総 説
REVIEW ARTICLE
高齢者の前立腺肥大症に対する外科的治療法: PVP と HoLEP
関 成人
公立学校共済組合 九州中央病院 泌尿器科 (平成26 年 11 月 17 日受理,平成 27 年 1 月 3 日掲載決定)Surgical Treatments for Older Men with Benign Prostatic Hyperplasia
Narihito Seki
Department of Urology, Kyushu Central Hospital of the Mutual Aid Association of Public School Teachers
(Received November 17, 2014, Accepted January 3, 2015)
要 旨 前立腺肥大症に対する手術治療として,波長532 nm の LBO レーザーを用いる光選択的レーザー前立腺蒸散術(PVP) ならびにHo:YAG レーザー(波長 2140 nm)による前立腺核出術(HoLEP) は,いずれも標準術式である経尿道的前立腺 切除術(TURP)と同等の治療効果を示す一方で,周術期の出血リスクの軽減や術後のカテーテル留置や入院期間の短 縮が期待できる有用な方法として我国において普及が進んでいる. キーワード:前立腺肥大症,光選択的レーザー前立腺蒸散術,ホルミウムレーザー前立腺核出術,経尿道的前立腺切除術 Abstract
Both photoselective vaporization of the prostate with LBO laser (532 nm in wave length) and holmium laser (2140 nm in wave length) enucleation of the prostate which does represent the technical development in the treatment of BPH, have been popular as endosurgical alternatives to traditional transurethral resection of the prostate. These techniques appear to be effective with less morbidity including a reduced rate of transurethral resection syndrome and minimal peri- and post-operative bleeding, as well as having a shorter duration of catheterization and hospital stay.
Key words:Benign prostatic hyperplasia, PVP, HoLEP, TURP
1. はじめに
前立腺肥大症(BPH: Benign prostatic hyperplasia)に対
する外科的治療(手術)は,下部尿路症状(LUTS: Lower urinary tract symptom)ならびに他覚所見(尿流量や残尿量)
をよく改善し,難治性あるいは再発性の尿閉や,BPH に 伴う重篤な合併症(持続する血尿,膀胱結石,再発性尿 路感染症など)を呈する症例,あるいは薬物治療にて効 果不十分な症例に対して,その治療選択肢の一つとして 推奨されている.現在,手術治療の標準的術式は高周波 電流を用いる経尿道的前立腺切除術(TURP: Transurethral
resection of the prostate)であるが,これ以外にも,従来の
開放手術(被膜下前立腺腺腫摘出術)に加え,各種レー ザーやマイクロ波等を利用する多数の経尿道的な術式が 開発され,日常診療に導入されてきた.本稿では,BPH
に対する外科的治療に関して概説するとともに,レーザ ーを利用する手術法である光選択的レーザー前立腺蒸 散術(PVP: Photoselective vaporization of the prostate)およ
びホルミウムレーザー前立腺核出術(HoLEP: Holmium laser enucleation of the prostate)について解説する.
〒815 −8588 福岡市南区塩原 3 −23 −1 TEL: 092 −541 −4936 FAX: 092 −541 −4540 (3 −23 −1, Shiobaru, Minami-ku, Fukuoka-city, Fukuoka, 815 −8588, Japan)
2. 外科的治療法の種類 BPH に 対 す る 手 術 療 法 は, 腺 腫 の 切 除(resection・ ablation)や蒸散(vaporization)を主体とする術式,腺腫の熱 凝固・変性を主体とする術式,ならびにその他の術式に 大別される(Table 1).経尿道的手術のうち,腺腫の切除 や蒸散を主体とする方法には,高周波電流を使用する方 法として,従来のTURP や,切除と蒸散の両方が可能で ある経尿道的前立腺電気蒸散切除術(TUVRP: Transurethral vapor-resection of the prostate),経尿道的前立腺切開術(TUIP: Transurethral incision of the prostate)に加え,生理食塩水中で
も切除や蒸散が可能なバイポーラーシステムを用いる生 理食塩水灌流経尿道的切除術(bipolar-TURP)や経尿道的バ
イポーラ電極前立腺核出術(TUBE: Transurethral enucleation with bipolar system)などがある.またレーザーを使用する
方 法 と し て は,Ho:YAG (holmium doped yttrium aluminum garnet)レーザーを用いた前立腺核出術(HoLEP)や蒸散
術(HoLAP: Holmium laser vaporization of the prostate),KTP
(Potassium -titanyl–phosphate) あるいは LBO (Lithium borate)
レーザー(いずれもNeodium:YAG レーザーの第 2 高調波を 使用したレーザーで,その発生にKTP または LBO 結晶を 使用している)による蒸散術(PVP)などが存在する. 一方,腺腫の熱凝固・変性を主体とする方法としては, マイクロ波,ラジオ波,レーザーあるいは高エネルギー超 音波を利用する高温度凝固治療法(経尿道的マイクロ波高 温度治療術 TUMT: Transurethral microwave thermotheray,
経 尿 道 的 ラ ジ オ 波 高 温 度 治 療 術 TURF: Transurethral radiofrequency thermotherapy,焦点式高エネルギー超音波
焼却術 HIFU: High-intensity focused ultrasonography,組織
内レーザー凝固術 ILCP: Interstitial laser coagulation of the prostate, 経 尿 道 的 針 焼 却 術 TUNA: Transurethral needle ablation of the prostate)が存在する.
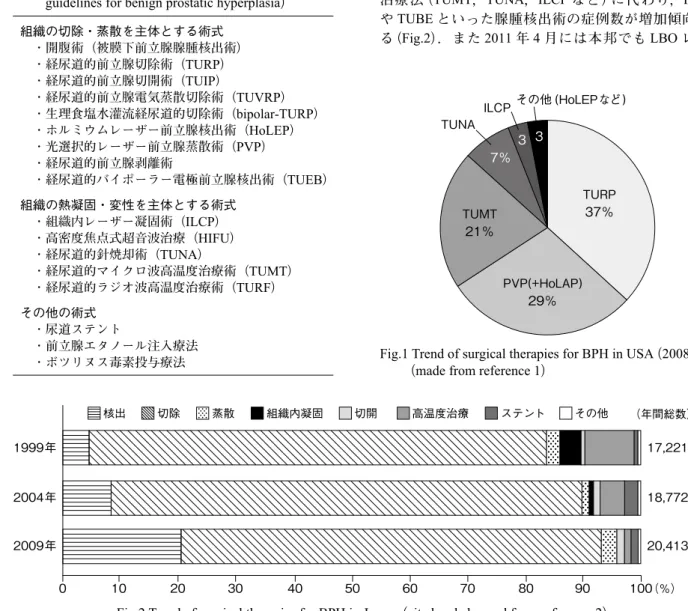
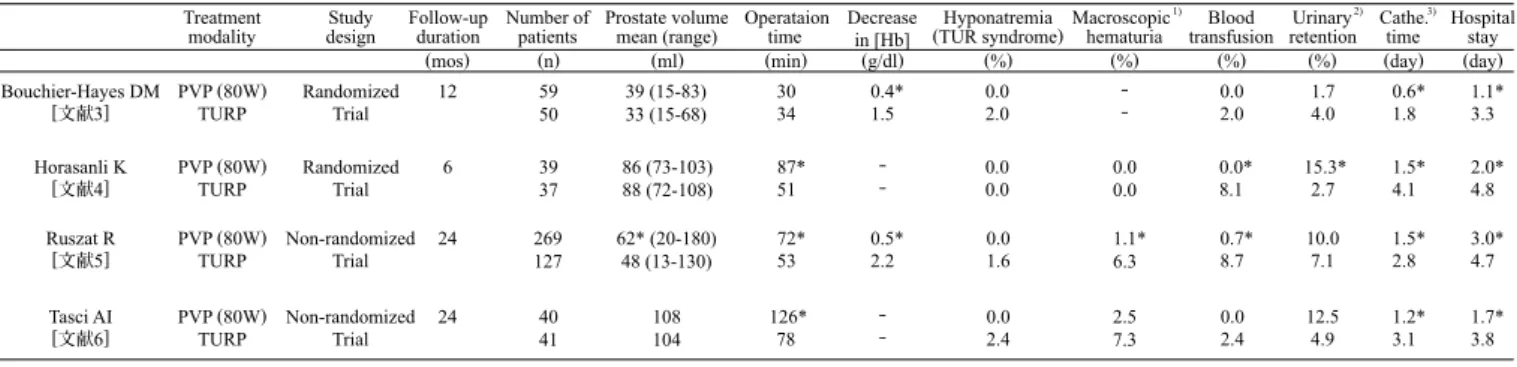
3. 外科的治療法の変遷 最近の米国における BPH に対する外科療法の動向調 査(2002-2008)によると,TURP 症例の総数に占める割 合は漸減傾向が持続している(2008 年度では約 37%). 代わって,PVP や HoLAP などのレーザーを用いた蒸散 術が占める割合は漸増しており,2008 年度には約 29% に達している1)(Fig.1). 一方,2010 年に本邦で行なわれたアンケート調査結 果2)では,漸減する従来のTURP や一連の高温度凝固 治療法(TUMT,TUNA,ILCP など)に代わり,HoLEP やTUBE といった腺腫核出術の症例数が増加傾向にあ る(Fig.2).また 2011 年 4 月には本邦でも LBO レーザ
Fig.2 Trend of surgical therapies for BPH in Japan.(cited and changed from reference 2)
Fig.1 Trend of surgical therapies for BPH in USA(2008).
(made from reference 1) Table 1 Surgical treatments for BPH.(cited from JUA clinical
guidelines for benign prostatic hyperplasia)
TURP 37% TUMT 21% 7% 3 3 PVP(+HoLAP) 29% その他 (HoLEPなど) TUNA ILCP 0 1999年 2004年 2009年 17,221 18,772 20,413 10 20 30 40 50 60 70 80 90 100(%) (年間総数) 核出 切除 蒸散 組織内凝固 切開 高温度治療 ステント その他 組織の切除・蒸散を主体とする術式 ・開腹術(被膜下前立腺腺腫核出術) ・経尿道的前立腺切除術(TURP) ・経尿道的前立腺切開術(TUIP) ・経尿道的前立腺電気蒸散切除術(TUVRP) ・生理食塩水灌流経尿道的切除術(bipolar-TURP) ・ホルミウムレーザー前立腺核出術(HoLEP) ・光選択的レーザー前立腺蒸散術(PVP) ・経尿道的前立腺剥離術 ・経尿道的バイポーラー電極前立腺核出術(TUEB) 組織の熱凝固・変性を主体とする術式 ・組織内レーザー凝固術(ILCP) ・高密度焦点式超音波治療(HIFU) ・経尿道的針焼却術(TUNA) ・経尿道的マイクロ波高温度治療術(TUMT) ・経尿道的ラジオ波高温度治療術(TURF) その他の術式 ・尿道ステント ・前立腺エタノール注入療法 ・ボツリヌス毒素投与療法
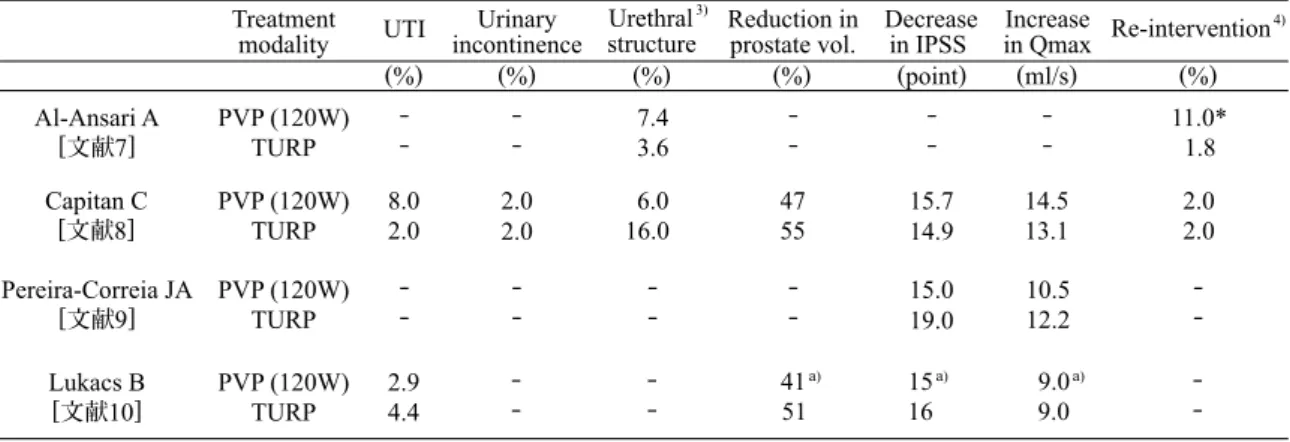
れる.治療効果に関しても,従来の外科療法に劣らない ことが報告されている.これら良好な安全性ならびに有 効性に加えて,PVP は比較的手技習得が容易な術式で あり,BPH に対する有望な新規治療法と考えられる. 一方,PVP は TURP と比較して手術時間が長いこと が指摘されているが,レーザー発生装置の発展に伴い最 大出力は上昇しており,体系的な手技向上に加え,蒸散 効率の向上による治療時間の短縮が期待される.また PVP では,個々のレーザーファイバーからの出力エネル ギーに制限があるため,大きな腺腫の治療にはコスト面 での課題が残っている.PVP の普及に伴い,治療効果 や周術期ならびに術後合併症に関するTURP との比較試 験の報告が集積されている. 4.2 有効性と安全性 80W KTP レーザーを用いた PVP と TURP の無作為化 比較研究を含めた最近の研究3-6)では,自覚症状(国際
前立腺症状スコア IPSS: International Prostate Symptom Score)や最大尿流量(Qmax)の改善効果(変化量)は両者 ほぼ同等との報告が多いが,前立腺体積が比較的大きい 症例群での検討結果4)では,TURP に比べて PVP の効 果が劣る可能性も報告されている(Table 2 および Table 3).また周術期のデータについては,PVP においてカテ ーを用いたPVP に薬事承認がおり,保険診療が可能と なったことから徐々に普及しつつある. 高齢者の良性疾患であるBPH の術式選択に際しては, 良好で安定した効果に加え,より低侵襲で安全性の高い 治療法が重視されることから,HoLEP や PVP などのレ ーザーによる核出ならびに蒸散術の臨床現場への導入が 一層加速されるものと考えられる. 4. 光選択的レーザー前立腺蒸散術(PVP) 4.1 概要 波長532 nm の KTP あるいは LBO レーザーを用いる 経尿道的蒸散術である.波長532 nm のレーザーは水よ り酸化ヘモグロビンに吸収され易く,前立腺など血流豊 富な組織では光侵達の深度が浅い(0.5-2 mm 程度)ため, 効率的な蒸散が可能である.前立腺部尿道にTURP と同 様なcavity が形成され,術後早期より症状の改善が期待 できる.灌流液には生理食塩水が使用でき,術中出血が 非常に少なく安全性が高い方法であり,抗凝固治療中や 重篤な循環器系疾患を合併するハイリスク症例にも適応 される.従来のTURP と比較した利点として,1)術中 から術後にかけて出血リスクが低い,2)低ナトリウム血 症(TUR 症候群)の発症頻度が低い,3)術後のカテーテ ル留置や在院期間の短縮が可能であることなどが挙げら
Table 3 Post-operative outcomes and complications of PVP with 80 W KTP laser reported in TURP-controlled studies. Table 2 Study design, patients background and peri-operative results of reported TURP-controlled studies for PVP with 80 W KTP laser.
Treatment
modality designStudy Follow-upduration Number ofpatients
(mos) (n)
Bouchier-Hayes DM
[文献3] PVP (80W)TURP RandomizedTrial 12 5950
Horasanli K
[文献4] PVP (80W)TURP RandomizedTrial 6 3937
Ruszat R
[文献5] PVP (80W)TURP Non-randomizedTrial 24 269127
Tasci AI
[文献6] PVP (80W)TURP Non-randomizedTrial 24 4041
* P<0.05 (PVP vs TURP)
1) Hematuria required bladder washout or re-catheterization 2) Acute urinary retention with temporary catheterization 3) Duration of post-operative urethral indwelling catheterization
Prostate volume
mean (range) Operataiontime Decreasein [Hb] (TUR syndrome)Hyponatremia Macroscopic
1) hematuria (ml) (min) (g/dl) (%) (%) (%) (%) 39 (15-83) 33 (15-68) 3034 0.4*1.5 0.02.0 ‐‐ 86 (73-103) 88 (72-108) 87*51 ‐‐ 0.00.0 0.00.0 62* (20-180) 48 (13-130) 72*53 0.5*2.2 0.01.6 1.1*6.3 108 104 126*78 ‐‐ 0.02.4 2.57.3 Blood transfusion Urinary 2) retention Cathe. 3)
time Hospitalstay
(day) (day) 0.0 2.0 1.74.0 0.6*1.8 1.1*3.3 0.0* 8.1 15.3*2.7 1.5*4.1 2.0*4.8 0.7* 8.7 10.07.1 1.5*2.8 3.0*4.7 0.0 2.4 12.54.9 1.2*3.1 1.7*3.8 Treatment
modality UTI4) incontinenceUrinary Urethral
5)
structure Reduction inprostate vol. Decrease
6)
in IPSS in QmaxIncrease
(%) (%) (%) (%) (point) (ml/s) Bouchier-Hayes DM [文献3] PVP (80W)TURP 8.54.0 ‐ ‐ 6.88.0 268 15.513.5 10.010.1 Horasanli K [文献4] PVP (80W)TURP 15.313.5 0.00.0 5.18.1 41*63 5.8*13.8 4.7*10.5 Ruszat R [文献5] PVP (80W)TURP 7.17.9 ‐‐ 8.95.5 4463 ‐‐ ‐‐ Tasci AI [文献6] PVP (80W)TURP 7.57.3 12.25.0 0.04.9 ‐51 18.818.3 13.110.6 * P<0.05 (PVP vs TURP)
4) Urinary tract infection
5) Stricture or bladder neck constricute with intervention 6) Decrease in International Prostate Symptom Score 7) Re-intervention for the resection of residual adenoma
Re-intervention7) (%) 10.2 4.0 17.9* 0.0 6.7 3.9 7.5 2.4
ーテル留置期間と入院期間は有意に短く,出血量(ヘモ グロビン密度 [Hb] 低下量)も有意に少ないが,手術時間 はTURP と比較して有意に長いとの報告が多い4-6).低 ナトリウム血症(TUR 症候群)の発症率は,TURP でや や高い傾向(1.6-2.4%)が認められる.さらに術後出血に 伴うトラブルにて処置(膀胱洗浄による血塊除去,血塊 による尿閉/ カテ留置)を要した症例の割合は TURP で 高い傾向にある5).特に,術中~術後の出血により輸血 を必要とした割合はTUR 群で有意に高いとの報告が多 く見られる.術後の主な合併症では,尿路感染症や膀胱 頚部/ 尿道狭窄症の発症率に大きな差は認めないが,観 察期間中にBPH に対する再手術を行った割合は TURP 群(0- 4%)と比べ PVP 群で約 7-18% と高く,特に大きな 前立腺では再手術率が有意に高い.前立腺体積の減少率 は,TURP で 50-60%,PVP で概ね 40% 程度である. 一方,わが国で保険承認された120W LBO レーザー を用いたPVP(LBO-PVP)についても,自他覚所見の改
善効果(IPSS ならびに Qmax の変化量)は良好で,TURP
との間に有意差を認めていない7-10). 80W KTP-PVP と同様に,LBO-PVP 群のカテーテル留 置ならびに入院期間はTURP 群に比較して有意に短く, [Hb] 低下量も少ない.また手術時間についても,TURP 群に比べLBO-PVP 群で有意に長いとの報告が多いが, 80W KTP-PVP の結果と比較すると,TURP との時間差 は減少傾向にある7,8,10).低ナトリウム血症や術中/ 術後 の出血に関しても,80W KTP-PVP と同様か,やや良好な 結果が報告されている.また膀胱洗浄を要した血尿や, 輸血を要した出血の割合も,TURP 群に比べ LBO-PVP 群 で低く,輸血率について両群間に有意差を認めている7). 術後の合併症に関しても,80W KTP-PVP と同様の傾 向が確認され,尿路感染症や膀胱頚部/ 尿道狭窄症およ び尿失禁の発症率は,TURP とほぼ同等である.一方, BPH に 対 す る 再 手 術 率 は,KTP-PVP(7-18%)に 比 べ LBO-PVP では約 2-11% とやや低下を認めるが,依然と してTURP 群(2%)と比べて高い.前立腺体積の減少率は,
LBO-PVP では 45% 程度である(Table 4 および Table 5).
5. ホルミウムレーザー前立腺核出術(HoLEP) 5.1 概要 Ho:YAG レーザーは波長が 2140 nm で水によく吸収さ れ,組織への光侵達深さが0.4 mm と浅く一定しており, 軟部組織に対する優れた蒸散,切開ならびに止血(凝固) 作用を有している.HoLEP は本レーザーを用いて経尿 道的に肥大した腺腫を前立腺の外科的被膜(移行領域と
Table 5 Post-operative outcomes and complications of PVP with 120 W LBO laser reported in TURP-controlled randomized studies.
Table 4 Study design, patients background and peri-operative results of reported TURP-controlled randomized studies for PVP with 120 W LBO laser.
Blood transfusion Urinary
2)
retention Cathe.time Hospitalstay
(day) (day) 0.0* 20.0 1.4*2.7 2.3*4.1 0.0 6.0 10.08.0 1.0*3.0 1.6*3.6 0.0 0.0 0.00.0 2.03.0 1.5 1.5 2.97.1 Treatment
modality designStudy Follow-upduration Number ofpatients Prostate volumemean (range) Operataiontime Decreasein [Hb] (TUR syndrome)Hyponatremia Macroscopic
1)
hematuria
(mos) (n) (ml) (min) (g/dl) (%) (%) (%) (%)
Al-Ansari A
[文献7] PVP (120W)TURP RandomizedTrial 36 6060 6062 89*80 0.72.9 0.05.0 10.0 0.0 ‐‐
Capitan C
[文献8] PVP (120W)TURP RandomizedTrial 24 5050 5153 54*48 0.04.0
Pereira-Correia JA
[文献9] PVP (120W)TURP RandomizedTrial 24 1010 43 (30-58)47 (30-60) 4540
Lukacs B
[文献10] PVP (120W)TURP RandomizedTrial 12 6970 51 (20-80)50 (20-85) 71*
a) 55 1.0* a) 2.5 ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐‐ ‐ ‐ ‐‐ ‐ ‐ ‐ ‐ * P<0.05 (PVP vs TURP) a) median value
1) Hematuria required bladder washout or re-catheterization 2) Acute urinary retention with temporary catheterization
Treatment
modality UTI incontinenceUrinary Urethral
3)
structure Reduction inprostate vol. Decreasein IPSS in Qmax Re-interventionIncrease 4)
(%) (%) (%) (%) (point) (ml/s) (%) Al-Ansari A [文献7] PVP (120W)TURP 7.43.6 11.0* 1.8 Capitan C [文献8] PVP (120W)TURP 8.02.0 2.02.0 16.0 6.0 4755 15.714.9 14.513.1 2.02.0 Pereira-Correia JA [文献9] PVP (120W)TURP ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐‐ ‐‐ ‐ ‐ 15.019.0 10.512.2 Lukacs B [文献10] PVP (120W)TURP 2.94.4 ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐ 41a) 51 15 a) 16 9.0 a) 9.0 * P<0.05 (PVP vs TURP)
3) Stricture or bladder neck constricute with intervention 4) Re-intervention for the resection of residual adenoma
辺縁領域との境界面)に沿って剥離し核出する方法であ る.核出した組織は膀胱内にて細切吸引(morcellation)
される.PVP と同様に前立腺部尿道に real time に cavity
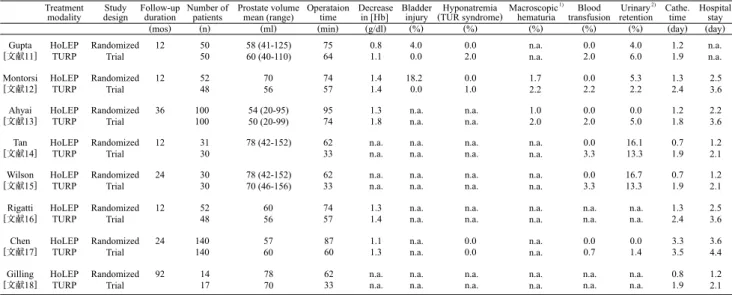
が形成され,早期より自他覚所見の改善が期待できる. 灌流液には生理食塩水が使用でき,術中出血も少なく低 侵襲な方法とされ,治療効果も従来の外科療法に劣らな いことが報告されており,BPH に対する有望な治療法 として本邦でも普及が進んでいる.HoLEP は TURP と 比較して,1)大きな腺腫にも安全に施行可能,2)低ナ トリウム血症(TUR 症候群)の発症頻度が低い,3)術後 のカテーテル留置や在院期間の短縮が可能であることが 利点とされる一方,手術時間が長いことが指摘されてい る.さらに本手技の習得にやや時間がかかることも問題 とされている.本手術の有用性に関して,従来のTURP との比較試験が多数報告されている. 5.2 有用性と安全性 無作為化比較研究11-18)では,HoLEP の自覚症状なら びに最大尿流量の改善効果はTURP と同等かやや優れて いることが報告されている(Table 6 および Table 7).周 術期の指標では,[Hb] の低下量は両者ほぼ同等である が,低ナトリウム血症(TUR 症候群)の発症率は HoLEP において低く,カテーテル留置期間と入院期間も有意 に短い.一方,手術時間はいずれの報告においても
Table 7 Post-operative outcomes and complications of HoLEP reported in TURP-controlled randomized studies.
Table 6 Study design, patients background and peri-operative results of reported TURP-controlled randomizerd studies for HoLEP.
Treatment
modality designStudy Follow-upduration Number ofpatients Prostate volumemean (range) Operataiontime Decreasein [Hb] Bladderinjury (TUR syndrome)Hyponatremia Macroscopic
1)
hematuria transfusionBlood Urinary
2)
retention Cathe.time Hospitalstay
(mos) (n) (ml) (min) (g/dl) (%) (%) (%) (%) (%) (day) (day)
HoLEP
TURP RandomizedTrial 12 5050 58 (41-125)60 (40-110) 7564 0.81.1 0.04.0 0.02.0 n.a.n.a. 0.02.0 4.06.0 1.21.9 n.a.n.a.
HoLEP
TURP RandomizedTrial 12 5248 7056 7457 1.41.4 18.2 0.0 0.01.0 1.72.2 0.02.2 5.32.2 1.32.4 2.53.6
HoLEP
TURP RandomizedTrial 36 100100 54 (20-95)50 (20-99) 9574 1.31.8 n.a.n.a. n.a.n.a. 1.02.0 0.02.0 0.05.0 1.21.8 2.23.6
HoLEP
TURP RandomizedTrial 12 3130 78 (42-152) 6233 n.a.n.a. n.a.n.a. n.a.n.a. n.a.n.a. 0.03.3 16.113.3 0.71.9 1.22.1
HoLEP
TURP RandomizedTrial 24 3030 78 (42-152)70 (46-156) 6233 n.a.n.a. n.a.n.a. n.a.n.a. n.a.n.a. 0.03.3 16.713.3 0.71.9 1.22.1
HoLEP
TURP RandomizedTrial 12 5248 6056 7457 1.31.4 n.a.n.a. n.a.n.a. n.a.n.a. n.a.n.a. n.a.n.a. 1.32.4 2.53.6
HoLEP
TURP RandomizedTrial 24 140140 5760 8760 1.11.3 n.a.n.a. 0.00.0 n.a.n.a. 0.00.7 0.01.4 3.33.5 3.64.4
HoLEP TURP Gupta [文献11] Montorsi [文献12] Ahyai [文献13] Tan [文献14] Wilson [文献15] Rigatti [文献16] Chen [文献17] Gilling
[文献18] RandomizedTrial 92 1417 7870 6233 n.a.n.a. n.a.n.a. n.a.n.a. n.a.n.a. n.a.n.a. n.a.n.a. 0.81.9 1.22.1
1) Hematuria required electric coagulation 2) including clot retention
Treatment
modality Enucleationweight Urinary
3)
incontinence Urethral
4)
structure Decreasein IPSS in QmaxIncrease Re-intervention5)
(g) (%) (%) (point) (ml/s) (%)
Gupta
[文献11] HoLEPTURP 1725 2.02.0 2.04.0 18.217.7 20.019.2 n.a.n.a. Montorsi
[文献12] HoLEPTURP 3625 1.72.2 1.77.4 17.518.0 16.916.9 n.a.n.a. Ahyai [文献13] HoLEPTURP 3637 1.11.1 7.26.6 19.418.1 24.121.6 1.03.0 Tan [文献14] HoLEPTURP 4025 3.20.0 10.0 3.2 21.718.7 13.410.0 0.03.3 Wilson [文献15] HoLEPTURP 4025 3.33.3 10.0 3.3 20.018.5 12.611.0 0.06.7 Rigatti
[文献16] HoLEPTURP n.a.n.a. 5.74.1 3.87.4 17.518.0 16.916.9 n.a.n.a. Chen
[文献17] HoLEPTURP 4941 n.a.n.a. 0.71.4 18.618.9 16.716.3 n.a.n.a. Gilling
[文献18] HoLEPTURP 4025 n.a.n.a. n.a.n.a. 18.413.4 13.8 9.6 17.6 0.0 3) De nove incontinence presisting for more than 3 months
4) including bladder neck contracture
HoLEP で長い傾向が確認されている.また術中~術後 の出血により輸血を必要とした割合はTUR 群で有意に 高いが,術後の血尿や尿閉/ カテ再留置症例の割合は両 者ほぼ同等である.なおHoLEP では morcellation に伴う 膀胱損傷のリスクが報告されている. 術後の主な合併症では,尿失禁の発症率に有意な差は 認めていないが,膀胱頚部/ 尿道狭窄の発症率は TURP で高いとの報告が多い.観察期間中にBPH に対する再 手術を行った割合はTURP に比較して低く,この傾向は 長期データからも確認されている18).なおHoLEP は前 立腺体積が100 ml を超える症例や抗凝固治療中の症例 にも安全に施行可能であるが19),他の治療法に比較し て手技の習得に時間を要する20). 6. おわりに PVP ならびに HoLEP はいずれも,BPH の標準手術で あるTURP と比較して,周術期の侵襲性が低い利点を有 しており,かつ治療効果(速効性を含めて)に殆ど遜色 がないことから,設備投資を含めた治療コストの問題は 残るものの,BPH に対する外科的治療法の有力な選択 肢として,我国において今後とも普及していく可能性が 極めて高いと考えられる. 利益相反の開示 利益相反なし. 参考文献
1) B.S. Malaeb, X. Yu, A.M. McBean, S.P. Elliott: National trends in surgical therapy for benign prostatic hyperplasia in the United State. Urology, 79(5): 1111-1116, 2012.
2) N. Masumori, T. Kamoto, N. Seki, Y. Homma: Surgical procedures for benign prostatic hyperplasia: a nationwide survey in Japan. Int. J. Urol., 18: 166-170, 2011.
3) D.M. Bouchier-Hayes, S. Van Appledorn, P. Bugeja, H. Crowe, B. Challacombe, A.J. Costello: A randomized trial of photoselective vaporization of the prostate using the 80-W potassium-titanyl-phosphate laser vs transurethral prostatectomy, with a 1-year follow-up. BJU Int., 105: 964-969, 2008.
4) K. Horasanli, M.S. Silay, B. Altay, O. Tanriverdi, K. Sarica, C. Miroglu: Photoselective potassium titanyl phosphate (KTP) laser vaporization versus transurethral resection of the prostate for prostates larger than 70 ml: a short-term prospective randomized trial. Urology, 71: 247-251, 2008.
5) R. Ruszat, S.F. Wyler, M. Seitz, K. Lehmann, C. Abe, G. Bonkat, O. Reich, T.C. Gasser, A. Bachmann: Comparison of potassium-titanyl-phosphate laser vaporization of the prostate and transurethral resection of the prostate: update of a prospective non-randomized two-center study. BJU Int., 102(10): 1432-1438, 2008. 6) A.I. Tasci, V. Tugcu, S. Sahin, F. Zorluoglu: Photoselective
vaporization of the prostate versus transurethral resection of the prostate for the large prostate: a prospective nonrandomized bicenter trial with 2-year follow-up. J. Endourol., 22(2): 347-353, 2008. 7) A. Al-Ansari, N. Younes, V.P. Sampige: GreenLight HPS 120-W
laser vaporization versus transurethral resection of the prostate for treatment of benign prostatic hyperplasia: a randomized clinical trial with midterm follow-up. Eur. Urol., 58: 349-355, 2010. 8) C. Capitan, C. Blazquez, M.D. Martin, V. Hernandez, E. de la
Pena, C. Llorente: GreenLight HPS 120-W laser vaporization versus transurethral resection of the prostate for the treatment
of lower urinary tract symptoms due to benign prostatic hyperplasia: a randomized clinical trial with 2-year follow-up. Eur. Urol., 60(4): 734-739, 2011.
9) J.A. Pereira-Correia, K.D. de Moraes Sousa, J.B.P. Santos, D. de Morais Perpetuo, L.F. Lopes-da-Silva, R.L. Krambeck, V.J.F. Muller, F.P. Vas: GreenLight HPSTM 120-W laser vaporization vs transurethral resection of the prostate (<60mL): a 2-year randomized double-blind prospective urodynamic investigation. BJU Int., 110: 1184-1189, 2012.
10) B. Lukacs, J. Loeffler, F. Bruyere, P. Blanchet, A. Gelet, P. Coloby, A. De la Taille, P. Lemaire, J-C. Baron, J-N. Corun, M. Aout. H. Rousseau, E. Vicaut: Photoselective vaporization of the prostate with GreenLight 120-W laser compared with monopolar transurethral resection of the prostate: a multicenter randomized controlled trial. Eur. Urol., 61: 1165-1173, 2012. 11) N. Gupta, Sivaramakrishna, R. Kumar, P.N. Dogra, A. Seth:
Comparison of standard transurethral resection, transurethral vapor resection and holmium laser enucleation of the prostate for managing benign prostatic hyperplasia of > 40g. BJU. Int., 97(1): 85-89, 2006.
12) F. Montorsi, R. Naspro, A. Salonia, N. Suardi, A. Briganti, M. Zanoni, S. Valenti, I. Vavassori, P. Rigatti: Holmium laser enucleation versus transurethral resection of the prostate: results from a 2-center, prospective, randomized trial in patients with obstructive benign prostatic hyperplasia. J. Urol., 172: 1926-1929, 2004.
13) S.A. Ahyai, K. Lehrich, R.M. Kuntz: Holmium laser enucleation versus transurethral resection of the prostate: 3-year follow- up results of a randomized clinical trial. Eur Urol 52(5): 1456-1464, 2007.
14) A.H. Tan, P.J. Gilling, K.M. Kennett, C. Frampton, A.M. Westenberg, M.R. Fraundorfer: A randomized trial comparing holmium laser enucleation of the prostate with transurethral resection of the prostate for the treatment of bladder outlet obstruction secondary to benign prostatic hyperplasia in large glands (40 to 200 grams). J. Urol., 170: 1270-1274, 2003. 15) L.C. Wilson, P.J. Gilling, A. Williams, K.M. Kennett, C.M.
Frampton, A.M. Westenberg, M.R. Fraundorfer: A randomized trial comparing holmium laser enucleation versus transurethral resection in the treatment of prostates larger than 40 grams: results at 2 years. Eur. Urol., 50(3): 569-573, 2006.
16) L. Rigatti, R. Naspro, A. Salonia, A. Centemero, M. Ghezzi, G. Guazzoni, A. Briganti, P. Rigatti, F. Montorsi: Urodynamics after TURP and HoLEP in urodynamically obstructed patients: are there any differences at 1 year of follow-up? Urology, 67 (6): 1193-1198, 2006.
17) Y.B. Chen, Q. Chen, Z. Wang, Y.B. Peng, L.M. Ma, D.C. Zheng, Z.K. Cai, W.J. Li, L.H. Ma: A prospective randomized clinical trial comparing plasmakinetic resection of the prostate with holmium laser enucleation of the prostate based on a 2-year followup. J. Urol., 189: 217-222, 2013.
18) P.J. Gilling, L.C. Wilson, C.J. King, A.M. Westenberg, C.M. Frampton, M.R. Fraundorfer: Long-term results of a randomized trial comparing holmium laser enucleation of the prostate and transurethral resection of the prostate: results at 7 years. BJU Int., 109: 408-411, 2011.
19) E.A. Elzayat, E.I. Habib, M.M. Elhilali: Holmium laser enucleation of prostate for patients in urinary retention. Urology, 66(4):789-793, 2005.
20) N. Seki, O. Mochida, N. Kinukawa, K. Sagiyama, S. Naito: Holmium laser enucleation for prostatic adenoma: analysis of learning curve over the course of 70 consecutive cases. J. Urol., 170: 1847-1850, 2003.