1. Introduction
Nonalcoholic fatty liver disease (NAFLD) is a chronic liver disease caused primarily by obesity 1-3). In developed countries,
overeating and lack of exercise are steadily increasing the obese population, and this development has made NAFLD the most frequently occurring liver disease, control of which is urgent. Though most NAFLD presents as simple steatosis, 10-20% is nonalcoholic steatohepatitis (NASH) progressing to hepatic cirrhosis or hepatocellular carcinoma. Aging is an extremely important risk factor for pathologic progression, and the disease is certainly one in the purview of this academic symposium. The keynote address of the symposium held to share the most recent information on NAFLD was followed by a presentation of recent findings concerning mechanisms of exercise therapy inhibiting steatosis, the relation between the Anti-Aging hormone dehydroepiandrosterone (DHEA) and progression of NAFLD, and the role of growth hormone (GH) in NAFLD pathology and treatment. Our paper summarizes this information.
Review Article
Science of Nonalcoholic Fatty Liver Disease in Anti-Aging Medicine 2011
Yoshio Sumida
1), Yuji Naito
2), Etsuko Hashimoto
3), Wataru Aoi
4), Yutaka Takahashi
5), Yoshikazu Yonei
6),
Toshikazu Yoshikawa
2)1) Center for Digestive and Liver Diseases, Nara City Hospital
2) Department of Molecular Gastroenterology and Hepatology, Kyoto Prefectural University of Medicine 3) Department of Internal Medicine and Gastroenterology, Tokyo Women's Medical University
4) Laboratory of Health Science, Graduate School of Life and Environmental Sciences, Kyoto Prefectural University 5) Division of Diabetes and Endocrinology, Kobe University Graduate School of Medicine
6) Anti-Aging Medical Research Center, Graduate School of Life and Medical Sciences, Doshisha University
Abstract
Nonalcoholic fatty liver disease (NAFLD) is a chronic liver disease caused primarily by obesity, and its incidence among Japanese adults is rapidly rising at 10-40%. Most NAFLD presents as simple steatosis, but some are nonalcoholic steatohepatitis (NASH) progressing to hepatic cirrhosis or hepatocellular carcinoma. NAFLD is diagnosed by the following three features; (1) alcohol non-consumers (“non-drinkers”), (2) steatosis, and (3) exclusion of liver disease caused by other factors, with non-drinkers including light consumers of alcohol in amounts not engendering alcoholic liver disease. Dietary treatment is the basis of therapy, but evidence concerning exercise therapy has accumulated recently, and its mechanisms have been explained.
Dehydroepiandrosterone (DHEA) is an androgenic intermediate metabolite produced by the adrenals and known as an Anti-Aging hormone with an improving effect on insulin resistance, an antioxidant effect, and an antifibrotic effect. Serum dehydroepiandrosterone sulfate (DHEA-s) has been shown to present low levels in advanced stages of NAFLD and diminished DHEA may contribute to progression of NAFLD. Growth hormone (GH) plays a crucial role not only in childhood growth but also in adult metabolic regulation, and adult GH deficiency (GHD) leads to increased visceral fat, dyslipidemia, and decreased QOL. Complicating NAFLD/NASH is a frequent occurrence in adult GHD and is improved by GH replacement therapy. On this basis, aging is an important risk factor for progression of NASH, which suggests a need for discussion of NASH and NAFLD from the perspective of Anti-Aging Medicine.
KEY WORDS: oxidative stress, insulin resistance,exercise, dehydroepiandrosterone, growth hormone
Published online: Feb. 29, 2012
Anti-Aging Medicine 9 (1) : 24-33, 2012 Yoshio Sumida, M.D. Ph.D
2. What is NAFLD/NASH
1) Overview of NAFLD/NASH
Excess fat in the liver is stored in the hepatic cytoplasm as fat globules and presents as steatosis. The causes of steatosis include increased uptake of fatty acids by the liver, accelerated synthesis or decreased burning of fatty acids, and impaired synthesis or decreased hepatic release of very low density lipoproteins (VLDL). Pathologically, steatosis is defined as observation of fact globules in 5-10% or more of the hepatocytes
4-5). Steatosis includes simple steatosis and steatohepatitis,
and in the latter, deposition of fat is accompanied by necrotic, inflammatory changes and by fibrosis progressing gradually to hepatic cirrhosis. Clinically, fatty liver disease is classified as alcoholic and nonalcoholic (NAFLD). Causes of NAFLD include obesity, diabetes, dyslipidemia, drug agents (e.g., steroid, tetracycline), lipid metabolism disorder, endocrine disease (e.g., Cushing syndrome, GH deficiency), poisoning (e.g. white phosphorus), and advanced malnutrition, but the majority
originated in a basis of obesity, and particularly insulin resistance caused by visceral fat obesity. A “two-hit theory” has been proposed for the mechanism whereby some NAFLD is not limited to simple steatosis and leads to NASH 6). In this
hypothesis, the first hit is fat deposition in the hepatocytes, in other words, fatty liver, and NASH occurs when some type of additional second hit causes necrotic, inflammatory changes. Examples of second hits include oxidative stress, TNF-α and other cytokines, insulin resistance, CYP2E1 abnormality, and iron, but oxidative stress is regarded as the most important factor 6,7). Because the capacity to mitigate oxidative stress
decreases with age, aging represents a risk factor for pathologic progression. Recently, the importance of the patatin-like phospholipase 3 gene (PNPLA 3) as a genetic factor has also been shown 8).
2) NAFLD/NASH epidemiology
The incidence of NAFLD among individuals examined in Japan is 10-40%, making this a national disease. Because 10-20% of NAFLD is NASH, its incidence among adults is estimated as 1-5%. The incidence of NAFLD by sex and age reflects the distribution of the obese population itself among Japanese individuals 1-3,9). Males age 30-60 years demonstrate
a consistently high incidence of nearly 20-30%, and females age 20-60 show an incidence increasing gradually with age to a high of roughly 30% after menopause. Incidence is also correlated with obesity level, and in cases of high obesity with a body mass index (BMI) of 30 or more, NAFLD is diagnosed at a rate of 70-80%. Approximately 50% of individuals with diabetes also contract NAFLD, as do approximately 40% of those with dyslipidemia.
The incidence of NAFLD differs by race; in an epidemiological study diagnosing NAFLD by MR spectroscopy (MRS) in 2283 cases in the US, the incidence was significantly higher among Hispanics, at 45% for this group, versus 33% among whites, and 24% among blacks 10). Note should be taken that Japanese
are a racial group more readily susceptible to visceral disorders such as NASH and diabetes than to obesity.
3) NAFLD/NASH pathology
In more than 90% of cases, NAFLD or NASH complicates lifestyle-related diseases such as obesity, diabetes, dyslipidemia, hypertension 1-3). Subjective symptoms are often not recognized
until progression to hepatic cirrhosis, and the opportunities for diagnosis include regular health examinations. Hematology and biochemistry assays are characterized by elevated transaminases, ALT foremost, but note should be taken that the diseases occur not infrequently in cases with normal ALT levels. Hepatic fibrosis represents an index of severity which, with gradual progression, leads to hepatic cirrhosis. When fibrosis progresses to bridging fibrosis, hyaluronic acid and other markers of hepatic fibrosis rise, and in cirrhosis, platelets, coagulability, and albumin levels decrease. Decompensated cirrhosis presents symptoms of liver failure such as jaundice, hepatic coma, esophageal varices, and ascites.
With regard to prognosis, liver-related mortality in simple fatty liver disease is rare. In NASH, progression to hepatic cirrhosis is 10-25% in 5 years, and 5-year survival is 70-95%. The most frequent cause of death is cardiovascular event, followed by malignant tumor and liver-related death, and the incidence of cardiovascular events and liver-related death is significantly higher than that in the general population. NAFLD is the hepatic pathology of metabolic syndrome but
also aggravates insulin resistance in the liver and represents a cause of metabolic syndrome. The interaction of both diseases also engenders a vicious circle. Elevation of oxidative LDL, plaque formation on carotid duplex ultrasound, and other such findings are also observed frequently in NAFLD and are noted risk factors for cardiovascular events and diabetes. NAFLD must also be understood as a systemic disease, not merely a liver disease. In NASH-related cirrhosis 11), the 5-year rate
of hepatocarcinoma is approximately 10%, 5-year survival is approximately 70-80%, and liver-related death is the most frequent cause of death, at 70-80%.
4) NAFLD/NASH diagnosis
NAFLD is diagnosed by (1) no-alcohol consumption status (“non-drinker”), (2) diagnosis of fatty liver through liver tissue or diagnostic imaging (US, CT, MRI), and (3) exclusion of liver disease due to other causes 1-3). Non-drinkers
include individuals consuming alcohol to an extent not causing alcoholic liver dysfunction (ethanol conversion of 20 g/day or lower, Japanese sake conversion of 180 ml/day or lower). Given the lack of blood biochemistry markers to diagnose fatty liver, and its not infrequent occurrence among cases presenting normal AST and ALT, histological diagnosis or diagnostic imaging is essential. The need for exclusion of liver disease due to other causes stems from the fact that other liver diseases also cause fatty liver. NAFLD also complicates viral liver disease or autoimmune hepatitis and aggravates these conditions.
T he d iag nost ic c r it e r ia for NASH a re NA F LD accompanied by presentation of steatohepatitis in the hepatic pathology observed. Severity in the pathologic diagnosis of NASH is diagnosed by activity (grade: hepatocyte swelling, fat deposition, inflammatory cellular infiltration) and fibrosis (stage) 4,5,12).
Liver biopsy for pathologic diagnosis is an invasive test, but at present, there are no established hematology assay markers or diagnostic imaging methods for diagnosis of NASH. Indices under study include the apoptosis marker CK-18; TNF-α, IL-6 and other inflammatory cytokines; adiponectin, a beneficial adipocytokine; oxidative stress-induced thioredoxin; oxidative LDL; and high-sensitivity CRP 13). A number of
scoring systems combining multiple parameters have also been reported, and the NAFIC score, created in Japan, provides high diagnostic accuracy for NASH 14). Systems such as NAFLD
fibrosis score 15) relating to severity of fibrosis have also been
devised and are useful for assessing severity 16).
Problems in NASH diagnosis include the lack of hematodiagnostic markers and consequent reliance on exclusionary diagnosis, and the need for liver biopsy in diagnosis. From the standpoint of numbers as well, liver biopsy for diagnosis of NASH in all cases of NAFLD is impractical. Cases of diagnosed NAFLD also indicated for additional liver biopsy are (1) cases of NASH where stringent treatment is deemed necessary, and (2) cases requiring differential diagnosis of autoimmune hepatitis and other such liver disease. Cases of NASH requiring stringent treatment are cases of NAFLD in which improvement of lifestyle habits is not possible and AST or ALT elevation continues, and those among the elderly, highly obese, diabetics, and individuals with a pattern of decreased liver function.
5) NAFLD/NASH treatment
Treatment strategies devised for NAFLD are tailored to its cause. The pathology progresses through a “first hit” of fatty liver compounded by some type of “second hit.” In this respect,
the treatment first addresses fatty liver by treating obesity or lifestyle habits primarily through diet and exercise therapy; treatment also addresses the second hit (Fig. 1) 1-3),17-20).
Though the most important basic treatment is weight control through diet and exercise therapy, weight loss fails in nearly half of all cases, and this modality of treatment is not simple. In cases where obesity simply cannot be improved, drug treatment and surgical treatment are the final treatment alternatives for relief from the hardships of obesity treatment 20).
For diabetes, drugs improving insulin resistance are the first choice. Such drugs include thiazolidine derivatives (pioglitazone) and biguanide drugs (metformin). Pioglitazone is a drug agent which acts as a peroxisome proliferator-activated receptor γ (PPARγ) and is also reported to improve insulin resistance, accelerate burning of fatty acids by hepatic mitochondria, reduce inflammation, and increase adiponectin production. There are also many reports and a high evidence level for the agent in diabetes-complicated and non-complicated NAFLD 21). However, aggravation of pathology
by discontinuation from the drug makes the time frame of discontinuation a problem. Adverse effects also include weight gain and fluid retention (edema, heart failure). Risk of bladder cancer is another emergent problem.
Metfor m i n reg ulates blood suga r by i n h ibit i ng gluconeogenesis in the liver and increasing sugar uptake by the liver. Efficacy in NAFLD is also reported. Therapeutics for dyslipidemia (e.g., statins, bezafibrate, probucol, EPA), antihypertensives, hepatic fibrosis inhibitors, and drugs with an insulin resistance-improving effect or antioxidant effect (angiotensin II receptor blockers (ARB), calcium blockers) are also administered. Drugs administered to counter the second hit include antioxidants (vitamin E, vitamin C), and ursodeoxycholic acid (urso) used as a liver protectant. These are safe, widely administered drugs with virtually no adverse effects. Vitamin E in particular has drawn attention for a recent report of better efficacy in a comparison of therapeutic effect versus pioglitazone 22).
End-stage cirrhosis caused by NAFLD is a transplant-indicated disease. Recurrence of NAFLD after transplant is reported in approximately 30% of cases, but post-transplant survival is equivalent to that in other non-viral liver disease.
3. Exercise-derived prevention and improvement
of fatty liver
Accumulation of intrahepatic fat is caused by an increasd blood-borne influx of glucose and fatty acids, the basic substance of neutral fats, and lack of exercise and regular consumption of a diet high in fats and sugars thus contribute greatly to the formation of fatty liver. Additionally, when accumulation of visceral fat has led to a state of insulin resistance, levels of glucose and fatty acids in the blood are constantly elevated, and the inflow of these basic substances is increased; at the same time, the fat metabolism capability of the liver itself weakens, promoting fatty liver. In reality, most metabolic syndrome patients are also known to have concurrent fatty liver 23). Exercise has a one-time effect of raising energy
consumption during exercise as well as fitness effects including reduction of body fat and improvement of insulin resistance; exercise thus represents a plan contributing to prevention and improvement of fatty liver. Recent research has slowly and steadily increased evidence for the effect of exercise on fatty liver and the understanding of its mechanism.
1) Evidence for inhibition of fatty liver by exercise
By increasing the use of sugars and fats, the basic structures of energy, exercise is well known to move the energy balance of the body into deficit and thereby reduce levels of body fat and lipids in the blood. Because exercise dramatically increases energy metabolism particularly in skeletal muscle, to date there have been many studies concerning sugar metabolism and fat metabolism in skeletal muscle. Although there are not many research studies concerning liver function and exercise, it has been suggested that exercise improves liver function because exercise reduces levels of neutral fats, cholesterol, and free fatty acids in the blood and likewise inhibits elevation of aspartate aminotransferase and alanine aminotransferase, indices reflecting liver dysfunction 24,25). On
the other hand, it is quite recent that research efforts to find out the effects of exercise on intrahepatic fat started, and some reports from crosscutting research showed that individuals with exercise habits have little accumulation of intrahepatic fat. Perseghin et al.26) used MRI to evaluate intrahepatic fat and
reported that a significant negative correlation existed between
levels of routine physical activity and levels of intrahepatic fat, among both NAFLD patients and healthy individuals. In other words, their results suggested that increased energy consumption through increased physical activity inhibited not only fatty tissue, but also accumulation of intrahepatic fat. Krasnoff et al.27) also showed that maximum oxygen intake
levels were low among patients with a high NAFLD activity score, another finding indicating that performance of exercise greatly preserves cardiopulmonary function and suggesting a link to inhibition of fatty liver and consequent progression to NAFLD. Interventional research completed by St. George et al.28) also showed that 3 months of exercise therapy improved
indices of liver function in NAFLD patients, and that exercise contributed to improvement of NAFLD or prevention of its progression.
Aerobic exercise has long been regarded as fundamental for preventing disease, given its effects of energy consumption during exercise, reduction of body fat, and substantial efficacy in lowering blood sugar and fats in the blood. Because accumulation of visceral fat and concomitant insulin resistance contribute to progression of fatty liver, aerobic exercise is here again regarded as a fundamental form of exercise for prevention and improvement of these developments.
In contrast, Zelber-Sagi et al.29) reported that NAFLD
patients performing at least some form of exercise once or more per week had significantly lower accumulation of intrahepatic fat and neutral fats in blood, but in this instance, their research produced the highly interesting finding that effects were greater among individuals performing resistance exercise than those performing aerobic exercise. Likewise, Hallswort et al.30) completed interventional research involving
an 8-week resistance exercise program which found significant reductions of intrahepatic fat. More recently, a crosscutting study of subjects comprising 813 NAFLD patients found no significant improvement in NASH or hepatic fibrosis from exercise in individuals with habits of low-to-moderate intensity exercise, but a significant effect in individuals with habits of high-intensity exercise, leading the authors to state that exercise plans should place greater emphasis on exercise intensity than exercise quantity.
These results show that even resistance exercise or comparatively high-intensity, short-duration exercise can inhibit fatty liver or progression to NAFLD, i.e., this effect is not limited to walking, jogging, or other aerobic exercise alone. The results also suggest that such exercise is more effective than aerobic exercise performed for longer periods at low intensity.
2) Mechanism of exercise-derived inhibitory effect
on fatty liver
While immunological studies have shown that exercise inhibits accumulation of fat in the liver, many aspects of the mechanism are unclear. As mentioned previously, an excess influx of fatty acids and glucose to the liver accelerates synthesis of neutral fats, and it is easy to imagine that the considerable energy consumption of exercise inhibits fatty liver. At the same time, research in animal models of hepatic dysfunction stressed by overeating or by a choline-devoid, methionine-deficient diet have shown decreased fatty acid oxidation capability and substantially increased synthesis capability in the liver, indicating that accumulation of fat within the liver depends on the lipid metabolism capability of the liver itself 32,33). In other words, accumulation of neutral fats within
the liver is accelerated not simply by an excess blood-borne influx of their basic substances; the phenomenon occurs when the capability for oxidative decomposition of fatty acids in the liver decreases, and the capability for fatty acid synthesis is newly enhanced.
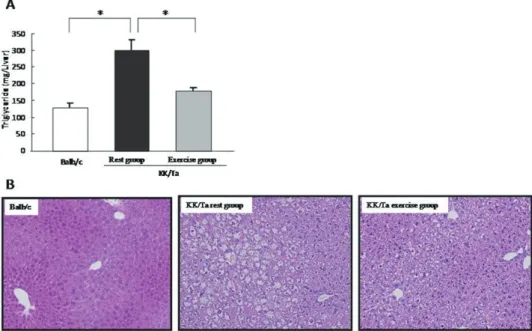
We used KK/Ta mice with fatty liver induced by a high-sucrose diet to investigate the effects of exercise on fatty liver and hepatic lipid metabolism-related enzymes. KK/Ta mice fed a high-sucrose diet for 12 weeks showed a marked increase in hepatic neutral fat content versus Balb/c mice (normal control mice). However, this accumulation of fat was inhibited significantly by the stress of 30 minutes of treadmill exercise 3 times per week (Fig. 2). At such time, fatty acid oxidation-related enzymes in mitochondria, i.e., carnitine palmitoyl transferase II, acyl-CoA dehydrogenase, and trifunctional enzyme were significantly elevated in the exercise group, while
the level of fatty acid synthase, a fatty acid synthesis enzyme, was substantially lower (Table 1). In other words, these results suggested that exercise inhibited fatty liver by improving the lipid metabolism of the liver itself.
Rector et al.34) reported that stress from 16 weeks of
spontaneous running exercise increased fatty acid oxidation capability in hepatic mitochondria in obese rats, which supports our results. Expression of these lipid metabolism-related enzymes is inhibited primarily by transcription factors such as sterol regulatory element-binding protein and PPARα 35,36).
Activity of the transcription factors is regulated by substances such as glucose, insulin, free fatty acids, adipokines in the blood 37,38), and exercise-derived improvement of visceral fats
and glucose tolerance is deemed related to inhibition of the blood-borne influx of these substances.
High-sucrose and high-fructose diets (fructose being a constituent sugar of sucrose) induce fatty liver more readily than high-glucose diets, starch diets, or high-fat diets 39,40).
One cause of this phenomenon is thought to be a higher hepatic glycogen storage rate of sucrose and fructose 41), which
accelerates synthesis of fatty acids from sugars saturating the liver. The possible linkage may be that fatty liver is inhibited by exercise-induced sugar consumption, accelerated release of hepatic glycogen into the blood, and inhibition of fatty acid synthesis from dietary sugars. In reality, in a study we completed, exercise inhibited fatty liver markedly, but improvement in glucose tolerance, blood insulin concentrations, and epididymal fat weight was less substantial. St. George et al.28) also reported that exercise-induced improvement in
NAFLD was observed independently of quantitative body fat reduction. These findings together suggest that exercise-derived inhibition of fatty liver is also influenced strongly by factors other than visceral fat loss and improvement of insulin resistance.
Additionally, we also observed that expression of heat shock protein 47 (HSP47), a collagen-binding protein, in the liver was lower in an exercise group 42). Because HSP47
functions as a molecular chaperone in the processes of pro-collagen biosynthesis and secretion in the liver, it is regarded as an index of hepatic fibrosis 43). Consequently, the fact that
exercise inhibits fatty liver also suggests a possible linkage to prevention of NASH progression, and these questions require further study.
4. Significance of dehydroepiandrosterone
(DHEA) in NAFLD
1) What is DHEA
DHEA is an androgenic intermediate metabolite produced and secreted primarily by the adrenals and gonads. It is also present in the body in sulfated form as DHEA-sulfate (DHEA-s), and these forms are mutually convertible. DHEA-s is the steroidal hormone present at highest concentration in the body. Changes in its levels typically track those of DHEA, do not change on an intraday basis, and can be measured stably. DHEA-s begins to increase in both males and females at approximately age 6-7 years, reaches a peak at puberty, continues at high levels until approximately age 13-25 years, and then decreases linearly with age 44). The effect
of DHEA as an androgen is approximately 5% weaker than that of testosterone but is known to produce various effects including improvement of insulin resistance 45-48), antioxidation 49), PPARα activation 50,51), inhibition of procollagen type
1 synthesis, inhibition of arteriosclerosis, and inhibition of osteoporosis.
2) Significance of serum DHEA-s measurement
A study of male residents of Baltimore found that high levels of DHEA served as an index of longevity in parallel with low body temperature and hypoinsulinemia. In Japan, a 27-year longitudinal study among residents of Taneshimaru, Fukuoka Prefecture found that survival rates among males were significantly higher in a high DHEA-s group, independent of blood pressure or blood sugar levels 52). Based on these data,
DHEA-s is known as an index of longevity at least among males and is measured as an Anti-Aging index 53). However, caution
is advised in that abnormal elevation is observed in Cushing syndrome, congenital adrenocortical hyperplasia, and other such diseases; low levels are observed in anorexia nervosa, chronic stress, and aggravation of diabetes; and improvement of these illnesses returns levels to normal. Elevation of DHEA levels is also reported to inhibit insulin resistance and metabolic syndrome 54), but elevation of DHEA is also conversely
reported to pose a risk of metabolic syndrome, and a consensus does not exist 55). Fukui et al. reported that decreased levels of
DHEA among males with type II diabetes were associated with arteriosclerosis and onset of kidney disease 56,57).
3) DHEA in NAFLD
Charlton et al. measured serum DHEA-s levels in NAFLD and reported that DHEA-s showed low values in cases progressing to NASH fibrosis 58). We also performed
Anti-Aging screening among 133 Japanese individuals diagnosed with NAFLD by liver biopsy and measured serum DHEA-s in 399 healthy age- and sex-matched individuals with normal ALT (30 IU/L or lower) who went through Anti-Aging screening
59). The composition of NAFLD cases included 90 with NASH
(Brunt stage 0-2 / 3-4: 73/17) and 43 non-NASH. In the NAFLD group, AST, ALP, γGTP, BMI, triglycerides, and HOMA-IR were significantly higher versus controls, but no significant difference between the groups in serum DHEA-s was observed. Other reports state that DHEA-s instead showed higher levels in cases of fatty liver versus non-fatty liver 60,61), indicating that
DHEA appears not to decline at least in NAFLD.
Investigation of the NAFLD group alone showed lower values in NASH versus non-NASH cases and decreasing levels of DHEA-s with progression of fibrosis reflected by Brunt stage, Mean ± standard error
ACD, acyl-coenzyme A dehydrogenase; CRT II, carnitine palmitoyl transferase II; ACC, acetyl-Coacarboxylase; ACL, ATP citrate lyase; FAS, fatty acid synthase.
*: p<0.05 vs Balb/c. #: p<0.05 vs KK/Ta rest group.
Table 1 Time for moderaExpression level of lipid
metabolism-related enzymes
Balb/c ACD CPT II Trifunctional enzyme ACC ACL FAS 100 100 100 100 100 100 3 8 5 8 6 11 ± ± ± ± ± ± KK/TaRest group Exercise group
57.5 74.4 45.3 126.3 84.0 124.5 4.3 7.5 1.9 7.5 3.6 10.7 * * * ± ± ± ± ± ± 75.8 135.0 59.3 126.2 103.0 77.6 5.1 6.7 3.9 6.2 7.4 4.1 *# *# *# * # ± ± ± ± ± ±
specifically, Stage 0: 170.4±129.2, Stage 1: 137.6±110.5, Stage 2: 96.2±79.3, Stage 3: 61.2±46.3, Stage 4: 30.0±32.0 mg/dL (mean ± SD, Fig. 3). Determination of factors contributory at stage 3 or higher by multivariate analysis showed that age, sex, and HOMA-IR were independent factors, and serum DHEA-s < 66 μg/mL was also a significant independent factor. The area under the receiver operating characteristics (ROC) curve and differentiation of Stage 3 and higher progression was good, at 0.79, and with serum DHEA-s of 66 μg/mL taken as a cutoff value, sensitivity was 77% and specificity was 73% 59). These
findings suggest an association between reduced DHEA-s and progression of NASH fibrosis and indicate that measurement of DHEA-s may be useful for discriminating cases of fibrotic progression.
4) Potential of DHEA as a therapeutic agent
A report in the JAMA concerning the anti-obesity effect of DHEA stated that a decrease in visceral and subcutaneous fat and improvement of insulin resistance were obtained among a DHEA-supplemented group in a double-blind, comparative study 62); however, a negative report followed 63), and the
usefulness of DHEA in lifestyle habit diseases is controversial at present. Improvement of fatty liver by administration of DHEA was reported in a DHEA-supplement group of an animal model 64), and DHEA supplementation may in the future serve
as a treatment for NASH.
5. A close association between GH/IGF-I
system and pathophysiology of NAFLD/
NASH
1) Age-dependent decrement in GH secretion and
the role of GH and IGF-I in the development of
NASH.
Secretion of growth hormone (GH) from the pituitary declines with age, and serum IGF-I also decreases. Though decreased muscular strength, decreased bone mass, and increased visceral fat are generally observed with increasing age, at least a part of these phenomena are considered to be related to the physiological decline in GH secretion. From this perspective, GH has been administered experimentally for Anti-Aging objectives, but at present, there is no clear evidence demonstrating usefulness. However, considering that the incidence of NAFLD increases with age, there is a substantial plausibility that the age-attendant decline in GH secretion bears on the risk for onset of NAFLD in the general population.
Adult growth hormone deficiency (GHD) is a state of impaired GH secretion caused by functional or organic abnormalities. Causes of adult GHD include tumors of the hypothalamic and pituitary regions, inflammation, granuloma, leukemia, head trauma, and aftereffects of radiotherapy. Epidemiologically, the annual rate of new onset of GHD is estimated as approximately 1800 individuals among 7000 patients examined each year for panhypopituitarism, in which GHD often occurs, but many additional latent cases are thought to exist.
Fatigability, decreased stamina and concentration, and other diminishments of QOL are observed as subjective symptoms of adult GHD, as are the physical symptoms of increased body fat (visceral fat), decreased bone mass, and decreased muscular strength. Increases in visceral fat in particular cause metabolic abnormalities, insulin resistance, and other conditions which are similar to those of metabolic
syndrome; cardiovascular changes are frequent; and the survival prognosis is poor 65). NAFLD may also be associated
with such increases in visceral fat. Supplementary treatment of adult GHD with GH was approved in Japan in April 2006. Supplementary GH treatment improves QOL and abnormal body composition (i.e., decreases in fat, particularly visceral fat, and increases in non-fat body weight). Though evidence as to whether survival prognosis is improved remains inadequate, one report states that rates of death, malignant tumor, and myocardial infarction were improved in a GH treatment group, suggesting that survival prognosis may also be improved 66).
2) Adult GHD with complicating NASH
Adult GHD presents pathologies highly resembling those of metabolic syndrome, with reported observations including frequent liver dysfunction, and small-scale retrospective research suggests that the incidence of NAFLD may be high
67,68). We reported our experience of a case demonstrating
dramatic improvement by GH treatment of adult GHD complicated by NASH 69). In this case of a 31-year-old
male, panhypopituitarism was attributed to pituitary stalk transection. In the pediatric phase, the patient received both cortisol and thyroxine and was also treated for short stature by GH supplementation, but at age 18 years, GH supplement therapy was discontinued. Thereafter, liver dysfunction and dyslipidemia worsened successively, and a detailed workup was performed. Visceral obesity and insulin resistance were observed, liver biopsy was performed for suspected severe NAFLD on abdominal ultrasound investigation, and NASH was diagnosed. When the patient was treated for adult GHD by GH supplementation, AST, ALT, and γGTP returned to normal rapidly (Fig. 4), and decreased high-sensitivity CRP concentration and decreased oxidative stress markers were observed. Ultimately, 6 months of GH treatment produced dramatic histological improvement (Fig. 5).
3) Incidence, therapeutic effect, prognosis of
NAFLD/NASH in adult GHD
When we analyzed 69 cases of panhypopituitarism with concomitant GH deficit from cases in our studies to elaborate the incidence of complicating NAFLD/NASH in adult GHD, we found a marked increase in this incidence. Cases in this group treated with GH supplementation demonstrated significant improvement of liver function, and cases who underwent liver biopsy before and after treatment demonstrated significant histological improvement of NASH (manuscript submitted). These results suggest that the GH-IGF-I system plays an important physiological role in the liver.
The prognosis of NASH in panhypopituitarism including adult GHD is reportedly poor 70). In 21 panhypopituitarism
patients who underwent liver biopsy, 10 had NASH, burnout NASH, or hepatic cirrhosis. When these cases were observed prospectively for 66 months, 2 of 6 deaths were found to be liver-related death, and an additional 2 cases were indicated for liver transplant due to liver failure 70). In a separate report, 133
of 1411 adult GHD cases in a no-GH therapy group developed malignant tumors in 5-year longitudinal observation (9%, relative risk versus control population: 1.83), and these included 7 cases of hepatocellular carcinoma (HCC). In contrast, the incidence of malignant tumor was significantly reduced in a GH therapy group, and no cases of HCC were observed 69).
This reduction in HCC may be attributable to a result in which progression from NASH to hepatic cirrhosis and then HCC was prevented.
4) Mechanism of onset for NAFLD/NASH in adult
GHD and therapeutic applications
Adult GHD presents elevation of inflammatory markers
71,72) and increased oxidative stress 73,74) associated with
increased visceral fat. GH supplementation improves these abnormalities. GH secretion is also inhibited among obese patients, and serum GH concentration is reportedly decreased generally in NAFLD 75), and these results suggest that decreased
GH secretion itself may play a causal role in obesity and onset of NAFLD/NASH. We analyzed a GH-deficient rat representing a model of adult GHD to investigate this pathology and found that NASH occurred as in humans, and that administration of GH/IGF-I reduced oxidative stress and improved both mitochondrial morphology and liver tissue. Administration of GH/IGF-I to a NASH model mouse to investigate general therapeutic application in NASH also demonstrated an improvement of histology. Though the general treatment of NASH through weight loss and improvement of lifestyle habits achieves some effect, as do other treatments such as antioxidant agents and insulin resistance-improving agents, treatments are nonetheless still inadequate for improving long-term outcomes. Further exploration of the relationship between adult GHD and NAFLD/NASH may achieve linkages between general understanding of the onset mechanism for NASH and therapeutic applications.
6. Conclusion
In Japan, where the era of gluttony has arrived, NAFLD has become the most prevalent liver disease. In the span of several years, NAFLD/NASH is predicted to become the most important disease causing hepatic cirrhosis and hepatocellular carcinoma. Age-related decreases in DHEA and GH have been suggested as contributory to pathologic progression of NAFLD, and future therapeutic application of these substances is possible; further investigation of the pathology of NASH is needed from perspectives of endocrinology and Anti-Aging Medicine 76). Though there is no disagreement regarding
the usefulness of exercise therapy as treatment, additional scientific validation is needed to determine the optimal exercise parameters for preventing fatty liver. Reports of telomere shortening 77) and decreased expression of senescence
marker protein-30 in cases progressing to NASH 78) are highly
interesting in the context of associations between aging and pathologic progression of NASH; these observations portend an understanding of the pathology informed by aging, and the development of relevant modes of treatment.
Conflict of interest statement:
The authors declare no financial or other conflicts of interest in the writing of this paper.
References
1) Okanoue T, Tamura S, Tsubouchi H, et al: 2010 Guide to Medical Care for NASH/NAFDL. The Japan Society of Hepatology (ed.), Bunkodo 2010
2) Okanoue T, Nishihara T, Ono M, et al: Japan Society of Hepatology Consensus Kobe 2009: Diagnosis and treatment of NASH. Liver 2009 50:741-7
3) Hashimoto E: Nonalcoholic fatty liver disease (NAFLD): Causes, pathology, and treatment. Japan Medical Journal 2010 4491:49-53
4) Hashimoto E: Atlas of pathologic diagnosis (9): Pathological diagnosis of liver disease. Journal of Tokyo Women's Medical University 2008 78:85-9
5) Hashimoto E: Pathological diagnosis of NAFLD. Treatment 2007 89:1656-62
6) Day CP, James O F.W: Steatohepatitis: A tale of two “hits”? Gastroenterology 1998: 114:842-84
7) Sumida Y, Naito Y, Yoshikawa T: Free radicals and nonalcoholic fatty liver disease (NAFLD)/nonalcoholic steatohepatitis (NASH). Free Radical Biology in Digestive Diseases 2011 29: 144-55
8) Romeo S, Kozlitina J, Xing C, et al: Genetic variation in PNPLA3 confers susceptibility to nonalcoholic fatty liver disease. Nat Genet. 2008 40:1461-5
9) Hashimoto E, Tokushige K: Prevalence, gender, ethnic variations and prognosis of NASH. J Gastroenterol 2011: 46S: 63-9 10) Browning JD, Szczepaniak LS, Dobbins R,et al: Prevalence of
hepatic steatosis in an urban population in the United States: impact of ethnicity. Hepatology. 2004; 40:1387-95
11) Yatsuji S, Hashimoto E, Tobari M, et al: Clinical features and outcomes of cirrhosis due to non-alcoholic steatohepatitis compared with cirrhosis caused by chronic hepatitis C. J Gastroenterol Hepatol. 2009 ;24: 248-54
12) Kleiner DE, Brunt EM, Van Natta M, et al: Nonalcoholic Steatohepatitis Clinical Research Network. Related Articles: Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005; 41: 1313-1321 13) Hashimoto E. Farrell GC: “Will non-invasive markers replace
liver biopsy for diagnosing and staging fibrosis in NASH?” J Gastroenterol Hepatol 2009:24; 501-8
14) Sumida Y, Yoneda M, Hyogo H, et al: A simple clinical scoring system using ferritin, fasting insulin, and type IV collagen 7S for predicting steatohepatitis in nonalcoholic fatty liver disease. J Gastroenterol. 2011; 46: 257-68
15) Angulo P, Hui JM, Marchesini G, et al: The NAFLD fibrosis score: a noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007; 45: 846-54
16) Sumida Y, Eguchi Y, Ono M: Current status and agenda in the diagnosis of nonalcoholic steatohepatitis in Japan. World J Hepatol 2010; 2: 374-83
17) New developments in d r ug therapy for nonalcoholic steatohepatitis (NASH). Japan Medical Association 2009 138:1117-20
18) Vuppalanchi R, Chalasani N: Nonalcoholic fatty liver disease and nonalcoholic steatohepatitis: selected practical issues in their evaluation and management. Hepatology. 2009: 49: 306-317 19) Musso G, Gambino R, Cassader M, et al: A meta-analisis of
randomized trials for the treatment of nonalcoholic fatty liver disease. Hepatology 2010; 52; 79-104
20) Onji M, et al: The Japanese Societies Gastroenterology, ed. Obesity and Gastroenterological Disease. Kanehara Shuppan 2010
21) Belfort R, Harrison SA, Brown K, et al: A placebo-controlled trial of pioglitazone in subjects with nonalcoholic steatohepatitis. N Engl. J Med 2006; 355: 2297-2307
22) Sanyal AJ, Chalasani N, Kowdley KV, et al: Pioglitazone, Vitamin E, or Placebo for Nonalcoholic Steatohepatitis. N Engl J Med 2010; 362;18 1675-1685
23) Shimamoto K: Metabolic Syndrome and NASH: Best approaches to treatment of NASH. Tokyo, Chugai-Igakusha, 46-51, 2008
24) Durstine JL, Grandjean PW, Cox CA, et al: Lipids, lipoproteins, and exercise. J Cardiopulm Rehabil 22: 385-398, 2002
25) Sreenivasa Baba C, Alexander G, Kalyani B, et al: Effect of exercise and dietary modification on serum aminotransferase levels in patients with nonalcoholic steatohepatitis. J Gastroenterol Hepatol 21: 191-198, 2006
26) Perseghin G, Lattuada G, De Cobelli F, et al: Habitual physical activity is associated with intrahepatic fat content in humans. Diabetes Care 30: 683-688, 2007
27) Krasnoff JB, Painter PL, Wallace JP, et al: Health-related fitness and physical activity in patients with nonalcoholic fatty liver disease. Hepatology 47: 1158-1166, 2008
28) St George A, Bauman A, Johnston A, et al: Independent effects of physical activity in patients with nonalcoholic fatty liver disease. Hepatology 50: 68-76, 2009
29) Zelber-Sagi S, Nitzan-Kaluski D, Goldsmith R, et al: Role of leisure-time physical activity in nonalcoholic fatty liver disease: a population-based study. Hepatology 48: 1791-1798, 2008 30) Hallsworth K, Fattakhova G, Hollingsworth KG, et al: Resistance
exercise reduces liver fat and its mediators in non-alcoholic fatty liver disease independent of weight loss. Gut 60: 1278-1283, 2011 31) Kistler KD, Brunt EM, Clark JM, et al: Physical activity
recommendations, exercise intensity, and histological severity of nonalcoholic fatty liver disease. Am J Gastroenterol 106: 460-468, 2011
32) Basaranoglu M, Kayacetin S, Yilmaz N, et al: Understanding mechanisms of the pathogenesis of nonalcoholic fatty liver disease. World J Gastroenterol 16: 2223-2226, 2010
33) Rinella ME, Elias MS, Smolak RR, et al: Mechanisms of hepatic steatosis in mice fed a lipogenic methionine choline-deficient diet. J Lipid Res 49: 1068-1076, 2008
34) Rector RS, Thyfault JP, Morris RT, et al: Daily exercise increases hepatic fatty acid oxidation and prevents steatosis in Otsuka Long-Evans Tokushima Fatty rats. Am J Physiol Gastrointest Liver Physiol 294: G619-G626, 2008
35) Latruffe N, Vamecq J: Peroxisome proliferators and peroxisome proliferator activated receptors (PPARs) as regulators of lipid metabolism, Biochimie 79: 81-94, 1997
36) Shimano H, Yahagi N, Amemiya-Kudo M, et al: Sterol regulatory element-binding protein-1 as a key transcription factor for nutritional induction of lipogenic enzyme genes. J Biol Chem 274: 35832-35839, 1999
37) Shimomura I, Bashmakov Y, Horton JD, et al: Increased levels of nuclear SREBP-1c associated with fatty livers in two mouse models of diabetes mellitus. J Biol Chem 274: 30028-30032, 1999
38) Pégorier JP, Le May C, Girard J: Control of gene expression by fatty acids. J Nutr 34: 2444S-2449S, 2004
39) Kawasaki T, Igarashi K, Koeda T, et al: Rats fed fructose-enriched diets have characteristics of nonalcoholic hepatic steatosis. J Nutr 139: 2067-2071, 2009
40) Nseir W, Nassar F, Assy N: Soft drinks consumption and nonalcoholic fatty liver disease. World J Gastroenterol 16: 2579-2588, 2010
41) Nilsson LH, Hultman E: Liver and muscle glycogen in man after glucose and fructose infusion. Scand J Clin Lab Invest 33: 5-10, 1974
42) Aoi W, Naito Y, Hang LP, et al: Regular exercise prevents high-sucrose diet-induced fatty liver via improvement of hepatic lipid metabolism. Biochem Biophys Res Commun 2011;413(2) :330-335
43) Sauk JJ, Nikitakis N, Siavash H: Hsp47 a novel collagen binding serpin chaperone, autoantigen and therapeutic target. Front Biosci 10: 107-118, 2005
44) Arlt W: Dehydroepiandrosterone and ageing. Best Pract Resn Clin Endocrinol Metab 2004; 18: 363-80
45) Lasco A, Frisina N, Morabito N, et al: Metabolic effects of dehydroepiandrosterone replacement therapy in postmenopausal women. Eur J Endocrinol 2001; 145: 457-61
46) Jakubowicz D, Beer N, Rengifo R: Effect of dehydroepiandrosterone on cyclic-guanosine monophosphate in men of advancing age. Ann N Y Acad Sci 1995; 774: 312-5
47) Kawano M: Complement regulatory proteins and autoimmunity. Arch Immunol Ther Exp (Warsz) 2000;48:367-72
48) Dhatariya K, Bigelow ML, Nair KS. Effect of dehydroepiandrosterone replacement on insulin sensitivity and lipids in hypoadrenal women. Diabetes 2005; 54: 765-9
49) Bed narek-Tupi kowska G, Gosk I, et al: Inf luence of dehydroepiandrosterone on platelet aggregation, superoxide dismutase activity and serum lipid peroxide concentrations in rabbits with induced hypercholesterolemia. Med Sci Monit 2000; 6: 40-5
50) Poynter ME, Daynes RA: Peroxisome proliferator-activated receptor alpha activation modulates cellular redox status, represses nuclear factor-kappaB signaling, and reduces inflammatory cytokine production in aging. J Biol Chem 1998; 273: 32833-41
51) Peters JM, Zhou YC, Ram PA, et al: Peroxisome proliferator-activated receptor alpha required for gene induction by dehydroepiandrosterone-3 beta-sulfate. Mol Pharmacol 1996; 50: 67-74
52) Enomoto M, Adachi H, Fukami A, et al: Serum dehydroepiandrosterone sulfate levels predict longevity in men: 27-year follow-up study in a community-based group (Tanushimaru study) . J Am Geriatr Soc 2008; 56: 994-8
53) Yonei Y: Antiaging screening, Rinsho to Kenkyu 2010 87:459-464, 2010
54) Phillips AC, Carroll D, Gale CR, et al: Cortisol, DHEAS, their ratio and the metabolic syndrome: evidence from the Vietnam Experience Study. Eur J Endocrinol 2010; 162: 919-23.
55) Chen YC, Chang HH, Wen CJ, et al: Elevated ser um dehydroepiandrosterone sulphate level correlates with increased risk for metabolic syndrome in the elderly men. Eur J Clin Invest 2010; 40: 220-5
56) Fukui M, Kitagawa Y, Nakamura N, et al: Association between urinary albumin excretion and serum dehydroepiandrosterone sulfate concentration in male patients with type 2 diabetes: a possible link between urinary albumin excretion and cardiovascular disease. Diabetes Care 2004; 27: 2893-7.
57) F u k u i M , K it a g aw a Y, Na k a m u r a N , e t a l: S e r u m dehydroepiandrosterone sulfate concentration and carotid atherosclerosis in men with type 2 diabetes. Atherosclerosis 2005; 181: 339-44
58) Charlton M, Angulo P, Chalasani N, et al: Low circulating levels of dehydroepiandrosterone in histologically advanced nonalcoholic fatty liver disease. Hepatology 2008; 47: 484-92 59) Sumida Y, Yonei Y, Kanemasa K, et al: Lower circulating levels
of dehydroepiandrosterone, independent of insulin resistance, is an important determinant of severity of nonalcoholic steatohepatitis in Japanese patients. Hepatol Res 2010; 40: 901-10 60) Völzke H, Aumann N, Krebs A, et al: Hepatic steatosis is
associated with low serum testosterone and high serum DHEAS levels in men. Int J Androl 2010; 33: 45-53
61) Koga M, Saito H, Mukai M, et al: Serum dehydroepiandrosterone sulphate levels in patients with non-alcoholic fatty liver disease. Intern Med 2011; 50: 1657-1661
62) Villareal DT, Holloszy JO: Effect of DHEA on abdominal fat and insulin action in elderly women and men:a randomized controlled trial. JAMA 2004; 292: 2243-8.
63) Nair KS, Rizza RA, O’Brien P, et al: DHEA in elderly women and DHEA or testosterone in elderly men. N Engl J Med 2006; 355:1647-59
64) Goto H, Yamashita S, Makita T. Preventive effects of dehydroepiandrosterone acetate on the fatty liver induced by orotic acid in male rats. Exp Anim 1998; 47: 257-60.
65) Stochholm K, Gravholt CH, Laursen T, et al: Mortality and GH deficiency: a nationwide study. Eur J Endocrinol 2007;157(1) :9-18 66) Svensson J, Bengtsson BA, Rosen T, Oden A, Johannsson G:
Malignant disease and cardiovascular morbidity in hypopituitary adults with or without growth hormone replacement therapy. J Clin Endocrinol Metab 2004;89(7) :3306-12
67) Kaji H, Sakurai T, Iguchi G, et al: Adult growth hormone deficiency in Japan: results of investigation by questionnaire. Endocr J 2002;49(6) :597-604
68) Ichikawa T, Hamasaki K, Ishikawa H, et al: Non-alcoholic steatohepatitis and hepatic steatosis in patients with adult onset growth hormone deficiency. Gut 2003;52(6) :914
69) Takahashi Y, Iida K, Takahashi K, et al: Growth hormone reverses nonalcoholic steatohepatitis in a patient with adult growth hormone deficiency. Gastroenterology 2007;132(3) :938-43 70) Adams LA, Feldstein A, Lindor KD, Angulo P: Nonalcoholic
fatty liver disease among patients with hypothalamic and pituitary dysfunction. Hepatology 2004;39(4) :909-14
71) Sesmilo G, Biller BM, Llevadot J, et al: Effects of growth hor mone ad m i n ist rat ion on i nf lam mator y and other cardiovascular risk markers in men with growth hormone deficiency. A randomized, controlled clinical trial. Ann Intern Med 2000;133(2) :111-22
72) Sesmilo G, Miller KK, Hayden D, Klibanski A: Inflammatory cardiovascular risk markers in women with hypopituitarism. J Clin Endocrinol Metab 2001;86(12) :5774-81
73) Evans LM, Davies JS, Anderson RA, et al: The effect of GH replacement therapy on endothelial function and oxidative stress in adult growth hormone deficiency. Eur J Endocrinol 2000;142(3) :254-62
74) Kokoszko A, Karbownik M, Lewinski A: Increased lipid peroxidation in growth hormone-deficient adult patients. Neuro Endocrinol Lett 2006;27(1-2) :225-30
75) Lonardo A, Loria P, Leonardi F, et al: Growth hormone plasma levels in nonalcoholic fatty liver disease. Am J Gastroenterol 2002;97(4) :1071-2
76) Loria P, Carulli L, Bertolotti M, Lonardo A: Endocrine and liver interaction: the role of endocrine pathways in NASH. Nat Rev Gastroenterol Hepatol 2009; 6: 236-47
77) Nakajima T, Moriguchi M, Katagishi T, et al: Premature telomere shortening and impaired regenerative response in hepatocytes of individuals with NAFLD. Liver Int 2006; 26: 23-31
78) Park H, Ishigami A, Shima T, et al: Hepatic senescence marker protein-30 is involved in the progression of nonalcoholic fatty liver disease. J Gastroenterol 2010; 45: 426-34