he surgical repair of mycotic abdominal aortic aneurysms is often difficult especially because of in situ recurrence. Brown reported a mortality rate of 32% and re-infection rate of 16% for this procedure when reconstructed in situ, and a mortality rate of 13% when reconstructed with an extra-anatomic bypass, with the overall mortality rate being 40%.1In the present study
we report our recent experience and treatment.
Case Report
A 66-year-old man was referred to the emergency room at JR Tokyo General Hospital by ambulance complaining of low-grade fever, hypogastralgia, vomiting, and back pain. On physical examination, a pulsatile mass, measuring 5 cm in diameter, was palpated in his abdomen. An abdominal roentgenogram showed airation in his left psoas muscle area. Computed tomography (CT) examination revealed extravasation of the contrast media from the infra-renal abdominal aorta. The aorta was surrounded by an aerated low-density area (Fig 1). Under the diagnosis of ruptured mycotic abdominal aorta, an urgent operation was per-formed. During the procedure, a right axillo-bilateral fem-oral artery bypass graft was first installed using a branched 8-mm ring-reinforced EPTFE graft. This wound was closed and wrapped with a drape.
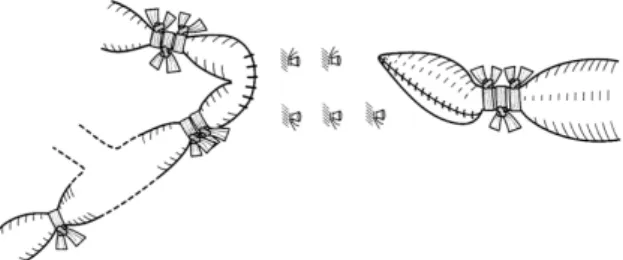
Thereafter, a median laparotomy was made and the infected part of the infra-renal lumbar part of the aorta was totally excised. The stumps were obliquely excised and closed. Moreover, the intact abdominal aorta proximal to the stump and the common iliac arteries distal to the stumps were ligated with Teflon tapes in order to reduce the pres-sure to the stumps (Fig 2). The surrounding hematoma was almost removed, the omentum was mobilized, and the infected area covered.
Japanese Circulation Journal Vol.65, December 2001
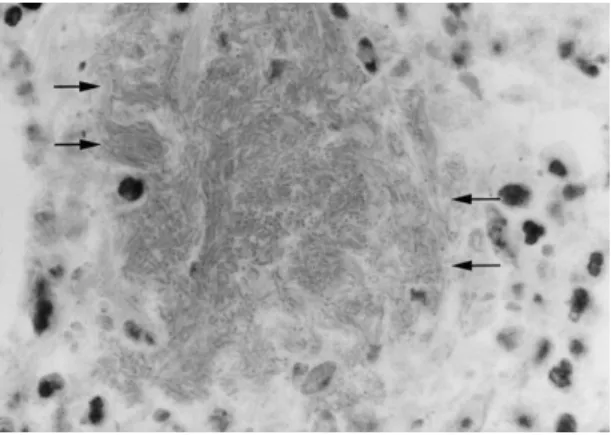
Pathological examination of the resected aorta revealed bacterial nests of Enterobactor cloacae (Fig 3). The patient’s postoperative course was uneventful; his fever had receded and any inflammatory changes had normalized after 6 weeks. He was discharged from hospital 4 months after the operation. Oral antibiotic therapy was continued for 6 months. The patient is alive and well and without any inflammatory signs 1 year after the operation.
Discussion
The diagnosis of an infected aneurysm is difficult. Jpn Circ J 2001; 65: 1085 – 1086
(Received December 8, 2000; revised manuscript received March 2, 2001; accepted April 12, 2001)
Division of Thoracic and Cardiovascular Surgery, JR Tokyo General Hospital, Tokyo, Japan
Mailing address: Motohiro Kawauchi, MD, Division of Thoracic and Cardiovascular Surgery, JR Tokyo General Hospital, 2-1-3 Yoyogi, Shibuya-ku, Tokyo 151-8528, Japan
‘No-Touch’ Isolation Procedure for Ruptured Mycotic
Abdominal Aortic Aneurysm
Kimihiro Tanaka, MD; Motohiro Kawauchi, MD; Yoshihiro Murota, MD; Akira Furuse, MD
The present study reports a case of the successful surgical repair of a ruptured infra-renal mycotic abdominal aorta with Enterobactor cloacae in a 66-year-old man. During the operative procedure, an extra-anatomic bypass was installed before the laparotomy in order to avoid bacterial contamination. A complete resection of the infected aorta, tapering of the arterial stumps, wrapping of the omentum, and ligation of the aorta and arteries with Teflon tapes was carried out. The patient is alive and well 1 year postsurgery. (Jpn Circ J 2001; 65: 1085 – 1086)
Key Words: Axillo-femoral bypass; Enterobactor cloacae; Mycotic abdominal aortic aneurysm; Rupture
T
Fig 1. Abdominal computed tomography. Arrow indicates extravasa-tion of contrast media. Aeraextravasa-tion was observed around the infra-renal abdominal aorta.
1086 TANAKA K et al.
Japanese Circulation Journal Vol.65, December 2001 Because mycotic aneurysms are thin-walled and friable by
inflammation, they readily rupture; hence, only 53% of cases with an abdominal mass are detected before opera-tion.1Rupture is often the most frequent symptom,2
there-fore, CT plays an essential role in a correct diagnosis. In the present case, CT revealed extravasation of contrast media, as well as aeration in the surrounding area, suggest-ing infection by gram-negative bacterium.2As infection was
highly suspected but bacteria are invisible during the surgi-cal procedure, a ‘no-touch’ isolation extra-anatomic bypass procedure was adopted.
There are 2 methods of treatment for such cases: (i) installing an extra-anatomic bypass, as carried out in the present case;3and (ii) anatomically replacing the
cryopre-served homograft.4,5Because the present case was a rupture,
there was no time to access the homograft and so the extra-anatomic bypass procedure was elected. In situ replace-ment of Dacron grafts has a high incidence of reinfecting,1
but there are also some disadvantages to conducting an extra-anatomic bypass procedure.4 First, extra-anatomic
revascularization does not exclude the risk of graft contam-ination, so it was installed first before the laparotomy and the wound was then closed. Second, a blow-out of the aortic stump may lead to a dismal prognosis,4,5accounting for 43%
of early deaths.4Therefore, in addition to totally debriding
the infection site and suturing the omentum, the aortic stump was tapered and the proximal aorta was ligated with Teflon tape to reduce the pressure load to the stump.
Postoperative antibiotics are mandatory. Pasic et al recommend 2–12 weeks of intravenous administration followed by 4–16 weeks of oral administration.3Based on
treatment for infective endocarditis, in the present case, intravenous administration was conducted for 12 weeks and oral administration for 6 months, and life-long admin-istration was considered unnecessary.
Conclusion
Although the surgical treatment of a ruptured mycotic aneurysm is often difficult, the ‘no-touch’ extra-anatomic bypass grafting procedure can prevent an artificial graft from becoming contaminated during the operation, result-ing in an increased chance of a successful surgical repair.
References
1. Brown SL, Busuttil RW, Baker JD, Machlender HI, Moore WS, Barker WF: Bacteriologic and surgical determinants of survival in patients with mycotic aneurysms. J Vasc Surg 1984; 1: 541 – 547 2. Sessa C, Farah I, Voirin L, Magne JL, Brion JP, Guidicelli H: Infected
aneurysms of the infrarenal abdominal aorta: Diagnostic criteria and therapeutic strategy. Ann Vasc Surg 1997; 11: 453 – 463
3. Pasic M, Carrel T, Tonz M, Vogt P, von Segesser L, Turina M: Mycotic aneurysm of the abdominal aorta: Extra-anatomic versus in
situ reconstruction. Cardiovasc Surg 1993; 1: 48 – 52
4. Vogt PR, von Segesser LK, Goffin Y, Niederhauser U, Geroni M, Kunzli A, et al: Eradication of aortic infections with the use of cryop-reserved arterial homografts. Ann Thorac Surg 1996; 62: 640 – 645 5. Alonso M, Caeiro S, Cachaldora J, Segura R: Infected abdominal
aneurysm: In situ replacement with cryopreserved arterial homo-graft. J Cardiovasc Surg 1997; 38: 371 – 375
Fig 3. Microscopic examination revealed nests (arrows) of gram-negative rods.