moreover, the
37
performance evaluation experiments of the collision protection for the proposed mechanism have been carried out. Based on the results of these evaluation experiments, the collision protection mechanism has made great contribution to alleviate the further collision trauma for blood vessels by quickly releasing the catheter or the guidewire. The mechanism provides important insights into the design of safe and reliable robot-assisted catheter systems that effectively improve the security of operation during the endovascular catheterization.
Chapter 4 employs the pinion and rack mechanism with two high-precision rotary encoders as the ergonomic motion input device to take full advantage of natural manipulation skills. A magnetorheological (MR) fluids-based haptic interface is used in combination with the proposed motion input device to achieve the elimination of tremor. Furthermore, the palpable collision warning in haptic cues is realized by the application of the haptic interface in the master side. The design of the proposed master haptic interface provides some insights for the future development of ergonomically optimized endovascular robotic systems incorporating force feedback, haptic feedback and collision warning, as well as skilled motion patterns.
The performance evaluation, including bilateral operation, collision warning in haptic cues and collaborative motion, for the proposed robot-assisted endovascular catheterization system is performed in Chapter 5, by using the slave robotic platform presented
38
in Chapter 2 and the ergonomic master haptic interface introduced in Chapter 4. Furthermore, the latter two items are evaluated in combination with in vitro experiments using Endo Vascular Evaluator (EVE) model. By evaluating different performance metrics, the results indicate the feasibility of augmenting the surgeon's actions, the advantages of collision warning in haptic cues and the collaborative motion for a catheter and a guidewire. The use of EVE model provides further significant insights into the initial assessment and evaluation of endovascular robotic systems because it has the artificial internal environment which is more similar to the real one.
6.2 Future Research Directions
Despite the growing interest and increased use of robot-assisted operating systems for endovascular intervention procedures, the distal-force sensing in the tip of catheters or guidewires as well as side forces is still a potential challenge at the present, particularly for peripheral vascular procedures. Therefore, for widespread use of robot-assisted endovascular catheterization systems, the development of intelligence and high-precision robotic catheter/guidewire operating system incorporating natural manipulation skills, haptic feedback and tip force sensing is a potential area for future research.
Additionally, the results presented in Chapter 3 and Chapter 5 validate the feasibility of the proposed collision protection mechanism at the slave side and advanced collision warning in haptic cues at the
39
master side. While the studies were conducted on in vitro phantoms, the future researches with animals leading to clinical trials are encouraged to provide real tool-tissue interactions. This can provide significant insights into evaluating the safety of robotic endovascular procedures through the actual collision protection threshold and collision warning threshold which are determined by the applied forces relating to the risk of tissue damage.
41
Publication List
International Journal Papers
1. Linshuai Zhang, Shuxiang Guo, Huadong Yu, Yu Song, Takashi Tamiya, Hideyuki Hirata, Hidenori Ishihara, “Design and performance evaluation of collision protection-based safety operation for a haptic robot-assisted catheter operating system,” Biomedical Microdevices, vol.20, no.2:22, 2018.
2. Linshuai Zhang, Shuxiang Guo, Huadong Yu, Yu Song, “Performance evaluation of a strain-gauge force sensor for a haptic
robot-assisted catheter operating system,” Microsystem
Technologies, vol.23, no.10, pp.5041-5050, 2017.
3. Yu Song, Shuxiang Guo, Xuanchun Yin, Linshuai Zhang, Hideyuki Hirata, Hidenori Ishihara, Takashi Tamiya, “Performance evaluation of a robot-assisted catheter operating system with haptic feedback,” Biomedical Microdevices, vol.20, no.2:50, 2018.
4. Yu Song, Shuxiang Guo, Xuanchun Yin, Linshuai Zhang, Yu Wang, Hideyuki Hirata and Hidenori Ishihara, “Design and Performance Evaluation of a Haptic Interface based on MR Fluids for Endovascular Tele-surgery”, Microsystem Technologies, vol.24, no.2, pp.909-918, 2018.
42
International Conference Papers
1. Linshuai Zhang, Shuxiang Guo, Huadong Yu, Yu Song, Dapeng Song, “Adaptive Clamping Mechanism-based a Novel Slave Manipulator for Endovascular Catheterization”, Proceedings of 2018 IEEE International Conference on Mechatronics and Automation, pp.2358-2363, 2018.
2. Linshuai Zhang, Shuxiang Guo, Huadong Yu, Yu Song, Dapeng Song, “Rotary Encoder-based Position Transmission and Feedback of a Novel Robotic Catheter System for Endovascular Catheterization”, Proceedings of 2018 IEEE International Conference on Information and Automation, pp.32-36, 2018.
3. Linshuai Zhang, Shuxiang Guo, Huadong Yu, Shuoxin Gu, Yu Song, Miao Yu, “Electromagnetic Braking-based Collision Protection of a Novel Catheter Manipulator”, Proceedings of 2017 IEEE International Conference on Mechatronics and Automation, pp.1726-1731, 2017.
4. Linshuai Zhang, Shuxiang Guo, Huadong Yu, Yu Song, “Design and Principle Analysis for Electromagnetic Brake Clamping Mechanism of a Novel Slave Manipulator”, Proceedings of 2016 IEEE International Conference on Mechatronics and Automation, pp.490-495, 2016.
43
5. Yu Song, Shuxiang Guo, Linshuai Zhang, “An Ergonomic Master
Haptic Interface for the Robot-assisted Endovascular
Catheterization System”, Proceedings of 2018 IEEE International Conference on Mechatronics and Automation, pp. 416-420, 2018. 6. Miao Yu, Shuxiang Guo, Yu Song, Linshuai Zhang, “The
Characteristics Evaluation of a VR Simulator-based Catheter Training System”, Proceedings of the 2018 13th World Congress on Intelligent Control and Automation, pp. 153-158, 2018.
7. Yu Song, Shuxiang Guo, Linshuai Zhang, Miao Yu, “Haptic Feedback in Robot-assisted Endovascular Catheterization”, Proceedings of 2017 IEEE International Conference on Mechatronics and Automation, pp. 404-409, 2017.
8. Shuxiang Guo, Miao Yu, Yu Song, Linshuai Zhang, “The Virtual Reality Simulator-based Catheter Training System with Haptic Feedback”, Proceedings of 2017 IEEE International Conference on Mechatronics and Automation, pp. 922-926, 2017.
9. Yu Song, Shuxiang Guo, Linshuai Zhang, Xuanchun Yin, “MR Fluid Interface of Endovascular Catheterization Based on Haptic Sensation”, Proceedings of 2016 International Conference on Mechatronics and Automation, pp. 542-546, 2016.
45
Biographic Sketch
Linshuai Zhang received his B.S. degree in Mechanical Design-Manufacture and Automation at Changchun University of Science and Technology, Jilin province, China, in 2011 and his M.S. degree in Mechanical Manufacturing and Automation at Changchun University of Science and Technology, Jilin province, China, in 2015. He is currently working toward the Ph.D. degree in Intelligent Mechanical Systems Engineering at the Kagawa University, Japan. His current research interests include mechanical engineering and endovascular robotic systems.
He has published over 6 refereed journal and conference papers in recent three years.
![Figure 1-1 Endovascular procedures and tool manipulation [4-7]](https://thumb-ap.123doks.com/thumbv2/123deta/5737694.1020679/14.892.119.734.159.674/figure-endovascular-procedures-tool-manipulation.webp)