経皮的内視鏡下椎間板ヘルニア摘出術(percutaneous
endoscopic lumbar discectomy
:PELD)には,椎間孔経
由(transforaminal:TF)と椎弓間経由がある.代表的な
アプローチである TF は,Kambin triangle(別名 safety
triangle
)を指標に内視鏡を刺入し,椎間孔を経由して脊
柱管内の硬膜腹側病変を観察し,病変を処置する.椎間
孔および,その周辺の微小解剖の知識と理解は手術適応
と成績を左右するために必要不可欠である.また,後外
側筋間(Wiltse)のアプローチや経椎間孔経由椎体間固
定(transforaminal lumbar interbody fusion:TLIF)の際
に必要となる Kambin triangle から椎間孔を構成する微
小解剖について,文献をレビューし概説する.
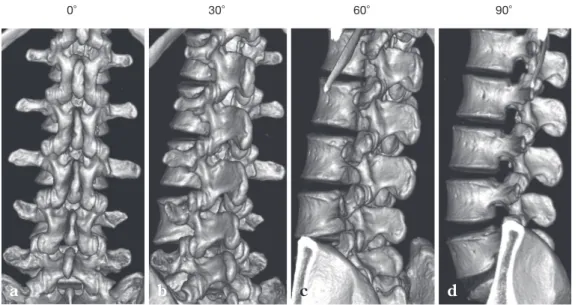
腰椎椎間孔はみる方向により,その孔形が異なる.正
常人の腰椎 3 次元 computed tomography(3D CT)画像
において椎間孔は背側からは確認できないが,外側に 30
度ずつ角度をずらしてみると徐々に開口し,90 度左外側
方向からで最大となる.L1/2 椎間孔の上位から L4/5 の
下位レベルに従い,徐々に広くなる.L5/S1 椎間孔は,
腸骨稜のため 60 度以上外側では確認できない(Fig. 1).
腰椎椎間孔は,楕円形で高さ 19.4 mm(平均値 15.5∼
24.2
),幅 8.8 mm(平均値 6.4∼12.3)で,L5/S1 椎間孔
はじめに
腰椎椎間孔と Kambin triangle
原 著
Original Article
Spinal Surgery 31(3)276 282,2017経椎間孔アプローチの際に必要となる椎間孔周囲の微小解剖
―文献レビュー―
Microsurgical Anatomy of the Lumbar Intervertebral Foramen for the
Minimally Invasive Spine Surgery―Review of the Literature―
内 門 久 明
*1服 部 剛 典
*2森 岡 基 浩
*2内 田 晋
*3Hisaaki Uchikado, M.D., Ph.D.*1, Gosuke Hattori, M.D., Ph.D.*2, Motohiro Morioka, M.D., Ph.D.*2, Shin Uchida, M.D., Ph.D.*3
Abstract
Percutaneous endoscopic lumbar discectomy(PELD)is a minimally invasive spinal technique.
PELD can be performed using the transforaminal(TF)or interlaminar(IL)approach. The TF approach
is a well-established modality in the treatment of patients with a herniated lumbar disc. This technique
makes the most of the space within the intervertebral foramen, where Kambin s triangle permits a safe
approach to the lesion.
Knowledge of the anatomy of the lumbar artery and its branches and the ligaments of the
interver-tebral foramen is necessary to perform successful surgery and avoid complications.
(Received:February 20, 2017;accepted:March 14, 2017)
Key words
lumbar intervertebral foramen, percutaneous endoscopic lumbar discectomy, microsurgical anatomy
*1 医療法人ニューロスパインうちかど脳神経外科クリニック/Uchikado Neuro Spine Clinic
連絡先:〒812 0893 福岡市博多区那珂 1 2 3 医療法人ニューロスパインうちかど脳神経外科クリニック 内門久明〔Address reprint requests to:Hisaaki Uchikado, M.D., Ph.D., Uchikado Neuro Spine Clinic, 1 2 3 Naka, Hakata ku, Fukuoka shi, Fukuoka 812 0893, Japan〕
で最大となる
1).
Kambin triangle は椎間板造影,神経根ブロックなどの
穿刺に際し,重要な透視の指標となる 3 次元的な直角三
角形である
2).別名 safety triangle とも呼ばれている.2
次元平面での Kambin triangle は底辺を下位椎体上縁終
板,高さは上関節突起の椎間孔側,上位の exiting nerve
root
を斜辺とした三角である
3)(Fig. 2).屍体での
Kam-bin triangle
の計測では腰椎下位レベル(L4/5)に移行す
るに従い,その三角面積範囲は広くなる
3).TLIF および
PELD
の TF での surgical safety working zone
4,5)の知識は
非常に重要である.
神経根走行と椎間板および椎間孔との関係について
は,L5 神経根(下位レベル)に移行するに従い,冠状断
で神経根分岐角度が急峻になる
6,7).また,矢状断では L5
神経根(下位レベル)に移行するに従い,角度は緩やか
(腹側シフト)になる
7).神経根(exiting nerve root)の
走行により Kambin triangle は L5/S1 については L4/5 よ
り狭くなる
5).さらに,L5 神経根(下位レベル)になる
ほど,神経節の位置は椎間孔内から脊柱菅内へシフトす
る.よって,椎間板ヘルニア脱出の際に疼痛が誘発され
やすい
6,7).椎間内神経根は,L4(平均値 3.9 mm)が最
大で,L1(平均値 3.3 mm)で最小となる
1).各神経根
は,下位腰椎レベルにいくに従い椎間孔の頭側から尾側
にシフトし,より中央部を走行する
8).よって,最も安
全な穿刺部は Kambin triangle の直角により近い部位で
ある.椎間板および椎間関節の加齢変性に伴い,椎間板
高位が減少することで Kambin triangle は狭小化する.
腰椎後背側に存在する筋群(内側より多裂筋,最長筋,
腸肋筋)より椎間孔に向かうと横突起間靭帯(inter
transverse ligament:ITL)が存在する.その内側で椎間
関節外側部が椎間孔外側部の入り口である.この ITL と
isthmus
間に分節動脈からの筋枝(dorsal branch)が存
在 す る
9). 神 経 節 の 末 よ り 後 脊 髄 内 側 枝(dorsal
ramus:DR)が走行する.DR は下位レベル乳様突起と
腰椎椎間孔外の靭帯・血管解剖
0°a
30°b
60°c
90°d
Fig. 1 Three dimensional computed tomography(CT)of the left lumbar intervertebral foramen in a healthy adult
a :CT taken from posterior view. b :CT taken from left oblique 30 degrees. c :CT taken from left oblique 60 degrees. d :CT taken from left side view.
Exiting L4 nerve root
Superior endplate of the L5 vertebral body
L4/5 articular process
Fig. 2 The anatomic borders of Kambin s tri-angle(outlined in red)
副突起間を走行し,1 椎間下位の椎間関節へといたる
10).
たとえば,L3 神経節の末 からの DR は,L4 の乳様突
起と副突起間を通って L4/5 関節包にいたる.腰仙椎移
行部(L5/S1)の ITL は lumbosacral ligament である
11).
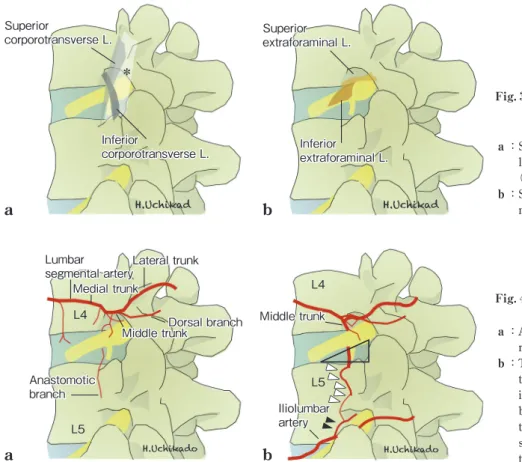
ITL を除去すると,椎間孔外に存在する靭帯は 2 層あ
る.第 1 層は下位椎体上縁から上位横突起(superior),
上位椎体下縁から下位横突起(inferior)に交叉する 2 本
の強靭な靭帯(corporotransverse ligament:CTL)であ
る(Fig. 3 a).第 2 層は,神経根を固定する上下の 2 本
の靭帯(extra foraminal ligament:EFL)である(Fig. 3
b).Transforaminal ligament(3 本)を除去することに
よって神経根(L3∼5,L5 で最大)の可動性が増すこと
が証明されている
12,13).Caglar ら
11)は,CTL を Y
liga-ment
として報告している.逆 Y 字で 3 つの compartment
に分かれる.Anterolateral compartment に神経前枝と腰
動静脈の median trunk,posterolateral compartment に
middle trumk
からの dorsal branch,middle compartment
に神経後枝と lateral trunk が通過する.腰仙椎移行部の
CTL
の浅層(inferior)は部位特異的な lumbosacral hood
を形成する
14).
EFL は 2 本存在し,Kraan ら
13)は T12 L1 神経根と L2
5
神経根で走行が異なることを報告した.Inferior EFL
る.この靭帯によって,椎間孔外神経が固定されている.
動脈分岐については,腹部大動脈から L1 4 の各分節
動脈(segmental もしくは lumbar artery)から medial,
middle,lateral trunkに分かれる(Fig. 4 a).Medial trunk
からは腰神経叢,筋枝を分枝した後,椎間孔頭腹側部で
spinal branch
および ganglionic branch が分枝する.
Middle trunk
からは dorsal,anastomotic branch が分枝
する
15,16).最終的に,lateral trunk
は腹壁にいたる.Spi-nal branch
に関しては,腰動脈から分枝される
Adamkie-wicz artery
は T12 L1 で 16%,L1 2 で 21.4%,L2 4 で
6
%と必ずしもまれでない.手術の際に,脊髄梗塞などに
注意が必要である
17).L5 spinal branch については,腰動
脈はなく,内腸骨動脈(internal iliac artery)から
iliolum-bar artery
もしくは medial sacral artery より分枝される.
Segmental artery
に椎間孔腹側から横突起腹側を縦走す
る交通枝が存在する.この交通枝は,おのおののレベル
でみられ,約半数に認められる
16).この交通枝は横突起
の約 4 mm 弱前方を走行する.L5 腰動脈は存在しないた
め,internal iliac artery からの iliolumbar artery もしくは
medial sacral arter y
から供給される.Medial sacral
artery
からの場合,L5/S1 椎間孔までは分枝されないた
め交通枝は存在しない.L4 L5 間に交通枝がみられる際
Inferior extraforaminal L. Superior corporotransverse L. Inferior corporotransverse L. Superior extraforaminal L. *b
a
L4 L5 Dorsal branch Lateral trunk Middle trunk Anastomotic branch Lumbar segmental artery Middle trunk Iliolumbar artery L4 L5 Medial trunka
b
Fig. 3 Schematic drawings of the external ligaments of the intervertebral fora-men
a : Superior and inferior corporotransverse
ligament(L), intertransverse ligament (asterisk).
b : Superior and inferior extraforaminal
liga-ment(L).
Fig. 4 Schematic drawings of the extrafo-raminal arteries
a : A lumbar artery and branch in the
extrafo-raminal region. L:lumbar vertebra
b : The anastomotic branch originating from
the middle trunk(L4)enters the L5/S1 inter ver tebral foramen. The L5 spinal branch(black arrowheads)and the anas-tomotic branch(white arrowheads)are shown between L4 and L5. L4/5 Kambin s triangle(black triangle).
椎間孔腹側の Kambin triangle の中を走行する(Fig. 4
b).特にその損傷は,後腹膜血腫
18)の原因と考える.
よって,本交通枝の損傷が疑われる症例では,術前検査
で血管走行の確認把握は重要と考える
19).
PELD に関しては,後腹膜臓器に関し,高位腰椎症例
で腎臓や腹膜に注意しなければいけない.腰神経叢は特
に陰部大腿神経に注意を要するが,Kambin triangle を指
標にするので問題となることは少ない
20).椎間孔周囲の
血管解剖の術前評価は,合併症回避のために非常に重要
である.穿刺の際,下位上関節突起に近い直角部が,よ
り安全である.
椎間孔を通る動脈は,spinal branch と ganglionic
branch
が重要である.椎間孔での動脈の存在について
3D CT angiography(3D CTA)を用いた研究では,
Kambin triangle
内でも動脈が認められることが報告さ
れている
21).よって,PELD の術前 3D CTA は術前検査
として重要と考えるため,今後検証する必要がある.
椎間孔における神経根の前根と,後根の走行のバリ
エーションについては菊地ら
22)により詳細に報告されて
いる.このバリエーションにより,臨床症状およびブ
ロックや除圧術の効果も左右される可能性が示唆されて
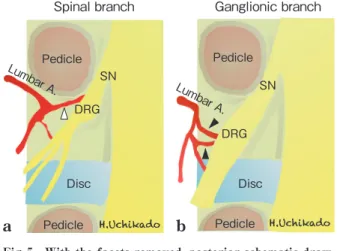
いる.Cho ら
23)は,神経根節(dorsal root ganglion:DRG)
周囲の動脈走行と硬膜の関係および前根および後根の組
織学的な報告をしている.Spinal branch および ganglion
branch
は硬膜貫通後に後根ではなく,前根と併走し,
radicular artery
となり,硬膜内を走行する(Fig. 5).
Akdemir
24)は,intraforaminal ligament(第 7 の椎間孔
靭帯)を報告した.これは,椎間孔内で神経根周囲を固
定している.椎間孔内にはほかに上,中,下の 3 本の
transforaminal ligament
と上下 2 本の corporopedicular
ligament
および ligamentum flavum
がある.Intraforami-nal ligament
の存在により,nerve stretch test の解剖学的
証明を報告した(Fig. 6).L5/S1 椎間孔は上位と異なり,
Zhao
ら
25)は superior,inferior および anterior,posterior
の radiating ligament の存在を報告した.
神経根は靭帯により固定されており,可動性のない椎
間孔ではカニューラ(外筒)操作には注意を要する(Fig.
7 a).Exiting nerve root の損傷を最小限にすべくさまざ
腰椎椎間孔内の靭帯・血管解剖
Intraforaminal L. Ligamentum flavum Mid-transforaminal L. NR A V Disk Pedicle Pedicle Facet Inferior corporopedicular L. Superior corporopedicular L. Inferior transforaminal L. Superior transforaminal L. Ganglionic branch DRG Pedicle Pedicle Lumbar A. Pedicle Pedicle Lumbar A. DRG Disc Disc SN SN Spinal brancha
b
Fig. 5 With the facets removed, posterior schematic draw-ings of the lumbar artery and its branches show the intraforaminal area
a : Spinal artery(white arrowhead)penetrates the sheath of the
spinal nerve(SN).
b : ganglionic branches(black arrowhead)to the dorsal root
ganglion(DRG).
SN:spinal nerve, DRG:dorsal root ganglion, Lumbar A:lumbar artery
Fig. 6 Schematic drawing of the interverte-bral foramen
Various intervertebral foraminal ligaments, intrafo-raminal ligaments, and nerve roots and vessels Superior and inferior corporopedicular ligament (L)and ligamentum flavum
Superior, mid-, and inferior transforaminal ligament (L)and intraforaminal ligament(L)
まな報告がなされている
26,27).変性や椎間孔狭窄を伴う
症例などでは foraminoplasty
28)を行ってアプローチする
か,顕微鏡視下手術を選択するほうが安全と考える.
椎間孔からみる脊柱管内は,articular segmentである.
この部位は椎間板,黄色靭帯,下位上関節突起,上下椎
体終板で構成され,その変性は脊柱管および椎間孔狭窄
症の原因である.椎弓(黄色靭帯のない),椎体骨,椎弓
根に囲まれる部位は oseous segment であり,椎体後面の
硬膜腹側の epidural space は L3 より L4,L5 で広くな
る
29).Articular segment には浅層および深層からなる黄
色靭帯(脊柱管背側)と後縦靭帯(腹側)が存在する.
背側に存在する黄色靭帯は頭側椎弓腹側の中下 3 分の 1
から尾側椎弓上縁に付着する.外側は椎間孔部で椎間関
節の腹側に達し,関節包や骨膜に移行している.一方,
腹側の後縦靭帯は,椎体背面中央を縦走する.Articular
segment
である椎間板レベルで浅層は外側へ移行し,
epidural membrane
となり,epiradicular sheath を形成す
る.また,神経根周囲の nerve root axilla には豊富な脂肪
組織が存在すると同時に硬膜外静脈叢が発達している
(Fig. 8 a).PELD の TF の際,脊柱管腹側に後縦靭帯手
前を縦走する内椎体静脈層に遭遇する(Fig. 7 b).椎間
板ヘルニア脱出などでは静脈の途絶所見が報告されてい
硬膜囊は,線維性結合組織である epidural membrane
に包まれている.この薄い膜様組織は豊富な脂肪組織を
含有しつつ,背側および腹側正中部で,左右の黄色靭帯,
後縦靭帯にゆるく結合している.すなわち硬膜囊は,脊
柱管腹側と背側に存在する硬膜外靭帯(meningoverte-bral ligament) に よ り 固 定 さ れ て い る(Fig. 8 a).
Solarolgu
らは,L5 椎弓切除の術中初見で,硬膜囊背側
表面から黄色靭帯正中部頭側につながる 1∼2 本の靭帯
(ATA ligament
31))の存在を報告した.ATA の損傷は,
硬膜損傷ひいては術後髄液漏の原因となる.Shi ら
32)は
屍体を用い,腰仙椎レベルでの内視鏡解剖を報告してい
る.尾側に従い,その靭帯存在と本数(0∼2 or 3 本,幅
0.6 mm
前後,長さ 16 mm 前後,厚さ 0.15 mm)は増え,
仙骨レベルで最も太く強くなる.硬膜外脂肪血管との連
続性もみられることより,その損傷は術中・術後硬膜外
出血の原因になり得る
32).硬膜腹側では Hoffmann 靭
帯
33)と呼ばれ,後縦靭帯浅層から神経根囊部よりやや頭
側に付着している内側 Hoffmann 靭帯が,椎弓根内側の
骨膜や epidural membrane から始まる外側 Hoffmann 靭
帯がある(Fig. 8 a).その線維は神経根外側方の
epira-dicular sheath
の形成に関与している
27).この Hoffmann
靭帯の切離前後では,神経根の可動性は大きく変化す
る.この Hoffmann 靭帯の硬膜腹側の損傷により,髄液
漏,ひいては神経根ヘルニア
34),硬膜内への椎間板ヘル
ニア再脱出
35)が起こり得るため,その扱いは慎重に行う
椎間孔からみる脊柱管内
a
Exiting nerve root Exiting nerve rootb
Dural sac Dural sac PLL PLL Epidural fat Epidural fat Ligamentum flavum Disk PLL PLL Dural sacExiting nerve root
Disk Fragment
Fat Fat
L4 L5
c
Fig. 7 Intraoperative views of intraspi-nal caintraspi-nal seen from endoscopic transforaminal approach a : Exiting nerve root at left L4/5. b : Epiduroscopic view of ventral
anatomi-cal structures of the spinal dura.
c : Schematic drawing of intraspinal canal
structures seen from endoscopic trans-foraminal approach.
近年の術前画像診断の向上に伴い,術前に腰仙椎の移
行椎や神経走行異常は予測可能になってきた.神経根の
走行異常が疑われる場合は,経椎間孔アプローチは避け
るべきである.術中に思わぬ神経走行異常に遭遇する場
合がある.電気生理学的な機能解剖はもちろんである
が,遭遇した場合,神経根走行異常のタイプ
36,37)と内視
鏡視野での imaging は重要である.椎間孔からみえる脊
柱管内の構造物の内視鏡術中写真(Fig. 7 a, b)とシェー
マ(Fig. 7 c)を示す.
最後に,腰椎椎間孔周囲の解剖の知識は PELD の TF
法にとって必要不可欠である.また,その術前イメージ
ングは重要であり,合併症の予防および診断治療成績に
つながるものと確信している.
利益相反開示について 本論文に関し,著者らは開示すべき利益相反を有していな い. 文 献1) Torun F, Dolgun H, Tuna H, et al:Morphometric analysis of the roots and neural foramina of the lumbar vertebrae. Surg
Neural 66:148 151, 2006
2) Kambin P, Sampson S:Posterolateral percutaneous suction excision of herniated lumbar intervertebral discs:report of interim results. Clin Orthop Relat Res 207:37 43, 1986 3) Hoshide R, Feldman E, Taylor W:Cadaveric analysis of the
Kambin s triangle. Cureus 8:e475, 2016
4) Hardenbrook M, Lombardo S, Wilson MC, et al:The anatomic rationale for transforaminal interbody fusion:a cadaveic analy-sis. Neurosurg Focus 40:E12, 2016
5) Lertudomphonwanit T, Kaorochana G, Kraiwattanapon C, et al:Anatomic considerations of intervertebral disk perspective in lumbar posterolateral approach via Kambin s triangle: cadaveric study. Asian Spine J 10:821 827, 2016
6) Suh SW, Shingade VU, Lee SH, et al:Origin of lumbar spinal roots and their relationship to intervertebral disk:a cadaver and radiological study. J Bone Joint Surg 87:518 522, 2005 7) Wu YS, Lin Y, Zhang XL, et al:The projection of nerve roots on
the posterior aspect of spine from T11 to L5:a cadaver and radiological study. Spine 37:E1232 1237, 2012
8) Arslan M, Cömert A, Açar H, et al:Nerve root to lumbar disc relationships at the intervertebral foramen from a surgical viewpoint:An anatomical study. Clin Anat 25:218 223, 2012 9) Viswanathan R, Swamy NK, Tobler WD, et al:Extraforaminal
lumbar disc herniations:microsurgical anatomy and surgical approach. J Neurosurg 96(2 Suppl):206 211, 2002
10) Bogduk N, Long DM:The anatomy of the so called“articular nerves”and their relationship to facet denervation in the treat-ment of low back pain. J Neurosurg 51:172 177, 1979 11) Caglar YS, Dolgun H, Ugur HC, et al:A ligament in the lumbar
foramina:invert Y ligament:an anatomic report. Spine 29: 1504 1507, 2004
12) Grimes PF, Massie JB, Garfin SR:Anatomic and biomechanical analysis of the lower lumbar foraminal ligaments. Spine 25: 2009 2014, 2000
13) Kraan GA, Delwel EJ, Hoogland PV, et al:Extraforaminal liga-ment attachliga-ments of human lumbar nerves. Spine 30:601 605, 2005
14) Amonoo kuofi HS, el Badawi MG, Fatani JA, et al:Ligaments associated with lumbar intervertebral foramina. 2. The fifth lumbar level. J Anat 159:1 10, 1988
15) Caglar YS, Dolgun H, Ugur HC, et al:Extraforaminal lumbar arterial anatomy. Surg Neural 61:29 33, 2004
16) Arslan M, Comert A, Acar HI, et al:Surgical view of the lumbar arteries and their branches:An anatomical study. Neuro-
surgery 68(Suppl 1):16 22, 2011
17) Illuminati G, Koskas F, Bertagni A, et al:Variations in the origin of the artery of Adamkiewicz. Riv Eur Sci Med Farmacol 18: 61 66, 1996
18) Ahn Y, Kim JU, Lee BH, et al:Postoperative retroperitoneal hematoma following transforaminal endoscopic lumbar
discec-結 語
Ascending lumbar.V. (dorsal) Emissary V. Longitudinal antero-internal epidural V. (ventral) Longitudinal antero-external epidural V. (dorsal) *Hoffmann ligament ☆Meningovertebral ligament Disc Lamina LF PLL Dural sac SN * ☆a
b
Fig. 8 Schematic drawing of epidural ligaments and venous plexus a : Intraspinal canal ligaments and veins,
Hoffmann s ligaments(asterisk)at the ventral dura, meningovertebral liga-ments(star)at the dorsal dura.
b :Intraspinal canal epidural veins.
SN:spinal nerve, LF:ligamentum flavum, PLL:posterior longitudinal ligament, V: vein
tomy. J Neurosurg Spine 10:595 602, 2009
19) Sakai T, Tezuka F, Wada K, et al:Risk management for avoid-ance of major vascular injury due to lateral transpsoas approach.
Spine 41:450 453, 2016
20) Moro T, Kikuchi S, Konno S, et al:An anatomical study of the lumbar plexus with respect to retroperitoneal endoscopic sur-gery. Spine 28:423 428, 2003
21) Simon JI, McAuliffe M, Smoker D:Location of radicular spinal arteries in the lumbar spine from analysis of CT angiogram of the abdomen and pelvis. Pain Med 17:46 51, 2016
22) 菊地臣一,蓮江光男:腰仙椎部神経症状:カラーで見る解剖 学的背景.東京,金原出版,1996
23) Cho KH, Jin ZW, Abe H, et al:Neural dural transition at the thoracic and lumbar ner ve roots:A hitstological study of human late stage fetuses. Biomed Res Int, 2016, doi:10.1155/ 2016/8163519
24) Akdemir G:Thoracic and lumbar intraforaminal ligaments. J
Neurosurg Spine 13:351 355, 2010
25) Zhao Q, Zhong E, Shi B, et al:The morphology and signifi-cance of the intraforaminal ligaments at the L5 S1 levels. Spine
J 16:1001 1006, 2016
26) Cho JY, Lee SH, Lee HY:Prevention of development of postop-erative dysesthesia in transforaminal percutaneous endoscopic lumbar discectomy for intracanalicular lumbar disc hernia-tion:floating retraction technique. Minim Invasive Neurosurg
54:214 218, 2011
27) Choi KC, Kim JS, Park CK:Percutaneus endoscopic Lumbar Discectomy as an alternative to open lumbar microdiscectomy for large lumbar disc herniation. Pain Physician 19:E291 300, 2016
28) Henmi T, Terai T, Hibino N, et al:Percutaneous endoscopic
lumbar discectomy utilizing ventral epiduroscopic observation technique and foraminoplasty for transligamentous extruded nucleus purposes:technical note. J Neurosurg Spine 24:275 280, 2016
29) Teske W, Krämer J, Lichtinger T, et al:A morphometric cadaver study of the anterior lumbar epidural space. Eur Spine
J 21:1479 1482, 2012
30) Roland J, Treil J, Larde D, et al:Lumbar phlebography in the diagnosis of disc herniations. J Neurosurg 49:544 550, 1978 31) Solaroglu I, Okutan O, Beskonakli E:The ATA and its surgical
importance:a newly described ligament lying between the dural sac and the ligamentum flavum at the L5 level. Spine
36:1268 1272, 2011
32) Shi B, Li X, Li H, et al:The morphology and clinical significance of the dorsal meningovertebra ligaments in the lumbosacral epidural space. Spine 37:1093 1098, 2012
33) Tardieu GG, Fisahn C, Loukas M, et al:The epidural ligaments (of Hofmann):a comprehensive review of the literature. Cures
8:e779, 2016
34) Ahn Y, Lee HY, Lee SH, et al:Dural tears in percutaneous endoscopic lumbar discectomy. Eur Spine J 20:58 64, 2011 35) Tamaki Y, Sakai T, Miyagi R, et al:Intradural lumbar disc
her-niation after percutaneous endoscopic lumbar discectomy: case report. J Neurosurg Spine 23:336 339, 2015
36) Neidre A, MacNab I:Anomalies of the lumbosacral nerve roots. Review of 16 cases and classification. Spine 8:294 299, 1983
37) McCulloch JA, Waddell G:Variation of the lumbosacral myo-tome bony segmental anomalies. J Bone Joint Surg Br 62 B: 475 480, 1980